

Abstract
Hepatocellular carcinoma (HCC) the most common primary tumor of the liver usually develops in the setting of chronic liver disease. The presentation is usually due to worsening of chronic liver disease or being detected incidentally on imaging. Rarely metastasis to distant organ becomes the presentation. The authors describe a case of a 70-year-old woman who presented with dyspnea of 2 weeks duration. She was diagnosed as having HCC and extensive multiple pulmonary metastases. She was symptomatic only for the pulmonary metastasis with only 2 lesions in the liver. Because of advanced nature of disease, no specific therapy for the tumor was possible.
Abbreviations: HCC, hepatocellular carcinoma; HIV, human immunodeficiency virus
Keywords: HCC, hepatocellular carcinoma, lung metastases, dyspnea
Introduction
We report a case of hepatocellular carcinoma (HCC) presenting as severe dyspnea secondary to extensive pulmonary metastasis.
Case report
A 70-year-old Indian diabetic female without any previous history suggestive of liver disease presented to our outpatient department with complaint of dyspnea of two weeks duration. She was initially treated by the pulmonologist and the cardiologist in view of her presentation being severe dyspnea. She had a reduced oxygen saturation of 90%. She did not have any history of fever or cough. There was no history of alcohol consumption or smoking. The patient underwent a complete workup. Her laboratory tests showed a hemoglobin level of 12.8 g/dl, total leukocyte count of 5960/μl, platelet count of 252,000/μl, serum creatinine of 0.7 mg/dl. Her liver function tests were within normal range. Her 2D bubble echocardiography was non-contributory with no feature of any motion wall abnormality, pulmonary hypertension or hepatopulmonary shunt. Her chest X-ray showed multiple opacities. Ultrasound abdomen done showed 2 lesions in the liver. A dynamic CT of abdomen and chest was performed, which demonstrated the 2 liver lesions (segment 6, 7 and caudate lobe shown by arrows in Figure 1, Figure 2, larger measuring 5.7 cm × 4.4 cm) with hypervascularity in arterial phase (Figure 1) and washout in portal phase (Figure 2). In addition to liver lesions there were numerous lung lesions suggestive of metastasis (Figure 3, Figure 4). The rest of the liver parenchyma was non-cirrhotic and there were no features of portal hypertension or ascites. She had an elevated alpha feto-protein level of 21,700 IU/ml. Her workup was negative for hepatitis B, hepatitis C and human immunodeficiency virus (HIV). In view of the advanced disease only treatment possible was palliation and end of life care. She was put on domiciliary oxygen in view of her dyspnea. The patient succumbed to her illness after 2 weeks of presentation.
Figure 1.
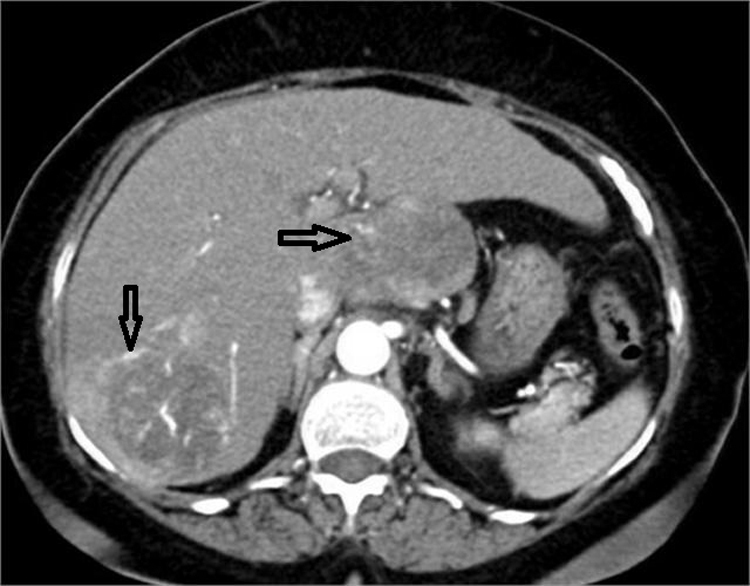
Arterial phase CT showing enhancement of 2 hepatic lesions.
Figure 2.
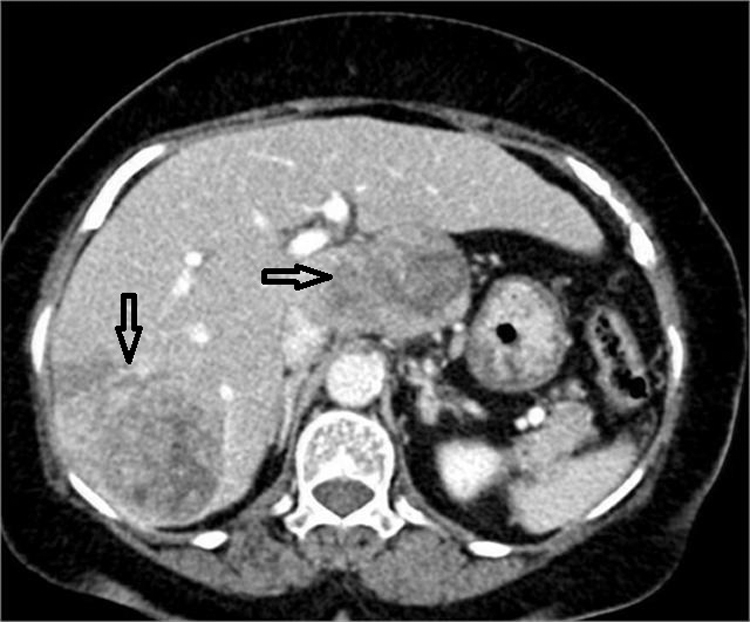
Portal venous phase CT showing washout of similar lesions as seen in Figure 1.
Figure 3.
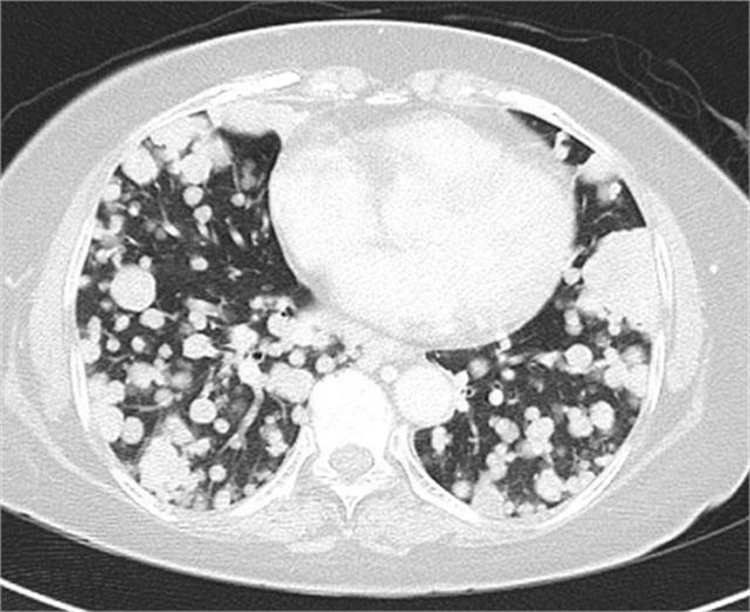
Axial chest image showing numerous metastatic lesions.
Figure 4.
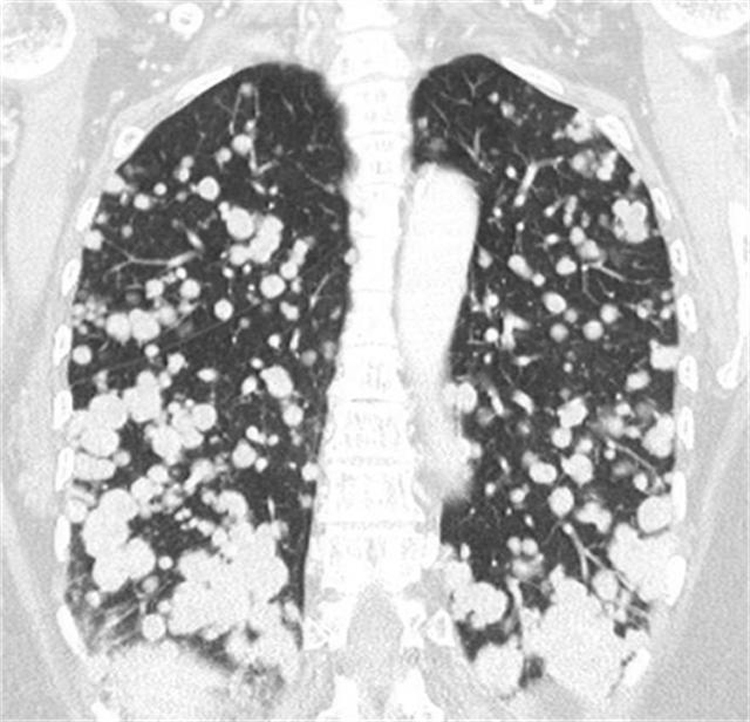
Coronal chest image showing numerous metastatic lesion.
Discussion
Major risk factors for HCC include infection with hepatitis B, hepatitis C, alcoholic liver disease, and non-alcoholic fatty liver disease.1, 2 HCC generally occurs in setting of cirrhosis and clinical features of cirrhosis are more common than symptoms due to HCC. Non-alcoholic steatohepatitis can lead to HCC without development of cirrhosis2 that was probable cause of HCC in present case as patient has diabetes. Metastases are most commonly intra-hepatic but lungs are main site of extrahepatic spread, followed by regional and distant lymph nodes, musculoskeletal system, adrenal glands, kidneys and bone marrow.3 Dyspnea as initial presentation of HCC is extremely rare. Shuangshoti S reported a case of 39-year-old women having progressive dyspnea as clinical presentation of HCC.4 Apart from extensive metastasis, dyspnea may also occur secondary to microemboli from HCC.5
Summary
We describe an extremely unusual presentation of HCC in a non-cirrhotic elderly patient, dyspnea at rest as initial manifestation due to innumerable pulmonary metastatic lesions.
Conflicts of interest
The authors have none to declare.
References
- 1.El-Serag H.B. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology. 2012;142:1264–1273. doi: 10.1053/j.gastro.2011.12.061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Torres D.M., Harrison S.A. Nonalcoholic steatohepatitis and noncirrhotic hepatocellular carcinoma: fertile soil. Semin Liver Dis. 2012;32:30–38. doi: 10.1055/s-0032-1306424. [DOI] [PubMed] [Google Scholar]
- 3.Trevisani F., Intino D., Caraceni P.E. Etiologic factors and clinical presentation of hepatocellular carcinoma, differences between cirrhotic and non cirrhotic Italian patients. Cancer. 1995;75:2220–2232. doi: 10.1002/1097-0142(19950501)75:9<2220::aid-cncr2820750906>3.0.co;2-4. [DOI] [PubMed] [Google Scholar]
- 4.Shuangshoti S. Hepatocellular carcinoma having progressive dyspnea as clinical presentation. J Med Assoc Thai. 1996;79:744–748. [PubMed] [Google Scholar]
- 5.Tanaka K., Nakasaya A., Miyazaki M. A case of hepatocellular carcinoma with respiratory failure caused by widespread tumor microemboli. Fukuoka Igaku Zasshi. 2011;102:298–302. [PubMed] [Google Scholar]