

Abstract
Recurrent anterior shoulder instability following shoulder dislocation has an incidence as high as 68% among the younger population, however its association with coracoid fracture is extremely rare. Majority of coracoid fractures reported earlier have been shown to be associated with seizure disorder. We report a case of displaced coracoid fracture associated with recurrent anterior instability in a patient with no history of seizure disorder and its implications in causation as well as management are discussed. A 28 year old male, paramedic by profession, presented with complaints of multiple episodes of shoulder dislocation of right dominant extremity for last ten months. Pre-operative CT scan showed Hill-Sach's lesion associated with coracoid process fracture. In view of significant engaging Hill-Sach's lesion, bony reconstruction of glenoid to increase the articular arc was planned. However in view of the small coracoid fragment occurred due to fracture, Latarjet's procedure could not be planned and iliac crest bone graft (ICBG) was planned instead. Till date only 10 cases of coracoid fracture with anterior shoulder instability have been reported in English literature. Of the ten cases, six cases had history of seizure disorder while four cases had only traumatic association. In our case as coracoid fragment was small, it could not be used for Latarjet's procedure and instead was fixed to its proximal stump with suture anchors. This case highlight's rare injury pattern and emphasises on good clinico-radiological examination supplemented by high index of suspicion needed to diagnose this unusual presentation.
Keywords: Recurrent anterior shoulder instability, Coracoid fracture, Iliac crest bone graft (ICBG)
1. Introduction
Coracoid process fracture is uncommon, with an incidence between 3 and 13% of all scapular fractures; which themselves constitute less than 1% of all fractures.1 It may present as an isolated avulsion injury or with associated dislocation of acromio-clavicular joint and shoulder joint.2, 3
Isolated coracoid process fractures and non-unions are easily missed as they rarely cause disturbing symptoms and are difficult to visualize on routine radiographs.4 Recurrent anterior shoulder instability following shoulder dislocation has an incidence as high as 68% among the younger population,5 however its association with coracoid fracture is extremely rare, with only 10 such cases have been reported in English literature.2, 4, 6, 7, 8, 9, 10, 11
Majority of coracoid fractures reported earlier have been shown to be associated with seizure disorder.12 We report a case of displaced coracoid fracture associated with recurrent anterior instability in a patient with no history of seizure disorder and its implications in causation as well as management are discussed.
2. Case report
A 28 year old male, paramedic by profession, presented with complaints of multiple episodes of shoulder dislocation of right dominant extremity for last ten months. Patient had a fall from stairs ten months back resulting in injury to right shoulder with presentation suggestive of anterior dislocation shoulder. He underwent closed reduction under sedation followed by immobilization for 3 weeks at another institution, and this was followed by uneventful recovery. Six months after the index injury, he sustained another episode of dislocation while playing volleyball, he again underwent closed reduction and immobilization for 3 weeks. Since then he had two more episodes of shoulder dislocation, both involving postures bringing shoulder in extremes of abduction and external rotation. Last episode was two months before presentation; he had no history of seizures or any psychiatric disorder. On examination, there was wasting of deltoid muscle. Bony contours of the clavicle, acromion, scapular spine, and greater tuberosity were normal. Apprehension test, anterior drawer test and relocation test for anterior shoulder bony instability were positive. There was no neurological deficit and signs suggestive of hyper laxity. Radiographic evaluation revealed the presence of significant Hill–Sach's lesion with a bony fragment on axillary view (Fig. 1a and b).
Fig. 1.

Preoperative radiographs of shoulder joint (a) AP view and (b) axillary view showing no obvious bony lesion on glenoid side. There is a Hill-Sach's lesion on humeral side. An unusual bony fragment is noted (arrow) represent coracoids avulsion.
MR imaging revealed the Bankart's lesion and wedge shaped depression along the postero-lateral aspect of the humerus suggestive of Hill-Sach's lesion (Fig. 2a and b). Pre-operative CT scan showed Hill-Sach's lesion associated with coracoid process fracture (Fig. 3). Glenoid bony deficiency as measured on 3DCT scan was <25%, not considered as significant.
Fig. 2.
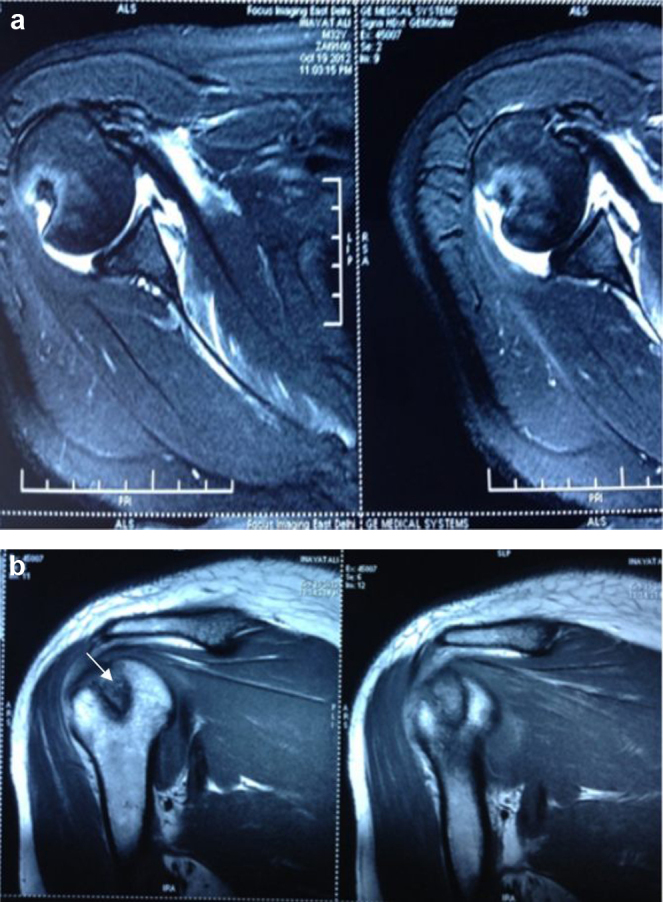
Magnetic resonance images (a) showing an anterior capsulo-labral tear (Bankart's lesion) and (b) wedge-shaped impaction (arrow) along the postero-lateral aspect of the humeral head (Hill-Sach's lesion).
Fig. 3.
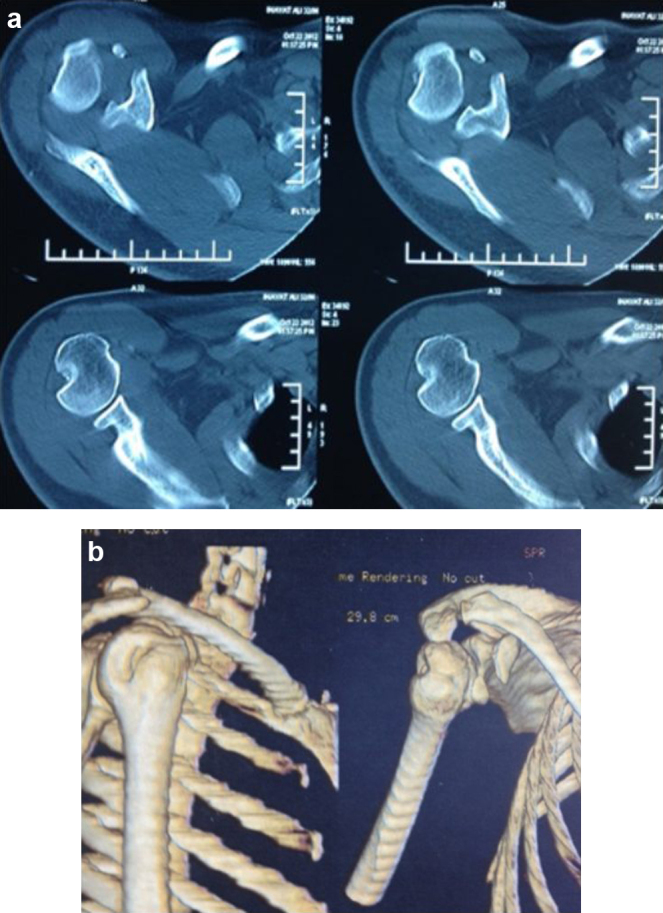
CT scan (a) showing Hill-Sach's lesion and (b) coracoid process fracture.
In view of significant engaging Hill-Sach's lesion, bony reconstruction of glenoid to increase the length of articular arc was planned. However in view of the small coracoid fragment occurred due to fracture, Latarjet's procedure could not be planned and iliac crest bone graft (ICBG) was planned instead.
Patient was placed in a beach chair position with a bolster in inter-scapular region to facilitate exposure. Delto-pectoral approach was used; small coracoid fragment with attached conjoined tendon was retracted to increase the exposure. ICBG was placed extra-capsularly. The ICBG was fixed using two 4.5 mm cannulated cancellous screws and the coracoid fracture was fixed with suture anchors to the base of coracoid (Fig. 4a and b). The wound was closed in layers and arm was supported with shoulder immobilizer postoperatively for 1 week. Passive range of motion exercises was started after 1 week. Six weeks post-operatively, active assisted ranges of motion exercises were started followed by standard rehabilitation protocol.
Fig. 4.

Follow up at 2 years (a) AP view and (b) axillary view showing incorporation of iliac crest bone graft.
At 2 years follow up, the patient has not had any further episode of shoulder dislocation and has returned to his pre-injury activity level with full shoulder range of motion (Fig. 5a and b).
Fig. 5.

Follow up at 2 years showing full range of shoulder motion (a) overhead abduction and (b) internal rotation.
3. Discussion
Coracoid process fractures are easily missed, as the symptoms are non-specific and routine radiographs are unremarkable.13 Isolated Fractures of the coracoid occur from direct blow to the coracoid or to lateral aspect of the shoulder.14, 15 Coracoid fractures may occur in association with acromio-clavicular dislocation with the coraco-clavicular ligaments remaining intact.3, 16, 17
The other mechanism of coracoid fractures include avulsion by muscle pull of biceps and coracobrachialis,18 direct contact of dislocating humeral head,19, 20 fatigue fractures,21 as a complication of tape fixation of acromio-clavicular joint20 or from medial migration of humeral head from cuff arthropathy.20 In our patient the mechanism of coracoid fracture was presumed to be due to direct impact of humeral head during anterior dislocation of shoulder.
The association of an anterior dislocation of the shoulder and a fracture of the coracoid process is very unusual. It is often unrecognized because of poor knowledge of this lesion and also the likelihood of them being missed due to poor quality of the radiographs performed in the emergency room.6 In our case, although radiographs did not reveal the fracture, pre-operative CT scan clearly demonstrated coracoid fracture along with significant Hill-Sach's lesion. The diagnosis of associated coracoid fracture requires good clinico-radiological examination with a lateral axillary view centered at coracoid performed after reducing the shoulder, which shows the fracture more clearly. Antero-posterior Cephalic Tilt View, Stryker Notch views have also been described to identify this innocuous fracture.22 However the best investigation remains CT scan with 3D reconstruction which can show associated injuries as well.23
Ogawa et al.24 classified the fracture of coracoids into two types on the basis of fracture site and attachment of coraco-clavicular ligament.24 Type 1 fractures include fracture of the coracoid occurring behind the attachment of ligament and Type 2 occurs anterior to the attachment of ligament.24 Type 2 fractures can be treated conservatively while Type 1 fractures usually need operative intervention as they are associated with disruption of scapulo-clavicular connection. Raviraj et al.23 stressed that all displaced fracture of the coracoid should be treated operatively to prevent the development of persistent pain and pseudoarthrosis.23 In our case although it was a Type 2 fracture as fracture but was too small to contribute for the modified Latarjet's procedure, thus it was fixed to its proximal stump to prevent painful pseudoarthrosis.
Till date only 10 cases of coracoid fracture with anterior shoulder instability have been reported in English literature. Of the ten cases, six cases had history of seizure disorder while four cases had only traumatic association.
In the four shoulders of coracoid nonunion, a standard Bristow-Latarjet procedure was performed.12 Robinson et al12 reported two cases in which the nonunion was more distal, therefore an Eden-Hybbinette procedure was performed.
Saragaglia et al.,6 reported three case of shoulder instability with associated coracoids fractures, all cases had fracture at the elbow of coracoid, while one case had fresh fracture, rest two presented with painful pseudo-arthrosis and all three cases underwent Latarjet's procedure emphasizing the high incidence of missed injuries in such cases.
While in the 10th case, the coracoid fracture was diagnosed intra-operatively and where only the coracoid anatomy was restored as recurrent shoulder instability was thought to occur secondary to coracoid fracture.11
In our case as coracoid fragment was small, it could not be used for Latarjet's procedure and instead was fixed to its proximal stump with suture anchors. Anterior glenoid bony reconstruction was done with iliac crest bone graft fixed with two cannulated cancellous screws (4.5 mm). This case highlight's rare injury pattern and emphasises on good clinico-radiological examination supplemented by high index of suspicion needed to diagnose this unusual presentation.
Conflicts of interest
The authors have none to declare.
References
- 1.McGinnis M., Denton J.R. Fractures of the scapula: a retrospective study of 40 fractured scapulae. J Trauma. 1989;29:1488–1493. [PubMed] [Google Scholar]
- 2.Garcia-Elias M., Salo J.M. Non-union of a fractured coracoid process after dislocation of the shoulder. A case report. J Bone Jt Surg Br. 1985;67:722–723. doi: 10.1302/0301-620X.67B5.4055868. [DOI] [PubMed] [Google Scholar]
- 3.Bernard T.N., Jr., Brunet M.E., Haddad R.J., Jr. Fractured coracoid process in acromioclavicular dislocations. Report of four cases and review of the literature. Clin Orthop Relat Res. 1983;175:227–232. [PubMed] [Google Scholar]
- 4.Cottias P., le Bellec Y., Jeanrot C., Imbert P., Huten D., Masmejean E.H. Fractured coracoid with anterior shoulder dislocation and greater tuberosity fracture – report of a bilateral case. Acta Orthop Scand. 2000;71(1):95–97. doi: 10.1080/00016470052943982. [DOI] [PubMed] [Google Scholar]
- 5.Vermeiren J., Handelberg F., Casteleyn P.P., Opdecam P. The rate of recurrence of traumatic anterior dislocation of the shoulder. A study of 154 cases and a review of the literature. Int Orthop. 1993;17(6):337–341. doi: 10.1007/BF00180449. [DOI] [PubMed] [Google Scholar]
- 6.Saragaglia D., Picard F., Gérard P., Tourne Y., Leroy J.M. Anterior instability of the shoulder associated with fracture of the coracoid process. Apropos of 3cases. Rev Chir Orthop Reparatrice Appar Mot. 1994;80(7):651–655. [PubMed] [Google Scholar]
- 7.Subramanian A.S., Khalik M.A., Shah M.M. Isolated fracture of the coracoid process associated with unstable shoulder. ANZ J Surg. 2007;77(3):188–189. doi: 10.1111/j.1445-2197.2006.04005.x. [DOI] [PubMed] [Google Scholar]
- 8.Kälicke T., Andereya S., Gekle J., Müller E.J., Muhr G. Coracoid pseudarthrosis caused by anterior shoulder dislocation with concomitant coracoid fracture. Unfallchirurg. 2002;105(9):843–844. doi: 10.1007/s00113-002-0427-2. [DOI] [PubMed] [Google Scholar]
- 9.Goodier D., Maffulli N., Good C.J. Coracoid process and greater tuberosity fracture in unreduced shoulder dislocation. Injury. 1994;25(2):113–116. doi: 10.1016/0020-1383(94)90116-3. [DOI] [PubMed] [Google Scholar]
- 10.Wong-Chung J., Quinlan W. Fractured coracoid process preventing closed reduction of anterior dislocation of the shoulder. Injury. 1989;20(5):296–297. doi: 10.1016/0020-1383(89)90173-3. [DOI] [PubMed] [Google Scholar]
- 11.Lal H., Bansal P., Sabharwal V.K., Mawia L., Mittal D. Recurrent shoulder dislocations secondary to coracoid process fracture: a case report. J Orthop Surg. 2012;20(1):121–125. doi: 10.1177/230949901202000127. [DOI] [PubMed] [Google Scholar]
- 12.Robinson C.M., Al-Hourani K., Malley T.S., Murray I.R. Anterior shoulder instability associated with coracoid nonunion in patients with a seizure disorder. J Bone Jt Surg Am. 2012;94(7):e40. doi: 10.2106/JBJS.K.00188. [DOI] [PubMed] [Google Scholar]
- 13.Zilberman Z., Rejovitzky R. Fracture of the coracoid process of the scapula. Injury. 1981;13(3):203–206. doi: 10.1016/0020-1383(81)90239-4. [DOI] [PubMed] [Google Scholar]
- 14.Mariani P.P. Isolated fracture of the coracoid process in an athlete. Am J Sports Med. 1980;8(2):129–130. doi: 10.1177/036354658000800214. [DOI] [PubMed] [Google Scholar]
- 15.Gil J.F., Haydar A. Isolated injury of the coracoid process: case report. J Trauma. 1991;31(12):1696–1697. doi: 10.1097/00005373-199112000-00023. [DOI] [PubMed] [Google Scholar]
- 16.Herscovici D., Jr., Fiennes A.G., Allgöwer M., Rüedi T.P. The floating shoulder: ipsilateral clavicle and scapular neck fractures. J Bone Jt Surg Br. 1992;74(3):362–364. doi: 10.1302/0301-620X.74B3.1587877. [DOI] [PubMed] [Google Scholar]
- 17.Zettas J., Muchnic P. Fractures of the coracoid process base in acute acromioclavicular separation. Orthop Rev. 1976;5:77–79. [Google Scholar]
- 18.Rounds R.C. Isolated Fracture of the coracoid process. J Bone Jt Surg Am. 1949;31A(3):662. [PubMed] [Google Scholar]
- 19.Garcia-Elias M., Salo J.M. Non-union of a fractured coracoid process after dislocation of the shoulder. A case report. J Bone Jt Surg Br. 1985;67(5):722–723. doi: 10.1302/0301-620X.67B5.4055868. [DOI] [PubMed] [Google Scholar]
- 20.Moneim M.S., Balduini F.C. Coracoid fracture as a complication of surgical treatment by coracoclavicular tape fixation. A case report. Clin Orthop Relat Res. 1982;168:133–135. [PubMed] [Google Scholar]
- 21.Boyer D.W., Jr. Trapshooter's shoulder: stress fracture of the coracoid process. Case report. J Bone Jt Surg Am. 1975;57(6):862. [PubMed] [Google Scholar]
- 22.Rockwood C.A. Management of fractures of the scapula. Orthop Trans. 1986;10:219. [Google Scholar]
- 23.Raviraj A., Anand A., Vijay S. An isolated displaced fracture of the coracoid process treated with osteosynthesis—a case report and review of literature. Surg Sci. 2013;4:184–187. [Google Scholar]
- 24.Ogawa K., Yoshida A., Takahashi M., Ui M. Fractures of the coracoid process. J Bone Jt Surg. 1997;79:17–19. doi: 10.1302/0301-620x.79b1.6912. [DOI] [PubMed] [Google Scholar]