

Abstract
Introduction
The cardiopulmonary exercise test (CPET) assesses maximal oxygen uptake (VO2max) and is commonly performed on a leg cycle ergometer (LC). However, some individuals would rather perform the CPET on an arm cycle ergometer (AC).
Objective
The objectives of this study were to undertake a systematic review and meta-analysis of the difference in VO2max achieved by AC compared to LC in healthy adults and to explore factors that may be predictive of this difference.
Methods
MEDLINE, EMBASE, CINAHL, and PEDro were searched in April 2015. The differences in VO2max (ACLCdiff) were pooled across studies using random effects meta-analysis and three different methods were used to estimate the ratio between the values obtained from the tests (ACLCratio).
Results
This paper included 41 studies with a total of 581 participants. The mean ACLCdiff across studies was 12.5 ml/kg/min and 0.89 l/min with a mean ACLCratio of 0.70. The ACLCdiff was lower in studies with higher mean age and lower aerobic capacity.
Conclusion
There is linear association between the AC and LC values in healthy adults. The AC values were on average 70% of the LC values. The magnitude of this difference appeared to be reduced in studies on older and less active populations.
Level of evidence
3a
Keywords: Aerobic capacity, exercise testing, oxygen uptake, leg cycle, arm cycle, ergometer, systematic review, meta-analysis
INTRODUCTION
The cardiopulmonary exercise test (CPET) is the gold standard for the direct assessment of maximal oxygen uptake (VO2max).1-5 VO2max determines the maximal ability for the human body to deliver, obtain and consume oxygen during maximal exercise and is a measure of maximum aerobic capacity.4 Assessments of aerobic capacity are used by healthcare professionals to evaluate exercise capacity,5 exercise intolerance6 and functional aerobic impairment,7 which all provide important information on health status and prognosis in various populations.2,8-11
CPET is commonly performed on a treadmill or on a leg cycle ergometer (LC).3,5 However, due to disability, co-morbidity, preference or athletic discipline there is a need to investigate alternatives to the LC test.12 In some cases, it could be more important to assess aerobic fitness using the arms when leg exercise is not feasible or possible.13-15 A potential alternative is to perform the test with the upper body using an arm cycle ergometer (AC).13 However, the AC has limitations as studies have shown that untrained individuals will achieve a lower level of VO2max on the AC, due to a reduced stress on the cardiovascular system, compared to the LC test.12,15,16 Having a smaller amount of muscle mass being active during the test, AC is likely to result in an earlier termination of the CPET due to peripheral factors such as an earlier onset of lactate threshold, rather than central cardiovascular limitations.12,17 While individual studies have directly assessed the difference in VO2max of a CPET conducted using AC compared to LC in healthy adults, no previous systematic review of these studies has been published.
The objectives of this study were to undertake a systematic review and meta-analysis of the difference in VO2max achieved by AC compared to LC in healthy adults and to explore factors that may be predictive of this difference. The determination of this factor would allow the direct comparison of data obtained on the two tests.
METHODS
This review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.18
DATA SOURCES AND SEARCHES
Preliminary searches were conducted and relevant search terms identified. A formal search of the databases MEDLINE, EMBASE, CINAHL, and PEDro was undertaken in April 2015. References of the identified studies in the preliminary searches were screened and relevant search terms were added to the search strategy. The search strategy consisted of a combination of relevant keywords and MeSH/Thesaurus terms for: 1) direct assessment of VO2max (or VO2peak), 2) a CPET performed on an AC and 3) a CPET performed on an LC. No language or publication limits were applied. The reference lists of identified studies were checked and the authors of unobtainable studies were contacted. Papers suggested by experts in the field were evaluated. Search strategies specified for MEDLINE are presented in Appendix 1.
STUDY SELECTION
Study selection was undertaken based on a priori defined criteria. Only original research papers reporting within comparison (AC and LC) VO2max (or VO2peak), as milliliter oxygen per kilogram per minute (ml/min/kg) or as liters per minute (l/min), were considered eligible for inclusion in this systematic review. The CPET had to be non-assisted on AC and LC. Studies that reported values for healthy adults (age > 18 years) with a level of physical activity < 300 minutes per week were included. People with higher physical activity levels were considered athletes and where therefore excluded.19
Two authors (RTL, CK) independently screened titles and abstracts and assessed eligible articles in full-text. Any inconsistencies between authors were discussed and disagreement was solved by consultation with a third author (JC).
DATA EXTRACTION AND RISK OF BIAS ASSESSMENT
The following information was extracted: sample size, gender distribution, mean age, mean height, body mass index (BMI) together with the VO2max values, peak respiratory exchange ratio (RER), CPET starting watt, and watt increment for both the AC and LC test.
The Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (QAT)20 was used to assess the methodological quality of all included studies. Six items (6-10 and 13) were considered not applicable for the studies included in this review and thus did not contribute to the quality rating total score (SumQAT). Two authors (RTL and CK) independently extracted data and undertook the quality assessment. Inconsistencies between reviewers were discussed and in cases of disagreement, a third reviewer (JC) was consulted.
DATA ANALYSIS
The mean VO2max difference between the AC test and the LC test (ACLCdiff) was calculated for each study. Given the within subject nature of these comparisons the standard deviation (SD) of this difference for the within subject correlation was adjusted, using the method described in chapter 16.4.6.1 of the Cochrane Handbook.21 Hereby the SD was calculated using an imputed r-value of 0.5. The level of statistical heterogeneity was assessed using the I2 score. Given the variation of participant characteristics across included studies the ACLCdiff, for ml/kg/min and l/min, were pooled across studies using a random effects meta-analysis. Summary of the characteristics of included studies are expressed as median values and interquartile range (IQR).
Meta-regressions were used to perform sub-group analyses to clarify which variables were affecting the main analysis on the ACLCdiff. The sub-groups included were: aerobic capacity (as a categorical variable based on the Åstrand classification -“low”, “fair”, “average”, “good” or “high”),22 participant mean age (in years), gender (percentage of males), study risk of bias (SumQAT), and the difference in obtained peak RER values during test.
Three different approaches were used to find the ratio between AC and LC (ACLCratio). First a meta-analysis of the ACLCratio was undertaken using the studies presenting the group mean ± SD of the within comparison ratio (%). Second, a linear regression model was determined using the group mean values. The linear regression analysis was weighted by sample size. Third the reported AC values were divided with the reported LC values, giving an estimate of the ratio in each study, which are expressed as a total mean ratio.
All analyses were performed using Review Manager 5.3 (Cochrane collaboration) software and Stata 14.0 software (StataCorp. 2013. Stata Statistical Software: Release 14.9 College Station, TX: StataCorp LP). A p-value ≤ 0.05 was considered statistically significant.
RESULTS
Results of the search
The electronic searches identified 3,300 records. After removal of 617 duplicates, 2,683 unique studies remained. 2,510 studies were excluded by screening their title and abstract and 171 studies were considered eligible for full text review. Of these, 130 did not meet the inclusion criteria. Thus, 41 studies (published between 1973 and 2014) were included in the review.12,15,17,23-60 The study selection process is summarized as a flow chart in Figure 1.
Figure 1.

Flowchart illustrating the systematic literature search, screening of studies and full text assessment.
Description of studies
A summary of the characteristics of the 41 included studies is provided in Table 1. Some of the included studies reported results from several groups and the data extraction and risk of bias were therefore performed on 53 groups. The full details of included studies are listed in Appendix 2.
Table 1.
Study Characteristics of the 53 included groups
| Continent of publication | (%) |
|---|---|
| North America | 56.6 % |
| Europe | 35.8 % |
| South America | 3.8 % |
| Asia | 3.8 % |
| Study Design | |
|---|---|
| RCT | 17.0 % |
| Non-RCT | 3.8 % |
| Cross-sectional | 79.2 % |
| Study risk of bias | Median (IQR) |
|---|---|
| SumQAT | 4 points (3 to 5) |
| Participant characteristics | |
|---|---|
| Gender | (%) |
| Male only | 66 % |
| Female only | 15.1 % |
| Mixed | 15.1 % |
| Not reported | 3.8 % |
| Median (IQR) | |
|---|---|
| Mean age years | 28.4 years (25 to 32.3) |
| Mean BMI, kg/m2 | 23.65 kg/m2 (22.7 to 25) |
| Aerobic capacity | (%) |
|---|---|
| Low | 3.8 % |
| Average | 28.7 % |
| Good | 5.6 % |
| High | 3.8 % |
| Did not report | 58.1 % |
| Test characteristics | |
|---|---|
| Order on AC/LC test | (%) |
| AC first | 3.8 % |
| LC first | 18.9 % |
| Random order | 45.3 % |
| Not reported | 32 % |
| Median (IQR) | |
|---|---|
| Time between tests (hours) | 72 (24 to 168) |
| AC start level (watts) | 25 (15 to 40) |
| LC start levels (watts) | 50 (30 to 50) |
| AC increase/min (watt) | 10.7 (5 to 17) |
| LC increase/min (watt) | 30 (20.7 to 30) |
IQR: Interquartile range, SumQAT: sum of quality assessment tool score, AC: Arm cycle, LC: Leg cycle
Risk of bias in included studies
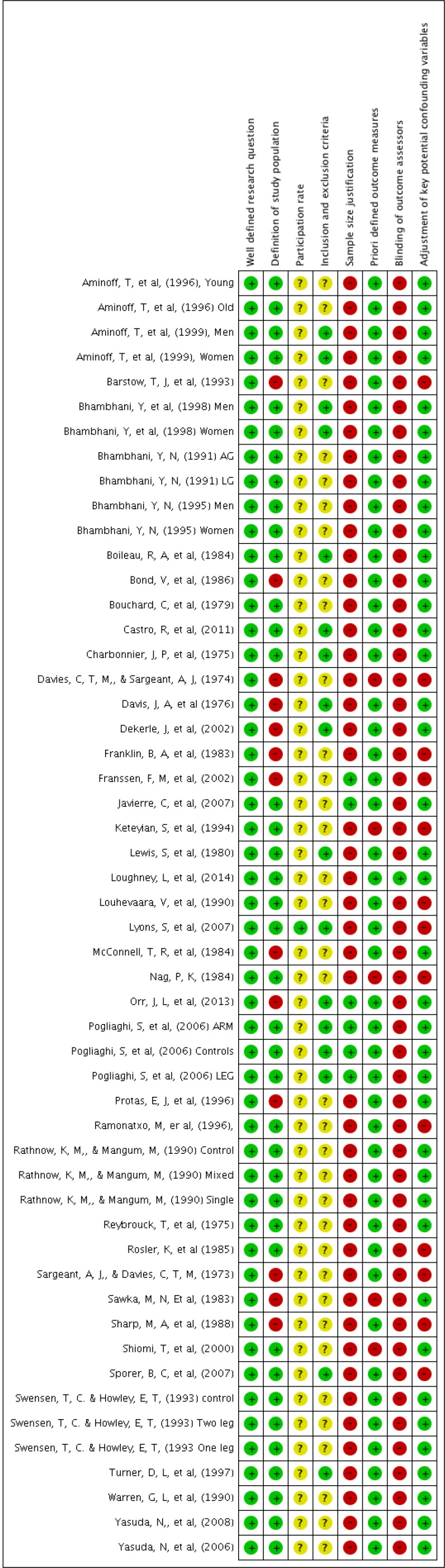
Figure 2 presents a summary of the risk of bias in the included groups. The median SumQAT was 4 points, (IQR: 3 to 5). A detailed risk of bias figure is presented in Appendix 3.
Figure 2.

Risk of bias graph. Review authors’ judgements about each risk of bias item presented as percentages across all included studies.
Research question and study population
Although all included groups were judged to have a well-defined research question (Item 1), 1315,17,25,30,34-38,44,47,52,53 had insufficient description of the population (Item 2). One group43 described the participation rate of eligible subjects (Item 3) and 13 15,24,26,29,32,33,35,36,41,43,46,55,57 had a well-defined description of the subject selection (Item 4). Four groups 15,38,39,46 included sample size justification (item 5).
Outcome measures
Five groups 17,34,40,45,53 did not report the VO2max as ml/kg/min but as l/min (item 11) and therefore did not adjust the outcome for subject weight.
Blinding and statistical analysis
One group12 blinded the outcome assessor (Item 12) and 1225,34,37,38,40,42,43,45,48,51,52,55 did not provide report a description of their statistical analysis methods (Item 14).
META-ANALYSIS OF VO2MAX DIFFERENCE BETWEEN AC AND LC
A total of 36 groups (413 participants) reported data for the ACLCdiff measured in ml/kg/min. The meta-analysis for the ACLCdiff is shown in Figure 3 with a pooled mean ACLCdiff of 12.5 ml/kg/min, (95% CI: 10.3 to 14.7, I2 = 59.9%, p > 0.001) favouring the LC test values. A total of 37 groups (415 participants) presented data of the ACLCdiff in l/min with a pooled mean ACLCdiff of 0.89 l/min, (95% CI: 0.78 to 1.00, I2 = 30.5%, p = 0.043) favouring the LC values as shown in Figure 4.
Figure 3.

Random effects meta-analysis of the difference between group means for arm cycle (AC) and leg cycle (LC) in ml/kg/min.
Figure 4.

Random effects meta-analysis of the difference between group means for arm cycle (AC) and leg cycle (LC) in l/min.
SUBGROUP ANALYSES
In univariate meta-regression and multivariate meta-regression lower participant mean age and higher aerobic capacity were found to be significantly associated to an increased ACLCdiff. The meta-regressions are shown in Table 2.
Table 2.
Meta-regression analyses performed on each variable (univariate) and adjusted for all variables (multivariate)
| Univariate meta-regression on ACLCdiff | Groups included in analysis | Mean coefficient (95% CI) | p-value |
|---|---|---|---|
| Aerobic capacity | 27 | 4.1 (95% CI: 1.5 to 6.6) | p = 0.003 |
| Gender distribution (% male) | 33 | −1.25 (95% CI: −7.4 to 4.9) | p = 0.684 |
| Mean age | 29 | −2.1 (95% CI: −0.3 to −0.1) | p<0.001 |
| Mean difference in peak RER values | 24 | −12.1 (95% CI: −68.8 to 44.6) | p = 0.663 |
| Risk of bias (SumQAT score) | 34 | −0.19 (95% CI: −2.6 to 2.2) | p = 0.875 |
| Multivariate meta-regression on ACLCdiff | |||
|---|---|---|---|
| Aerobic capacity | 16 | 4.0 (95% CI: 0.81 to 7.2) | p = 0.019 |
| Gender distribution (% male) | 16 | 4.5 (95% CI: −4.1 to 13.2) | p = 0.268 |
| Mean age (years) | 16 | −0.25 (95% CI: −0.4 to −0.06) | p = 0.014 |
| Mean difference in peak RER values | 16 | 7.9 (95% CI: −59.0 to 74.8) | p = 0.797 |
| Risk of bias (SumQAT score) | 16 | 0.9 (95% CI: −3.8 to 5.6) | p = 0.682 |
ACLCdiff: difference between obtained AC VO2max and obtained LC VO2max, 95% CI: 95% confidence intervals, RER: respiratory exchange ratio, SumQAT: sum of quality assessment tool score
ANALYSES OF THE AC/LC RATIO
The mean ratio between the AC test and the LC test for the 37 groups (n = 413 participants) reporting VO2max in ml/kg/min was 0.70 (95% CI: 0.66 to 0.73) in favour of the LC. The corresponding value of the 37 groups (n = 415 participants) reporting VO2max in l/min, the mean ACLCratio was 0.71 (95% CI: 0.66 to 0.75). The meta-analysis (n = 46 participants) for the ACLCratio across groups was 71%, (95% CI: 68 to 74, I2 = 0%, p = 0.530) (figure 5). The coefficient for the linear regression in Figure 6, between the AC and the LC mean VO2max was 0.65 ml/kg/min (95% CI: 0.48 to 0.81) with an r2 of 0.689.
Figure 5.

Random effects meta-analysis comparing studies that reports ratio values for the within person comparison between arm cycle (AC) and leg cycle (LC) as group mean ± SD.
Figure 6.

Two-way scatter plot and best fitted line between the mean arm cycle (AC) maximal oxygen uptake (VO2max) values and mean VO2max leg cycle (LC) values.
DISCUSSION
This systematic review and meta-analysis brings together data from 41 studies and 53 groups in 581 healthy individuals directly comparing VO2max values obtained from the AC compared to LC. The LC values were found to be substantively higher (mean difference: 12.5 ml/kg/min and 0.89 l/min) than the AC values. But with an I2 value of 59.9% for the ACLCdiff in ml/kg/min these results could be affected by substantial heterogeneity. The results support the belief that the AC test achieves lower oxygen uptake values as it involves a smaller amount of muscle mass and places less stress on the cardiovascular system.12,15,16
Both age and the aerobic capacity appear to be associated with the ACLCdiff. The difference is decreased with increasing age and increased with better aerobic capacity. This was expected, due to the fact that aerobic capacity decreases with age.22
The RER represents the relationship between the volume of carbon dioxide and the volume of oxygen in every breath and it is recommended to continue VO2max tests until RER values above 1.1 are reached in order to obtain a valid CPET.23 The majority of groups reporting RER values reported values in both tests to be above 1.1.23,24,26-29,32,36,38,46,60 Only one group reported RER values above 1.1 for the AC and below 1.1 for the LC,23 and three groups reported RER for both test to be below 1.1.33,39,49 The difference in the obtained RER values were expected to affect the ACLCdiff. However, this relationship was not found, which could be due to a lack of power, as not all included groups reported the values for the meta-regressions. The level of aerobic capacity is affected by gender.22 However, a correlation between gender distribution and the ACLCdiff was not found. This makes our results applicable for future research and clinical use in single gender groups as well as mixed gender groups.
The ACLCdiff does not seem to be affected by the risk of bias in the studies as low quality studies are reporting the same ACLCdiff as high quality studies. This may be explained by the precise and accurate equipment used during CPET,61 and thereby limits the possibility of imprecise testing in different settings, which increases the clinical applicability.
The most accurate estimate of the ratio is the meta-analysis of the reported ratios, but only four groups 33,39,46,54 reported mean ± SD (%) values for the ratio between the tests. The meta-analysis revealed a linear relationship between the AC test values and the LC test values with an ACLCratio of 0.7. This analysis should be seen as the main expression for the ratio between the values of the AC and the LC, where no important heterogeneity was found.62 Three different methods were used to estimate the ACLCratio. The calculation and the linear regression of the ACLCratio should only be used as a prediction, since they do not incorporate variation. Despite different approaches to estimate the ratio, the results are very similar and the ACLCratio of 0.7 is similar to the ones described in the literature.33,39,46,54 To investigate if the 0.7 is a valid estimate for the population mean ACLCratio, future research should report within comparison ratios between the AC and the LC, making them applicable for inclusion in meta-analysis.
This is the first systematic review and meta-analysis of the literature comparing arm and leg exercise, and it is thus important to stress that this paper has a number of limitations. First, some groups did not report ACLCdiff SD. Thus, imputation was performed of the value based on an assumed within participant correlation coefficient (r-value) between AC and LC VO2max. This method is recommended by the Cochrane Handbook21 but may still influence the accuracy of the findings. The only way to avoid these limitations in a meta-analysis is for future research to report the correlation coefficients between the two tests. However, sensitivity analyses were undertaken to assess the impact of this estimation on the findings. A small number of groups have reported a range of correlation coefficients between the AC test and the LC test (0.78, 0.94, 0.77, 0.32, 0.70).12,17,31,37,54 A sensitivity analysis was performed on the r-values and the pooled ACLCdiff was found to be 12.52 ml/kg/min (95% CI: 10.2 to 14.6) based on the lowest of the reported r-values (0.32) and 12.6 ml/kg/min (95% CI: 10.6 to 14.7) based on the highest reported r-value (0.94). Thus, it was shown that this imputation method made no difference to the pooled results. Future studies should report the standard deviation (or equivalent) of the mean difference between AC ad LC VO2max or the within person correlation coefficient.
Second, the quality of the included studies was variable. This review sought to assess study risk of bias using the QAT as it can be applied to cross-sectional studies.20 However, to make this tool relevant for this review some of the original QAT elements (items 6-10 and item 13) were dropped, as they were inapplicable to the research question. This could affect the reliability of the tool, and hereby the method of assessing the risk of bias, but the remaining items should be a good measure specific to the method of this paper.
Third, this review was limited to non-athlete healthy adults and limits generalizability of the current findings. Non-athlete healthy adults are expected to have a larger aerobic capacity when doing CPET using the legs compared to the arms due to everyday use and large lower limb muscle mass.29 However, in athletic populations, particularly arm-trained populations, the ACLCdiff is expected to be smaller than shown in this review.63 To avoid systematic bias, 18 comparisons in individuals performing more than 300 minutes per week of physical activity or involved in competitive exercise were excluded.19 Those groups contained ‘well trained subjects’, ‘triathletes’, ‘swimmers’, ‘cross-country skiers’ or ‘highly arm-trained’. However, no exclusion sedentary individuals was made. Two of the groups included extremely sedentary or sedentary subjects.39,47 But having an ACLCratio of 0.76 and 0.64 these groups are not likely to have had a systematic affect on the final results. A sensitivity analysis was performed without the two groups and showed no impact on the result as the pooled ACLCdiff was found to be 12.7 ml/kg/min (95% CI: 10.4 to 15.0). Future well-conducted studies that directly compare AC and LC in other populations are needed. Future research should also include disease populations with limitations by lower limb disability such as peripheral vascular disease or osteoarthritis, or trained and upper extremity dominant athletes.
CONCLUSION
This systematic review and meta-analysis showed that the VO2max achieved by the AC tests were on average 70% of the VO2max achieved by the LC test, in studies on healthy non-athletic individuals. There was a linear association between the VO2max for the AC test and the LC test. The magnitude of this difference appeared to be reduced in studies with older and less active populations.
APPENDIX 1.
Search strategy for MEDLINE
| Search item 1 | Search item 2 | Search item 3 |
|---|---|---|
| Bicycling [MeSH] | Arm [MeSH] | Oxygen consumption [MeSH] |
| Ergometry [MeSH] | CPET arm | Physical endurance [MeSH] |
| Leg [MeSH] | Arm cycle ergometry | Exercise test [MeSH] |
| CPET leg | Arm-crank ergometry | Fatigue [MeSH] |
| CPETleg | Arm ergometry | Physical exertion [MeSH] |
| Cycle ergometry | CPETarm | Oxygen uptake |
| Leg cycle ergometry | Arm crank | Physical fitness |
| cycle ergometer | Arm crank ergometer | VO2 |
| bicycle ergometer | Arm ergometer | VO2 max |
| Electromagnetically braked ergometer | Arm cycle ergometer | VO2max |
| Lower body exercise | Arm cycling | Oxygen consumption |
| Cardiopulmonary exercise testing leg | Upper body exercise | Peak oxygen consumption |
| Cardiopulmonary exercise testing | Arm cranking | Anaerobic threshold |
| ETT | Cardiopulmonary exercise testing arm | VO2 peak |
| Exercise tolerance test | Arm exercise | VO2peak |
| Leg exercise | Cranking | Maximal aerobic power |
| Cycling | Arm work | Aerobic power |
| Cycle exercise | Aerobic capacity | |
| Leg cycling | Work capacity | |
| Leg ergometry | Peak pulmonary O2 metabolic efficiency | |
| Maximal oxygen uptake | ||
| Oxygen uptake | ||
| Peak exercise | ||
| Peak physiologic responses | ||
| Cardiorespiratory responses | ||
| Physiological comparison |
APPENDIX 2.
Detailed characteristics of included studies
| Aminoff, T. et al. (1996) | |
| Title | Physical work capacity in dynamic exercise?with differing muscle masses in healthy young and older men |
| Methods | Cross-sectional |
| Participant status | 19 healthy, non-smokers, and physically active men. Subjects participated in conditioning exercises, on average, two to four times a week.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 4 |
| Notes | |
| Aminoff, T. et al. (1999) | |
| Title | Physiological strain during kitchen work in relation to maximal and task-specific peak values |
| Methods | Cross-sectional |
| Participant status | Nine kitchen workers from a large hospital kitchen with a conveyor belt, collecting and sorting dirty plates.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Bhambhani, Y, et al, (1998) | |
| Title | Muscle oxygenation during incremental arm and leg exercise in men and women |
| Methods | Cross-sectional |
| Participant status | Fifteen men and 10 women who were free from metabolic and cardiorespiratory diseases. The volunteers were university students and members of local sports club.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Bhambhani, Y, et al, (1995) | |
| Title | Prediction of stroke volume during upper and lower body exercise in men and women |
| Methods | Cross-sectional |
| Participant status | 37 recreationally active subjects not involved in any particular exercise-training programme.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Bhambhani, Y, et al, (1991) | |
| Title | Transfer effects of endurance training with the arms and legs |
| Methods | RCT |
| Participant status | 16 healthy middle-aged male subjects in the arm group, and 8 healthy middle-aged male subjects in the leg group.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 4 |
| Notes | |
| Barstow, T. J. et al. (1993) | |
| Title | O2 uptake kinetics and the O2 deficit as related to exercise intensity and blood lactate |
| Methods | Cross-sectional |
| Participant status | Four untrained subjects aged 24-38 years, weight 59-89 kg
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 3 |
| Notes | |
| Boileau, R. A. et al. (1984) | |
| Title | Cardiovascular and metaboli contributions to the maximal power of the arms and legs |
| Methods | Cross-sectional |
| Participant status | Moderately active, nonathletic male college students.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 6 |
| Notes | |
| Bond, V. et al. (1986) | |
| Titel | Aerobic capacity during two-arm and one-leg exercise |
| Methods | Cross-sectional |
| Participant status | Eight healthy males. The subjects had not participated in any upper or lower body conditioning for 12 months prior to the tests
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 4 |
| Notes | |
| Bouchard, C. et al. (1979) | |
| Title | Specificity of maximal aerobic power |
| Methods | Cross-sectional |
| Participant status | 30 moderately active male subjects.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 5 |
| Notes | The study reports a correlation coefficient between AC and LC on r = 0.70. |
| Castro, R. et al. (2011) | |
| Title | Different ventilatory responses to progressive maximal exercise test performed with either the arms or legs |
| Methods | Cross-sectional |
| Participant status | 12 subjects of hospital staff and university students. They were considered healthy upon a clinical evaluation (physical examination and clinical history) and a maximal exercise test performed on a cycle ergometer. None of the subjects were engaged in regular physical exercise. None of the subjects were accustomed to arm-crank exercise.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 6 |
| Notes | |
| Charbonnier, J. P. et al. (1975) | |
| Title | Experimental study on the performance of competition swimmers. |
| Methods | Cross-sectional |
| Participant status | Six non-swimmers with a mean age of 31 ± 4 years, a mean height of 178 ± 3 cm and a mean bodyweight of 71 ± 5 kg. The swimmers were among the best in the country and the non-swimmers were members of the laboratory staff.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Davies, C. T. M., & Sargeant, A. J. (1974) | |
| Title | Indirect determination of maximal aerobic power output during work with one or two limbs. |
| Methods | Cross-sectional |
| Participant status | 12 healthy male subjects. All except four subjects were accustomed to physical investigations.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 1 |
| Notes | |
| Davis, J. A. et al (1976) | |
| Title | Anaerobic threshold and maximal aerobic power for three modes of exercise. |
| Methods | Cross-sectional |
| Participant status | 39 healthy university male students. None of them had been endurance training four months prior to the experiment. Nine of the 39 subjects participated only in the validation period.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 4 |
| Notes | |
| Dekerle, J. et al. (2002) | |
| Title | Ventilatory thresholds in arm and leg exercices with spontaneously chosen crank and pedal rates. |
| Methods | Cross-sectional |
| Participant status | 20 male students in physical education with a mean age of years, a mean height of cm and a mean bodyweight of kg.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 4 |
| Notes | |
| Franklin, B. A. et al. (1983) | |
| Titel | Aerobic requirements of arm ergometry: implications for exercise testing and training |
| Methods | Cross-sectional |
| Participant status | 10 healthy male subjects.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 2 |
| Notes | The study reports a correlation coefficient between AC and LC on r = 0.32. |
| Franssen, F. M. et al. (2002) | |
| Title | Arm mechanical efficiency and arm exercise capacity are relatively preserved in chronic obstructive pulmonary diseas |
| Methods | Cross-sectional |
| Participant status | Controls, male/female (14/6) did not participate in any exercise-training program and were found through an advertisement in the local newspaper
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 4 |
| Notes | |
| Javierre, C. et al. (2007) | |
| Title | Physiological responses to arm and leg exercise in women with chronic fatigue syndrome. |
| Methods | Cross-sectional |
| Participant status | 15 healthy controls that were extremely sedentary. Their occupation did not require physical effort, they did not perform physical activity and or their hobbies were sedentary.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 6 |
| Notes | |
| Keteyian, S. et al. (1994) | |
| Title | Cardiovascular responses of cardiac transplant patients to arm and leg exercise. |
| Methods | Cross-sectional |
| Participant status | 10 healthy normal men. Five healthy subjects performed leg exercise three or more times per week and one healthy adult performed arm and leg exercise three times per week.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 3 |
| Notes | |
| Lewis, S. et al. (1980) | |
| Title | Transfer effects of endurance training to exercise with untrained limbs |
| Methods | RCT |
| Participant status | Five healthy male college students.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 6 |
| Notes | |
| Loughney, L. et al. (2014) | |
| Title | Comparison of oxygen uptake during arm or leg cardiopulmonary exercise testing in vascular surgery patients and control subjects |
| Methods | Cross-sectional |
| Participant status | Twenty healthy control subjects .
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 5 |
| Notes | The study reports a correlation coefficient between AC and LC on r = 0.77. |
| Louhevaara, V. et al. (1990) | |
| Title | Differences in cardiorespiratory responses during and after arm crank and cycle exercise. |
| Methods | Cross-sectional |
| Participant status | 21 untrained healthy men.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 3 |
| Notes | |
| Lyons, S. et al. (2007) | |
| Title | Excess post-exercise oxygen consumption in untrained men following exercise of equal energy expenditure: comparisons of upper and lower body exercise |
| Methods | Cross-sectional |
| Participant status | The subjects were recruited from the local university and city community, and consisted of individuals who were already participating in at least 30 min of moderate recreational physical activity on most days of the week.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 6 |
| Notes | |
| McConnell, T. R. et al. (1984) | |
| Title | The hemodynamic and physiologic differences between exercise modalities |
| Methods | Cross-sectional |
| Participant status | Healthy subjects.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 3 |
| Notes | |
| Nag, P. K. (1984) | |
| Title | Circulo-respiratory responses to different muscular exercises |
| Methods | Cross-sectional |
| Participant status | Five young men, free from any cardiovascular. They actively participated habitually in moderately heavi agricultural work, none were the limb and trunk muscles specially trained.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 3 |
| Notes | |
| Orr, J. L. et al. (2013) | |
| Title | Cardiopulmonary exercise testing: arm crank vs cycle ergometry |
| Methods | Cross-sectional |
| Participant status | Fifteen healthy women were recruited from the University of Dundee.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Pogliaghi, S. et al. (2006) | |
| Title | Adaptations to endurance training in the healthy elderly: arm cranking versus leg cycling |
| Methods | RCT study |
| Participant status | 18 men were recruited by local advertisements in the metropolitan area of Verona (Italy).
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 7 |
| Notes | |
| Protas, E. J. et al. (1996) | |
| Title | Cardiovascular and metabolic responses to upper- and lower-extremety exercise in men with idiopathic Parkinson's disease. |
| Methods | Cross-sectional study |
| Participant status | 7 control subjects from the local community with a mean age of 65 (53-71) were recruited. The controls were more sedentary than the PD group.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 3 |
| Notes | |
| Rathnow, K. M., & Mangum, M. (1990) | |
| Title | Cardiopulmonary exercise testing: arm crank vs. cycle ergometry |
| Methods | Cross-sectional |
| Participant status | The single mode treatment group consisted of six males and three females. The mixed mode treatment group consisted of five males and three females. Due to the presentation of data in the study, and mixture of sexes in the groups this study will appear with no demographic data.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Reybrouck, T. et al. (1975) | |
| Title | Limitations to maximum oxygen uptake in arm, leg and combined arm and leg ergometry. |
| Methods | Cross-sectional |
| Participant status | The untrained subject was 25 years old.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 4 |
| Notes | |
| Ramonatxo, M. er al. (1996). | |
| Title | Differences in mouth occlusion pressure and breathing pattern between arm and leg incremental exercise. |
| Methods | Cross-sectional study |
| Participant status | Eight normal male subjects. No subjects were involved in exercise training but all maintained their accustomed exercise training.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 3 |
| Notes | |
| Rösler, K. et al (1985) | |
| Title | Transfer effects in endurance exercise. |
| Methods | Trial |
| Participant status | Ten healthy male subjects with a mean age of 30.5 (23-37) years, a mean height of 178 (172-182) cm and a mean bodyweight of 70.8 (64-83) kg. None of them had been involved in regular training during the preceding two years, although some of then did some recreational jogging or cycling.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 4 |
| Notes | |
| Sargeant, A. J., & Davies, C. T. M. (1973). | |
| Title | Perceived exertion during rhythmic exercise involving different muscle mass |
| Methods | Cross-sectional study |
| Participant status | Six healthy male subjects. All of the subjects had taken part of physiological investigations before and were habituated to the exercise modalities in the study. All of the physical characteristics are given individually. The age ranges from 24-39 years, the height ranges from 171.8-189.0 cm and the bodyweight from 63.0-98.0 kg.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 2 |
| Notes | |
| Sawka, M. N. Et al. (1983) | |
| Title | Physiological factors affecting upper body aerobic exercise |
| Methods | Cross-sectional study |
| Participant status | Nine male subjects.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 2 |
| Notes | The study reports a correlation coefficient between AC and LC on r = 0.94. |
| Sharp, M. A. et al. (1988) | |
| Title | Maximal aerobic capacity for repetitive lifting: comparison with three standard exercise testing modes |
| Methods | Cross-sectional study |
| Participant status | 18 male subjects.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 2 |
| Notes | |
| Shiomi, T. et al. (2000) | |
| Title | Physiological responses and mechanical efficiency during different types of ergometric exercises. |
| Methods | Cross-sectional study |
| Participant status | Seven healthy male. No subjects were performing regular exercise and none had orthopaedic diseases. The subjects performed the tests at least two hours after the last meal and did not exercise before the tests.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 4 |
| Notes | The study reports a correlation coefficient between AC and LC on r = 0.78. |
| Sporer, B. C. et al. (2007) | |
| Title | Entrainment of breathing in cyclists and non-cyclists during arm and leg exercise |
| Methods | Cross-sectional study |
| Participant status | Eight control subjects.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Swensen, T. C., & Howley, E. T. (1993) | |
| Title | Effect of one- and two-leg training on arm and two-leg maximum aerobic power |
| Methods | RCT |
| Participant status | 21 untrained college-age men participated. They had a mean age of 22.8 (19-32) years and a mean bodyweight of 73 (45-91) kg.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max and RER |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Turner, D. L. et al. (1997) | |
| Title | Effects of endurance training on oxidative capacity and structural composition of human arm and leg muscles. |
| Methods | Trial |
| Participant status | Six healthy male subjects. None of the subjects trained systematically although they were recreationally active.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 6 |
| Notes | |
| Warren, G. L. et al. (1990) | |
| Title | Is gender difference in peak VO2 greater for arm than leg exercise? |
| Methods | Cross sectional study |
| Participant status | The untrained subjects had not participated in any form of regular aerobic exercise or strength training three months prior to the study.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Yasuda, N., et al. (2008) | |
| Title | No gender-specific differences in mechanical efficiency during arm or leg exercise relative to ventilatory threshold |
| Methods | Cross sectional study |
| Participant status | The women had a mean age of 23.4 ± 3.6 years, mean BMI 22.8 ± 2.1 units, a mean height of 167.3 ± 6.2 cm and a mean bodyweight of 63.6 ± 5.5 kg.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 5 |
| Notes | |
| Yasuda, N., et al. (2006) | |
| Title | Substrate oxidation during incremental arm and leg exercise in men and women matched for ventilator threshold |
| Methods | Cross sectional study |
| Participant status | The subject performed low intensity exercises, such as running og cycling, for less than 1 hour per week for a maximum of 4 times per week.
|
| Study protocol | |
|
|
| Outcomes of interest | VO2max |
| Risk of bias | SumQAT: 5 |
| Notes | |
APPENDIX 3.
Detailed risk of bias assessment
REFERENCES
- 1.Young EL, Karthikesalingam A, Huddart S, et al. A systematic review of the role of cardiopulmonary exercise testing in vascular surgery. Eur J Vasc Endovasc Surg. 2012;44(1):64-71. [DOI] [PubMed] [Google Scholar]
- 2.Steins Bisschop CN, Velthuis MJ, Wittink H, et al. Cardiopulmonary exercise testing in cancer rehabilitation: a systematic review. Sports Med. (Auckland, N.Z.). 2012;42(5):367-379. [DOI] [PubMed] [Google Scholar]
- 3.Albouaini K, Egred M, Alahmar A. Cardiopulmonary exercise testing and its application. Postgrad Med J. 2007;83(985):675-682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Herdy AH, Uhlendorf D. Reference values for cardiopulmonary exercise testing for sedentary and active men and women. Arq Bras Cardiol. 2011;96(1):54-59. [DOI] [PubMed] [Google Scholar]
- 5.Paap D, Takken T. Reference values for cardiopulmonary exercise testing in healthy adults: A systematic review. Expert Rev Cardiovasc Ther. 2014;12(12):1439-1453. [DOI] [PubMed] [Google Scholar]
- 6.Stickland MK, Butcher SJ, Marciniuk DD, Bhutani M. Assessing Exercise Limitation Using Cardiopulmonary Exercise Testing. Pulm Med. 2012;2012:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2003;167(2):211-277. [DOI] [PubMed] [Google Scholar]
- 8.Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH, Jr., Wilson JR. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circ. 1991;83(3):778-786. [DOI] [PubMed] [Google Scholar]
- 9.Vanhees L, Fagard R, Thijs L, Amery A. Prognostic value of training-induced change in peak exercise capacity in patients with myocardial infarcts and patients with coronary bypass surgery. Am J Cardiol. 1995;76(14):1014-1019. [DOI] [PubMed] [Google Scholar]
- 10.West M, Jack S, Grocott MPW. Perioperative cardiopulmonary exercise testing in the elderly. Best Pract Res Clin Anaesthesiol. 2011;25(3):427-437. [DOI] [PubMed] [Google Scholar]
- 11.Vanhees L, De Sutter J, Gelada SN, et al. Importance of characteristics and modalities of physical activity and exercise in defining the benefits to cardiovascular health within the general population: recommendations from the EACPR (Part I). Eur J Prev Cardiol. 2012;19(4):670-686. [DOI] [PubMed] [Google Scholar]
- 12.Loughney L, West M, Pintus S, et al. Comparison of oxygen uptake during arm or leg cardiopulmonary exercise testing in vascular surgery patients and control subjects. Br J Anaesth. 2014;112(1):57-65. [DOI] [PubMed] [Google Scholar]
- 13.Walker RD, Nawaz S, Wilkinson CH, Saxton JM, Pockley AG, Wood RFM. Influence of upper- and lower-limb exercise training on cardiovascular function and walking distances in patients with intermittent claudication. J Vasc Surg. 2000;31(4):662-669. [DOI] [PubMed] [Google Scholar]
- 14.Sutbeyaz ST, Sezer N, Koseoglu BF, Ibrahimoglu F, Tekin D. Influence of knee osteoarthritis on exercise capacity and quality of life in obese adults. Obesity (Silver Spring, Md.). 2007;15(8):2071-2076. [DOI] [PubMed] [Google Scholar]
- 15.Orr JL, Williamson P, Anderson W, Ross R, McCafferty S, Fettes P. Cardiopulmonary exercise testing: Arm crank vs cycle ergometry. Anaesthesia. 2013;68(5):497-501. [DOI] [PubMed] [Google Scholar]
- 16.Secher NH, Volianitis S. Are the arms and legs in competition for cardiac output? Med Sci Sports Exerc. 2006;38(10):1797-1803. [DOI] [PubMed] [Google Scholar]
- 17.Sawka MN, Foley ME, Pimental NA, Pandolf KB. Physiological factors affecting upper body aerobic exercise. Ergonomics. 1983;26(7):639-646. [DOI] [PubMed] [Google Scholar]
- 18.Moher D, Liberati A, Tetzlaff J, Altman DG, The PG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009;6(7):e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.WHO. Global recommendations on physical activity for health. Switzerland: WHO;2010. [PubMed] [Google Scholar]
- 20.NHLBI. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. 2014; https://www.nhlbi.nih.gov/health-pro/guidelines/in-develop/cardiovascular-risk-reduction/tools/cohort. Accessed 28.05.2015, 2015.
- 21.Higgins J, Deeks JJ, Altman DG. Chapter 16: Special topics in statistics. Cochrane Handbook for Systematic Reviews of Interventions. Vol 5.1.02011. [Google Scholar]
- 22.Åstrand I. Aerobic work capacity in men and women with special reference to age. Acta Phys Scand Suppl. 1960;49(169):1-92. [PubMed] [Google Scholar]
- 23.Aminoff T, Smolander J, Korhonen O, Louhevaara V. Physical work capacity in dynamic exercise with differing muscle masses in healthy young and older men. Eur J Appl Physiol Occup Physiol. 1996;73(1-2):180-185. [DOI] [PubMed] [Google Scholar]
- 24.Aminoff T, Smolander J, Korhonen O, Louhevaara V. Physiological strain during kitchen work in relation to maximal and task-specific peak values. Ergonomics. 1999;42(4):584-592. [DOI] [PubMed] [Google Scholar]
- 25.Barstow TJ, Casaburi R, Wasserman K. O2 uptake kinetics and the O2 deficit as related to exercise intensity and blood lactate. J Appl Physiol. 1993;75(2):755-762. [DOI] [PubMed] [Google Scholar]
- 26.Bhambhani Y, Maikala R, Buckley S. Muscle oxygenation during incremental arm and leg exercise in men and women. Europ J Appl Physiol. 1998;78(5):422-431. [DOI] [PubMed] [Google Scholar]
- 27.Bhambhani YN. Prediction of stroke volume during upper and lower body exercise in men and women. Arch Phys Med Rehabil. 1995;76(8):713-718. [DOI] [PubMed] [Google Scholar]
- 28.Bhambhani YN, Eriksson P, Gomes PS. Transfer effects of endurance training with the arms and legs. Med ci Sports Exerc. 1991;23(9):1035-1041. [PubMed] [Google Scholar]
- 29.Boileau RA, McKeown BC, Riner WF. Cardiovascular and metabolic contributions to the maximal aerobic power of the arms and legs. Int J Sports Cardiol. 1984;1(2):67-75. [Google Scholar]
- 30.Bond V, Balkissoon B, Caprarola M, Tearney RJ. Aerobic capacity during two-arm and one-leg ergometric exercise. Int Rehab Med. 1986;8(2):79-81. [DOI] [PubMed] [Google Scholar]
- 31.Bouchard C, Godbout P, Mondor JC, Leblanc C. Specificity of maximal aerobic power. Europ J Appl Physiol. 1979;40(2):85-93. [DOI] [PubMed] [Google Scholar]
- 32.Castro RRT, Pedrosa S, Nobrega ACL. Different ventilatory responses to progressive maximal exercise test performed with either the arms or legs. Clinics. 2011;66(7):1137-1142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Charbonnier JP, Lacour JR, Riffat J, Flandrois R. Experimental study of the performance of competition swimmers. Eur J Appl Physiol Occup Physiol. 1975;34(3):157-167. [DOI] [PubMed] [Google Scholar]
- 34.Davies CTM, Sargeant AJ. Indirect determination of maximal aerobic power output during work with one or two limbs. Europ J Appl Physiol. 1974;32(3):207-215. [DOI] [PubMed] [Google Scholar]
- 35.Davis JA, Vodak P, Wilmore JH. Anaerobic threshold and maximal aerobic power for three modes of exercise. J Appl Physiol. 1976;41(4):544-550. [DOI] [PubMed] [Google Scholar]
- 36.Dekerle J, Dupont L, Caby I, et al. Ventilatory thresholds in arm and leg exercises with spontaneously chosen crank and pedal rates. Percept Mot Skills. 2002;95(3 Pt 2):1035-1046. [DOI] [PubMed] [Google Scholar]
- 37.Franklin BA, Vander L, Wrisley D, Rubenfire M. Aerobic requirements of arm ergometry: Implications for exercise testing and training. Phys Sportsmed. 1983;11(10):81-90. [DOI] [PubMed] [Google Scholar]
- 38.Franssen FME, Wouters EFM, Baarends EM, Akkermans MA, Schols AMW. Arm mechanical efficiency and arm exercise capacity are relatively preserved in chronic obstructive pulmonary disease. Med Sci Sports Exerc. 2002;34(10):1570-1576. [DOI] [PubMed] [Google Scholar]
- 39.Javierre C, Alegre J, Ventura JL, et al. Physiological responses to arm and leg exercise in women patients with chronic fatigue syndrome. J Chronic Fatigue Syndr. 2007;14(1):43-53. [Google Scholar]
- 40.Keteyian S, Marks CRC, Levine AB, et al. Cardiovascular responses of cardiac transplant patients to arm and leg exercise. Europ J Appl Physiol. 1994;68(5):441-444. [DOI] [PubMed] [Google Scholar]
- 41.Lewis S, Thompson P, Areskog NH, et al. Transfer effects of endurance training to exercise with untrained limbs. Eur J Appl Physiol Occup Physiol. 1980;44(1):25-34. [DOI] [PubMed] [Google Scholar]
- 42.Louhevaara V, Sovijarvi A, Ilmarinen J, Teraslinna P. Differences in cardiorespiratory responses during and after arm crank and cycle exercise. Acta Physiol Scand. 1990;138(2):133-143. [DOI] [PubMed] [Google Scholar]
- 43.Lyons S, Richardson M, Bishop P, Smith J, Heath H, Giesen J. Excess post-exercise oxygen consumption in untrained men following exercise of equal energy expenditure: Comparisons of upper and lower body exercise. Diabetes Obes Metab. 2007;9(6):889-894. [DOI] [PubMed] [Google Scholar]
- 44.McConnell TR, Swett DD, Jeresaty RM. The hemodynamic and physiologic differences between exercise modalities. J Sports Med Phys Fitness. 1984;24(3):238-245. [PubMed] [Google Scholar]
- 45.Nag PK. Circulo-respiratory responses to different muscular exercises. Europ J Appl Physiol 1984;52(4):393-399. [DOI] [PubMed] [Google Scholar]
- 46.Pogliaghi S, Terziotti P, Cevese A, Balestreri F, Schena F. Adaptations to endurance training in the healthy elderly: Arm cranking versus leg cycling. Europ J Appl Physiol. 2006;97(6):723-731. [DOI] [PubMed] [Google Scholar]
- 47.Protas EJ, Stanley RK, Jankovic J, MacNeill B. Cardiovascular and metabolic responses to upper- and lower-extremity exercise in men with idiopathic Parkinson's disease. Phys Ther. 1996;76(1):34-40. [DOI] [PubMed] [Google Scholar]
- 48.Ramonatxo M, Prioux J, Prefaut C. Differences in mouth occlusion pressure and breathing pattern between arm and leg incremental exercise. Acta Physiol Scand. 1996;158(4):333-341. [DOI] [PubMed] [Google Scholar]
- 49.Rathnow KM, Mangum M. A comparison of single-versus multi-modal exercise programs: Effects on aerobic power. J Sports Med Phys Fitness. 1990;30(4):382-388. [PubMed] [Google Scholar]
- 50.Reybrouck T, Heigenhauser GF, Faulkner JA. Limitations to maximum oxygen uptake in arm, leg, and combined arm leg ergometry. J Appl Physiol. 1975;38(5):774-779. [DOI] [PubMed] [Google Scholar]
- 51.Rosler K, Hoppeler H, Conley KE, Claassen H, Gehr P, Howald H. Transfer effects in endurance exercise. Adaptations in trained and untrained muscles. Eur J Appl Physiol Occup Physiol. 1985;54(4):355-362. [DOI] [PubMed] [Google Scholar]
- 52.Sargeant AJ, Davies CTM. Perceived exertion during rhythmic exercise involving different muscle masses. J Hum Ergol. 1973;2(1):3-11. [PubMed] [Google Scholar]
- 53.Sharp MA, Harman E, Vogel JA, Knapik JJ, Legg SJ. Maximal aerobic capacity for repetitive lifting: Comparison with three standard exercise testing modes. Europ J Appl Physiol. 1988;57(6):753-760. [DOI] [PubMed] [Google Scholar]
- 54.Shiomi T, Maruyama H, Saito A, Umemura M. Physiological responses and mechanical efficiency during different types of ergometric exercise. J Phys Ther Sci. 2000;12(1):67-73. [Google Scholar]
- 55.Sporer BC, Foster GE, Sheel AW, McKenzie DC. Entrainment of breathing in cyclists and non-cyclists during arm and leg exercise. Respir Physiol Neurobiol. 2007;155(1):64-70. [DOI] [PubMed] [Google Scholar]
- 56.Swensen TC, Howley ET. Effect of one- and two-leg training on arm and two-leg maximum aerobic power. Eur J Appl Physiol Occup Physiol. 1993;66(3):285-288. [DOI] [PubMed] [Google Scholar]
- 57.Turner DL, Hoppeler H, Claassen H, et al. Effects of endurance training on oxidative capacity and structural composition of human arm and leg muscles. Acta Physiol Scand. 1997;161(4):459-464. [DOI] [PubMed] [Google Scholar]
- 58.Warren GL, Cureton KJ, Dengel DR, Graham RE, Ray CA. Is the gender difference in peak V(O2) greater for arm than leg exercise? Europ J Appl Physiol. 1990;60(2):149-154. [DOI] [PubMed] [Google Scholar]
- 59.Yasuda N, Gaskill SE, Ruby BC. No gender-specific differences in mechanical efficiency during arm or leg exercise relative to ventilatory threshold. Scand J Med ci Sports. 2008;18(2):205-212. [DOI] [PubMed] [Google Scholar]
- 60.Yasuda N, Ruby BC, Gaskill SE. Substrate oxidation during incremental arm and leg exercise in men and women matched for ventilatory threshold. J Sports Sci. 2006;24(12):1281-1289. [DOI] [PubMed] [Google Scholar]
- 61.Bhagwat M, Paramesh K. Cardio-pulmonary exercise testing: An objective approach to pre-operative assessment to define level of perioperative care. Indian J Anaesth. 2010;54(4):286-291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Higgins J, Deeks JJ, Altman DG. 9.5.2 Identifying and measuring heterogeneity. Cochrane Handbook for Systematic Reviews of Interventions. Vol 5.1.02011. [Google Scholar]
- 63.Secher NH, Ruberg-Larsen N, Binkhorst RA, Bonde-Petersen F. Maximal oxygen uptake during arm cranking and combined arm plus leg exercise. J Appl Physiol. 1974;36(5):515-518. [DOI] [PubMed] [Google Scholar]