

Abstract
Objectives:
The study aimed to evaluate and compare the dental prosthetic status and treatment needs of adult population in Jizan, Saudi Arabia, in relation to the age.
Materials and Methods:
A total of 1779 people aged 35–74 years from 4 survey areas (Hay al matar, Mahata khams, Dara ut tawhid, and Suq ad dakhili) selected through convenient sampling, around Jizan University, were surveyed, using the WHO survey criteria, 1997.
Statistical Analysis:
Number and percentages were calculated, and univariate analysis was performed using Chi-square test at 5% level of significance.
Results:
Different forms of prosthesis were present among patients in the upper (19.9%) and lower (19%) arches, respectively. Prosthetic treatment need was recognized in subjects, 56.4% for the upper and 57.2% for the lower arches, respectively. The prosthetic status and treatment needs differed statistically with respect to age.
Conclusion:
More than half of the surveyed adult populations were in need of some or the other forms of prosthesis. This study provides data for an oral health-care provider program for Jizan.
Keywords: Fixed prosthesis, prosthetic status, prosthetic treatment needs, removable prosthesis
INTRODUCTION
Tooth loss profoundly affects the psychosocial well-being of the patients.[1] It leads to a decrease in the height and width of the alveolar bone leading to a decrease in the size of denture-bearing area, radical alteration in the facial appearance giving rise to a “dished in” appearance, and reduced masticatory efficiency, leading to diminished nutritional intake. Hence, to prevent or ameliorate decrements in oral health-related quality of life, removable or fixed prosthetic treatment for edentulousness is often recommended.[2]
Studies reporting the dental prosthetic status of people give an indication of the awareness and perception of patients toward dental treatment, accessibility to dental services, priorities, and willingness to take treatment. Further, studies assessing the prosthetic treatment needs of the population indicate the burden of unmet treatment needs, and the data are highly useful for planning an oral health promotional program and improvement of prosthetic treatment facilities.
Jizan city (also spelled Jazan, Gizan, or Gazan) is situated on the coast of the Red sea and lies in the Southwest corner of Saudi Arabia. It is a large agricultural heartland having a population of 1.5 million.[3] Its oral health system is in a transitional developmental stage, and planning oral health care for the masses needs systematic data collection. Literature review indicates that oral cancer is a significant public health problem for the residents of Jizan;[4] besides this, there is hardly any scientific data regarding their oral health status.
Against this background, the present study was undertaken in Jizan, as a part of population-based oral health survey to formulate an oral health-care provider program. The primary aim of the study was to evaluate the dental prosthetic status and treatment needs among the 35–74-year-old adults of Jizan, with the secondary objective of comparing the prosthetic status and treatment needs in relation to age.
MATERIALS AND METHODS
A cross-sectional study was conducted among the adult population of Jizan aged 35–74 years. The study was conducted for 4 months (January–April 2013), and the study sample comprised all the patients examined during that period. For practical purposes, four survey areas (hay al matar, mahata khams, dara ut tawhid, and suq ad dakhili) around Jizan University were selected through convenient sampling method. The survey was conducted at workplaces as well as households. Using the formula, the sample size derived was 1800. Only those in the age group of 35–74 years were included. Person with any acute illness and not willing for the examination were excluded from the study. During the stipulated survey period, a total of 1779 patients were examined. The enrolled patients were first interviewed to obtain general information and sociodemographic variables. This was followed by oral examination, which was performed by a single calibrated (intra-examiner consistency of 88%) examiner who assessed the dental prosthetic status and treatment needs according to the criteria described in the WHO Oral health assessment form 1997.[5]
The WHO Code and criteria were as follows:[5]
Prosthetic status
Code 0: No prosthesis
Code 1: Bridge
Code 2: More than one bridge
Code 3: Partial denture
Code 4: Both bridge(s) and partial denture(s)
Code 5: Full removable denture
Code 9: Not recorded.
Prosthetic need
Code 0: No prosthesis needed
Code 1: Need for one-unit prosthesis
Code 2: Need for multi-unit prosthesis
Code 3: Need for a combination of one- and/or multi-unit prosthesis
Code 4: Need for full prosthesis (replacement of all teeth)
Code 9: Not recorded.
The study was approved by the Ethics Committee of the Faculty of Dentistry, Jizan University. Informed consent was obtained from the patients. The data were compiled and subjected to descriptive and inferential analysis using the SPSS software version 17 (SPSS Inc., 233 South Wacker Drive, 11th Floor, Chicago, IL). Univariate analysis was performed using Chi-square test at 5% level of significance.
RESULTS
Of the total 1779 patients examined, 1103 (62.0%) were males and 676 (38.0%) were females. Three hundred and thirty-three (18.7%) were professionals, 752 (42.3%) were semi-professionals, 324 (18.2%) were skilled/semiskilled, and 371 (20.9%) were unemployed.
Table 1 represents the prosthetic status of the upper arch in the different age groups. Overall, 79.1% were free of prosthesis, 18.7% had partial prosthesis (Code 1, 2, 3, and 4), and only 2.2% had full removable prosthesis (Code 5). The highest percentages of patients with no prosthesis (Code 0) were from the 35–44 years group (81.7%). There was a statistically significant difference between prosthetic status of the upper arch and the age groups (χ2 = 69.49, P < 0.001).
Table 1.
Comparison of the prosthetic status of the upper arch according to age groups

However, as the age advanced, there was no increase in the percentage of patients with prosthesis (Code 0, 1, 3, and 4), but a linear increase was appreciated for Codes 2 and 5 with regard to increasing age.
Table 2 represents the prosthetic status of the lower arch. Overall, 81% were free of any prosthesis, 17% had some kind of partial edentulousness for which prosthesis was placed, and only 2% had full prosthesis. The highest percentage for Code 0 (no prosthesis) was reported in the age group of 45–54 years (83.8%). A statistically significant difference was observed between prosthetic status of the lower arch and the age groups. A linear increasing trend in the percentage of patients for Code 5 was appreciated.
Table 2.
Comparison of the prosthetic status of the lower arch according to age groups

Table 3 represents the prosthetic treatment need of the upper arch. Overall, 43.4% did not need any kind of prosthetic treatment. Fifty percent were in need of some or the other forms of partial prosthesis (Code 1, 2, and 3) and only 6.4% needed full prosthesis (Code 4). A statistically significant difference was seen between the prosthetic treatment need codes and age. As the age advanced, the percentage of patients needing prosthetic treatment linearly increased and was clearly appreciable for Codes 3 and 4.
Table 3.
Comparison of the prosthetic treatment needs of the upper arch according to age groups
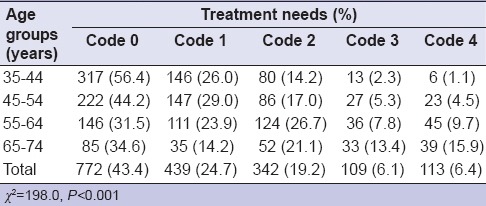
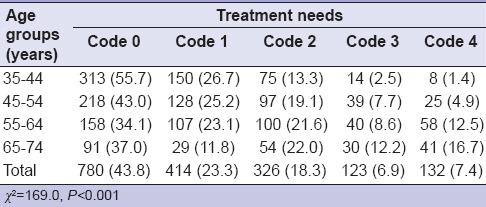
Table 4 represents the prosthetic treatment need of the lower arch. Overall, 43.8% did not need any kind of prosthetic treatment. Nearly, 49.8% were in need of some or the other forms of partial prosthesis and only 7.4% needed a full prosthesis. A statistically significant difference was seen between the treatment need codes and the age. As the age advanced, the percentage of patients requiring prosthetic treatment also increased and was clearly appreciated for Codes 2, 3, and 4. In addition, it was observed that implants were present, but only in 1.3% (n = 24) of the sample.
Table 4.
Comparison of the prosthetic treatment needs of the lower arch according to age groups
DISCUSSION
In the present study, it was observed that some or the other kinds of prosthesis (Code 2, 3, 4, and 5) were present in 19.9% of the patients in the upper arch and 19% of the patients in the lower arch. Compliant with the fact that tooth loss steadily increases with age[6] and comparison with the tooth loss figures[7] provided by a study, (people with tooth loss in different age groups being; 59.1% [35–44 years], 83.2% [45–54 years], 81.3% [55–64 years], and 94.1% [65–74 years],) the percentage of people in Jizan with prosthetic rehabilitation appears to be low. In addition, other study reports[8,9] have showed a greater percentage of people with prosthesis.
In the present study, the burden of unmet treatment need (treatment need code 2, 3, and 4) was recognized among 56.4% of the patients for the upper arch and 57.2% of the patients for the lower arch. Only 6.4% needed full prosthesis, the majority being from the 65–74 years age group. Overall, greater percentage of people needed partial prosthesis as compared to full prosthesis which was similar to the findings of the Turkish population,[10] while contrasting to the study report by Slade et al.[11]
Partial tooth loss should also be given due importance (as total edentulousness) and considered for prosthetic rehabilitation. Literature on partial edentulousness indicates that the first mandibular molar is the frequently missing tooth, followed by the maxillary anterior teeth and the mandibular molars.[6] It can be observed that a greater percentage of people consider fixed prosthetic dentures (33.21%) over removal prosthetic dentures (16.32).[12] This was in line with the present study, in which the percentage of patients with fixed prosthesis (Codes 1 and 2) was more as compared to removable prosthesis (Code 3) (14.7% patients had fixed prosthesis vs. only 2.7% having removable prosthesis in the upper arch, 13.2% had fixed prosthesis vs. just 2.9% having removable prosthesis in the lower arch).
People with edentulousness and without prosthetic rehabilitation suggest that they are not motivated to take treatment, cannot bear the finances,[13] are not aware of the different treatment modalities,[14] have time constrains to take treatment,[13,15] or have the fear of dental treatment.[16] Since the level of education[17] also influences the treatment-seeking behavior, this may have had an impact on the prosthetic rehabilitation of the people in Jizan, as nearly 30% of Jizan population studied were illiterate. Further, income may not play a major role with respect to prosthetic rehabilitation, as the Saudi government provides free dental treatment to the people.[6]
Even today, conventional removable dentures continue to represent the first rehabilitative option offered to the edentate in many places around the world.[18] In the present study, implants were reported in very less number of patients. Cost is not a hindrance in Jizan, but creating awareness, motivation, and imparting correct knowledge about the treatment procedure may improve the implant placement among the people.
In the present study, only four areas around the university were selected which may not be representative of Jizan. However, these areas were selected for practical reasons as they were in close vicinity of the university, and treatment could be provided to the survey patients with no transportation issues.
CONCLUSION
This study provides data for an oral health-care provider program for Jizan. It was evident from the study that more than half of the surveyed adult population were in need of some or the other forms of prosthesis. The study confirms the relationship between increasing age and prosthetic status and treatment needs.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Allen PF, McMillan AS. A review of the functional and psychosocial outcomes of edentulousness treated with complete replacement dentures. J Can Dent Assoc. 2003;69:662. [PubMed] [Google Scholar]
- 2.Kumar S, Tadakamadla J, Tibdewal H, Prabu D, Kulkarni S. Dental prosthetic status and treatment needs of green marble mine laborers, Udaipur, India. Dent Res J (Isfahan) 2011;8:123–7. [PMC free article] [PubMed] [Google Scholar]
- 3.Education in Saudi Arabia. 2012. [Last accessed on 2013 Aug 20]. Available from: http://www.en.wikipedia.org/wiki/Education_in_Saudi_Arabia .
- 4.Brown A, Ravichandran K, Warnakulasuriya S. The unequal burden related to the risk of oral cancer in the different regions of the Kingdom of Saudi Arabia. Community Dent Health. 2006;23:101–6. [PubMed] [Google Scholar]
- 5.World Health Organization. Assessment form. In: Oral Health Survey: Basic Methods. 4th ed. Geneva: World Health Organization; 1997. pp. 21–46. [Google Scholar]
- 6.Idowu AT, Al Shamrani SM. Pattern of tooth loss in a selected population at King Saud university college of dentistry. Saudi Dent J. 1995;7:135–40. [Google Scholar]
- 7.Oral Health US. Section 4. Tooth Loss. 2002. [Last accessed on 2013 Aug 12]. Available from: http://www.drc.hhs.gov/report/pdfs/section4-toothloss.pdf .
- 8.Moutlak MF. Tooth loss, prosthodontics treatment need and association factors in a sample of adults attending college of dentistry, Al Mustansiriya university. J Al Rafidain Univ Coll. 2013;31:125–36. [Google Scholar]
- 9.Sveikata K, Balciuniene I, Tutkuviene J. Needs for prosthetic treatment in Vilnius population at the age over 45 years old. Stomatol Balt Dent Maxillofac J. 2012;14:81–4. [PubMed] [Google Scholar]
- 10.Pekiner F, Gumru B, Borahan MO, Aytugar E. Evaluation of demands and needs for dental care in a sample of the Turkish population. Eur J Dent. 2010;4:143–9. [PMC free article] [PubMed] [Google Scholar]
- 11.Slade GD, Spencer AJ, Gorkic E, Andrews G. Oral health status and treatment needs of non-institutionalized persons aged 60 in Adelaide, South Australia. Aust Dent J. 1993;38:373–80. doi: 10.1111/j.1834-7819.1993.tb05519.x. [DOI] [PubMed] [Google Scholar]
- 12.Mukatash GN, Al-Rousan M, Al-Sakarna B. Needs and demands of prosthetic treatment among two groups of individuals. Indian J Dent Res. 2010;21:564–7. doi: 10.4103/0970-9290.74221. [DOI] [PubMed] [Google Scholar]
- 13.Shigli K, Hebbal M, Angadi GS. Attitudes towards replacement of teeth among patients at the institute of dental sciences, Belgaum, India. J Dent Educ. 2007;71:1467–75. [PubMed] [Google Scholar]
- 14.Idrees N, Ghani F. Demands, needs, expectations, patterns and reasons among patients for treatment with fixed dental prostheses. [Last accessed on 2013 Aug 12];J Postgrad Med Inst. 2008 22 Available from: http://www.jpmi.org.pk/index.php/jpmi/article/view/1110 . [Google Scholar]
- 15.George AC, Hoshing A, Joshi NV. A study of the reasons for irregular dental attendance in a private dental college in a rural setup. Indian J Dent Res. 2007;18:78–81. doi: 10.4103/0970-9290.32425. [DOI] [PubMed] [Google Scholar]
- 16.Erten H, Akarslan ZZ, Bodrumlu E. Dental fear and anxiety levels of patients attending a dental clinic. Quintessence Int. 2006;37:304–10. [PubMed] [Google Scholar]
- 17.Bahannan SA. Knowledge and behaviour of tooth loss and artificial teeth among females residing in Jeddah, Saudi Arabia. JKAU: Med Sci. 2001;9:47–63. [Google Scholar]
- 18.Sahoo S, Kumar P, Sethi K, Goel M. Trends and attitude of edentate patients towards conventional and implant rehabilitative therapies: An Indian outlook. Int J Med Public Health. 2013;3:126–7. [Google Scholar]