

Abstract
Introduction
Little research has been conducted to evaluate protocols and trends in orthodontic retention. The purpose of this study was to identify the general retention protocols used by orthodontists in the United States. Additionally, our goal was to identify trends in these orthodontic retention protocols by evaluating how they have changed over the past 5 years and how they might continue to change in the next 5 years.
Methods
The study was conducted via a 36-question electronic survey (REDCap, Nashville, Tenn) with branching logic on certain questions. The survey was sent to all 9143 practicing members of the American Association of Orthodontists in the United States, and 1632 (18%) responded.
Results and Conclusions
Mean retention protocols of the surveyed population showed predominant use of Hawley or vacuum-formed retainers in the maxillary arch and fixed retention in the mandibular arch. For both arches, there is a current shift away from Hawley retainers and toward vacuum-formed retainers and fixed retention. Respondents who extract fewer teeth reported increased use of fixed retention in the maxillary (P = 0.041) and mandibular (P = 0.003) arches. Respondents who extract fewer teeth and use removable retainers were more likely to tell their patients to wear their retainers at night for the rest of their lives (P = 1.63 × 10−6).
The goal of orthodontic retention is to increase the stability of the dentition after orthodontic treatment.1 Studies have shown that 40% to 90% of orthodontic patients have unacceptable dental alignment 10 years after treatment.2 Various methods of retention are in use today.3–5 Three main types of retainers used in the United States are Hawley, vacuum-formed, and fixed retainers.6
The first of the 2 phases of retention is called the retention phase. In this phase, the final alignment of the dentition is maintained as the associated soft tissues remodel at a rate above the baseline.2 The length of this remodeling process varies among different associated tissue types. Reorganization of the periodontal ligament occurs over a 3 to 4 month period. The gingival collagen-fiber network takes 4 to 6 months to remodel, and the elastic supracrestal fibers remain deviated for more than 7 months.7 It is generally accepted that this phase is completed within a year of debonding.
The second phase of retention, called the postretention phase, begins when increased remodeling of the supporting tissues after orthodontic treatment is complete and lasts the rest of the patient’s life. During this extended period of time, teeth are subjected to variable muscular forces acting on the periodontium with associated modeling and remodeling. The goal of the postretention phase is to maintain the alignment of the dentition regardless of changing forces.2 It is generally accepted that patients need to wear retainers for less time per day during the postretention phase compared with the retention phase.
A Cochrane Review of orthodontic retention reported that, “There are insufficient data on which to base our clinical practices on retention present … Given that the vast majority of orthodontic patients undergo a phase of retention, this vital area of orthodontic research should be given priority in the near future.”1
Little research has been published that addresses patient compliance with orthodontic retainers. An Australian study in 2005 concluded that there is a strong positive relationship between maxillary retainer compliance and patient-reported appliance comfort.8
A survey conducted at the University of Kentucky in 2008 evaluated patient compliance with orthodontic retainers.9 The authors found that the patient’s age, sex, amount of time since debonding, understanding of proper compliance, and retainer type all significantly influenced patient compliance. It was also found that patients were more compliant with vacuum-formed retainers than Hawley retainers initially after debonding. However, compliance decreased at a much faster rate with vacuum-formed retainers than with Hawley retainers. As a result, patients were more compliant overall with Hawley retainers than with vacuum-formed retainers. Finally, this study found that very few patients wore their retainers as instructed at 5 years after debonding.9
A review of the literature yielded 3 studies that evaluated retention protocols in Australia and New Zealand, the United Kingdom, and the Netherlands.3–5 Preferred methods of retention varied among the providers in these countries. Orthodontists in Australia and New Zealand preferred vacuum-formed retainers for the maxillary arch and fixed retention for the mandibular arch.5 Private practices in the United Kingdom preferred a combination of vacuum-formed retainers and fixed retention.4 Orthodontists in the Netherlands preferred fixed retention for both arches.3 The wide variations in the data of these studies support the position of the Cochrane review that practice guidelines are needed for orthodontic retention.
Keim et al6 conducted surveys regarding orthodontic trends over the past 25 years in the United States. They found that between 1986 and 2008 there was an increase in the use of vacuum-formed and fixed retainers as the preferred retainer types. During this same time period, they also found a corresponding decrease in the use of Hawley retainers. These authors reported an increase in lifelong retention protocols among US orthodontists during this time period.
A recent study by Valiathan and Hughes10 surveyed 2000 members of the American Association of Orthodontists (AAO) in the United States regarding orthodontic retention; they received 658 responses. The survey asked for the orthodontists’ most popular retention modality for each arch. Just over 58% of respondents preferred the Hawley retainer for the maxillary arch, and 40.2% preferred the fixed lingual retainer for the mandibular arch. Commentary responding to this study in the American Journal of Orthodontics and Dentofacial Orthopedics suggested that it would be of interest to determine “why orthodontists retain as they do.” Specifically, the reader feedback called for the study of a possible relationship among practicing orthodontists between their preferred retention protocols and their decisions on extractions.
The purpose of this study was to identify the general retention protocols used by US orthodontists via a census survey. Multiple variables were tested for possible associations, including type and duration of instructed retainer wear, practice of phase 1 treatment, and extraction rate. An additional goal was to identify how these protocols have changed over the past 5 years and how they might continue to change over the next 5 years.
MATERIAL AND METHODS
The study was conducted via an online, 36-question survey (REDCap, Nashville, Tennessee) with branching logic where appropriate. The AAO approved the survey before sending it to its US members, excluding residents and graduate students (approximately 9143 orthodontists). The survey was sent twice, with the second mailing 3 weeks after the first mailing. The survey concluded approximately 2 months after the initial mailing, when virtually all responses had ceased. Statistical analysis was conducted to identify trends (P <0.05) in the responses by using chi-square tests, analysis of variance (ANOVA), and linear regression, when appropriate.
RESULTS
One thousand six hundred thirty-two responses were received (18%). Thirty-nine percent of the respondents were certified by the American Board of Orthodontics, and 61% were uncertified. The respondents were evenly allocated in their number of years in practice; 83% of the respondents were men.
A summary of the data from this study is presented in Tables I and II. Average protocols reported are as follows (Fig 1): Hawley retainers were the most frequently used retainer type for the maxillary arch (47%), followed closely by vacuum-formed retainers (41%). Fixed retention (11%) was used much less frequently. In the mandibular arch, fixed retention (42%) was used most frequently, followed by an even distribution of Hawley retainers (29%) and vacuum-formed retainers (29%). Just over half (53%) of the responding orthodontists believed that their patients were more compliant with vacuum-formed retainers than with Hawleys, whereas only 6% believed the reverse to be true. Forty-one percent of our sample believed that there was no difference in compliance between the 2 retainer types (Fig 2).
Table I.
Summary of questionnaire responses
| Question | Response |
|---|---|
| What is your gender? | Male = 83% Female = 17% |
| When did you graduate from your orthodontic residency program? | Before 1970 = 6% |
| 1970–1980 = 20% | |
| 1980–1990 = 25% | |
| 1990–2000 = 25% | |
| 2000-present = 24% | |
| Are you certified by the American Board of Orthodontics? | Yes = 39% |
| No = 61% | |
| Do you use Phase I treatment in your practice? | Yes = 94% |
| No = 6% | |
| What percentage of patients in your practice receive extractions as part of their treatment plan? | Less than 1/4th = 76% |
| Between 1/4th and 1/2 = 22.5% | |
| Between 1/2 and 3/4th = 1.5% | |
| More than 3/4ths = 0% | |
| Do you practice a post-retention phase of retainer wear? (Do you have patients continue to wear retainers after the hard and soft tissues have completed remodeling following orthodontic therapy?) | Yes = 99% |
| No = 1% | |
| Does your post-retention phase last the rest of the patient’s file? | Yes = 82% |
| No = 18% | |
| Does whether or not a patient received extractions as part of their orthodontic therapy influence the type of retainer that you will give a patient? | Yes = 46% |
| No = 54% | |
| Do you charge for retainer checks? | Yes = 11% |
| No = 89% | |
| With which of the following types of retainers do you believe patients are more complaint? | VFR = 53% |
| Hawley = 6% | |
| No Difference = 41% | |
| Do you believe that a patient’s age influences their retainer compliance? | Yes = 86% |
| No = 14% |
Table II.
Summary of questionnaire responses
| Question | Responses (n) | Minimum | Mean | Median | Maximum | SD |
|---|---|---|---|---|---|---|
| How many hours per day do you require patients to wear their retainers during the retention phase of treatment? (0–24 hours) | 1362 | 3.4 | 17.1 | 19.4 | 24.0 | 5.8 |
| How long does your retention phase last? (0–1 year) | 1362 | 0.0 | 0.8 | 1.0 | 1.0 | 0.3 |
| How many hours per day do you require patients to wear their retainers during the post-retention phase of treatment? (0–24 hours) | 1109 | 0.0 | 8.6 | 8.2 | 24.0 | 2.9 |
| How long does your post-retention phase last? (0–6 year) | 171 | 0.0 | 3.4 | 3.2 | 6.0 | 1.6 |
| What percentage of your patient population receives Hawley retainers for the maxillary arch? | 1362 | 0.0 | 53.6 | 60.0 | 100.0 | 36.7 |
| What percentage of your patient population receives vacuum-form retainers for the maxillary arch? | 1362 | 0.0 | 47.5 | 45.0 | 100.0 | 37.1 |
| What percentage of your patient population receives fixed retention for the maxillary arch? | 1362 | 0.0 | 13.0 | 5.0 | 100.0 | 22.7 |
| What percentage of your patient population receives Hawley retainers for the mandibular arch? | 1362 | 0.0 | 32.6 | 15.0 | 100.0 | 34.9 |
| What percentage of your patient population receives vacuum-form retainer for the mandibular arch? | 1362 | 0.0 | 32.7 | 11.0 | 100.0 | 36.4 |
| What percentage of your patient population receives fixed retention for the mandibular arch? | 1362 | 0.0 | 48.0 | 40.0 | 100.0 | 39.4 |
| What percentage of your patient population receives a fiberotomy following treatment? | 1362 | 0.0 | 4.1 | 1.0 | 100.0 | 10.2 |
| How long do your patients continue to return to your practice for scheduled retainer check appointments? (0–10 + years) | 1362 | 0.0 | 2.9 | 2.3 | 10.0 | 2.2 |
| How often do your patients return for retainer checks? (0–6 times per year) | 1362 | 0.0 | 2.1 | 1.9 | 6.0 | 1.3 |
| How long after debonding do you begin charging for retainer checks? (0–4 years) | 127 | 0.0 | 1.2 | 1.0 | 4.0 | 18.4 |
| When you charge for retainer checks, what is the average fee charged? ($0–200) | 138 | 0.0 | 52.9 | 26.5 | 196.0 | 1.0 |
| What percentage of patients do you believe to be compliant with your retention protocols six months following bebonding? | 1362 | 1.0 | 69.4 | 75.0 | 100.0 | 17.5 |
| What percentage of patients do your believe to be complaint with your retention protocols one year following debonding? | 1362 | 2.0 | 57.5 | 60.0 | 100.0 | 20.5 |
| What percentage of patients do you believe to be compliant with your retention protocols three years following debonding? | 1362 | 0.0 | 39.4 | 38.0 | 100.0 | 21.5 |
| What percentage of patients do you believe to be complaint with your retention protocols five years following debonding? | 1362 | 0.0 | 29.8 | 25.0 | 100.0 | 21.5 |
Fig 1.
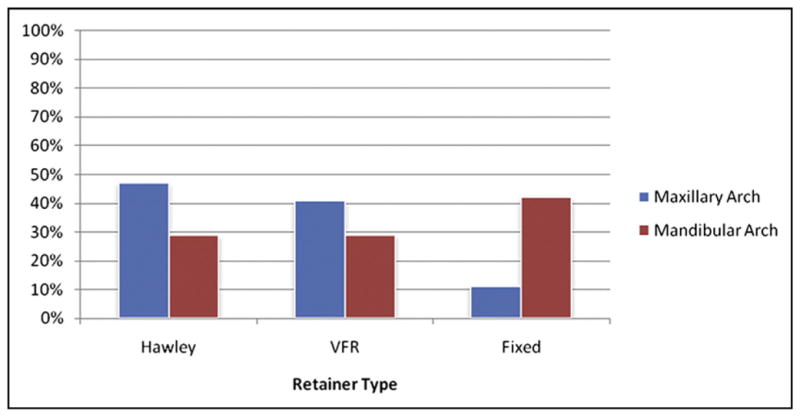
Mean responses of retainer types used. VFR, Vacuum-formed retainer.
Fig 2.
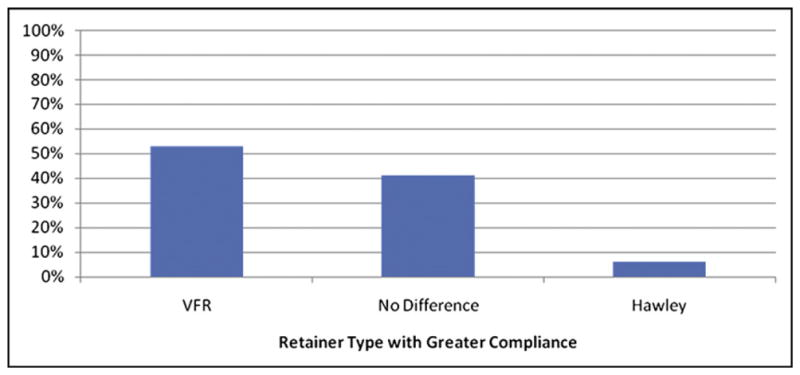
Orthodontists’ perceptions of patient compliance with Hawley vs vacuum-formed reatiners. VFR, Vacuum-formed retainer.
Statistically significant relationships in the data were identified. Respondents who extracted fewer teeth reported increased use of fixed retention in both the maxillary and mandibular arches (P = 0.041 and P = 0.003, respectively). Respondents who extracted fewer teeth and preferred removable retainers were more likely to tell their patients to wear their retainers at night for the rest of their lives (P = 1.63 × 10−6). Orthodontists who practiced phase 1 treatment were more likely to report extracting fewer teeth during phase 2 treatment (P = 4.79 × 10−8). However, it was also found that orthodontists who practiced phase 1 therapy were more likely to use fixed retention than those who did not (P =0.042). A linear model regressing fixed retention rates and extraction frequency on phase 1 practice suggests that fixed retention preference drives the relationship with phase 1 treatment preference. In other words, excluding the effects of an orthodontist’s choice whether to use fixed retention, there was no statistically significant relationship between phase 1 treatment and the frequency of extracting teeth.
Nearly half of the orthodontists (44%) reported reducing their use of Hawley retainers over the past 5 years, and only 6% reported increasing Hawley use over the same time period. The data suggest that this trend will most likely continue over the next 5 years. Slightly more orthodontists reported decreasing their use of vacuum-formed retainers (14%) than those who reported increasing their use (11%) over the past 5 years. However, significantly more orthodontists reported that they will increase their use of vacuum-formed retainers (29%) over the next 5 years than those who reported that they will decrease their use (5%). More orthodontists reported increasing their use of fixed retention (36%) over the past 5 years than those who reported decreasing it (11%). The data suggest that this trend can also be expected to continue over the next 5 years (Fig 3).
Fig 3.
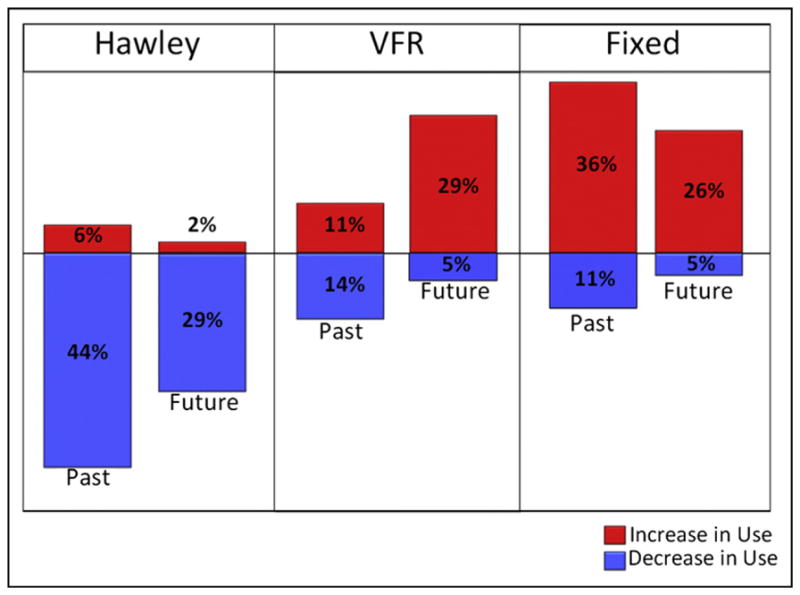
Changes in retainer use over the past 5 years and projections for the next 5 years. VFR, Vacuum-formed retainer.
DISCUSSION
When comparing our results with those of Keim et al6 and Valiathan and Hughes,10 our study seems to show an increased use of vacuum-formed retainers for the maxillary arch. However, those studies asked only for each orthodontist’s predominant method of retention, whereas we requested percentages of patients who receive the 3 retainer types evaluated. Our study shows that vacuum-formed retainers are used to a considerable degree in the maxillary arch, even though it is less than Hawley use. Only with the method of questioning used in this study would this information become apparent.
The results of this study show a definite shift in preferred retainer types among US orthodontists. A graphic representation of this shift is shown in Figure 3. These data are consistent with the results of Keim et al.6 Overall, US orthodontists are moving away from Hawley retainers and toward vacuum-formed retainers and fixed retention.
The current trend toward vacuum-formed retainers and away from Hawley retainers found in this study is consistent with certain previous studies showing that patients are more compliant with vacuum-formed retainers.8,11 However, these studies evaluated compliance less than 2 years into retention. Another study evaluating long-term patient compliance by Pratt et al9 showed that compliance was initially higher with vacuum-formed retainers but decreased at a significantly faster rate than with Hawley retainers. That study showed that Hawley retainer compliance surpasses that of vacuum-formed retainers about 2 years after debonding. As a result, patient compliance is greater with Hawley retainers overall.
Mollov et al11 surveyed patients after orthodontic treatment. They found that patients who had an “invisible” retainer were significantly more likely to be compliant with proper retainer wear than those with a Hawley retainer. However, the patients surveyed with Hawley retainers had been in retention for a significantly longer period of time that those with “invisible” retainers. Consequently, it is possible that their conclusion that patients were more complaint with “invisible” retainers over Hawleys is more a function of length of time in retention than of retainer preference.
Of the orthodontists surveyed in this study who believed that retainer type impacts patient compliance, the vast majority believed that patients are more compliant with vacuum-formed retainers than with Hawley retainers (Fig 2). On average, the orthodontists we surveyed stopped seeing their patients for retainer checks between 2 and 3 years after debonding. As a result, it is certainly conceivable that orthodontists do not report favorable compliance rates with Hawley retainers because they have already stopped seeing patients for retainer checks before the shift in compliance reported by Pratt et al.9
The trend of orthodontists using more fixed retention might be related to long-term dental changes that they have seen in their own practices. It is not uncommon for an orthodontic patient to return to a practice for retreatment years after the initial treatment. The logistic regression model from Pratt et al9 shows that patient compliance with removable retainers is poor, even by 5 years out of treatment. Additionally, Cerny et al12 found that patients favor permanently bonded retainers over removable ones. Some orthodontists might have concluded, rightly or wrongly, that the only way to promote long-term stability is with fixed retention.
There are both similarities and differences in the retention protocols of countries in which similar studies have been conducted. In all countries studied, fixed retention is at least part of the preferred option for the mandibular arch. Orthodontists in the United States use Hawley retainers much more frequently than in any other country studied. The amount of fixed retention used in the maxillary arch varies greatly among countries. Not only do the protocols vary among these countries, but they also vary greatly in each country. There does not seem to be much consistency in how practitioners choose the retainer types they use. This supports the need for practice guidelines for orthodontic retention.
Accuracy of orthodontists’ predictions of patient compliance varied when compared with the findings of Pratt et al9 (Table II). Those surveyed underestimated patient compliance at 6 months after debonding. On the other hand, they grossly overestimated patient compliance at 5 years out of treatment. Again, this overestimation might be because those surveyed reported a median value of slightly over 2 years for the duration of their retainer checks. It is possible that orthodontists have misconceptions regarding patient compliance at 5 years out of treatment because they do not follow their patients for that length of time.
Orthodontists who reported extracting less frequently also reported significantly increased use of fixed retention in both the maxillary and mandibular arches (P = 0.041 and P =0.003, respectively). Orthodontists who reported extracting less were more likely to tell their patients to wear their retainers at night for the rest of their lives (P = 1.63 × 10−6). Although lifelong retention should be the standard, perhaps these orthodontists use these protocols more frequently because they are concerned about the stability of their nonextraction treatment.
Often, 1 goal of phase 1 treatment is to increase the arch perimeter. After eliminating the effects of fixed retention in our study, there was no significant difference in the frequency of extracted teeth between orthodontists who practiced phase 1 treatment and those who did not. This finding supports the concept that 2 phases of treatment do not result in an increased arch perimeter over a single phase of treatment. These findings are consistent with those of a randomized controlled trial at the University of Florida between 1990 and 2003: no significant differences were found in the arch length discrepancies of Class II patients who received 1-phase vs 2-phase treatment.13
This study had some limitations: (1) a few AAO members might not have received this survey if they do not have e-mail or do not use the e-mail address that they gave to the AAO; (2) the survey “sliders” (continuously movable sliding selection indicators) used to record some responses might have been a source of error, considering the difficulty in selecting an exact percentage for a response; (3) the survey did not ask how many active patients each orthodontist treats, so, since some orthodontists see more patients than others, the exact percentage of patients who receive a given treatment modality could not be evaluated; (4) we did not ask whether previous and future changes in protocols would differ between the mandibular and maxillary arches; (5) the survey did not include an “I don’t know” option for questions related to the orthodontist’s perception of patient compliance; and (6) no information differentiating respondents from nonrespondents is available.
This study provides a baseline of current orthodontic retention protocols preferred by US members of the AAO. It also illustrates the current trends in orthodontic retention. Future studies might incorporate which treatment modalities are most effective for a specific patient. Retention should be tailored to the treatment provided and the problems corrected with that treatment. Research should be conducted to identify which retention modalities are most effective for specific orthodontic issues. For example, even an orthodontist who prefers vacuum-formed retainers in general might at least consider a bonded retainer in a case that involved the unraveling of a severely crowded mandibular arch. Methods of increasing patient compliance with removable retainers would also be of benefit. The ultimate goal should be well-conducted research that combines effective retention protocols with methods for increasing patient compliance. Such research might move us closer to a day when the preferred retainer type and the most effective retention protocol will coincide.
CONCLUSIONS
US orthodontists reported predominant use of Hawley (47%) and vacuum-formed retainers (41%) for retention in the maxillary arch, and fixed retention (42%) in the mandibular arch.
There is an overall shift away from Hawley retainers and toward vacuum-formed retainers and fixed retention.
Respondents who extract less frequently reported increased use of fixed retention for the maxillary (P = 0.041) and mandibular (P = 0.003) arches.
Respondents who extract less and use removable retainers were more likely to prescribe lifelong retention (P = 1.63 × 10−6).
Fifty-three percent of those surveyed believe that patients are more compliant with vacuum-formed retainers than with Hawley retainers, and only 6% believe that the reverse is true.
Those surveyed grossly overestimated patient compliance with removable retainers at 5 years after de-bonding.
Practicing phase 1 treatment did not decrease the percentage of patients who were treated with extraction therapy, after adjusting for the effects of fixed retention.
Footnotes
The authors report no commercial, proprietary, or financial interest in the products or companies described in this article.
References
- 1.Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. 2006:CD002283. doi: 10.1002/14651858.CD002283.pub3. [DOI] [PubMed] [Google Scholar]
- 2.Thilander B. Orthodontic relapse versus natural development. Am J Orthod Dentofacial Orthop. 2000;117:562–3. doi: 10.1016/s0889-5406(00)70200-9. [DOI] [PubMed] [Google Scholar]
- 3.Renkema AM, Sips ET, Bronkhorst E, Kuijpers-Jagtman AM. A survey on orthodontic retention procedures in The Netherlands. Eur J Orthod. 2009;31:432–7. doi: 10.1093/ejo/cjn131. [DOI] [PubMed] [Google Scholar]
- 4.Singh P, Grammati S, Kirschen R. Orthodontic retention patterns in the United Kingdom. J Orthod. 2009;36:115–21. doi: 10.1179/14653120723040. [DOI] [PubMed] [Google Scholar]
- 5.Wong PM, Freer TJ. A comprehensive survey of retention procedures in Australia and New Zealand. Aust Orthod J. 2004;20:99–106. [PubMed] [Google Scholar]
- 6.Keim RG, Gottlieb EL, Nelson AH, Vogels DS., 3rd 2008 JCO study of orthodontic diagnosis and treatment procedures, part 1: results and trends. J Clin Orthod. 2008;42:625–40. [PubMed] [Google Scholar]
- 7.Melrose C, Millett DT. Toward a perspective on orthodontic retention? Am J Orthod Dentofacial Orthop. 1998;113:507–14. doi: 10.1016/s0889-5406(98)70261-6. [DOI] [PubMed] [Google Scholar]
- 8.Wong P, Freer TJ. Patients’ attitudes towards compliance with retainer wear. Aust Orthod J. 2005;21:45–53. [PubMed] [Google Scholar]
- 9.Pratt M, Kluemper G, Lindstrom A. Patient compliance with orthodontic retainers in the postretention phase. Am J Orthod Dentofacial Orthop. 2011;140:196–201. doi: 10.1016/j.ajodo.2010.02.035. [DOI] [PubMed] [Google Scholar]
- 10.Valiathan M, Hughes E. Results of a survey-based study to identify common retention practices in the United States. Am J Orthod Dentofacial Orthop. 2010;137:170–7. doi: 10.1016/j.ajodo.2008.03.023. [DOI] [PubMed] [Google Scholar]
- 11.Mollov ND, Lindauer SJ, Best AM, Shroff B, Tufekci E. Patient attitudes toward retention and perceptions of treatment success. Angle Orthod. 2010;80:468–73. doi: 10.2319/102109-594.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cerny R, Cockrell D, Lloyd D. A survey of patient opinions on fixed vs. removable retainers. J Clin Orthod. 2009;43:784–7. [PubMed] [Google Scholar]
- 13.Wortham JR, Dolce C, McGorray SP, Le H, King GJ, Wheeler TT. Comparison of arch dimension changes in 1-phase vs 2-phase treatment of Class II malocclusion. Am J Orthod Dentofacial Orthop. 2009;136:65–74. doi: 10.1016/j.ajodo.2007.06.020. [DOI] [PubMed] [Google Scholar]