

Abstract
Background:
Thyroid nodule is one of the most common endocrinopathies occurring children and adolescents. Though thyroid nodule is rare in the pediatric age group, the rate of malignancy is much higher in this age group compared to adult population.
Aim:
The objective is to study the application of The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) in pediatric patients and compare the findings with histology.
Materials and Methods:
A total of 218 cases younger than 18 years were studied in a 4-year period from August 2010 to July 2014. The smears were categorized according to TBSRTC into six categories — Nondiagnostic, benign, atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS), suspicious for follicular neoplasm (SFN), suspicious for malignancy (SM), and malignancy.
Results:
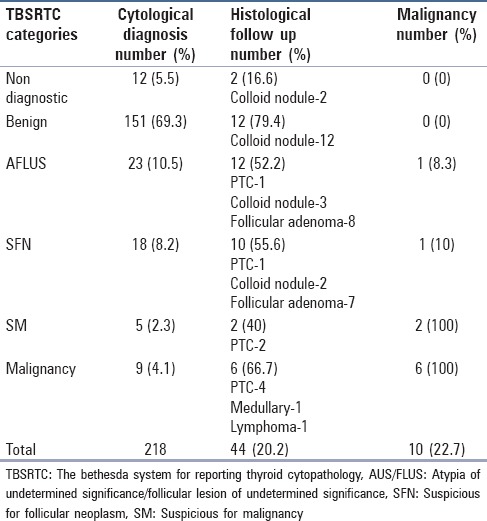
Out of 218 cases, 33 were males and 185 were females. Histological follow-up was available in 44 cases. The diagnosis according to TBSRTC included 12 (5.5%) nondiagnostic, 151 (69.26%) benign, 23 (10.5%) AUS/FLUS, 18 (8.2%) SFN, 5 (2.3%) SM, and 9 (4.1%) malignancy cases. On histological follow-up, the rate of malignancy in each category was 0%, 0%, 8.3%, 10% 100%, and 100%, respectively.
Conclusion:
The study demonstrates that TBSRTC in pediatric thyroid nodule is as sensitive and specific as in adults, especially with 100% accuracy in the diagnosis of benign and malignant categories.
Keywords: Cytopathology, the Bethesda System, thyroid nodule
Introduction
Thyroid swellings are uncommon in the pediatric age group and the reported incidence, in the age group of 8-18 years, is estimated to be 0.05-1.8%, and in adult population the reported incidence ranges between 3.2% and 8%.[1,2] But the risk of malignancy in children varies widely, ranging from 5% to 50%, in the different studies, and in adults it varies from 5% to 15%.[3,4,5]
In adults, the role of fine-needle aspiration cytology (FNAC) has been well established and FNAC can be effectively used for the diagnosis and management of thyroid swelling with a high degree of reliability.[6,7] The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) provides relatively accurate reporting system for FNAC of thyroid and it is the most accurate method suggested by American Thyroid Association.[8]
Most studies have applied this system for adult thyroid cytology reporting.[9,10] Only a very few studies have analyzed TBSRTC for reporting pediatric thyroid nodule.[11,12,13,14] However, most of these studies applying TBSRTC were based on the data from adult population and there were no distinct and specified guidelines for the evaluation of thyroid cytology in pediatric thyroid swellings. So, this study aims to evaluate the usefulness of TBSRTC in pediatric patients and to correlate the findings with histology.
TBSRTC describes a six-tier system for uniform reporting of thyroid nodules and also helps develop a standardized management plan and propose treatment guidelines.
Materials and Methods
During a period of 4 years, from August 2010 to July 2014, a total of 218 pediatric patients with thyroid swelling were studied. Their clinical data, radiological data, serum testing for hormone studies, cytological diagnosis, and histological diagnosis were reviewed.
Aspiration was performed by a 23-gauze needle attached to a disposable 10 mL or 20 mL syringe with or without a syringe holder. The small nodules were aspirated under ultrasonologic guidance and the aspirated material was smeared onto the slides. Half of the slides were air-dried and stained with May-Grünwald-Giemsa (MGG) stain and others were fixed with 95% alcohol and stained with hematoxylin and eosin and Papanicoalaou (PAP) stains, and these cases were reviewed by two cytopathologists.
The smears were categorized according to TBSRTC into the following six categories:
Nondiagnostic.
Benign.
Atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS).
Suspicious for follicular neoplasm (SFN).
Suspicious for malignancy (SM).
Malignancy.
Histological follow-up was available in 44 cases and based on clinical, radiological, cytological, and histological findings, all the data were tabulated and analyzed in a systemic manner to know the sensitivity and specificity of FNAC in different categories of TBSRTC.
Results
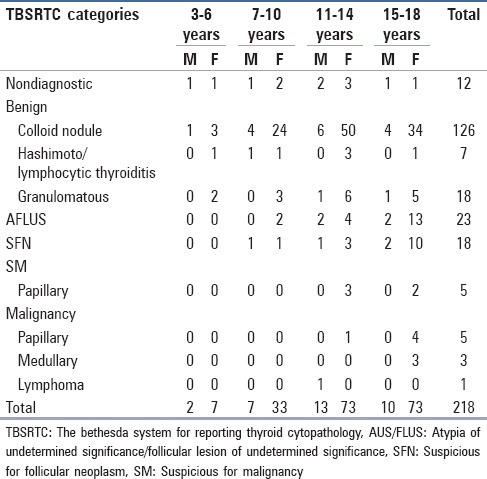
A total of 218 cases were studied out of which 33 (15%) were males and 185 (85%) were females [Table 1]. Overall, the thyroid nodules were more prevalent in the adolescent age group (11-14 years) [Table 2].
Table 1.
Categorization of lesion according to TBSRTC and their distribution according to sex
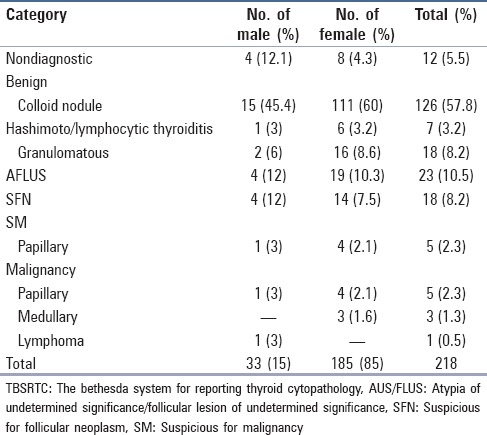
Table 2.
Distribution of lesions in different age groups
Out of total 151 cases negative for malignant category the most common diagnosis was benign colloid nodule (126 cases) and histological follow up was available in 12 cases and in all the cases the histological diagnosis was consistent with the cytological diagnosis with 100% sensitivity and specificity of FNAC in benign cases. Out of the 23 cases of AFLUS category, the histological follow-up was available in 12 cases with 3 cases proved to be colloid nodule and 8 cases proved to be follicular adenoma and one 1 was found to be papillary carcinoma of thyroid. Out of 18 cases of the SFN category, histological follow-up was available in 10 cases out of which only 2 cases turned out to be colloid nodule, 7 were follicular adenoma, and 1 was papillary carcinoma. All the FNACs with a diagnosis of suspicious or positive for malignancy were found to be malignant on histological follow-up with 100% sensitivity and specificity [Table 3].
Table 3.
Correlation of cytological and histopathological findings
Discussion
TBSRTC is a unique internationally accepted reporting system for cytology of thyroid nodule and several studies have shown the utility of this system in FNAC of adult thyroid nodule but only a few studies have applied this system for reporting of pediatric thyroid nodule.[11,12,13,14] This study analyzed the utility of the six-tier system for reporting of pediatric thyroid nodule and showed that TBSRTC can be applied for the diagnosis of thyroid nodule in children as effectively as in adults. Thyroid nodules in children are less common as compared to that in adults but have an increased risk of malignancy as compared to adult thyroid nodule.[3,4,5] The rate of malignancy in surgically resected pediatric patient was 22.7% in our study, and the results of our study are in concordance with other studies examining surgically resected nodules in children and adults.[3,14,15,16]
Out of a total 218 cases, 12 cases (5.5%) were nondiagnostic, and the uncooperative child patient leading to inadequate or poor-quality and insufficient-quantity aspirate can be the explanation for this. Out of the 218 cases, 151 cases were benign, and colloid nodule was the commonest benign lesion. Lymphocytic and granulomatous thyroiditis were other benign lesions and these lesions are common in female in the age group of 11-14 years. Histological follow-up was available in 12 cases cytologically diagnosed as benign thyroid nodule, and all cases were confirmed to be benign thyroid nodule on histological follow-up, so the sensitivity and specificity of TBSRTC were 100% in this study.
AFLUS, SFN, and SM categories of TBSRTC are often included under the intermediate category lesions.[7] Intermediate thyroid lesions are a heterogeneous group that do not fit into either frank benign or malignant category and this is the group where the real application of the TBSRTC is needed. In the present study, this group comprise 21.1% (46 cases) of total pediatric nodule and histological follow-up was available in 24 cases out of which 4 cases (16.6%) were proved to be malignant, and the study demonstrates that the rate of malignancy in this category was high than that seen in adults.[9] This can be explained as often cytologists are overcautious to diagnose frank malignancy in young patients.
In the present study, the rate of malignancy diagnosed by TBSRTC was 4.1% (9 cases), and 6 cases were confirmed on histological follow-up. The papillary carcinoma of thyroid form the major proportion and the sensitivity and specificity of TBSRTC in diagnosis of malignancy was 100% and the results are similar to those of the previous studies.[13,14]
So overall in our experience, TBSRTC can be effectively applied to pediatric thyroid nodule and this six-tier categorization correlates with an increased risk of malignancy, especially in the intermediate category, leading to a more consistent management approach and the increased risk of malignancy in this category reflects the importance of TBSRTC.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Huang SA. Thyromegaly. In: Lifshitz, editor. Pediatric Endocrinology. 5th ed. New York: Informa Healthcare; 2007. pp. 443–53. [Google Scholar]
- 2.Huang SA, Brown RS. The thyroid and its disorder. In: Brook C, Clayton P, Brown R, editors. Clinical Pediatric Endocrinology. 5th ed. USA: Blackwell; 2005. pp. 218–253. [Google Scholar]
- 3.Niedziela M. Pathogenesis, diagnosis and management of thyroid nodules in children. Endocr Relat Cancer. 2006;13:427–53. doi: 10.1677/erc.1.00882. [DOI] [PubMed] [Google Scholar]
- 4.Al-Shaikh A, Ngan B, Daneman A, Daneman D. Fine-needle aspiration biopsy in the management of thyroid nodules in children and adolescents. J Pediatr. 2001;138:140–2. doi: 10.1067/mpd.2001.109609. [DOI] [PubMed] [Google Scholar]
- 5.Belfiore A, Giuffrida D, La Rosa GL, Ippolito O, Russo G, Fiumara A, et al. High frequency of cancer in cold thyroid nodules occurring at young age. Acta Endocrinol (Copenh) 1989;121:197–202. doi: 10.1530/acta.0.1210197. [DOI] [PubMed] [Google Scholar]
- 6.Baloch ZW, LiVolsi VA, Asa SL, Rosai J, Merino MJ, Randolph G, et al. Diagnostic terminology and morphologic criteria for cytologic diagnosis of thyroid lesions: A synopsis of the National Cancer Institute Thyroid Fine-Needle Aspiration State of the Science Conference. Diagn Cytopathol. 2008;36:425–37. doi: 10.1002/dc.20830. [DOI] [PubMed] [Google Scholar]
- 7.Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid Cytopathology. Thyroid. 2009;19:1159–65. doi: 10.1089/thy.2009.0274. [DOI] [PubMed] [Google Scholar]
- 8.Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Revised American Thyroid Association (ATA) Guidelines for patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2009;19:1167–214. doi: 10.1089/thy.2009.0110. [DOI] [PubMed] [Google Scholar]
- 9.Bongiovanni M, Krane JF, Cibas ES, Faquin WC. The atypical thyroid fine-needle aspiration: Past, present, and future. Cancer Cytopathol. 2012;120:73–86. doi: 10.1002/cncy.20178. [DOI] [PubMed] [Google Scholar]
- 10.Faquin WC, Baloch ZW. Fine-needle aspiration of follicular patterned lesions of the thyroid: Diagnosis, management, and follow-up according to National Cancer Institute (NCI) recommendations. Diagn Cytopathol. 2010;38:731–9. doi: 10.1002/dc.21292. [DOI] [PubMed] [Google Scholar]
- 11.Hoperia V, Larin A, Jensen K, Bauer A, Vasko V. Thyroid fine needle aspiration biopsies in children: Study of cytological-histological correlation and immunostaining with thyroid peroxidase monoclonal antibodies. Int J Pediatr Endocrinol 2010. 2010 doi: 10.1155/2010/690108. 690108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bargren AE, Meyer-Rochow GY, Sywak MS, Delbridge LW, Chen H, Sidhu SB. Diagnostic utility of fine-needle aspiration cytology in pediatric differentiated thyroid cancer. World J Surg. 2010;34:1254–60. doi: 10.1007/s00268-010-0391-x. [DOI] [PubMed] [Google Scholar]
- 13.Gupta A, Ly S, Castroneves LA, Frates MC, Benson CB, Feldman HA, et al. A standardized assessment of thyroid nodules in children confirms higher cancer prevalence than in adults. J Clin Endocrinol Metab. 2013;98:3238–45. doi: 10.1210/jc.2013-1796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Monaco SE, Pantanowitz L, Khalbuss WE, Benkovich VA, Ozolek J, Nikiforova MN, et al. Cytomorphological and molecular genetic findings in pediatric thyroid fine-needle aspiration. Cancer Cytopathol. 2012;120:342–50. doi: 10.1002/cncy.21199. [DOI] [PubMed] [Google Scholar]
- 15.Scholz S, Smith JR, Chaignaud B, Shamberger RC, Huang SA. Thyroid surgery at Children's Hospital Boston: A 35-year single-institution experience. J Pediatr Surg. 2011;46:437–42. doi: 10.1016/j.jpedsurg.2010.09.009. [DOI] [PubMed] [Google Scholar]
- 16.Singh RS, Wang HH. Eliminating the “atypia of undetermined significance/follicular lesion of undetermined significance” category from the Bethesda System for Reporting Thyroid Cytopathology. Am J Clin Pathol. 2011;136:896–902. doi: 10.1309/AJCPIX52MBOKTICP. [DOI] [PubMed] [Google Scholar]