

Abstract
Purpose
Investigate the clinical characteristics, radiographic patterns, and treatment course of PD-1 inhibitor-related pneumonitis in advanced cancer patients.
Experimental Design
Among patients with advanced melanoma, lung cancer, or lymphoma treated in trials of nivolumab, we identified those who developed pneumonitis. Chest CT scans were reviewed to assess extent, distribution, and radiographic patterns of pneumonitis.
Results
Among 170 patients treated in 10 different trials of nivolumab, 20 patients (10 melanoma, 6 lymphoma, 4 lung cancer) developed pneumonitis. Five patients received nivolumab monotherapy and 15 received combination therapy. Median time from therapy initiation to pneumonitis was 2.6 months. Radiographic pattern was cryptogenic organizing pneumonia (COP) in 13, nonspecific interstitial pneumonia (NSIP) in 3, hypersensitivity pneumonitis (HP) in 2, and acute interstitial pneumonia (AIP)/acute respiratory distress syndrome (ARDS) in 2 patients. AIP/ARDS pattern had the highest grade, followed by COP, while NSIP and HP had lower grade (median Grade: 3, 2, 1, 1, respectively; p=0.006). COP pattern was most common in all tumors and treatment regimens. Most patients (17/20;85%) received corticosteroids, and 3 (15%) also required infliximab. Seven patients restarted nivolumab therapy; two of them developed recurrent pneumonitis and were successfully retreated with corticosteroids. One of the patients experienced a pneumonitis flare after completion of corticosteroid taper without nivolumab retreatment.
Conclusions
PD-1 inhibitor-related pneumonitis showed a spectrum of radiographic patterns, reflecting pneumonitis grades. COP was the most common pattern across tumor types and therapeutic regimens. Most patients were successfully treated with corticosteroids. Recurrent pneumonitis and pneumonitis flare were noted in a few patients.
Keywords: PD-1 inhibitor, pneumonitis, nivolumab, pembrolizumab, immune-related adverse event
INTRODUCTION
Immune-checkpoint inhibitor therapy has emerged as a promising treatment option for advanced cancers.(1–3) Programmed cell death (PD)-1 inhibitors are the most actively studied group of agents, and have shown marked efficacy in trials for advanced melanoma,(4–9) non-small-cell lung cancer (NSCLC),(10–14) renal cell carcinoma (RCC),(15–17) and Hodgkin lymphoma.(18) Two PD-1 inhibitors have been approved by the U.S. Food and Drug Administration (FDA) for the clinical cancer treatment, including nivolumab for advanced melanoma, NSCLC, and RCC, and pembrolizumab for melanoma and NSCLC. A combination therapy using nivolumab and ipilimumab, a CTLA-4 inhibitor, has also been approved as a treatment for advanced melanoma.(19, 20) Given the evidence for clinical efficacy in a wide spectrum of tumor types, PD-1 immune-checkpoint inhibitor therapy as monotherapy or in combination is projected to be increasingly used by oncologists.
Immune-checkpoint blockade by PD-1 inhibitors is associated with unique toxicities, termed immune-related adverse events (irAEs), which can involve different organs throughout the body.(21–23) Among the irAEs, pneumonitis is a relatively rare, but clinically serious and potentially life-threatening toxicity, and is recognized as an “event of special interest”.(2, 6) In a phase 1 trial of nivolumab in advanced solid tumors,(2) three pneumonitis-related deaths were reported. Subsequently, a phase 1 trial of nivolumab for advanced NSCLC reported three pneumonitis-related deaths,(13) and a phase 1 trial of pembrolizumab for advanced NSCLC reported one pneumonitis-related death.(12) In spite of the potentially serious outcome of PD-1 inhibitor-related pneumonitis, there have been no systematic investigations of this entity focusing on its radiographic manifestations, treatment, and follow-up. Although the incidence of PD-1 inhibitor-related pneumonitis in these trials was reported as part of the safety assessments, the description of the clinical and radiographic details have been limited and comparisons across different cohorts have not been performed because of the relatively low incidence of pneumonitis.
Several cases of PD-1 inhibitor-related pneumonitis were reported recently, describing the radiographic and clinical details of pneumonitis in the initial experiences with PD-1 inhibitors in melanoma(24) and NSCLC.(25) These cases indicated that PD-1 inhibitor-related pneumonitis may have a spectrum of radiologic manifestations that includes different radiographic patterns described in ATS/ERS classifications of interstitial pneumonias.(24, 25) Clinical courses of pneumonitis were also variable among patients; some patients required admission to the intensive care unit (ICU) and intubation, while others were treated successfully with oral corticosteroids on an outpatient basis and were able to restart their anti-PD-1 therapy without experiencing recurrent pneumonitis.(24, 25) The variability of clinical presentation and outcome of PD-1 inhibitor-related pneumonitis reported in these initial cases indicated a need for the systematic study of a larger number of cases.
The purpose of the present study is to investigate the clinical characteristics, radiographic patterns, treatment, and outcome of PD-1 inhibitor-related pneumonitis in patients treated on clinical trials of PD-1 inhibitor therapy, and to compare these characteristics among patients with different tumor types and different treatment regimens.
MATERIALS AND METHODS
Patients
Patients with advanced melanoma, lung cancer, or lymphoma who developed pneumonitis while enrolled on clinical trials using nivolumab at Dana Farber Cancer Institute were identified based on review of the clinical trial records (ClinicalTrials.gov Identifiers: NCT00730639, NCT01721746, NCT01714739, NCT01783938, NCT01928394, NCT02186249, NCT01592370, NCT02038933, NCT02038946, NCT02181738). The medical records and the imaging studies of these patients were retrospectively reviewed with an approval from the institutional review board.
Evaluation of chest CT findings of pneumonitis
Chest CT scans obtained at the time of the diagnosis of pneumonitis were reviewed by a consensus of three radiologists with expertise in thoracic and oncologic imaging (M.N., N.H.R., H.H.), as described previously.(24–27) CT findings of pneumonitis were evaluated for 1) extent in upper, middle and lower lungs (none, <5%, 5–25%,25–50%, >50%), 2) distributions in terms of (a) peripheral, diffuse, central or mixed; and (b) upper, lower, diffuse, multifocal or focal, 3) lobar involvement, and 4) specific CT findings including traction bronchiectasis, consolidation, reticular opacities, ground glass opacities (GGO), centrilobular nodularity, and honeycombing.(24–27) In each case, radiographic patterns of pneumonitis were classified referring to ATS/ERS international multidisciplinary classification of interstitial pneumonias, as 1) usual interstitial pneumonia (UIP) pattern, 2) non-specific interstitial pneumonia (NSIP) pattern, 3) cryptogenic organizing pneumonia (COP) pattern, 4) acute interstitial pneumonia (AIP)/acute respiratory distress syndrome (ARDS) pattern, 5) hypersensitivity pneumonitis (HP) pattern, and 6) not applicable, as described previously.(24–28) Follow-up chest imaging studies after the onset of pneumonitis were also reviewed to assess the resolution of the findings.
Medical record review
The toxicity grades for pneumonitis assigned during the trials according to the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE) were obtained from the records. Clinical presentations, the treatment regimen for pneumonitis, and the clinical course were obtained from the medical record.
Statistical analysis
Comparison between the groups divided according to tumor types, therapeutic regimen, and radiographic patterns of pneumonitis was performed using Fisher exact test for categorical data and Wilcoxon test for continuous data. All p values were based on a two-sided hypothesis. A p value of less than 0.05 was considered to be significant.
RESULTS
Clinical characteristics of patients with pneumonitis
Among 170 patients treated on 10 different trials of nivolumab, either alone (n=74) or in combination with other immune checkpoint inhibitors (n=96), 20 patients (11.8%) developed pneumonitis. Thirteen of these 20 patients (65%) were female, their median age was 52 (range 28–71); 5 patients received nivolumab monotherapy and 15 patients received combination therapy (with ipilimumab in 12 and with the anti-KIR (killer IgG-like receptor) antibody lirilumab in 3 patients). Ten patients had melanoma, 6 had lymphoma, and 4 had lung cancer including 3 with NSCLC and one with small-cell lung cancer (SCLC). Three patients (two lymphoma patients and a SCLC patient) had received chest radiotherapy prior to PD-1 inhibitor therapy. The cases of 3 of the melanoma patients were reported previously in the initial experience of PD-1 pneumonitis at our institution.(24) Severity of pneumonitis was Grade 1 in 5 patients (25%), Grade 2 in 10 patients (50%), and Grade 3 in 5 patients (25%). Most common symptoms were cough in 12 patients (60%) and dyspnea in 11 patients (55%). Further clinical details of each patient are summarized in Table 1.
Table 1.
Clinical characteristics of 20 patients with PD-1 pneumonitis
| Pt | Tumor | Sex | Age | Agents | Treatment regimen and drug dosage | Time to the onset of pneumonitis (month) | Grade | Symptoms |
|---|---|---|---|---|---|---|---|---|
| 1 | Melanoma | M | 58 | Nivolumab | Nivolumab (1 mg/kg q2w) | 1.7 | 2 | Cough |
| 2 | Melanoma | F | 38 | Nivolumab | Nivolumab (3 mg/kg q2w) | 3.6 | 3 | Dyspnea, hypoxia |
| 3 | Melanoma | M | 70 | Nivolumab & ipilimumab | Nivolumab (3 mg/kg, q2w) × 6 then ipilimumab (3 mg/kg, q3w) × 4 | 5.6 | 3 | Cough, dyspnea, hypoxia, subacute fever |
| 4 | Melanoma | F | 66 | Nivolumab & ipilimumab | Nivolumab (3 mg/kg, q2w) × 6 then ipilimumab (3 mg/kg, q3w) × 4 | 5.4 | 1 | None |
| 5 | Melanoma | F | 40 | Nivolumab & ipilimumab | Nivolumab (3 mg/kg, q2w) × 6 then ipilimumab (3 mg/kg, q3w) × 4 | 7.3 | 2 | Cough, dyspnea |
| 6 | Melanoma | M | 64 | Nivolumab & ipilimumab | Nivolumab (3 mg/kg, q2w) × 6 then ipilimumab (3 mg/kg, q3w) × 4 | 3.7 | 2 | Cough, dyspnea |
| 7 | Melanoma | M | 57 | Nivolumab & ipilimumab | Nivolumab (1 mg/kg) & ipilimumab (3 mg/kg) q3w ×4, then nivolumab alone (3mg/kg, q2w) | 2.7 | 2 | Cough, dyspnea |
| 8 | Melanoma | F | 47 | Nivolumab & ipilimumab | Nivolumab (1 mg/kg) & ipilimumab (3 mg/kg) q3w ×4, then nivolumab alone (3mg/kg, q2w) | 2.4 | 1 | None |
| 9 | Melanoma | F | 35 | Nivolumab & ipilimumab | Nivolumab (1 mg/kg) & ipilimumab (3 mg/kg) q3w ×4, then nivolumab alone (3mg/kg, q2w) | 1.6 | 3 | Cough, dyspnea, fever |
| 10 | Melanoma | F | 52 | Nivolumab & ipilimumab | Nivolumab (1 mg/kg) & ipilimumab (3 mg/kg) q3w ×4, then nivolumab alone (3mg/kg, q2w) | 2.7 | 1 | None |
| 11 | Lung (Adenoca) | F | 56 | Nivolumab | Nivolumab (10 mg/kg, q2w) | 1.4 | 3 | Cough, dyspnea, fever |
| 12 | Lung (Adenoca) | F | 40 | Nivolumab | Nivolumab (1 mg/kg q2w) | 1.2 | 1 | None |
| 13 | Lung (Adenoca) | F | 52 | Nivolumab & lirilumab | Nivolumab (3 mg/kg, q2w) & Lirilumab (3 mg/kg, q4w) | 1.1 | 2 | Dyspnea, hypoxia |
| 14 | Lung (SCLC) | M | 59 | Nivolumab | Nivolumab 3 mg/kg q2w | 0.5 | 3 | Dyspnea, hypoxia |
| 15 | Lymphoma (Hodgkin) | F | 30 | Nivolumab & ipilimumab | Nivolumab (3mg/kg) & ipilimumab (1mg/kg) q3w × 4, then nivolumab (3 mg/kg q2w) | 11.5 | 2 | Cough |
| 16 | Lymphoma (Hodgkin) | F | 33 | Nivolumab & ipilimumab | Nivolumab (3mg/kg) &ipilimumab (1mg/kg) q3w × 4, then nivolumab (3 mg/kg q2w) | 1.4 | 2 | Cough, dyspnea |
| 17 | Lymphoma (Hodgkin) | F | 71 | Nivolumab & ipilimumab | Nivolumab (3mg/kg) & ipilimumab (1mg/kg) q3w × 4, then nivolumab (3 mg/kg q2w) | 1.4 | 2 | Cough, dyspnea |
| 18 | Lymphoma (T cell) | F | 62 | Nivolumab & ipilimumab | Nivolumab (3mg/kg) & ipilimumab (1mg/kg) q3w × 4, then nivolumab (3 mg/kg q2w) | 4.6 | 2 | Cough |
| 19 | Lymphoma (Hodgkin) | M | 30 | Nivolumab & lirilumab | Nivolumab (3mg/kg, q2w) & lirilumab (3 mg/kg, q4w) | 4.1 | 1 | None |
| 20 | Lymphoma (Hodgkin) | M | 28 | Nivolumab & lirilumab | Nivolumab (3mg/kg, q2w) & lirilumab (3 mg/kg, q4w) | 0.8 | 2 | Cough, fever |
Adecnoca: Adenocarcinoma
SCLC: small-cell lung cancer
Median time from treatment initiation to the development of pneumonitis was 2.6 months (range: 0.5–11.5) in the whole cohort of 20 patients; of note it was shorter in the 4 lung cancer patients compared to the 16 patients with melanoma and lymphoma (median time to pneumonitis: 1.1 vs. 3.1 months, respectively; p=0.008).
CT findings and radiographic patterns of pneumonitis
Table 2 summarizes the CT characteristics of pneumonitis during nivolumab therapy in all 20 patients. The extent of lung involvement by pneumonitis was highest in the lower lungs, followed by the middle lungs, and was lowest in the upper lungs, with a median extent score of 3 (25–50%) for the lower, 2.5 for the middle, and 2 (5–25%) for the upper lungs. The most common distribution of CT findings of pneumonitis was mixed and multifocal (n=8), followed by peripheral and lower (n=4) and diffuse (n=4). In 15 patients (75%), all lobes of the lung including the lingula were involved. Among the specific CT findings, GGOs were present in all 20 patients, with reticular opacities in 19 and with consolidations in 12 patients. Centrilobular nodularity was present in 3 patients. Traction bronchiectasis was noted in 2 patients. Pneumonitis in lung cancer patients had more extensive involvement on CT than others (p=0.007).
Table 2.
CT findings and radiographic patterns of PD-1 pneumonitis
| Pt | Extent | Distribution | Lobar involvement | Specific CT findings | Radiographic pattern | ||
|---|---|---|---|---|---|---|---|
| Upper | Middle | Lower | |||||
| 1 | 5–25% | 5–25% | 25–50% | Peripheral and lower | All lobes | GGOs, reticular opacities, consolidations | NSIP |
| 2 | >50% | >50% | >50% | Diffuse | All lobes | GGOs, reticular opacities, consolidations, traction BE, centrilobular nodularity | AIP/ARDS |
| 3 | 25–50% | >50% | >50% | Diffuse | All lobes | GGOs, reticular opacities, consolidations, traction BE | AIP/ARDS |
| 4 | None | <5% | 5–25% | Mixed and lower | RLL | GGOs, reticular opacities | NSIP |
| 5 | 5–25% | 25–50% | >50% | Peripheral and lower | All lobes | GGOs, reticular opacities, consolidations | COP |
| 6 | 5–25% | 5–25% | 5–25% | Mixed and multifocal | LUL, lingual, LLL | GGOs, reticular opacities, consolidations, | COP |
| 7 | 5–25% | 5–25% | <5% | Mixed and multifocal | All lobes | GGOs, reticular opacities | COP |
| 8 | >50% | 25–50% | 25–50% | Diffuse | All lobes | GGOs, reticular opacities | HP |
| 9 | 5–25% | 5–25% | 25–50% | Peripheral and lower | All lobes | GGOs, reticular opacities, consolidations | COP |
| 10 | <5% | 5–25% | 25–50% | Peripheral and lower | All lobes | GGOs, reticular opacities, consolidations | NSIP |
| 11 | 25–50% | 25–50% | >50% | Mixed and multifocal | All lobes | GGOs, reticular opacities, | COP |
| 12 | >50% | >50% | >50% | Diffuse | All lobes | GGOs, centrilobular nodularity | HP |
| 13 | >50% | >50% | 25–50% | Mixed and upper | All lobes | GGOs, reticular opacities, | COP |
| 14 | 25–50% | 25–50% | >50% | Mixed and multifocal | All lobes | GGOs, reticular opacities, | COP |
| 15 | 25–50% | 25–50% | 25–50% | Peripheral and multifocal | All lobes | GGOs, reticular opacities, consolidations | COP |
| 16 | 5–25% | 5–25% | 25–50% | Mixed and multifocal | All lobes | GGOs, reticular opacities, consolidations | COP |
| 17 | <5% | <5% | 5–25% | Mixed and lower | RLL, LLL | GGOs, reticular opacities, consolidations | COP |
| 18 | 5–25% | 5–25% | >50% | Mixed and multifocal | All lobes | GGOs, reticular opacities, consolidations | COP |
| 19 | None | 5–25% | 5–25% | Mixed and multifocal | LLL | GGOs, reticular opacities, consolidations | COP |
| 20 | 5–25% | 25–50% | 25–50% | Mixed and multifocal | RUL, RML, LLL | GGOs, reticular opacities, centrilobular nodularity | COP |
GGO: ground-glass opacities
NSIP: non-specific interstitial pneumonia
AIP/ARDS: acute interstitial pneumonia/acute respiratory distress syndrome
COP: cryptogenic organizing pneumonia
HP: hypersensitivity pneumonitis
RUL: right upper lobe
RLL: right lower lobe
LUL: left upper lobe
LLL: left lower lobe
The overall radiographic pattern of pneumonitis on chest CT was most commonly COP pattern noted in 13 patients (65%)(Fig. 1A–B), followed by NSIP pattern in 3 (15%)(Fig. 1C–D), HP pattern in 2 (10%)(Fig. 1E–F), and AIP/ARDS pattern in 2 patients (10%)(Fig. 1G–H). The radiographic patterns were associated with the toxicity grades of pneumonitis; AIP/ARDS pattern had the highest grade (median grade: 3), followed by COP pattern (median grade: 2), and NSIP and HP patterns had lower grade (median 1 for both)(p=0.006).
Fig. 1.
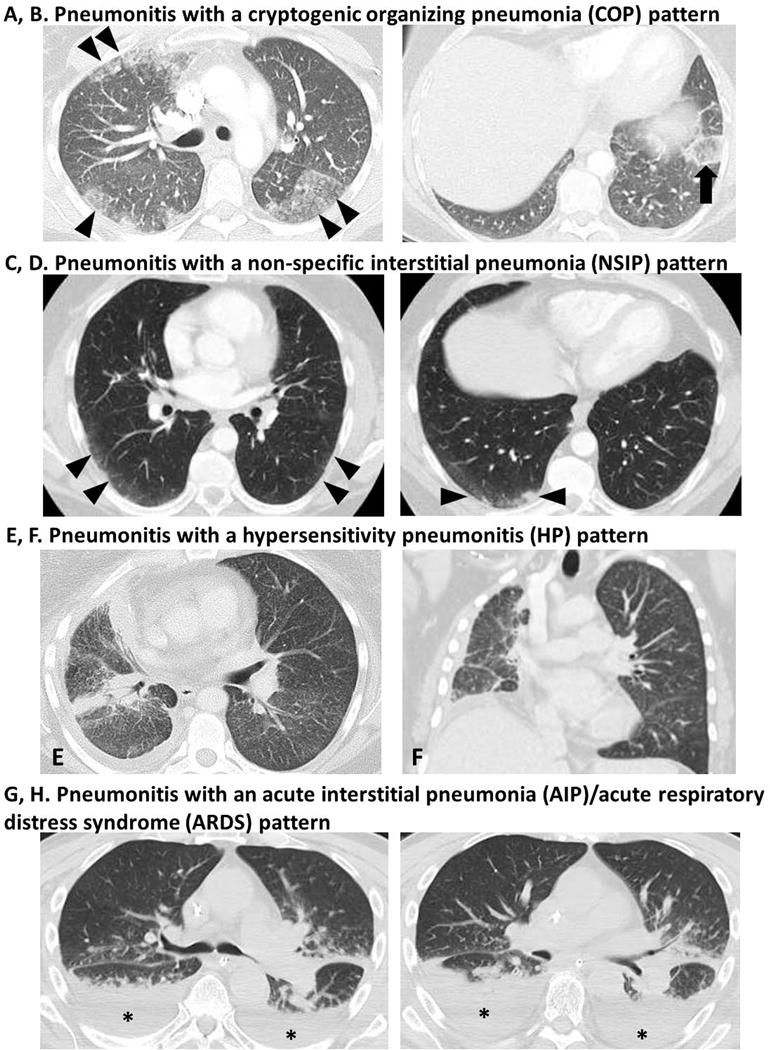
Spectrum of radiographic manifestations of PD-1 inhibitor-related pneumonitis.
A, B. Pneumonitis with a COP pattern in a 30-year-old female with Hodgkin lymphoma treated with nivolumab and ipilimumab combination therapy (Patient 15).
CT scan of the chest at 11.5 months of therapy demonstrated a development of ground-glass and reticular opacities and consolidations involving both lungs with a multifocal distribution (arrowheads, A), representing a COP pattern. One of the involved areas in the left lower lobe demonstrated a “reversed halo” sign (arrow, B) with central GGO surrounded by dense air-space consolidation of crescentic shape, which has been reported as a radiographic manifestation of COP.
C, D. Pneumonitis with a NSIP pattern in a 58-year-old male with melanoma treated with nivolumab monotherapy (Patient 1).
Chest CT scan at 1.7 months of therapy demonstrated new ground glass and reticular opacities and consolidations (arrowheads, C, D) indicative of a NSIP pattern.
E, F. Pneumonitis with a HP pattern in a 40-year-old female with lung adenocarcinoma treated with nivolumab monotherapy (Patient 12).
Chest CT scan at 1.2 months of therapy demonstrated new diffuse GGOs and centrilobular nodularity in both lungs, indicative of a HP pattern of pneumonitis. Note that the consolidations and interlobular septal thickening in the right lung demonstrate tumor involvement by lung cancer, which were present since the baseline scan.
G, H. Pneumonitis with an AIP/ARDS pattern in a 70-year-old man with melanoma treated with sequentially administered nivolumab and ipilimumab combination therapy (Patient 3).
Chest CT scan at 5.6 months of therapy demonstrated ground-glass and reticular opacities, consolidations and traction bronchiectasis as well as pleural effusions (asterisks), involving both lungs.
COP pattern was the most common pattern in all tumor types (3/4 in lung, 6/6 in lymphoma, 4/9 in melanoma), and in both monotherapy (2/5) and combination therapy (11/15). No significant differences were observed in the radiographic patterns between monotherapy and combination therapy (p=0.30), or among different tumor types (p=0.19).
Treatment for pneumonitis and follow-up
The details of the treatment regimen for pneumonitis and the clinical course are shown in Table 3. Nivolumab therapy was held at the time of pneumonitis in all patients. The majority (17/20; 85%) of the patients received corticosteroids as a treatment for pneumonitis. Three patients (15%) also received infliximab in addition to corticosteroids. Three patients received no corticosteroids for pneumonitis; of these, one patient was on hydrocortisone 15 mg daily for adrenal insufficiency that had been previously diagnosed. Seven patients were admitted to the hospital for treatment of pneumonitis, including 3 melanoma patients and all 4 lung cancer patients. Two of the melanoma patients were admitted to the intensive care unit (ICU), and one patient required intubation during ICU admission.
Table 3.
Treatment for pneumonitis and follow-up course
| Pt | Treatment for pneumonitis# | Admission for pneumonitis | Outcome of pneumonitis treatment | Re-initiation of nivolumab therapy | Recurrent pneumonitis | Details of follow-up and retreatment |
|---|---|---|---|---|---|---|
| 1 | Oral prednisone taper starting with 120 mg daily | No | Clinical and radiographic improvement | Yes | No | Restarted nivolumab and no recurrent pneumonitis for 46 months |
| 2 | IV methylprednisolone taper 240mg daily, IV infliximab (5 mg/kg), ICU admission | Yes | Referred for hospice care and died | No | No | Referred for hospice care and died |
| 3 | IV methylprednisolone taper 150mg daily, IV infliximab (5 mg/kg), ICU admission, intubation | Yes | Clinical and radiographic improvement | No | No | Follow-up without therapy; no recurrent pneumonitis for 26 months |
| 4 | None◊ | No | Radiographic improvement | Yes | No | Restarted maintenance nivolumab monotherapy (3mg/kg, q2w) with no recurrent pneumonitis for 22 months |
| 5 | None | No | Clinical and radiographic improvement | No | No | Started on next systemic therapy |
| 6 | Oral prednisone 120mg daily | No | Clinical and radiographic improvement | No | No | Started on next systemic therapy |
| 7 | Oral prednisone taper starting at 80 mg | No | Clinical and radiographic improvement | Yes | Yes | Restarted nivolumab (3mg/kg, q2w) and developed recurrent pneumonitis after receiving 4 doses of nivolumab* |
| 8 | Oral prednisone taper starting at 100 mg | No | Radiographic improvement | No | No | Follow-up without therapy; no recurrent pneumonitis for 3 months |
| 9 | Oral steroid taper at outside institution▲ | Yes | Clinical and radiographic improvement | No | No | Follow-up without therapy; no recurrent pneumonitis for 7 months |
| 10 | None | No | Radiographic improvement | No | No | Started on next systemic therapy |
| 11 | IV methylprednisolone 120 mg, then oral prednisone taper starting at 60 mg, and IV infliximab (5 mg/kg) | Yes | Clinical and radiographic improvement | No | No | Referred for palliative care |
| 12 | Oral prednisone taper starting at 60 mg daily | Yes | No imaging before next therapy | No | No | Started on next systemic therapy |
| 13 | IV methylprednisolone 250 mg, then oral dexamethasone 12 mg daily and prednisone taper starting at 60 mg daily | Yes | Clinical and radiographic improvement | No | No | Referred for palliative care |
| 14 | IV methylprednisolone 140 mg daily, then oral prednisone taper starting at 140 mg daily | Yes | Clinical and radiographic improvement | No | No | Started on next systemic therapy |
| 15 | Oral prednisone taper starting at 60 mg daily | No | Clinical and radiographic improvement | Yes | No | Restarted nivolumab monotherapy with no recurrent pneumonitis for 5 months |
| 16 | Oral prednisone taper starting at 100 mg daily | No | Clinical and radiographic improvement | Yes | Yes | Restarted nivolumab & ipilimumab and received 2 doses of nivolumab & ipilimumab, and 2 doses of nivolmab, developed recurrent pneumonitis** |
| 17 | Oral prednisone taper starting at 70 mg daily | No | Clinical and radiographic improvement | No | No | Follow-up without therapy without recurrent pneumonitis for 8 months |
| 18 | Oral prednisone taper starting at 40 mg daily | No | Clinical and radiographic improvement | No | No | Started on next systemic therapy |
| 19 | Oral prednisone taper starting at 60 mg daily | No | Radiographic improvement | Yes | No | Restarted nivolumab & lirilumab with no recurrent pneumonitis for 2 months |
| 20 | Oral prednisone taper starting at 80 mg daily | No | Clinical and radiographic improvement | Yes | No | Restarted nivolumab & lirilumab with no recurrent pneumonitis for 3 months |
Nivolumab therapy was held at the time of pneumonitis in all patients.
Nivolumab was held and the patient was treated again with prednisone taper and improved; followed without rechallenge or therapy for 4 months.
Nivolumab was held and the patient was again treated with prednisone taper starting at 100 mg with subsequent improvement; however, the patient experienced two episodes of pneumonitis flare, where a similar pattern of pneumonitis recur after the completion of corticosteroid taper without retreatment of nivolumab or other systemic therapy. (See Fig. 5)
The patient has been on hydrocortisone 15 mg/day for adrenal insufficiency
No further treatment details are available for this patient treated at the outside institution
During the treatment and follow-up course, 14 patients with grade 2 or above had clinical and radiographic improvement, and 4 patients with grade 1 pneumonitis without symptoms had radiographic improvement. One patient with grade 1 pneumonitis started the next systemic therapy without further follow-up CT. One patient was referred to hospice care without follow-up CT, and passed away.
Nivolumab therapy was restarted in 7 patients (35%), including 3 melanoma and 4 lymphoma patients; of these 7 patients, 5 patients had COP pattern and 2 had NSIP pattern. One patient has received nivolumab monotherapy and 6 had received combination therapy at the time of pneumonitis. During retreatment, 4 patients received nivolumab monotherapy (including 3 patients who restarted on maintenance monotherapy after the initial doses of combination regimen) and 3 patients restarted combination therapy (nivolumab and ipilimumab in 1, nivolumab and lirilumab in 2)(Table 3).
Among the 7 patients with retreatment, recurrent pneumonitis was noted in 2 patients. One of them was a melanoma patient restarted on maintenance nivolumab monotherapy, and developed recurrent pneumonitis after 4 doses of nivolumab, which was successfully treated with corticosteroid taper without further nivolumab retreatment or recurrence for 4 months after the second episode. The other patient was a lymphoma patient who restarted on nivolumab and ipilimumab therapy, and developed recurrent pneumonitis after receiving 2 doses of nivolumab and ipilimumab, and 2 doses of nivolumab (Fig. 2). Nivolumab was again held and the patient was again treated with prednisone taper with subsequent improvement; one month after the completion of the 2-month course of the prednisone taper, the patient again developed pneumonitis without nivolumab retreatment or any other systemic therapy, indicating a “pneumonitis flare” phenomenon. Another course of prednisone taper was given for 2.7 month. After 2 weeks from the completion of the prednisone taper, the patient again experienced a pneumonitis flare, which was histologically confirmed (Fig. 3). Prednisone taper at 60 mg daily was again initiated, with subsequent clinical improvement.
Fig. 2.
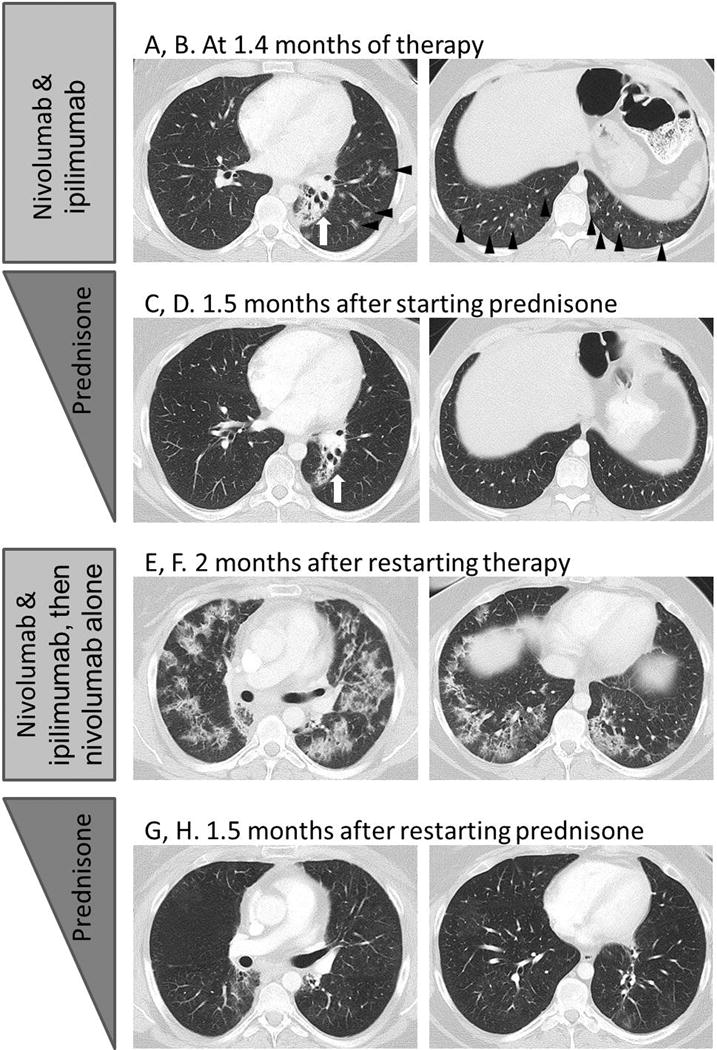
Pneumonitis with a COP pattern in a 33-year-old female with Hodgkin lymphoma treated with nivolumab and ipilimumab combination therapy (Patient 16), with a recurrence during retreatment and two episodes of pneumonitis flare after completion of corticosteroid taper.
A, B. CT scan of the chest at 1.4 months of therapy demonstrated ground-glass and reticular opacities and consolidations with multifocal distribution, indicative of a COP pattern of pneumonitis (arrowheads). Left perihilar opacity and traction bronchiectasis are due to prior radiation therapy (arrows).
C, D. The patient was treated with oral prednisone taper, and the findings have resolved on the follow-up scan performed 1.5 month later.
E, F. The patient restarted therapy and received 2 doses of nivolumab and ipilimumab and 2 doses of nivolmab monotherapy, then developed recurrent pneumonitis after 2 months since restarting therapy. The scan at the time of recurrent pneumonitis demonstrated similar findings with muitifocal ground-glass and reticular opacities and consolidations, again representing a COP pattern. The findings were more extensive than the first episode.
G, H. Nivolumab was held and the patient was treated again with prednisone taper for pneumonitis, with subsequent improvement.
Fig. 3.
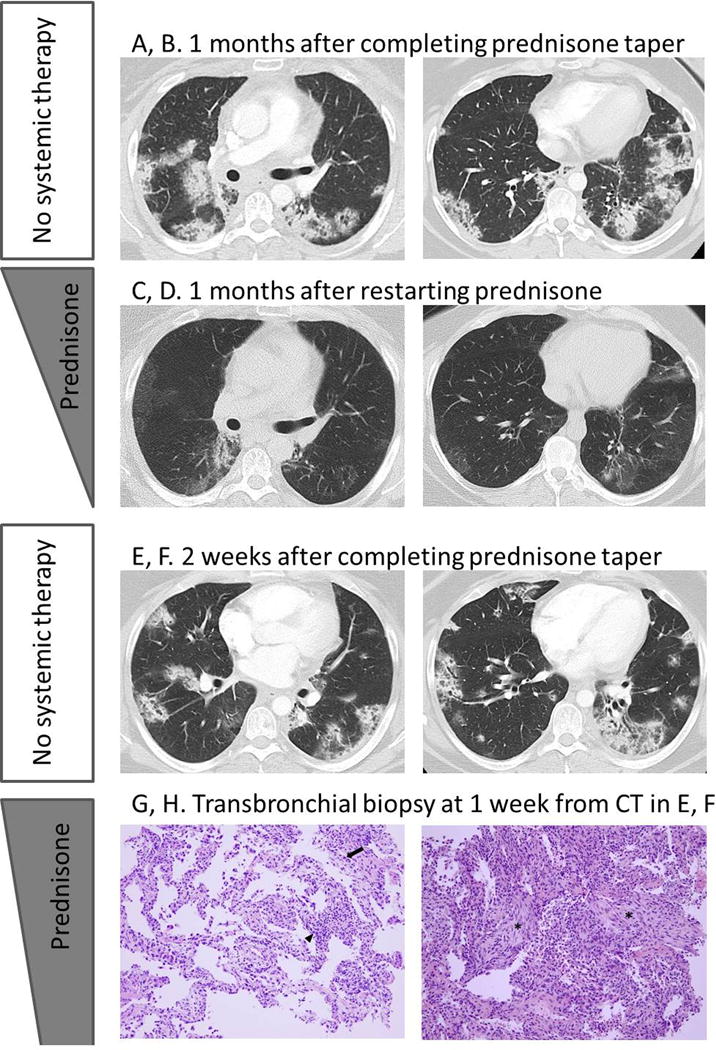
Pneumonitis with a COP pattern in a 33-year-old female with Hodgkin lymphoma treated with nivolumab and ipilimumab combination therapy (Patient 16), with a recurrence during retreatment and two episodes of pneumonitis flare after completion of corticosteroid taper.
A, B. The patient completed 2 months of corticosteroid taper and after one month, she experienced another episode of pneumonitis with a very similar radographic pattern, without nivolumab retreatment or other systemic therapy, indicating a pneumonitis flare.
C, D. Another course of corticosteroid taper was given and with subsequent improvement.
E, F. The 2.7-month course of corticosteroid taper was completed and after 2 weeks, the patient again developed a pneumonitis flare with a similar radiographic pattern as the prior episodes.
G, H. The sampled fragments of lung obtained by transbronchial biopsies showed interstitial pneumonitis evolving to organizing pneumonia. Findings included lymphocyte-predominant interstitial pneumonitis (arrowhead, O, H&E stain, 200X)with rare eosinophils (arrow, O), and areas of organizing pneumonia with fibroblast plugs and foamy macrophages filling the airspaces (asterisks, P, H&E stain, 200X). No tumor cells, microorganisms, or viral cytopathic changes were identified.
The patient started another course of prednisone taper with subsequent clinical improvement, and is schedule for a follow-up CT scan.
DISCUSSION
Among the patients who developed PD-1 inhibitor-related pneumonitis during nivolumab therapy for advanced cancers including melanoma, lung cancer, and lymphoma, a COP pattern was the most common radiographic pattern of pneumonitis in all tumor types and therapeutic regimens. The radiographic patterns were associated with the toxicity grades of pneumonitis. Most patients were successfully treated with corticosteroids. Seven patients (35%) restarted nivolumab therapy, with recurrent pneumonitis noted in 2 patients during retreatment. To our knowledge, this is the first study that systematically characterized a spectrum of the radiographic patterns of PD-1 inhibitor-related pneumonitis according to ATS/ERS classification, and provided treatment and follow-up details in advanced cancer patients treated with nivolumab.
The distribution of the toxicity grades in our cohort is similar to the published trial reports in that more patients had Grade ≤ 2 than Grade ≥ 3.(2, 5, 7, 19, 20, 29) Distributions between Grade 1 and Grade 2 are not described in most trial reports because toxicities are categorized as “all grades” and “grade 3 or above” in trial reports. Most patients (75%) were symptomatic with cough and dyspnea, which is similar to the prior clinical reports of the entity.(24, 25)
Time from initiation of therapy to the development of pneumonitis had a wide range (0.5–11.5 months), indicating an importance of careful observation and follow-up for signs and symptoms of pneumonitis throughout treatment. Shorter time to onset of pneumonitis in lung cancer compared to melanoma and lymphoma may be due to a higher pulmonary tumor burden among lung cancer patients, which can result in an earlier onset of respiratory symptoms. In addition, clinicians may have a lower threshold for performing additional chest CT scans in lung cancer patients. In a prior report of two cases of PD-1 pneumonitis in advanced NSCLC, pneumonitis was also noted during early course of nivolumab therapy (at 1 month of therapy in one patient and at 2 months in the other patient).(25) These observations indicate a trend of early onset of PD-1 pneumonitis among lung cancer patients which can be further studied in a larger cohort.
The CT characteristics of pneumonitis showed a higher extent of involvement in lower lobes, which is often seen in pneumonitis related to other molecular targeting agents including mTOR inhibitors.(26, 27) Mixed and multifocal distribution was most common and all lung lobes plus the lingula were involved in 75% of the patients, reflecting a relatively extensive lung involvement by PD-1 inhibitor-related pneumonitis as noted in the prior reports.(24, 25) Among the specific CT findings, GGOs (n=20), reticular opacities (n=18), and consolidation (n=12) were most commonly noted, as in most of the cases with drug-related pneumonitis during immune-checkpoint inhibitor therapies and molecular targeting therapies.(22, 24–27, 30) The extent of involvement was higher in lung cancer patients, which goes along with the trial reports of PD-1 inhibitors in NSCLC describing high grade pneumonitis with serious consequence, including pneumonitis-related deaths in phase 1 trials.(12, 13)
Radiographic pattern of pneumonitis according to ATS/ERS classification was most frequently a COP pattern, noted in 65% of the patients, without significant differences among different tumor types or therapeutic regimen. COP pattern was seen in the previous report of commercially-treated NSCLC patients with nivolumab-related pneumonitis,(25) and was also the most common pattern for mTOR inhibitor-related pneumonitis in advanced neuroendocrine tumors and Waldenstrom macroglobulinemia.(26, 27) However, other patterns were noted in the remaining patients in the present study, including NSIP, HP, and AIP/ARDS patterns, demonstrating a wide spectrum of radiographic presentation of PD-1 pneumonitis. Notably, these radiographic patterns were associated with the NCI/CTCAE grade of pneumonitis, where the grades were highest in AIP/ARDS pattern, followed by COP, and lowest in NSIP and HP patterns. The results indicate the value of the radiographic pattern-based approach in categorizing and prognosticating PD-1 inhibitor-related pneumonitis.
Treatment and follow-up course of PD-1 inhibitor-related pneumonitis are an important and challenging issue in the current immuno-oncology practice. Nivolumab therapy was held at the diagnosis of pneumonitis in all patients; most patients were treated with corticosteroids, with a median time of corticosteroid therapy of 6.1 weeks. Varying doses of oral and intravenous corticosteroids were used, which reflects a spectrum of clinical severity of PD-1 pneumonitis, and a need for consensus as to the optimal treatment algorithm. All 4 lung cancer patients were admitted at the time of pneumonitis treatment, indicating a higher clinical severity and concerns in this subgroup of patients. All lung cancer patients have been heavily treated prior to PD-1 inhibitor therapy, with 3–5 lines of systemic therapy including platinum-based chemotherapy and tyrosine kinase inhibitors in 3 NSCLC patients, and with platinum-based chemotherapy plus concurrent chest radiotherapy in a SCLC patient, which may have also contributed to the clinical severity of pneumonitis.
In most patients, clinical and radiographic improvements were noted after treatment, indicating that this entity, although potentially serious, is treatable if diagnosed and managed appropriately. The observation emphasizes the importance of timely recognition, accurate diagnosis, and early intervention in the setting of PD-1 inhibitor-related pneumonitis. Bronchoscopy and bronchoalveolar lavage (BAL) were performed at the time of pneumonitis in 4 patients (1 melanoma, 2 NSCLC, and 1 lymphoma patients), and demonstrated acute inflammation in 2 patients, reactive pneumocytes in one patient, and malignant cells due to underlying lung metastasis that has been present before starting PD-1 inhibitor therapy in one NSCLC patient; this patient’s pneumonitis was radiographically distinct from underlying lung metastasis and improved after corticosteroid treatment. Given the limited available data of BAL in PD-1 inhibitor-related pneumonitis, as well as its sensitivity and specificity in diagnosing this entity, its exact role in this context remains to be established.
Retreatment with anti-PD1 therapy in patients with pneumonitis after nivolumab is another challenging issue with very limited data. Of the 7 patients who restarted nivolumab therapy, 2 patients developed recurrent pneumonitis, while pneumonitis did not reoccur in the remaining 5 patients at the time of analysis with a follow-up time ranging 2–46 months. Further studies are needed to effectively identify patients who can safely restart PD-1 therapy after experiencing pneumonitis. Both patients with recurrent pneumonitis were successfully treated with corticosteroids, again demonstrating the steroid responsive nature of the entity in the setting of increased awareness and early recognition. However, one of the 2 patients subsequently developed “pneumonitis flare”, where pneumonitis recurred after completing corticosteroid taper in the absence of nivolumab retreatment, as seen in a case described in the prior report among NSCLC patients.(25) Notably, the patient in the present study experienced two episodes of pneumonitis flare, which may suggest a recurrent nature of the phenomenon and thus indicate another clinical challenge as to when to complete corticosteroid therapy for pneumonitis. Although the exact incidence and further characteristics of a pneumonitis flare remains to be systematically investigated, the histologic findings consistent with pneumonitis obtained during the flare episode in this patient provide further support of this unique phenomenon among patients treated with PD-1 inhibitors.
The limitations of the present study include a relatively small number of patients with PD-1 inhibitor-related pneumonitis treated in a single institution. However, to our knowledge, this is the first report of systematic investigation focusing on clinical and radiographic details of this entity. Retrospective design for the imaging review is a limitation, however, patients were treated in clinical trials and thus prospectively assessed and diagnosed for PD-1 inhibitor-related pneumonitis. The treatment regimen included nivolumab monotherapy and combination therapy, which is a reflection of the heterogeneous nature of the trial designs. The combination regimen only included those with other immune-checkpoint inhibitors (anti-CTLA-4 and anti-KIR), and did not include cytotoxic chemotherapy or targeted agents, in order to allow the study to focus on pneumonitis noted as an irAE. The present study focused on the clinical and radiographic description of pneumonitis, and the assessment of risk factors and predictors of pneumonitis were not performed. Of note, 3 of the 20 patients had prior chest radiotherapy, including a lymphoma patient who developed recurrent pneumonitis and two episodes of pneumonitis flare. Further studies are needed to determine the impact of prior chest radiotherapy on the development, severity, and treatment outcome of PD-1 inhibitor-related pneumonitis.
In conclusion, PD-1 inhibitor-related pneumonitis showed a spectrum of radiographic patterns, which were associated with toxicity grades. Most cases were responsive to corticosteroids and one-third of the patients were able to restart nivolumab therapy, though a few patients experienced recurrent pneumonitis during retreatment. These observations emphasize the importance of increased awareness of the entity for the early diagnosis and treatment. The wide spectrum of radiographic manifestations and complex clinical courses noted in some of the cases provide additional diagnostic and management challenges in the clinical setting, which calls for a multidisciplinary approach using expertise from oncology, radiology, pulmonology, and pathology to optimize patient care. Future studies in larger cohorts are needed to identify risk factors and early markers for pneumonitis development and recurrence, and to establish optimal management guidelines for this entity.
Translational Relevance.
PD-1 inhibitor-related pneumonitis is a clinically serious and potentially life-threatening toxicity, resulting in pneumonitis-related deaths in phase I trials, and is recognized as an “event of special interest”; however, little has been known about the clinical and radiographic details of the entity. The present study systematically investigated the clinical characteristics, radiographic patterns, treatment and outcome of pneumonitis in patients treated in trials of PD-1 inhibitors, and characterized a spectrum of radiographic patterns of pneumonitis that were associated with toxicity grades. Most cases were responsive to corticosteroids and one-third of the patients were able to restart PD-1 inhibitor therapy, though a few patients experienced recurrent pneumonitis during retreatment. The results of the present study are directly relevant to the current practice of oncology with increasing use of immune-checkpoint inhibitors, meet the urgent needs of the community to advance knowledge of this serious toxicity, and provide a basis for further studies.
Acknowledgments
The investigator, M. Nishino, was supported by 5K23CA157631 (NCI).
Footnotes
Conflict of Interest:
Nishino: Consultant to Bristol-Myers Squibb, Toshiba Medical Systems, WorldCare Clinical; Research grant from Merck Investigator Studies Program.
Ramaiya: Nothing to disclose
Awad: Consultant to AstraZeneca, AbbVie, Boehringer-Ingelheim, Merck, Pfizer, Genentech. Research grant from the Conquer Cancer Foundation of the American Society of Clinical Oncology; and the International Association for the Study of Lung Cancer
Sholl: Scientific advisory board for Genentech
Maattala: Nothing to disclose
Taibi: Nothing to disclose
Hatabu: Research support from Canon Inc, Toshiba Medical systems, AZE Inc., Konica-Minolta inc.; Consultant to Toshiba Medical systems
Ott: Dr. Ott has served as a consultant to Bristol-Myers Squibb and has received clinical trial support from Bristol-Myers Squibb and Merck.
Armand: Dr. Armand has served as a consultant to Bristol-Myers Squibb, Merck, and Infinity Pharmaceuticals, and has received clinical trial support from Bristol-Myers Squibb, Merck, Tensha Therapeutics, Sequenta, Otsuka, and Sigma-Tau.
Hodi: Dr. Hodi has served as a non-paid consultant to Bristol-Myers Squibb and has received clinical trial support from Bristol-Myers Squibb, advisor and clinical trial support from Merck, and advisor and clinical trial support from Genentech, consultant to Novartis and Amgen.
References
- 1.Brahmer JR, Drake CG, Wollner I, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. 2010;28:3167–3175. doi: 10.1200/JCO.2009.26.7609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. N Engl J Med. 2012;366:2443–2454. doi: 10.1056/NEJMoa1200690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363:711–723. doi: 10.1056/NEJMoa1003466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hamid O, Robert C, Daud A, et al. Safety and tumor responses with lambrolizumab (anti-PD-1) in melanoma. N Engl J Med. 2013;369:134–144. doi: 10.1056/NEJMoa1305133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Robert C, Ribas A, Wolchok JD, et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: a randomised dose-comparison cohort of a phase 1 trial. Lancet. 2014;384:1109–1117. doi: 10.1016/S0140-6736(14)60958-2. [DOI] [PubMed] [Google Scholar]
- 6.Topalian SL, Sznol M, McDermott DF, et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J Clin Oncol. 2014;32:1020–1030. doi: 10.1200/JCO.2013.53.0105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ribas A, Puzanov I, Dummer R, et al. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): a randomised, controlled, phase 2 trial. Lancet Oncol. 2015;16:908–918. doi: 10.1016/S1470-2045(15)00083-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Robert C, Schachter J, Long GV, et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N Engl J Med. 2015;372:2521–2532. doi: 10.1056/NEJMoa1503093. [DOI] [PubMed] [Google Scholar]
- 9.Weber JS, D’Angelo SP, Minor D, et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015;16:375–384. doi: 10.1016/S1470-2045(15)70076-8. [DOI] [PubMed] [Google Scholar]
- 10.Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N Engl J Med. 2015;373:1627–1639. doi: 10.1056/NEJMoa1507643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Brahmer J, Reckamp KL, Baas P, et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N Engl J Med. 2015;373:123–135. doi: 10.1056/NEJMoa1504627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Garon EB, Rizvi NA, Hui R, et al. Pembrolizumab for the treatment of non-small-cell lung cancer. N Engl J Med. 2015;372:2018–2028. doi: 10.1056/NEJMoa1501824. [DOI] [PubMed] [Google Scholar]
- 13.Gettinger SN, Horn L, Gandhi L, et al. Overall Survival and Long-Term Safety of Nivolumab (Anti-Programmed Death 1 Antibody, BMS-936558, ONO-4538) in Patients With Previously Treated Advanced Non-Small-Cell Lung Cancer. J Clin Oncol. 2015;33:2004–2012. doi: 10.1200/JCO.2014.58.3708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rizvi NA, Mazieres J, Planchard D, et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): a phase 2, single-arm trial. Lancet Oncol. 2015;16:257–265. doi: 10.1016/S1470-2045(15)70054-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McDermott DF, Drake CG, Sznol M, et al. Survival, Durable Response, and Long-Term Safety in Patients With Previously Treated Advanced Renal Cell Carcinoma Receiving Nivolumab. J Clin Oncol. 2015;33:2013–2020. doi: 10.1200/JCO.2014.58.1041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Motzer RJ, Escudier B, McDermott DF, et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N Engl J Med. 2015;373:1803–1813. doi: 10.1056/NEJMoa1510665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Motzer RJ, Rini BI, McDermott DF, et al. Nivolumab for Metastatic Renal Cell Carcinoma: Results of a Randomized Phase II Trial. J Clin Oncol. 2015;33:1430–1437. doi: 10.1200/JCO.2014.59.0703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ansell SM, Lesokhin AM, Borrello I, et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin’s lymphoma. N Engl J Med. 2015;372:311–319. doi: 10.1056/NEJMoa1411087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wolchok JD, Kluger H, Callahan MK, et al. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med. 2013;369:122–133. doi: 10.1056/NEJMoa1302369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N Engl J Med. 2015;373:23–34. doi: 10.1056/NEJMoa1504030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Michot JM, Bigenwald C, Champiat S, et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer. 2016;54:139–148. doi: 10.1016/j.ejca.2015.11.016. [DOI] [PubMed] [Google Scholar]
- 22.Tirumani SH, Ramaiya NH, Keraliya A, et al. Radiographic Profiling of Immune-Related Adverse Events in Advanced Melanoma Patients Treated with Ipilimumab. Cancer Immunol Res. 2015;3:1185–1192. doi: 10.1158/2326-6066.CIR-15-0102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Nishino M, Tirumani SH, Ramaiya NH, Hodi FS. Cancer immunotherapy and immune-related response assessment: The role of radiologists in the new arena of cancer treatment. Eur J Radiol. 2015;84:1259–1268. doi: 10.1016/j.ejrad.2015.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Nishino M, Sholl LM, Hodi FS, Hatabu H, Ramaiya NH. Anti-PD-1-Related Pneumonitis during Cancer Immunotherapy. N Engl J Med. 2015;373:288–290. doi: 10.1056/NEJMc1505197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nishino M, Chambers ES, Chong CR, et al. Anti-PD-1 Inhibitor-Related Pneumonitis in Non-Small Cell Lung Cancer. Cancer Immunol Res. 2016;4:289–293. doi: 10.1158/2326-6066.CIR-15-0267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Nishino M, Brais LK, Brooks NV, Hatabu H, Kulke MH, Ramaiya NH. Drug-related pneumonitis during mammalian target of rapamycin inhibitor therapy in patients with neuroendocrine tumors: a radiographic pattern-based approach. Eur J Cancer. 2016;53:163–170. doi: 10.1016/j.ejca.2015.10.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Nishino M, Boswell EN, Hatabu H, Ghobrial IM, Ramaiya NH. Drug-Related Pneumonitis During Mammalian Target of Rapamycin Inhibitor Therapy: Radiographic Pattern-Based Approach in Waldenstrom Macroglobulinemia as a Paradigm. Oncologist. 2015;20:1077–1083. doi: 10.1634/theoncologist.2015-0033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Travis WD, Costabel U, Hansell DM, et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am J Respir Crit Care Med. 2013;188:733–748. doi: 10.1164/rccm.201308-1483ST. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Postow MA, Chesney J, Pavlick AC, et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med. 2015;372:2006–2017. doi: 10.1056/NEJMoa1414428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Maroto JP, Hudes G, Dutcher JP, et al. Drug-related pneumonitis in patients with advanced renal cell carcinoma treated with temsirolimus. J Clin Oncol. 2011;29:1750–1756. doi: 10.1200/JCO.2010.29.2235. [DOI] [PubMed] [Google Scholar]