

Abstract
A case of broken drill bit during arthroscopic ACL reconstruction and the technique adopted to overcome this complication is presented. We also review the literature for intra-operative incidents and technical complications during arthroscopic ACL reconstruction and various precautions we should implement to prevent such technical pitfalls from coming into reality.
Keywords: ACL reconstruction, Complications, Drill bit failure, Intraoperative incidents, Technical tip
1. Introduction
Arthroscopic ACL reconstruction is one of the most common arthroscopic surgeries performed in the world today.1 This surgery is a technically challenging and is often associated with many complications. Although post-operative complications have been described in great detail, data on intra-operative complications is relatively sparse.1
Instrument breakage during arthroscopic knee surgeries is considered a relatively common occurrence due to the delicate arthroscopic instrumentation, limited manoeuvring space, inappropriate instrument selection, incorrect surgical techniques and overuse of worn out instruments being the most common underlying reasons.1, 2, 3
However, after extensively reviewing the available literature, we could not find any case report mentioning a broken drill bit during arthroscopic ACL reconstruction using bone patellar tendon bone graft (BPTB graft) and interference screw fixation technique.
The purpose of this case report is not only to describe this rare complication but also to describe the unique technique we adopted to retrieve the broken drill bit. We also analysed the probable reasons for instrument breakage and how best we can prevent such complications from occurring.
2. Case report
A 26-year-old male sustained a direct contact injury to his right knee in a road traffic accident, 2 years prior to presentation. He was diagnosed with a chronic ACL deficiency for which he was operated. ACL reconstruction was performed using an ipsilateral bone patellar tendon bone (BPTB) autograft and standard technique. He was operated under regional spinal anaesthesia with the use of a tourniquet. The surgery went on uneventfully till the femoral tunnel placement/drilling step.
The femoral tunnel was being drilled using the trans-tibial technique with the knee in 90° of flexion. The femoral over-the-top aiming guide was placed through the tibial tunnel aiming for the 11 o’ clock position after debriding the ACL stump and ensuring good visualisation of the posterior femoral cortex. The over-the-top guide was removed and a guidewire was passed through the distal femur, which exited the thigh antero-laterally and was held in place there by a holding forceps. The guidewire used was straight and had no abrasions on it. A 4.5 mm cannulated drill bit was now advanced over the guidewire via the tibial tunnel. After penetrating the lateral femoral condyle for a distance of about 1 cm, the drill bit gave away suddenly (Fig. 1).
Fig. 1.
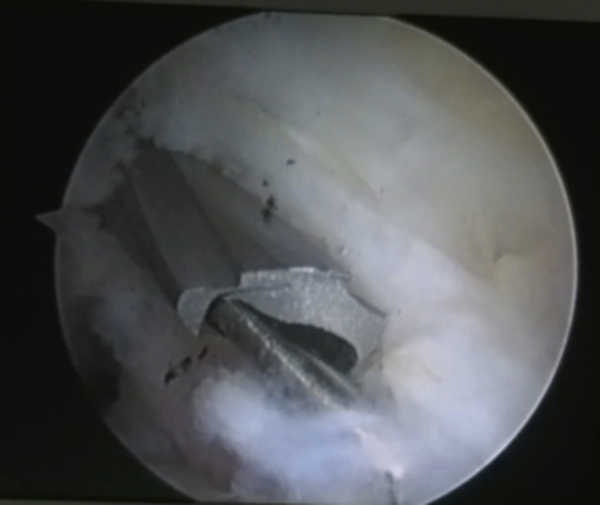
Arthroscopic image showing broken drill bit tip lodged in the lateral femoral condyle with dissipated minute fragments in the near vicinity.
Inflow of irrigation fluid into the knee joint was immediately stopped to prevent dissipation of small metal particles. On attempting to remove the broken drill bit mechanically using various types of grabbing forceps including a Kocher's forceps, the broken drill bit did not budge from its position. We then passed another cannulated 4.5 mm drill bit in a retrograde direction on the same guidewire. When both the drill bits came into contact, the broken drill bit disimpacted and we further pushed it out of the knee down the tibial tunnel. The broken drill bit piece was then retrieved easily using a Kocher forceps (Fig. 2, Fig. 3).
Fig. 2.

Image showing reverse drill-out technique of retrieval of broken, impacted drill bit.
Fig. 3.

The broken drill bit which has been mechanically pushed out of the tibial tunnel over the guidewire.
Eventually, the femoral tunnel drilling step was repeated with a new drill bit on the same guidewire and the rest of the surgical procedure was uneventful. The surgical wound healed without complications and the post-operative rehabilitation also went on in the usual fashion.
3. Discussion
ACL reconstruction surgery is loaded with a large number of possible technical pitfalls.4 Intra-operative complications during ACL reconstructions have been categorised into 4 groups: (1) during graft harvest, (2) during graft fixation, (3) during tunnel placement or (4) during graft tensioning.5 Instrument breakage can occur at any stage of the surgery but commonly occurs during tunnel placement/drilling and graft fixation steps.1, 2, 3
Although broken instruments during ACL reconstruction surgery are not uncommon and a few reports have been published,1, 2, 3 to the best of our knowledge, only one case of broken drill bit has been mentioned in the literature.4 Miller reported a case of broken endobutton drill bit during ACL reconstruction using a semitendinosus–gracilis autograft (STG) which was left in place, as it did not appear likely to migrate or to affect graft fixation.4 Also, the broken drill bit mentioned in this case report pertains to an endobutton drill bit which was intended for a single use but had been used multiple times by the authors which is unlike our case where the cannulated drill bit is not intended for single use.
Milankov et al. reported a case of broken femoral guide during arthroscopic ACL reconstruction by anteromedial portal technique of femoral tunnel placement. In the same publication, they also reported 11 cases of arthroscopic instrument breakage among 1350 arthroscopic ACL reconstructions performed over a period of 13 years which accounted for 0.81% of their cases. The broken instruments mentioned in their study include probe hooks (2), guide wires (3), forceps scissors (2) and fore-part of a burr shaver (1), all of which were successfully retrieved arthroscopically during surgery.3
Almazan et al. analysed intra-operative incidents and complications in a series of 426 arthroscopic ACL reconstructions performed over a period of 6 years and described just two cases of instrument breakage – a broken screwdriver and a broken bio-absorbable screw.1
From 1992 to 2015, more than 3000 ACL reconstructions have been performed by our group in our institute among which we have had only 4 other incidents of broken instrumentation, which are 3 biodegradable screws and 1 scissor. This accounts for less than 0.17% of the cases operated by our team which highlights the rarity of this incident.
It has been suggested by Milankov et al. that when instrument breakage occurs, inflow of irrigation fluid must be promptly stopped lest the broken part migrates into the posterior compartment from where it may become a difficult task to retrieve.3
Both surgeons and nurses should always inspect instruments carefully, before and after usage, to detect instrument breakage on table and to avoid missing out on this complication.3 Employing nurses trained well in arthroscopic surgery would be beneficial, as then, even the minutest changes in the instrumentation can be picked up immediately.3
One of the possible explanations of this complication is the repeated usage of the same cannulated drill bit for multiple surgeries which probably lead to the fatigue of the material. Arthroscopic instruments must be regularly replaced after a certain number of surgeries by the operating room personnel in accordance with the specifications provided by the manufacturer.3 Prior to this incident, we followed a policy of using the same cannulated drill bit for around 20–25 ACL cases. Following this incident, we have started replacing the drill bit every 10 cases. Also, repeated autoclaving of instruments may have an effect on the material properties.3 Therefore, it is essential to limit the number of sterilisation cycles that the instruments are subjected to.
We should understand that the number of technical pitfalls during arthroscopic ACL reconstruction is so vast that irrespective of the surgeons’ experience, it is still possible to end up discovering a new pitfall. Therefore, a surgeon must always anticipate and be prepared to face and solve such technical pitfalls during surgery.
Conflicts of interest
The authors have none to declare.
References
- 1.Almazán A., Miguel A., Odor A. Intraoperative incidents and complications in primary arthroscopic anterior cruciate ligament reconstruction. Arthroscopy. 2006;22(November (11)):1211–1217. doi: 10.1016/j.arthro.2006.06.019. [DOI] [PubMed] [Google Scholar]
- 2.Arthroscopic burs and blades are breaking in patients. Health Devices. 1999;28:234. [PubMed] [Google Scholar]
- 3.Milankov M.Z., Miljkovic N., Ninkovic S. Femoral guide breakage during the anteromedial portal technique used for ACL reconstruction. Knee. 2009;16:165–167. doi: 10.1016/j.knee.2008.10.005. [DOI] [PubMed] [Google Scholar]
- 4.Miller M.D. EndoButton drill bit failure. Arthroscopy. 2002;18(March (3)):322–324. doi: 10.1053/jars.2002.29936. [DOI] [PubMed] [Google Scholar]
- 5.Sekiya J.K., Ong B.C., Bradley J.P. Complications in anterior cruciate ligament surgery. Orthop Clin N Am. 2003;34:99–105. doi: 10.1016/s0030-5898(02)00058-5. [DOI] [PubMed] [Google Scholar]