

Abstract
Study Objectives:
Several organizations have provided recommendations to ensure high school starts no sooner than 08:30. However, although there are plausible biological reasons to support such recommendations, published recommendations have been based largely on expert opinion and a few observational studies. We sought to perform a critical review of published evidence regarding the effect of high school start times on sleep and other relevant outcomes.
Methods:
We performed a broad literature search to identify 287 candidate publications for inclusion in our review, which focused on studies offering direct comparison of sleep time, academic or physical performance, behavioral health measures, or motor vehicular accidents in high school students. Where possible, outcomes were combined for meta-analysis.
Results:
After application of study criteria, only 18 studies were suitable for review. Eight studies were amenable to meta-analysis for some outcomes. We found that later school start times, particularly when compared with start times more than 60 min earlier, are associated with longer weekday sleep durations, lower weekday-weekend sleep duration differences, reduced vehicular accident rates, and reduced subjective daytime sleepiness. Improvement in academic performance and behavioral issues is less established.
Conclusions:
The literature regarding effect of school start time delays on important aspects of high school life suggests some salutary effects, but often the evidence is indirect, imprecise, or derived from cohorts of convenience, making the overall quality of evidence weak or very weak. This review highlights a need for higher-quality data upon which to base important and complex public health decisions.
Citation:
Morgenthaler TI, Hashmi S, Croft JB, Dort L, Heald JL, Mullington J. High school start times and the impact on high school students: what we know, and what we hope to learn. J Clin Sleep Med 2016;12(12):1681–1689.
Keywords: high school, sleep start time, timing
INTRODUCTION
There is a growing awareness of the need for adequate sleep for health, mental and physical alertness, executive function, quality of life, and safety in the workplace and on the roads. This need exists for all age groups including adolescents and teens. The Centers for Disease Control and Prevention (CDC) partnered with two professional societies for sleep, the American Academy of Sleep Medicine and the Sleep Research Society, to create the National Healthy Sleep Awareness Project.1 The partnership has formed alliances with multiple stakeholders in sleep health, including regional sleep societies, primary care organizations, and public affairs specialists with the goal of developing and implementing a comprehensive, multiyear, nationwide sleep awareness program to promote healthy sleep. The program's primary goal is to promote the achievement of the Sleep Health objectives of Healthy People 2020, one of which is to increase the percentage of students in grades 9 through 12 who get sufficient sleep.2 The most recent national data from the Youth Risk Behavior Surveillance System show that only 31.6% of students in grades 9 through 12 got sufficient sleep (defined as 8 h or more of sleep on an average school night) in 2013, with no improvement since the first national data was collected in 2007.3 Therefore, a wide gap exists between healthy sleep practices and achievement in an unacceptable proportion of our school-aged youth.
It has been increasingly recognized that high school students get less sleep than is recommended.4,5 There are multiple factors that may be associated with decreased sleep time in this group. Anecdotal information suggests that high school start times are commonly earlier than they were decades ago, although national data have been available only for 2011 and 2014.6,7 Pressure to finish school early to allow earlier commutes, after-school activities, and administrative and transportation reasons may have influenced decisions to change to earlier start times.8 Juxtaposed against this trend is the evidence that suggests that the natural biological rhythms of adolescents and teens are a poor fit with early school start times. The circadian rhythm of teens is different than that of adults. Changes in sleep regulation associated with puberty, including delayed melatonin secretion and altered sleep drive, commonly lead to difficulty falling asleep at an early bedtime and to taking a longer time to fall asleep. Their “clocks” are set to prefer later sleep onset and later wakening.9 Early wake times necessitated by early school start times push against this natural biological clock. In addition, environmental factors such as homework, extracurricular activities, social activities, part-time work, and technology exacerbate the tendency for teens to decrease sleep time.10,11
Chronic sleep loss in adolescents and teens has been associated with physical health consequences such as increased risk of obesity,12,13 metabolic dysfunction, and cardiovascular morbidity.14–16 Health issues beginning in the teen years are likely to lead to increasingly poor health with age, imposing both an individual and societal burden. Safety issues such as an increased likelihood of motor vehicle accidents are linked to sleep loss in teens.17–19 Mental health consequences of inadequate sleep include an increased risk of anxiety and depression and decreased motivation.20–24 Academic performance is also likely to suffer in teens with chronic inadequate sleep.20,22,24–26
Largely based on these observational underpinnings, the American Academy of Pediatrics issued a policy statement recommending high school start times at 08:30 or later.27 However, in order to better promote consensus and understanding about the effects of delaying school start times on important social, educational, and health outcomes, the National Healthy Sleep Awareness Project Surveillance and Epidemiology workgroup was given the task of researching and critically reviewing the evidence from published studies regarding the effect of high school start times on sleep and other relevant outcomes.
METHODOLOGY
Literature Review
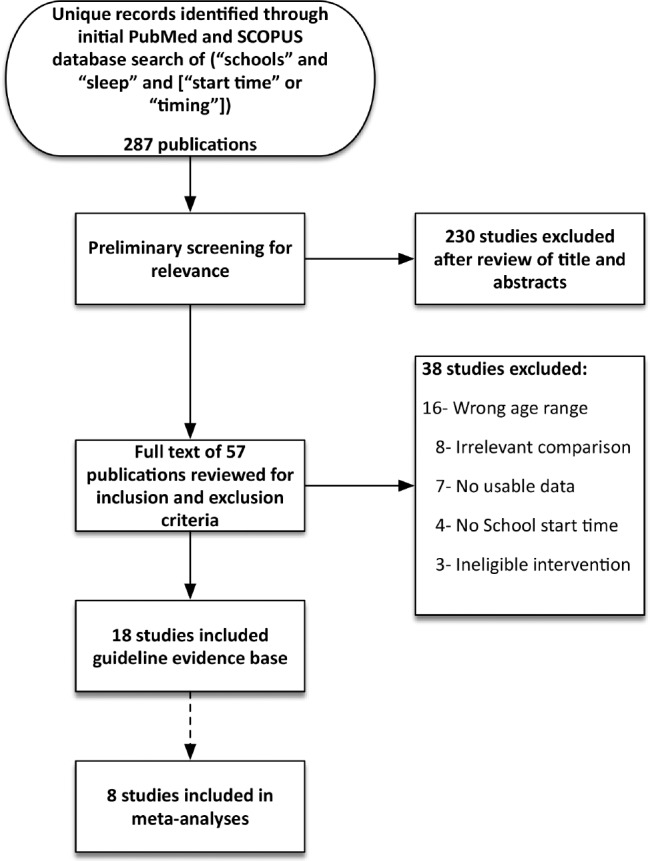
A comprehensive search was conducted in the PubMed and Scopus databases to identify any publications that addressed school start times and sleep duration. The search terms included the following keywords: “schools” and “sleep” and [“start time” or “timing”]. All searches were limited to humans and published in English. This yielded 287 records. Publication types such as reviews, newsletters, comments, editorials, and case reports were excluded. Articles that did not focus on 9th-and 12th-grade students were also excluded, but some articles that spanned grades 7 through 12 were included in the analysis.
This search strategy resulted in a total of 57 potentially relevant publications; of which 23 unique studies were identified through PUBMED and 37 through SCOPUS. A thorough review of all article titles and abstracts was conducted to identify articles of apparently sufficient relevance to review in full text. Following this review, 38 of the 57 articles were excluded, most often due to wrong age range or an irrelevant comparison, inclusion of qualitative-only data, or absence of documentation of school start times. After exclusions, 18 articles were reviewed, and 8 studies included in the meta-analysis. Figure 1 documents the literature search process.
Figure 1. PRISMA diagram for literature search to examine effect of high school start times on outcomes of interest.
Outcomes of Interest
During review of the 57 studies, the task force inventoried outcomes described in these studies and selected those most pertinent. Studies offering direct comparison of total sleep time (TST), academic performance, physical performance, behavioral health measures, and motor vehicular accidents in populations of students with different start times were of primary focus.
Extraction of Evidence
Quantitative data pertaining to the outcomes of interest as well as information necessary for systematic evaluation were extracted from accepted articles. Eight articles contained sufficient quantitative data to allow formatting for meta-analysis. Those with data presented in a format incompatible with desired statistical analyses were used selectively for further discussion.
Statistical Analyses and Interpretation
Meta-analysis was performed using Review Manager 5.2 software and included calculations of the mean difference (MD) ± standard deviation (SD) and standardized mean differences where applicable, for desired outcomes. All analyses were performed using the random effects model. The results of meta-analyses are depicted in figures within text, in association with a forest plot. Pooled MD (black diamond) on forest plots depicts the average response or magnitude of effect across all studies, and the width of the diamond represents the associated 95% confidence interval (CI) of the average response.
RESULTS
Evidence Base
Our search strategy resulted in 18 studies in total, including 10 cross-sectional studies comparing 2 contemporaneous student populations with different start times,18,19,23,24,26,28–32 7 prospective studies evaluating the effect of school start times within the same school populations,8,17,20,21,33–35 and 1 retrospective historical cohort study that compared outcomes in school populations of one geographical area separated by many years (and therefore different actual students).36
Although most studies evaluated public school populations, two prospective studies evaluated the effect of school-start time changes on outcomes in a boarding school population.20,33 Among the eight cohort studies, seven evaluated the effect of changes to a later school start times17,20,21,33–36 and one evaluated the effect of changes to an earlier school start time in the same school.8
Among the 18 studies, 12 provided comparisons between two conditions with different distinct school start times. Among these, 9 studies had the latest school start time at 08:30 or later.17–20,24,28,34–36 In three studies, the latest school start time was still prior to 08:30.8,21,33 The median time difference between the two comparison conditions was 60 min (range, 20 to 85 min).
In six studies there was not a distinct school start time declaration.23,26,29–32 The study by Eliasson et al. focused primarily on the relationship between TST and grade point average, and their survey did not inquire regarding specific school start time.29 Ming et al. surveyed students from five New Jersey high school programs and evaluated whether school start time was associated with sleep duration, quality of sleep, or symptoms of sleep disorders.26 There were several different start times, and results were dichotomized as before or at 07:30, or after 07:30. Orzech et al. produced a qualitative analysis regarding how messaging influenced sleep habits of high school students.30 Paksarian et al. used a nationally representative, cross-sectional survey of students from 245 schools to estimate associations of school start time with sleep duration and other outcomes, so only a range of start times (07:05 to 09:22, mean 08:01) were included in the analysis rather than two distinct start times.31 Short et al.32 surveyed students from two countries (USA and Australia) attending various schools. School start times in the USA in the survey population were 07:45 ± 37 minutess vs. 08:32 ± 28 min in Australia (mean ± SD).32 Finally, Winsler et al.23 surveyed students in a highly populated county in Virginia attending 25 regular high schools and 26 middle schools. High schools in this study started at 07:20. Sleep duration was compared among students with the contemporary average start time in the USA, which was quoted as being 08:00.23
Effect of School Start Time on Total Sleep Time and Sleepiness
The outcomes evaluated according to study type are shown in Table 1. TST, most often estimated by survey response, was recorded for school nights in 15 studies,8,17,20,21,23,24,26,28–34,36 and for nonschool nights in 10 studies.8,20,21,24,26,29–31,33,36 In general, later school start times were associated with longer TSTs on school nights, though in one prospective long-term evaluation the TST initially increased with a move toward later start times, but TSTs had returned to baseline at subsequent evaluation 9 mo after the change.34 Six studies supplied data in such a way that we could determine a pooled estimate of effect size. For the five studies in which early and later school start times differed by less than or equal to 60 min, school-night sleep times increased by an average of 18.65 min (95% CI 8.13 to 29.16) (Figure 2).20,21,28,33,34 Two of these studies demonstrated a 22% improvement (95% CI: 11% to 33%) in measures of sleepiness during school day21,35 (Figure 3). When the delayed school start time differed from the early start time by more than 60 min, TST was 52.56 min (95% CI: 38.74 to 66.37) longer with the later start time24,32 (Figure 4). The available data did not allow a pooled estimate of the effect of a greater than 60-min delay in start time on daytime sleepiness. However, in total there were seven studies with a difference in start times of greater than 60 min, six of which contained data on sleepiness measurements.20,21,33–36 In each of the six studies, indications of daytime sleepiness improved, though not always with statistical significance.
Table 1.
Evidence extraction.
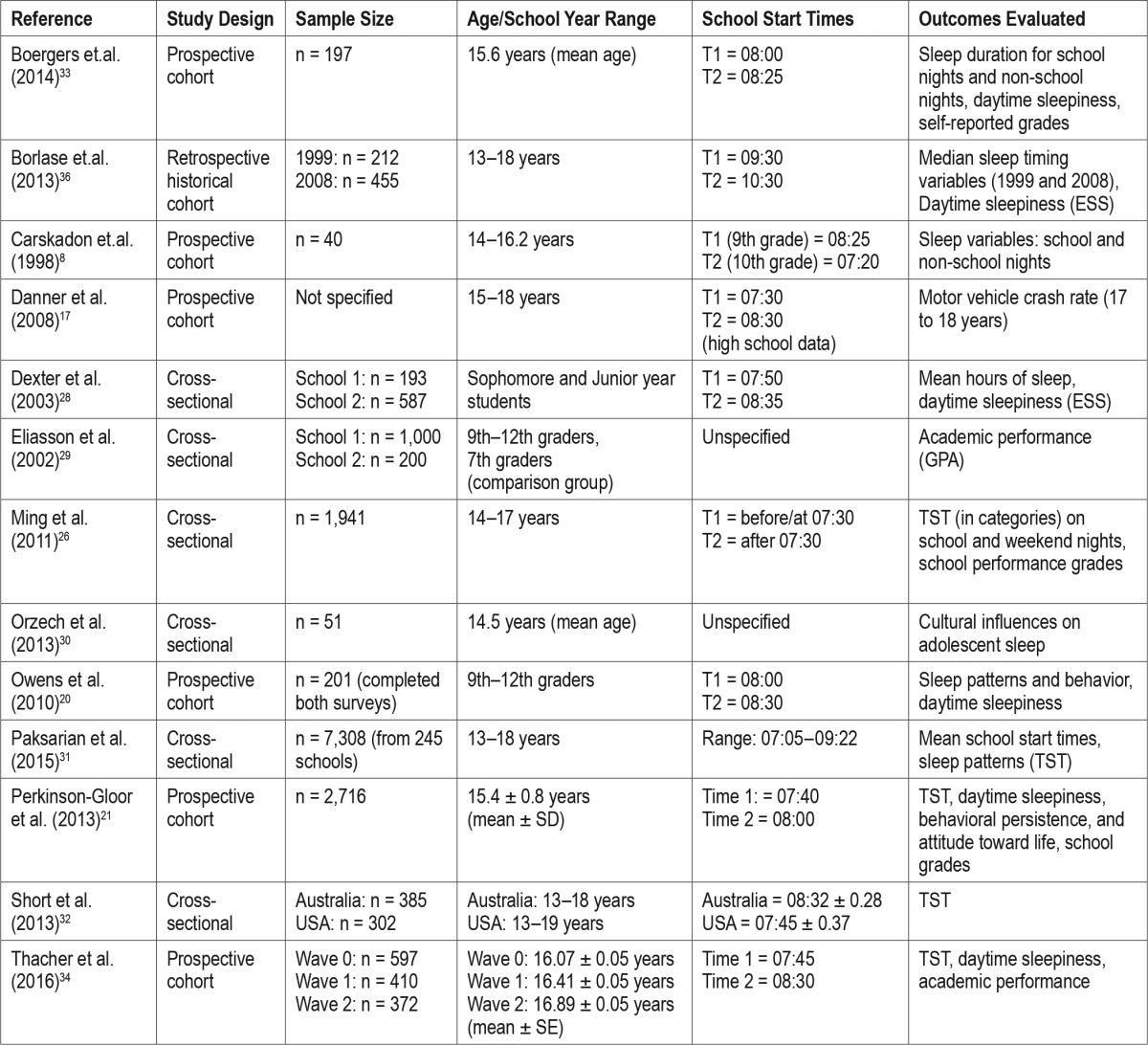
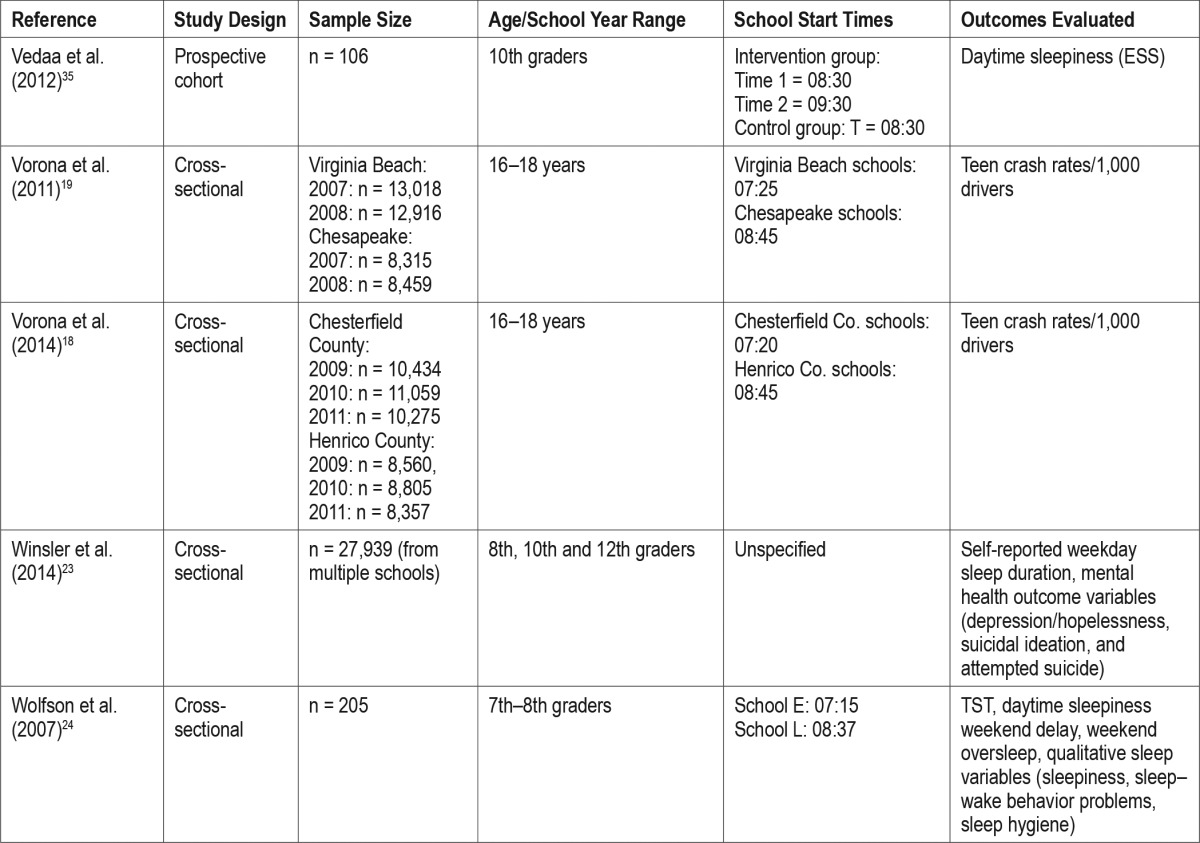
Figure 2. Average response or magnitude of effect across all studies for the effect of school start time differences 60 min or less on total school-night sleep time.

Figure 3. Average response or magnitude of effect across all studies for effect of school start time differences 60 min or less on measured sleepiness during the school day.

Figure 4. Average response or magnitude of effect across all studies for the effect of school start time differences 60 min or more on total school-night sleep time.

The estimated average duration of sleep on nonschool nights was 564.6 ± 86.9 min, compared to school night averages of 458.7 ± 74.3 min (based on data from five studies8,20,21,24,33 and nine studies,8,20,21,23,24,28,32–34 respectively). Among studies where start times differed by 60 min or less, a school night to a nonschool night's sleep difference declined by 28.08 min (95% CI: 10.55 to 45.61) (Figure 5).20,21,33 One study where the start time varied more than 60 min, the school night to nonschool night sleep time difference was reduced by 84.41 min (95% CI 65.94 to 102.88)24 (Figure 6).
Figure 5. Average response or magnitude of effect across all studies for the effect of school start time differences 60 min or less on nonschool night sleep time.

Figure 6. Average response or magnitude of effect for the effect of school start time differences more than 60 min on nonschool night sleep time.

Effect of School Start Times on Academic Performance
The effect of school start times on academic performance was examined in eight studies.20,21,24,26,29,32–34 In three, school start times varied by less than 30 min.20,21,33 None of these found a significant change in performance measured by grades, and in one no difference in hours spent engaged in either homework or extracurricular activities with the move to a later start time was reported.33 However, in studies by Boergers et al. and Owens et al., which were studies of students at boarding schools, the researchers found that teacher-reported first hour tardiness or absences declined significantly with the delay in school start time.20,33 In three studies, the difference in start times was 60 min or more.24,26,32 Ming et al.26 found that earlier school start times were associated with a greater percentage of students receiving less than 7 h of sleep during the school week. However, only if sleep duration was less on both school days and weekend days or if weekend sleep duration alone was less than 7 h did academic performance suffer.26 In the study by Wolfson et al., students with earlier start times experienced tardiness four times more often and the eighth graders had worse grade point averages as those with the later start times (76.85 ± 9.45 vs. 83.79 ± 8.80).24 Short et al. found that start times did not affect grade performance.32 In neither study by Eliasson et al. nor Thacher et al. was the differing school start time associated with significant differences in grade performance.29,34 Taken together, although delaying school start times appears to be associated with an increase in total sleep duration on school nights, this does not appear to translate into improved performance as reflected in grades or standardized test scores. The literature does, however, reflect teacher and student reports of more engagement in class time activities.20 There also may be a decrease in tardiness or truancy when school start times are later.
Behavioral Health Measures
Two cross-sectional23,24 and three prospective cohort studies20,21,33 recorded measures of behavioral health. In studies by Owens et al. and Boergers et al., which were prospective cohort studies, school start times were advanced by 30 min or less for students attending a boarding school.20,33 Both studies used the School Sleep Habits Survey to evaluate self-reported feelings of depressed mood and irritability, and both found statistically significant declines with advancing the school start times. In the study by Owens et al., there was a significant negative correlation between reported TST and depressive symptoms, and in the study by Boergers et al., depressive symptoms were less common in students who reported average sleep times exceeding 8 h.20,33 In the study by Perkinson-Gloor et al., school start times of 07:40 were compared with 08:00. In this study, there was no significant change in measures of depressed mood, anxiety, or stress experienced in the week prior to survey using the Depression, Anxiety and Stress Scale (DASS-21), a 21-item survey instrument.21 Wolfson et al. evaluated the sleep–wake patterns of young adolescents attending urban, public middle schools with early (07:15) versus later (08:37) start times. They also used the School Sleep Habits Questionnaire, but did not publish their findings regarding mood or anxiety.24 Winslor et al. evaluated students using the Fairfax County Youth Survey, an anonymous self-report survey designed to assess health, well-being, and behavioral risk factors among 27,937 adolescents in Fairfax County, VA. Their multivariate, logistic regression analyses of their large cohorts, controlling for background variables, indicated that 1 h less of weekday sleep was associated with greater odds of self-reported feelings of hopeless, serious consideration of suicide, suicide attempts, and substance use. Their results were obtained from a population of high school students with the same start times, 1 h earlier than the national average. However, the study design did not allow a determination of how school start time affected TST, which was the main independent variable in their evaluations.23
The data taken together suggest that later school start times may be associated with better behavioral health measures, but there are significant limitations in this evidence base. The studies of Owens et al. and Boergers et al. were short term, were in a primarily boarding school population, and may reflect seasonal effects because the delayed school start times coincided with spring term, versus fall term for earlier start times.20,33 The other three studies evaluating behavioral health either did not show any differences, did not report, or did not specifically evaluate the effect of a change in school start time.
Vehicular Accidents and Vigilance
Two studies by Vorona et al. and one by Danner et al. addressed the effect of school start times on the risk of vehicular accidents.17–19 In 2011, Vorona et al.19 compared accident rates across 2 y among two different cohorts of high school students with school start times that differed by 75 to 80 min. Crash rates were corrected for traffic congestion and compared with crash rates of other age groups in those communities. The cohort of students with the earlier start time had a statistically significantly higher vehicular crash rate (higher by 19.2 crashes/1,000 drivers). The increase in crash rate was particularly prevalent during school commuting times.19 In 2014, Vorona et al.18 evaluated teen cohorts from two geographically similar counties with adjacent public school systems that have different high school start times. The analysis was similar to that of the group's earlier publication, and again found a statistically significant increase in crash rates among the early start time cohort, again with peak accident rates during school commute times. In this second study, a post hoc analysis indicated that there was an increase in run-off road crashes to the right, a vehicle crash type that has been closely linked to driver fatigue and inattention.18 Danner et al. evaluated the effect of a 1-h delay in school start times in one population of students. There was a 16.5% decline in average crash rates in the 2 y following the delay in school start time among students in the cohort, compared with a 7.8% increase in crash rate across the entire state population.17 These data appear to provide consistent evidence for an association between later school start times and decreased crash rates among students.
One additional study evaluated the effect of a delay in start time on a test of sustained-attention, and reaction.35 The intervention school implemented a delay in start time of 1 h exclusively on Mondays 2 y prior to this study. Data collection took place on Mondays and Fridays for both the intervention and the control schools. They found that with the delay in school start time on Mondays, students in the intervention group slept more than 1 h longer on Sunday nights. Consequently, there was an improvement in the reaction time, a valid predictor of performance. Surprisingly, even though the reaction time suggested that the intervention group was less fatigued than students in the control group, there was not a significant improvement observed in the self-reported sleepiness scale.
DISCUSSION
A number of studies pertaining to high school start times have been evaluated with outcomes that cover a range of functional outcomes including total sleep time, sleepiness, academic performance, tardiness, absenteeism, mental health measures, substance abuse, vehicular accidents, and reaction times. Studies suggest that later school start times, particularly for delays of 60 min or more, may be effective in proffering greater sleep durations, lower weekday-weekend differences in sleep duration, and reduced daytime sleepiness. Visual reaction times and rates of vehicular accidents appear to benefit from changes to a later school start time. However, the aggregated quality of evidence supporting these associations is only moderate, and the combined evidence that scholastic improvements are associated with increasing sleep duration is weak.
Significant limitations of the current studies include the lack of information on adolescent subgroups such as those defined by sex, race/ethnicity, and socioeconomic status, as well as information on school characteristics such as urban/rural classification, transportation modes, and availability of extracurricular activities. One particularly significant problem in determining the effect of the start policy on these outcomes is the lack of studies that have examined the longitudinal effects of delayed school start times. This review and other similar recent reviews have relied primarily on cross-sectional studies that compared two or more schools with varying school start times.5,37,38 Because those schools have different characteristics that are not controlled for, study designs may vary in fundamental aspects such as duration of implementation of the change in start times, and academic term of implementation or assessment, it is difficult to determine whether actual differences in outcomes are related to the start time or to those other characteristics. For example, cross-sectional studies similar to those in this review may suffer from sampling bias brought about through nonresponse from one or another group (responders may differ from non-responders with respect to the studied outcome), or the bias associated with convenience sampling (sampling outcomes in a community that has changed its high school start time may have a greater interest in health and safety than those that do not).
As school districts begin changing school start policies, it would benefit our understanding of the effects, if pre-change and post-change outcomes were collected and evaluated in a standardized manner and published in order to contribute to a wider evidence-based literature of longitudinal intervention studies. Addition of propensity models may help reduce bias in such studies. In addition, follow-up assessments over longer time are needed in order to determine whether the observed sleep increases and other outcomes are maintained. It will also help us to understand the mechanisms of change. For instance, Perkinson-Gloor et al. claimed to see academic benefits through the pathway of improving positive attitude towards life, and also behavioral persistence.21 Longitudinal studies would provide better data for assessment of such hypotheses. Further, longitudinal studies are needed to better inform schools as to the best start times for specific ages and grades.
At least two important circadian factors warrant consideration for future research on the effect of changes in school start times. One is the location of a school within a time zone. For instance, studies in states with a large distance from east to west may have children waking at a different biological time or circadian phase, such that the same school start time will result in an earlier biological time for children in the west compared with the east. Knowing the circadian placement of the sleep period (bedtimes and rise times within the light-dark cycle) would be important for interpreting the data in future studies, and ultimately for advising the best practice for high school scheduling.
Another important circadian factor to consider in planning future studies, particularly those involving intervention, is evening exposure to light and/or “screen time,” such as watching television or using tablets, smart phones or other devices with light-emitting diodes (LEDs). Bright light, including that emitted by LEDs of eReaders, inhibits the production of melatonin, the hormone that signals the onset of nighttime and ensuing sleep time in humans.39 Use of these LED technologies during times shortly before bed, when melatonin is normally rising, is very common in adolescents. Knowing the dose of evening light exposure would be relevant in interpreting data, particularly intervention study data in this cohort.40
Various professional organizations including the American Academy of Pediatrics, the American Academy of Sleep Medicine, the American Thoracic Society, and the National Sleep Foundation recently have recognized that a healthy sleep is important for adolescents and children.27,41–43 The American Academy of Sleep Medicine and the National Sleep Foundation agree that adolescents should sleep 8 to 10 h for optimal health.41,43 However, national data for 2013 show that US high school students reported that 68.4% slept 7 h or less on school nights whereas only 23.2% slept 8 h, 6.0% slept 9 h, and 2.4% slept 10 h or more.3 In 2014, the American Academy of Pediatrics recommended that high schools and middle schools aim for start times of 08:30 or later to allow students the opportunity to achieve optimal hours of sleep and to improve physical and mental health, academic performance, safety, and quality of life.27 In the same year, the School Health Policies and Practices Study reported that 82.8% of middle schools and 92.7% of high schools started before 08:30.44 In a 2011–2012 national survey of US public schools, 81.1% of middle schools and 85.6% of high schools started before 08:30 with 40.7% of middle schools and 42.5% of high schools starting before 08:00.7 With such early start times and the morning preparation and transportation time needed for those start times, adolescents would have to initiate sleep at earlier hours than their natural circadian rhythms would allow in order to obtain at least 8 h of sleep. Therefore, it is not at all surprising that many adolescents do not receive sufficient sleep on school days.
Parent groups across the nation are active in lobbying their school leadership at a local level to delay school start times, as this is a decision often determined at the individual school system level rather than at a state level. Parent groups often meet with considerable resistance in terms of realistic school system concerns about changes in bus scheduling and potential increases in transportation costs; difficulties in planning after-school extracurricular activities and athletic events, which may run into darkness during the winter months; and potential increased traffic congestion during rush hours.27 Other parents have concerns about shifting younger children to earlier school hours; child care issues when older siblings serve as caretakers of younger children but may arrive home later; and student afternoon employment opportunities. Information about how some schools systems and communities have successfully overcome these barriers is available at http://www.startschool-later.net/case-studies.html
CONCLUSIONS
We have provided a systematic review with meta-analysis of certain key outcomes from studies seeking to understand the effect of early versus late start times on high school students. We have found that we know with some confidence that later start times are associated with increased total sleep duration, lower weekday-weekend differences in sleep duration, and reduced subjective daytime sleepiness. Due to limitations in study design, we do not know with confidence that movement of school start times from early to later will result in improved academic performance or in improved mental health parameters, though this may be the case. The current trend toward later school start times makes biological sense. However, there is much more to learn regarding circadian issues in youth of different ages. As a nation, we are in need of well-designed and appropriately powered research to illuminate these key issues so that complex trade-offs involved in community decisions to move school start times may be better informed and data driven.
DISCLOSURE STATEMENT
This was not an industry supported study. Funding for this project was provided by the American Academy of Sleep Medicine and Sleep Research Society, and by cooperative agreement 1U50DP004930-01 from the Centers for Disease Control and Prevention (CDC). The findings and conclusions in this report are those of the authors and do not necessarily represent the official views of the CDC. The authors have indicated no financial conflicts of interest. Ms. Hashmi and Mr. Heald are both employed by the American Academy of Sleep Medicine.
REFERENCES
- 1.Centers for Disease Control and Prevention. National Healthy Sleep Awareness Project. 2014 [cited 15 August 2016]; Available from: http://www.sleepeducation.org/healthysleep/about-the-national-healthy-sleep-awareness-project/
- 2.Centers for Disease Control and Prevention. Healthy People 2020. August 12 2016 [cited 2016 August 15]; Available from: http://www.healthypeople.gov/2020/topics-objectives/topic/sleep-health.
- 3.Wheaton AG, Olsen EO, Miller GF, Croft JB. Sleep duration and injury-related risk behaviors among high school students - United States, 2007-2013. MMWR Morb Mortal Wkly Rep. 2016;65:337–41. doi: 10.15585/mmwr.mm6513a1. [DOI] [PubMed] [Google Scholar]
- 4.Matricciani L, Olds T, Petkov J. In search of lost sleep: secular trends in the sleep time of school-aged children and adolescents. Sleep Med Rev. 2012;16:203–11. doi: 10.1016/j.smrv.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 5.Wheaton AG, Chapman DP, Croft JB. School start times, sleep, behavioral, health, and academic outcomes: a review of the literature. J School Health. 2016;86:363–81. doi: 10.1111/josh.12388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Centers for Disease Control and Prevention. Results from the School Health Policies and Practices Study 2014. 2015 [cited 2016 15 August]; Available from: http://www.cdc.gov/healthyyouth/data/shpps/pdf/shpps-508-final_101315.pdf.
- 7.Wheaton AG, Ferro GA, Croft JB. School start times for middle school and high school students--United States, 2011-12 school year. MMWR Morb Mortal Wkly Rep. 2015;64:809–13. doi: 10.15585/mmwr.mm6430a1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Carskadon MA, Wolfson AR, Acebo C, Tzischinsky O, Seifer R. Adolescent sleep patterns, circadian timing, and sleepiness at a transition to early school days. Sleep. 1998;21:871–81. doi: 10.1093/sleep/21.8.871. [DOI] [PubMed] [Google Scholar]
- 9.Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med. 2007;8:602–12. doi: 10.1016/j.sleep.2006.12.002. [DOI] [PubMed] [Google Scholar]
- 10.Cain N, Gradisar M. Electronic media use and sleep in school-aged children and adolescents: a review. Sleep Med. 2010;11:735–42. doi: 10.1016/j.sleep.2010.02.006. [DOI] [PubMed] [Google Scholar]
- 11.Knutson KL, Lauderdale DS. Sociodemographic and behavioral predictors of bed time and wake time among US adolescents aged 15 to 17 years. J Pediatr. 2009;154:426–30. doi: 10.1016/j.jpeds.2008.08.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lee JA, Park HS. Relation between sleep duration, overweight, and metabolic syndrome in Korean adolescents. Nutr Metab Cardiovasc Dis. 2014;24:65–71. doi: 10.1016/j.numecd.2013.06.004. [DOI] [PubMed] [Google Scholar]
- 13.Mitchell JA, Rodriguez D, Schmitz KH, Audrain-McGovern J. Sleep duration and adolescent obesity. Pediatrics. 2013;131:e1428–34. doi: 10.1542/peds.2012-2368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Au CT, Ho CK, Wing YK, Lam HS, Li AM. Acute and chronic effects of sleep duration on blood pressure. Pediatrics. 2014;133:e64–72. doi: 10.1542/peds.2013-1379. [DOI] [PubMed] [Google Scholar]
- 15.Azadbakht L, Kelishadi R, Khodarahmi M, et al. The association of sleep duration and cardiometabolic risk factors in a national sample of children and adolescents: the CASPIAN III study. Nutrition. 2013;29:1133–41. doi: 10.1016/j.nut.2013.03.006. [DOI] [PubMed] [Google Scholar]
- 16.Meininger JC, Gallagher MR, Eissa MA, Nguyen TQ, Chan W. Sleep duration and its association with ambulatory blood pressure in a school-based, diverse sample of adolescents. Am J Hypertens. 2014;27:948–55. doi: 10.1093/ajh/hpt297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Danner F, Phillips B. Adolescent sleep, school start times, and teen motor vehicle crashes. J Clin Sleep Med. 2008;4:533–5. [PMC free article] [PubMed] [Google Scholar]
- 18.Vorona RD, Szklo-Coxe M, Lamichhane R, Ware JC, McNallen A, Leszczyszyn D. Adolescent crash rates and school start times in two central Virginia counties, 2009-2011: a follow-up study to a southeastern Virginia study, 2007-2008. J Clin Sleep Med. 2014;10:1169–77. doi: 10.5664/jcsm.4192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vorona RD, Szklo-Coxe M, Wu A, Dubik M, Zhao Y, Ware JC. Dissimilar teen crash rates in two neighboring southeastern Virginia cities with different high school start times. J Clin Sleep Med. 2011;7:145–51. [PMC free article] [PubMed] [Google Scholar]
- 20.Owens JA, Belon K, Moss P. Impact of delaying school start time on adolescent sleep, mood, and behavior. Arch Pediatr Adolesc Med. 2010;164:608–14. doi: 10.1001/archpediatrics.2010.96. [DOI] [PubMed] [Google Scholar]
- 21.Perkinson-Gloor N, Lemola S, Grob A. Sleep duration, positive attitude toward life, and academic achievement: the role of daytime tiredness, behavioral persistence, and school start times. J Adolesc. 2013;36:311–8. doi: 10.1016/j.adolescence.2012.11.008. [DOI] [PubMed] [Google Scholar]
- 22.Shochat T, Cohen-Zion M, Tzischinsky O. Functional consequences of inadequate sleep in adolescents: a systematic review. Sleep Med Rev. 2014;18:75–87. doi: 10.1016/j.smrv.2013.03.005. [DOI] [PubMed] [Google Scholar]
- 23.Winsler A, Deutsch A, Vorona RD, Payne PA, Szklo-Coxe M. Sleepless in Fairfax: the difference one more hour of sleep can make for teen hopelessness, suicidal ideation, and substance use. J Youth Adolesc. 2015;44:362–78. doi: 10.1007/s10964-014-0170-3. [DOI] [PubMed] [Google Scholar]
- 24.Wolfson AR, Spaulding NL, Dandrow C, Baroni EM. Middle school start times: the importance of a good night's sleep for young adolescents. Behav Sleep Med. 2007;5:194–209. doi: 10.1080/15402000701263809. [DOI] [PubMed] [Google Scholar]
- 25.Asarnow LD, McGlinchey E, Harvey AG. The effects of bedtime and sleep duration on academic and emotional outcomes in a nationally representative sample of adolescents. J Adolesc Health. 2014;54:350–6. doi: 10.1016/j.jadohealth.2013.09.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ming X, Koransky R, Kang V, Buchman S, Sarris CE, Wagner GC. Sleep insufficiency, sleep health problems and performance in high school students. Clinical medicine insights. Circ Respir Pulm Med. 2011;5:71–9. doi: 10.4137/CCRPM.S7955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Adolescent Sleep Working GCoACoS, Health. School start times for adolescents. Pediatrics. 2014;134:642–9. doi: 10.1542/peds.2014-1697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dexter D, Bijwadia J, Schilling D, Applebaugh G. Sleep, sleepiness and school start times: a preliminary study. Wisc Med J. 2003;102:44–6. [PubMed] [Google Scholar]
- 29.Eliasson A, Eliasson A, King J, Gould B, Eliasson A. Association of sleep and academic performance. Sleep Breath. 2002;6:45–8. doi: 10.1007/s11325-002-0045-9. [DOI] [PubMed] [Google Scholar]
- 30.Orzech KM. A qualitative exploration of adolescent perceptions of healthy sleep in Tucson, Arizona, USA. Soc Sci Med. 2013;79:109–16. doi: 10.1016/j.socscimed.2012.05.001. [DOI] [PubMed] [Google Scholar]
- 31.Paksarian D, Rudolph KE, He JP, Merikangas KR. School start time and adolescent sleep patterns: results from the U.S. National Comorbidity Survey--Adolescent Supplement. Am J Public Health. 2015;105:1351–7. doi: 10.2105/AJPH.2015.302619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Short MA, Gradisar M, Lack LC, et al. A cross-cultural comparison of sleep duration between US And Australian adolescents: the effect of school start time, parent-set bedtimes, and extracurricular load. Health Educ Behav. 2013;40:323–30. doi: 10.1177/1090198112451266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Boergers J, Gable CJ, Owens JA. Later school start time is associated with improved sleep and daytime functioning in adolescents. J Devel Behav Pediatr. 2014;35:11–7. doi: 10.1097/DBP.0000000000000018. [DOI] [PubMed] [Google Scholar]
- 34.Thacher PV, Onyper SV. Longitudinal outcomes of start time delay on sleep, behavior, and achievement in high school. Sleep. 2016;39:271–81. doi: 10.5665/sleep.5426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Vedaa Ø, Saxvig IW, Wilhelmsen-Langeland A, Bjorvatn B, Pallesen S. School start time, sleepiness and functioning in Norwegian adolescents. Scand J Educ Res. 2012;56:55–67. [Google Scholar]
- 36.Borlase BJ, Gander PH, Gibson RH. Effects of school start times and technology use on teenagers' sleep: 1999-2008. Sleep Biol Rhythms. 2013;11:46–54. [Google Scholar]
- 37.Minges KE, Redeker NS. Delayed school start times and adolescent sleep: a systematic review of the experimental evidence. Sleep Med Rev. 2016;28:86–95. doi: 10.1016/j.smrv.2015.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Owens J, Drobnich D, Baylor A, Lewin D. School start time change: an in-depth examination of school districts in the United States. Mind Brain Educ. 2014;8:182–213. [Google Scholar]
- 39.Chang AM, Aeschbach D, Duffy JF, Czeisler CA. Evening use of light-emitting eReaders negatively affects sleep, circadian timing, and next-morning alertness. Proc Natl Acad Sci U S A. 2015;112:1232–7. doi: 10.1073/pnas.1418490112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.van der Lely S, Frey S, Garbazza C, et al. Blue blocker glasses as a countermeasure for alerting effects of evening light-emitting diode screen exposure in male teenagers. J Adoles Health. 2015;56:113–9. doi: 10.1016/j.jadohealth.2014.08.002. [DOI] [PubMed] [Google Scholar]
- 41.Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation's sleep time duration recommendations: methodology and results summary. Sleep Health. 2015;1:40–3. doi: 10.1016/j.sleh.2014.12.010. [DOI] [PubMed] [Google Scholar]
- 42.Mukherjee S, Patel SR, Kales SN, et al. An official American Thoracic Society statement: the importance of healthy sleep. Recommendations and future priorities. Am J Respir Crit Care Med. 2015;191:1450–8. doi: 10.1164/rccm.201504-0767ST. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Paruthi S, Brooks LJ, D'Ambrosio C, et al. Recommended amount of sleep for pediatric populations: a consensus statement of the American Academy of Sleep Medicine. J Clin Sleep Med. 2016;12:785–6. doi: 10.5664/jcsm.5866. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Centers for Disease Control and Prevention. School Health Policies and Practices Study (SHPPS) 2014 March 11, 2016 [cited 2016 15 August]; Available from: http://www.cdc.gov/healthyyouth/data/shpps/pdf/shpps-508-final_101315.pdf.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.