

Abstract
Hereditary multiple exostoses, an autosomal dominant condition, is a common benign tumor which is characterized by the development of multiple osteochondromas. Bilateral dorsal and ventral involvement of scapulae is extremely rare without any reported case in the literature. An 18-year-old girl was referred because of bilateral prominent scapulae and left-sided pain on shoulder girdle motion especially at more than 90° abduction and forward flexion. Radiograph evaluation showed multiple exostoses on ventral and dorsal surfaces of body of both scapulae; hence simple excision of the lesion was impossible. The patient was symptom-free about 18 months after partial scapulectomy of left side. Partial scapulectomy seems to be an effective treatment for the sandwiched scapula between dorsal and ventral benign tumors.
Keywords: Osteochondroma, Scapula, Scapulectomy, Multiple hereditary exostoses, Benign tumor
1. Introduction
Osteochondroma is the most common benign bone tumor but multiple hereditary exostoses is an infrequent entity.1 Diagnosis of multiple hereditary exostoses can be radiologically made with at least two osteochondromas around the juxta-epiphyseal region of the long bones.2 Osteochondroma is an autosomal dominant condition and approximately 62% of the patients with multiple hereditary exostoses have a positive family history. The prevalence of multiple hereditary exostoses is estimated at 1:50,000 persons within the general population with male predilection (male-to-female ratio: 1.5).2, 3, 4
Although different parts of scapula could be involved by osteochondroma, involvement of ventral surface is more common than dorsal one.5, 6, 7 To the best of our knowledge, involvement of both ventral and dorsal surfaces of bilateral scapulae in one patient has not been reported yet. We would suggest the name of “sandwiched scapulae” for this rare condition.
2. Case report
An 18-year-old girl, a known case of multiple hereditary exostoses, was referred to orthopedic clinic with complaint of bilateral prominent scapulae and left-sided pain on shoulder girdle motion especially at more than 90° abduction and forward flexion. The patient reported that lying on her back resulted in severe pain. She had history of an operation for excision of a mass on proximal of left leg about 10 years before the new presentation.
On physical exam, winging of left scapula in forward flexion was obvious. A big oval lobulated immobile mass with hard consistency was palpable on the dorsal aspect of the left scapula (Fig. 1). Also a smaller mass was obvious on the dorsal aspect of the right scapula. Moreover, multiple bony prominences were palpated at the proximal and distal parts of both legs and distal part of both femurs.
Fig. 1.

Mass of left scapula from posterior view.
Chest X-ray including both shoulders showed high-density shadows on both scapulae. Radiographic evaluation of both lower extremities revealed multiple osteochondromas at different parts. Computed tomography (CT) scan with three-dimensional reconstruction of the thoracic cage discovered large osteochondromas on dorsal and smaller lesions on ventral aspect of bodies of both scapulae (Fig. 2, Fig. 3). Axial cut of the CT scan showed the thin shell of bone between the osteochondromas (Fig. 4).
Fig. 2.
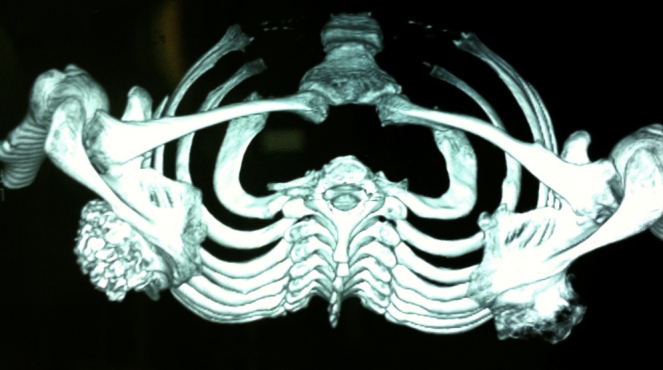
Reformatted CT scan of thoracic cage displays involvement of the ventral and dorsal surfaces of both scapulae.
Fig. 3.
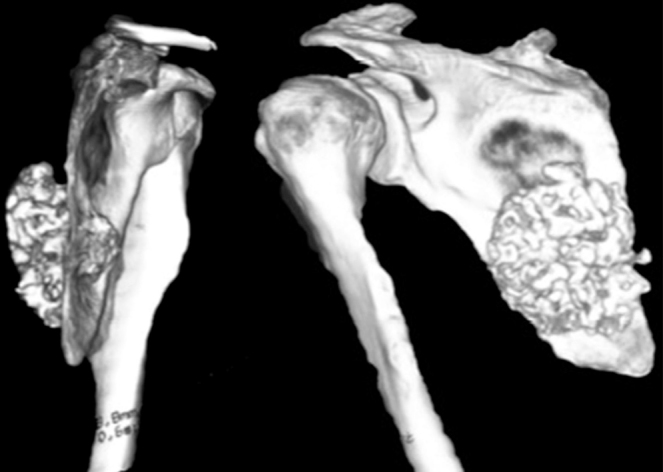
Left scapular involvement.
Fig. 4.

Thin shell of bone between the osteochondromas on axial cut CT scan.
The patient was scheduled for surgical excision of the left side lesion because the pain was nonresponsive to conservative trials including non-steroid anti-inflammatory medications and modification of activities. Under general anesthesia in prone position, elliptical skin incision was made encompassing the tumor and extending from the tip of the acromion, superolaterally to the paravertebral region inferomedially. Medial and lateral skin flaps were elevated. The huge mass (size: about 13 cm × 8 cm × 4 cm) was exposed without any anomalous bursa (Fig. 5). The ventral aspect of left scapula was involved as well as the dorsal aspect with just a thin shell of bone between them. Preservation of this thin layer of scapula was impossible. In other words, the scapula was sandwiched between the two masses. We think that one of the sources of pain in this patient might be the smaller ventral lesion (size: about 4 cm × 2 cm × 1 cm) with frictions on the chest wall, so partial scapulectomy was planned. The attachment of the latissimus dorsi to the inferior angle of the scapula was divided, and the muscle was retracted inferiorly. Then the inferior angle of scapula was pulled inferiorly using a towel clips and the attached muscles to the medial border of the scapula were divided. After retraction of the axillary contents out of the operation field by abducting the arm, attachments of muscles including teres major, teres minor, infraspinatus, and serratus anterior were divided from the scapula. Partial scapulectomy was performed by osteotomy of the scapula 2 cm proximal to the tumor margin (Fig. 6). After checking hemostasis, the insertions of the muscles were sutured to the chest wall and the remaining scapula. Stability of the muscles and motion of the scapula in passive range of motion of the shoulder was acceptable. Pathological report approved the diagnosis of benign osteochondroma without any sarcomatous transformation.
Fig. 5.
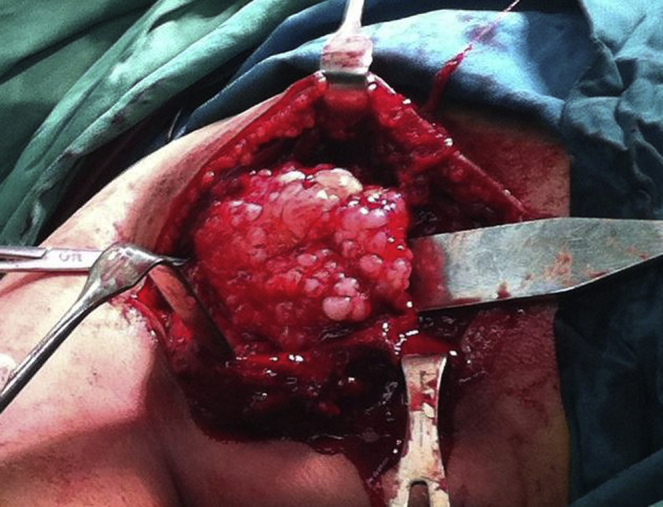
Intraoperative photography of huge dorsal osteochondroma of Lt scapula.
Fig. 6.
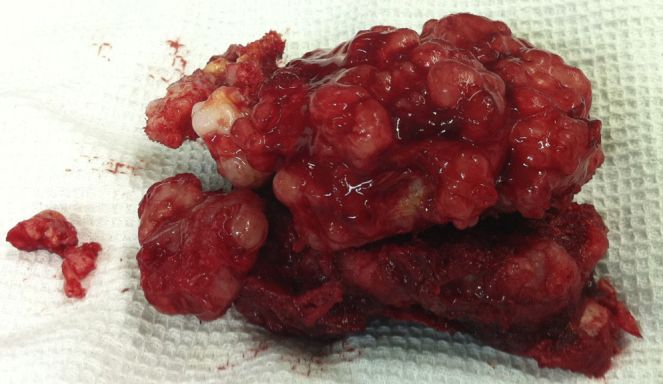
Resected body of scapula with huge osteochondromas.
The patient had no recurrence with normal active and passive painless range of motion at 18 months after the surgery (Fig. 7). Muscles powers of shoulder girdle were well except external rotators with power of 4 out of 5.
Fig. 7.

Normal painless range of motion of the patient at 18-month follow-up visit.
3. Discussion
Scapula is involved in 3–4.6% of all reported cases of osteochondroma.5 On the other hand, 14.4% of scapular tumors are osteochondroma.6 The ventral surface is involved more commonly than the dorsal one, followed by the inferior angle.5, 6, 7 The presenting symptoms of scapular osteochondroma could be different such as pain on motion, crepitus, decreased range of motion, mass, weakness of the shoulder girdle muscles, snapping, and pseudo-winging of the scapula7, 8; however, it might be an incidental finding.
Conservative treatments of osteochondroma of scapula are immobilization, physiotherapy, anti-inflammatory medications, and local anesthetic injection. In large tumors, the mechanical dysfunction and/or pain may continue and annoy the patient. Operative treatments are used for the patients after failure of conservative management or in clinical settings with high suspicion of malignant transformation.
In the presented case, the presence of only a thin layer of bone between the ventral and dorsal tumors precluded simple excision of the prominences. Partial scapulectomy was performed in the left side with the aforementioned technique. The patient had normal range of motion and was pain-free 18 months after operation. There is no clinical and radiographic sign of recurrence during follow-up period.
Surgical excision of osteochondroma of scapula is the preferred method of surgery. However when ventral and dorsal surfaces of scapula are extensively involved, preservation of scapula may be impossible. Partial scapulectomy seems to be a safe surgical solution with acceptable outcomes.
Conflicts of interest
The authors have none to declare.
Footnotes
Study was carried out in Bone and Joint Diseases Research Center, Department of Orthopedic Surgery, Chamran Hospital, Shiraz University of Medical Sciences, Shiraz, Iran.
Contributor Information
Kamran Mozaffarian, Email: kammoza@gmail.com.
Mohammad Javad Farahani, Email: mjfarahan@hotmail.com.
Amir Reza Vosoughi, Email: vosoughiar@hotmail.com.
References
- 1.Solooki S., Vosoughi A.R., Masoomi V. Epidemiology of musculoskeletal tumors in Shiraz, south of Iran. Indian J Med Paediatr Oncol. 2011;32:187–191. doi: 10.4103/0971-5851.95138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Legeai-Mallet L., Munnich A., Maroteaux P., Le Merrer M. Incomplete penetrance and expressivity skewing in hereditary multiple exostoses. Clin Genet. 1997;52:12–16. doi: 10.1111/j.1399-0004.1997.tb02508.x. [DOI] [PubMed] [Google Scholar]
- 3.Schmale G.A., Conrad E.U., Raskind W.H. The natural history of hereditary multiple exostoses. J Bone Jt Surg Am. 1994;76:986–992. doi: 10.2106/00004623-199407000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Wicklund L.C., Pauli R.M., Johnston D., Hecht J.T. Natural history study of hereditary multiple exostoses. Am J Med Genet. 1995;55:43–46. doi: 10.1002/ajmg.1320550113. [DOI] [PubMed] [Google Scholar]
- 5.Esenkaya I. Pseudowinging of the scapula due to subscapular osteochondroma. Orthopedics. 2005;28:171–172. doi: 10.3928/0147-7447-20050201-22. [DOI] [PubMed] [Google Scholar]
- 6.Fageir M.M., Edwards M.R., Addison A.K. The surgical management of osteochondroma on the ventral surface of the scapula. J Pediatr Orthop B. 2009;18:304–307. doi: 10.1097/BPB.0b013e32832f06f4. [DOI] [PubMed] [Google Scholar]
- 7.Frost N.L., Parada S.A., Manoso M.W., Arrington E., Benfanti P. Scapular osteochondromas treated with surgical excision. Orthopedics. 2010;33:804. doi: 10.3928/01477447-20100924-09. [DOI] [PubMed] [Google Scholar]
- 8.Kwon O.S., Kelly J.I. Delayed presentation of osteochondroma on the ventral surface of the scapula. Int J Shoulder Surg. 2012;6:61–63. doi: 10.4103/0973-6042.96996. [DOI] [PMC free article] [PubMed] [Google Scholar]