

Abstract
This study examined whether a group intervention focusing on building up preparedness for career management can prevent future sickness absence.
Register-based data on the number of sickness absence days and sickness absence episodes were examined as outcomes of the intervention among 684 employees in 17 organizations in a randomized controlled trial. Sickness absence data were collected covering a period from 1 year before (baseline) to approximately 2 years after the intervention (follow-up). The data were analyzed using zero-inflated negative binomial models.
After controlling for baseline absence, age, gender, and organization, the intervention was effective in decreasing the number of longer sickness absences (lasting longer than > 2 weeks), but no other significant effects were found.
These findings point out that it is feasible to use a career management intervention to prevent future sickness absence in work organizations.
The incidence of sickness absence and chronic illnesses among working-age population is a considerable public health and economic burden. Sickness absenteeism predicts future absence,1 future poor health,2–5 and even permanent work disability. Previous research also shows that longer absence from work reduces considerably the probability of returning to work, and rehabilitation is not always effective. Especially long sickness absence episodes have been found to predict early retirement due to disability.6 Therefore, it seems feasible to focus on preventing especially long-term absence and promoting return to work. This study introduces a resource-based framework for the prevention of sickness absence.
Our resource-based framework focuses on promoting career management preparedness of employees at workplaces. It relies on principles of social cognitive theories on social learning, behavioral control, and individual stress inoculation.7–10 Career management preparedness is defined here as a cognitive-motivational construct that contains specific self-efficacy9 and preparation against setbacks.10
Career management self-efficacy refers to the degree of confidence in one's ability to manage proactively one's career in a health-enhancing way. Career management self-efficacy is a motivational component that increases the likelihood of future behavior.8,9 In a work-life course framework, it is a useful concept not only during times of occupational transitions but also in promoting mental health, well-being, and productive careers.11 Preparation against setbacks refers to the ability to anticipate setbacks in managing one's career and the skill to cope with them. Preparation against setbacks is similar to inoculation against diseases, as individuals develop “learned resourcefulness” by the exposure to manageable levels of stress related to one's future career or health and well-being. It helps in maintaining motivation to perform difficult behaviors in the face of setbacks and prevents relapse.10 Both self-efficacy and preparation against setbacks are known psychological mechanisms explaining successful coping with, for example, chronic disease12 and prevention of depressive symptoms.11,13,14
The role of these psychological resources in reducing sickness absenteeism can be expected to be twofold. First, better preparedness for managing own career may directly have beneficial mental health outcomes by reducing sickness absences. Similarly, it has been found by earlier studies that career management intervention reduced symptoms of depression.11,14,15 Common mental disorders, such as symptoms of depression, may be associated with sickness absence.16–21 Second, the beneficial physical and mental health effects can be indirect. Improvement in the ability to cope with various symptoms or illnesses makes people feel more efficacious and positive about their ability to work, and they are more likely to continue working despite experiencing illnesses.12
Earlier results from return-to-work interventions show that both individual and work resources are relevant in promoting return to work after sick leave.22 This means that the aim can be either increasing the individual's coping abilities or changing the work environment, or both. Career management can involve both better control of the situation and change in the environment. Measures to strengthen preparedness for career management seem feasible for prevention of sickness absences, as in prior studies, it was found to decrease symptoms of depression and intentions to retire early, as well as to enhance intrinsic work motivation and to improve mental resources of employees in different kinds of jobs11,15 and stressful job situations.14 These positive effects of the intervention were mediated via enhanced preparedness for career management, which was the proximal aim of the intervention.11
There is some previous evidence showing that preventive interventions focusing on enhancing resources may decrease sickness absence. By treating employees on sick leave due to adjustment disorders through a combination of cognitive behavioral treatment and time contingency principles, the researchers were able to shorten the duration of sick leaves.23 A stress-management intervention was successful in decreasing self-reported absenteeism in a Danish study,24 and register-based absences in a Dutch study.25 In a German setting, self-efficacy and self-management of employees were enhanced, which seemed to reduce the rate of absence after the intervention.26 However, these studies did not have randomized controlled study (RCT) designs, did not control for previous absence, and were not targeting preparedness for career management but gave participants some other new resources for coping at work.
In this RCT study, we investigated if a career management intervention implemented at workplaces with the aim of promoting preparedness is effective in preventing sickness absence. Our first hypothesis concerns the main effect of the intervention on sickness absences.
Hypothesis 1 states that the preventive career management intervention decreases the number of sickness absence days and sickness absence episodes.
Our second hypothesis is related to the mechanism of change.
Hypothesis 2 states that the effect of the career management intervention is mediated via an increased level of career management preparedness as its proximal effect.
METHODS
Procedure and Participants
A total of 43 work organizations representing different sectors of working life were contacted by email and offered the opportunity to meet the researchers to discuss participation in the study. Of these, 17 chose to participate: nine municipal organizations, five governmental organizations, and three private enterprises. The size of the participating work organizations varied from about 100 to 13,900 employees, most participating organizations being large (with over 500 employees) and representing white-collar tasks. The personnel of the participating organizations were mostly women (75%).
All intervention materials and training for trainers were provided free of charge to the organizations. At least two employees from each organization were trained as trainers for 4 days at the Finnish Institute of Occupational Health. It was recommended that one of the trainers would come from occupational health services and the other from human resources.
In participating organizations, the offer to take part in the intervention was usually made to all employees via intranet, personnel magazines, or other established information channels used by the organizations in their daily communication, as a way to “get an extra buzz from your work.” The intervention was targeted at mid-career employees who might soon develop thoughts about early retirement. As we wanted to target the intervention to a time period just before such intentions could develop, we recruited participants at the age group of 40 years or more. Some younger employees also expressed active interest in the topic and were included into the study.
The information letter for the employees interested in the study included information on the study design as having two experimental conditions: either participation in group training for 16 hours during working hours or a literature package. To become a participant of the study, the employees had to agree to the randomization procedure, to give their consent (or to decline) for collecting sickness absence data, and to return the baseline questionnaire (T1) before the randomization. From the 732 people who originally responded, only 14 were rejected due to unknown addresses, returning the questionnaire too late, stated preference for either study group, or quitting the study.
Between the years 2006 and 2008, a total of 718 employees participated in the study. They were randomly assigned to the intervention (n = 369) or the comparison group (n = 349) (Fig. 1). The researchers carried out the randomization separately for each 17 participating organizations. Two researchers shuffled the received sealed envelopes including the baseline questionnaires, and divided them into two piles. The participants were given a research code and their questionnaires were sent to an independent company to be computed. The outcomes of the randomization were sent to the participating organizations, wherein the employees randomized into the intervention group were invited to take part in the group workshop. Those who were randomized into the comparison group received a literature package on career management and health-related information during the same week as the intervention group received their training.
FIGURE 1.
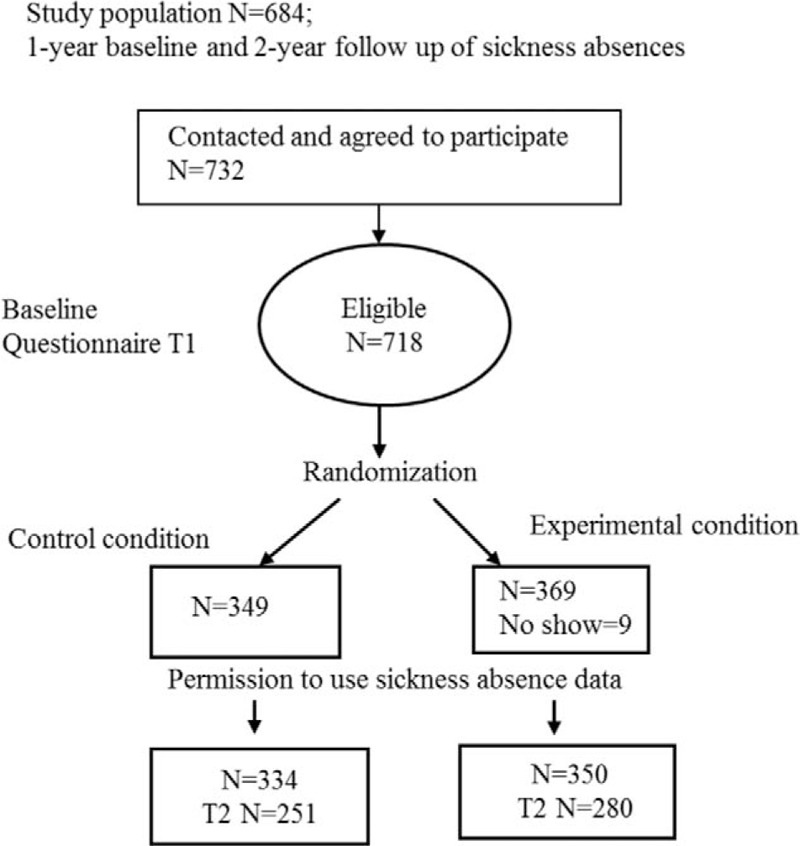
Flow chart of study design and study participants (T2 refers to respondents to time 2 measurement of proximal effects).
Of these 718 participants, 684 (350 in the intervention group and 334 in the comparison group) granted permission for the collection of their individual sickness absence data from the organizations’ absence registers.
A total of 34 workshops were carried out in the 17 participating organizations. The groups consisted of 6 to 15 employees and/or supervisors. The workshops lasted for 16 hours total. In most cases, they were organized as 4 half-day sessions during 2 consecutive weeks.
When we analyzed the no-show bias in the intervention, we found that the nine no-show participants were more often employed by the government than by municipal or private organizations (P < 0.05). Importantly, there were no differences at the baseline between the factors relating to the participants and the factors relating to those who did not give the permission to use their sickness absence data.
Intervention
The resource-enhancing intervention Towards Successful Seniority was developed at the Finnish Institute of Occupational Health to be implemented at workplaces to promote career management preparedness.11 The method was designed to be implemented as a collaboration tool for the occupational health services and human resources of organizations. The modules of the program included 4 half-day sessions, 16 hours in total. The program was recommended to be implemented at the workplace during working hours. The first half-day introduced skills training element, which includes defining one's own skills and strengths, and career goals and interests. The second half-day focused on the need for lifelong learning and coping with changes. The participants also familiarized themselves with change management and had a chance to interview an informant. The third module introduced obtaining career-related social resources, solving social conflicts, and managing stress and one's career. Finally, the participants built their own near-future career plan and committed to it before finishing the program.
One main theme of the program was individual well-being and health resources, as well as different options for, for example, decreasing job strain (flexibility at work, different options for sabbatical, etc.). Another theme was providing participants with the means, solutions, and confidence to manage their everyday challenges and problems. The group method was based on the mechanisms of strengthening self-efficacies and inoculation against setbacks, which together constitute the concept of career management preparedness.29
The method is based on active learning methods by making use of participants’ own career knowledge and skills in discussions and role plays. The skilled trainers work in pairs in order to facilitate group processes and give positive feedback. Social support is also provided by facilitating modeling and strengthening supportive behavior in the groups. Inoculation training helps in preparation against setbacks.11
MEASURES
Register-based Data on Sickness Absence
The sickness absence data were collected from the participating organizations’ comprehensive registers with the permission of the individual participants. The data covered all absence days and episodes of absences between 1 year before the intervention (baseline) and approximately 2 years after the intervention. In the registers, each absence episode is given a code indicating cause of absence, making it possible to differentiate absences related to individuals’ own sickness from, for example, caring for one's sick child. The length of follow-up was adjusted in the analyses for each person separately to exploit all the data available, as the follow-up time period slightly varied between the organizations. We used several sickness absence episode lengths to investigate the effects of the intervention. For instance, absences lasting 1 to 3 days are usually self-reported in organizations, whereas longer absences require a certificate. Furthermore, absences longer than approximately 2 weeks are partly reimbursed by social security and no longer fully compensated by employer. Data on sickness absence episodes did not include information on possible diagnoses.
Sociodemographic Factors
We used age, gender, and organization as sociodemographic covariates in the analysis.
Statistical Analysis
For each participant, we computed the number of sickness absence days, and the number of sickness absence episodes of different lengths during the period of 1 year before the intervention, and 2 years after the intervention, respectively. The outcome variables were adjusted using previous sickness absence in each absence category during a period of 1 year before the intervention. All models were also adjusted for age, gender and organization. The differences between the study groups in the variables at baseline were measured using Chi-square test and t tests.
As the statistical method for investigating Hypothesis 1, that is, whether intervention was successful in reducing the number of sickness absences, we used the Zero-Inflated Negative Binomial model (ZINB) in the analyses. The response was a count for different categories of absence days and episodes of absence. The distribution of these variables was clearly non-normal; they were skewed, and zero count was by far the most common value in the data. When comparing Poisson and negative binomial distributions with AIC and BIC fit-indices, the ZINB model performed best. We used GENMODE procedure of the SAS/STAT® version 9.4, statistical software (SAS Institute Inc, Cary, NC).
To study Hypotheses 2, that is, whether the effect of the intervention on longer sickness absences was mediated by career management preparedness, we estimated mediation model with MPlus Poisson regression analysis and Bootstrap method (confidence intervals and P value in two-tailed test). The model estimates indirect effect of the intervention on longer sickness absences via career management preparedness, taking into account the baseline level of preparedness. If the indirect effect is significant, the effect of the intervention is mediated via increase in preparedness due to the intervention.
According to the principals of Baron and Kenny, this was accomplished in a three-step procedure. First, preparedness was modeled at T2 to study the effect of the intervention on preparedness. Next, two models, with and without the preparedness variable at T2, were modeled to the study the effect of the intervention on the outcome variables. A variable functions as a mediator when it either eliminates or significantly reduces the effect of the independent variable (intervention) on the outcome.
RESULTS
There were no statistically significant differences in gender, age, or self-reported number of diagnosed illnesses at the baseline between the participants and nonparticipants. Most of the participants were women (n = 599; 88%) and aged between 40 and 59 years (Table 1).
TABLE 1.
Characteristics of Study Population by Intervention Group at the Baseline and During Follow-Up
| All (N = 684) | Intervention Group (N = 350) | Control Group (N = 334) | Difference Between the Groups (t test, P) | Sum of Absences Per Year in Intervention/Control Group | |
| Demographic variables (N, % or Mean, SD) | |||||
| Sex | Chi-square P = 0.131 | ||||
| Men | 85 (12%) | 50 (14%) | 35 (10%) | ||
| Women | 599 (88%) | 300 (86%) | 299 (90%) | ||
| Age | 50.02 (6.53) | 50.44 (6.57) | 49.58 (6.46) | −1.58, P = 0.116 | |
| Baseline sickness absence; Mean per person/year (SD) | |||||
| Sickness absence days | 11.85 (27.88) | 10.93 (28.50) | 12.81 (27.23) | 0.89, P = 0.375 | 3,876/4,270 |
| Sickness absence episodes | 1.75 (2.13) | 1.62 (1.92) | 1.88 (2.32) | 1.60, P = 0.110 | 580/622 |
| Short episodes (<4 days) | 1.20 (1.57) | 1.12 (1.46) | 1.29 (1.67) | 1.47, P = 0.142 | 398/427 |
| Long episodes (≥4 days) | 0.54 (1.00) | 0.50 (0.89) | 0.58 (1.11) | 1.10, P = 0.272 | 182/195 |
| Longer episodes (>14 days) | 0.14 (0.39) | 0.12 (0.35) | 0.16 (0.42) | 1.11, P = 0.267 | 43/52 |
| Sickness absence during follow-up; Mean per person/year (SD) | |||||
| Sickness absence days | 13.61 (29.23) | 12.22 (24.12) | 15.07 (33.74) | 1.56, P = 0.120 | 4,288/5,020 |
| Sickness absence episodes | 1.82 (2.10) | 1.76 (1.94) | 1.90 (2.26) | 1.27, P = 0.205 | 619/627 |
| Short episodes (<4 days) | 1.26 (1.58) | 1.22 (1.45) | 1.31 (1.70) | 1.22, P = 0.223 | 430/433 |
| Long episodes (≥4 days) | 0.56 (0.83) | 0.58 (0.86) | 0.54 (0.80) | 1.01, P = 0.314 | 189/194 |
| Longer episodes (>14 days) | 0.16 (0.33) | 0.15 (0.30) | 0.17 (0.37) | 0.58, P = 0.565 | 52/55 |
We found no differences between the experimental and the control group at baseline in any sickness absence variables. This indicates that the randomization was successful. As presented in Table 1, the mean level of sickness absence episodes seemed to increase in both intervention and control group during the follow-up.
The effects of the intervention on sickness absence were studied for 2 years after the intervention. Total sickness absence days and sickness absence episodes of different length were calculated. The baseline absence, age, and gender were taken into account in the analyses.
The results showed that there were no statistically significant differences between total sickness absence days or sickness absence episodes of the intervention and the comparison group. However, the number of very long-term sickness absence episodes was significantly lower in the intervention group than in the control group during the follow-up indicating a significant negative effect of the intervention on longer sickness absences (Table 2).
TABLE 2.
Main Effects of the Intervention on Sickness Absence Days and Episodes
| Model 0 | Model 1 | Model 2 | ||||
| Model | OR (95% CI) | P | OR (95% CI) | P | OR (95% CI) | P |
| Sickness absence days | 0.82 (0.62–1.08) | 0.158 | 0.78 (0.61–1.00) | 0.054 | 0.86 (0.68–1.09) | 0.208 |
| Sickness absence episodes (all) | 0.92 (0.78–1.11) | 0.416 | 0.92 (0.79–1.07) | 0.291 | 1.06 (0.94–1.21) | 0.324 |
| Short episodes (<4 days) | 0.92 (0.76–1.12) | 0.404 | 0.95 (0.81–1.11) | 0.529 | 1.07 (0.93–1.23) | 0.363 |
| Long episodes (≥4 days) | 0.87 (0.66–1.14) | 0.322 | 0.80 (0.65–1.00) | 0.050 | 0.88 (0.72–1.07) | 0.206 |
| Longer episodes (>14 days) | 0.65 (0.42–1.00) | 0.048 | 0.51 (0.34–0.78) | 0.001 | 0.53 (0.35–0.82) | 0.004 |
Model 0. Crude.
Model 1. Adjusted for age, gender, and organization.
Model 2. Adjusted for age, gender, organization, and previous absence.
Models adjusted for previous absence, age, gender, and organization (ZINB models).
95% CI, 95% confidence interval; OR, odds ratio.
In the mediation analyses, the non-normality of the outcome variable was taken into account.27 Indirect effects analysis of MPlus using Poisson regression method with bootstrap standard errors was being used for investigating whether the effect of the intervention on sickness absences is mediated via preparedness as the proximal effect of the intervention. The results suggest a mediation effect, as the indirect effect of the intervention on very long sickness absences (Estimate −0.034; confidence intervals −0.069 and −0.005; P = 0.054) was significant in one-sided testing.
DISCUSSION
The aim of the study was to investigate the effects of a career management group intervention in preventing sickness absenteeism. The main result was that the intervention was effective in preventing long (2 weeks or more) sickness absence episodes. In the participating organizations, this meant that the overall trend of increasing sickness absences during the follow-up was slightly attenuated due to the intervention among experimental group. This effect seemed to be most pronounced in the category of three or more long sickness absence episodes indicating that the benefits of the intervention could be focused on reducing repeated absence episodes. We found no statistically significant effect on short absence episodes or the total number of sickness absence days. In addition to the significant direct effect of the intervention on long sickness absence episodes, the results suggest that the decrease in long sickness absences was at least partly mediated by enhanced career management preparedness, which has previously been found to be the proximal effect of the intervention.11
One plausible explanation for these results is that the intervention does not prevent disabling health problems as such, but strengthens employees’ psychological resources to return to work after sickness absence without delays related to “yellow flags,” that is, psychological factors associated with unfavorable clinical outcomes and the transition to persistent disability.28 Longer episodes were so rare in this population that a significant difference between the total numbers of sickness absence days between the two study groups would have required more participants.
Our main result is in accordance with and strengthens the earlier findings that have reported positive long-term effects of career management interventions. It has been found that the intervention reduces symptoms of depression and increases mental resources of the work ability index,11 intrinsic work motivation,15 and work engagement among young employees.29 The result reveals that it is feasible to invest in preparedness for career management as a mean to prevent long-term sickness absence at workplaces. According to the best of our knowledge, this is the first controlled intervention study, in this case an RCT study, that demonstrates the causal effect of a career management group intervention on sickness absenteeism among working employees. Previous research has found positive effects of interventions among employees on sick leave23,30 or in specific risk groups.24
Our study has several strengths. First, the measure for sickness absence is based on the comprehensive sickness absence registers of the participating organizations. The empirical literature has typically used subjective measures for sickness absence that are prone to nonresponse, recall bias, or rounding error. Second, we were able to control for previous absence during the 1-year period before the intervention. A 1-year baseline has been deemed to be an appropriate time frame for a sickness absence baseline.1 Third, and most importantly, randomized controlled trials with a reasonable number of subjects are very rare in workplace contexts and are considered as the “golden standard” of methodology in intervention studies. In our study, we succeeded in conducting a randomized controlled trial with no baseline differences in the study variables between the study groups. A small number of respondents did not grant permission for the researchers to collect their personal sickness absence data from the company registers, but we found no significant differences between any background or health variables of the compliants and non-compliants.
Participation in our intervention was voluntary in the organizations and we did not select the participants. In most organizations, our intervention was particularly marketed to employees aged over 40 years. The mean age of the participants was consequently 50, and most of them were women in white-collar occupations. Because most of the participating organizations also had a female majority, the study sample is not representative of the whole working-age population.
Our results also support the acknowledged need to develop early preventive work-related interventions that have also previously been more effective treatment for common mental disorders, and more effectively supported return to work than ordinary Cognitive Behavioral Therapy.30 Several studies show that workplace psychosocial factors predict or interact with sickness absence.31–34 It remains an open issue for future studies to strengthen this evidence, as most previous interventions do not take advantage of the work context of employees when enhancing their resources.
As working life demands increase, the working population ages, and employees need to manage at work longer despite chronic illnesses, more emphasis should be given to developing preventive interventions for the working population and finding the most cost-effective ways to implement them. Preparedness for career management intervention seems to provide promising possibilities for improving workers’ abilities to cope with these phenomena.
Footnotes
This article is based on research supported by the Finnish Work Environment Fund (#106093), the Finnish Ministry of Finance (#31/37/2007), and the Academy of Finland (#124294).
The authors do not have any conflicts of interest.
REFERENCES
- 1.Roelen CAM, Koopmans PC, Schreuder JAH, et al. The history of registered sickness absence predicts future sickness absence. Occup Med 2012; 61:96–101. [DOI] [PubMed] [Google Scholar]
- 2.Anema JR, van der Beek AJ. Medically certified sickness absence. BMJ 2008; 337:a1174. [DOI] [PubMed] [Google Scholar]
- 3.Ferrie J, Kivimäki M, Westerlund H, et al. Differences in the association between sickness absences and long-term suboptimal health by occupational position: a 14-year follow-up in the GAZEL cohort. Occup Environ Med 2011; 68:729–733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Vahtera J, Westerlund H, Ferrie J, et al. All-cause and diagnosis-specific sickness absence as a predictor of sustained suboptimal health: a 14-year follow-up in the GAZEL cohort. J Epidem Comm Health 2010; 64:311–317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Virtanen M, Kivimäki M, Vahtera J, et al. Sickness absence as a risk factor for job termination, unemployment, and disability pension among temporary and permanent employees. Occup Environ Med 2006; 63:212–217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gjesdal S, Ringdal PR, Haug K, Mæland J. Predictors of disability pension in long-term sickness absence. Eur J Public Health 2004; 14:398–405. [DOI] [PubMed] [Google Scholar]
- 7.Vuori J, Price RH, Mutanen P, et al. Effective group training techniques in job search training. J Occup Health Psychol 2005; 10:261–275. [DOI] [PubMed] [Google Scholar]
- 8.Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process 1991; 50:179–211. [Google Scholar]
- 9.Bandura A. Social Foundations of Thought and Action. New York, NY: Prentice Hall; 1986. [Google Scholar]
- 10.Meichenbaum D. Stress Inoculation Training: A Clinical Guidebook. Elmsforth, NY: Pergamon Press; 1985. [Google Scholar]
- 11.Vuori J, Toppinen-Tanner S, Mutanen P. Effects of resource building group intervention in work organizations on career management and mental health: randomized controlled field trial (RCT). J Appl Psychol 2012; 97:273–286. [DOI] [PubMed] [Google Scholar]
- 12.McGonagle AK, Beatty JE, Joffe R. Coaching for workers with chronic illness: evaluating an intervention. J Occup Health Psychol 2014; 19:385–398. [DOI] [PubMed] [Google Scholar]
- 13.Vuori J, Price RH. Hartung PJ, Savickas ML, Walsh WB. Evidence-based job search interventions for unemployed workers and youth. APA Handbook of Career Intervention. Washington, DC: APA; 2015. 321–335. [Google Scholar]
- 14.Ahola K, Vuori J, Toppinen-Tanner S, et al. Resource-enhancing group method against depression at workplace: who benefits? A randomised controlled study with a 7-month follow-up. Occup Environ Med 2012; 69:870–876. [DOI] [PubMed] [Google Scholar]
- 15.Salmela-Aro K, Mutanen P, Vuori J. Promoting career preparedness and intrinsic work-goal motivation: RCT intervention. J Vocat Behav 2012; 80:67–75. [Google Scholar]
- 16.Bhui KS, Dinos S, Stansfeld S, White PD. A synthesis of the evidence for managing stress at work: a review of the reviews reporting on anxiety, depression, and absenteeism. J Environ Public Health 2012; 2012:515874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Stansfeld SA, Fuerer R, Head J. Impact of common mental disorders on sickness absence in an occupational cohort study. Occup Environ Med 2011; 68:408–413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Väänänen A, Toppinen-Tanner S, Kalimo R, et al. Job characteristics, physical and psychological symptoms, and social support as antecedent of sickness absence among men and women in the private industrial sector. Soc Sci Med 2003; 57:807–824. [DOI] [PubMed] [Google Scholar]
- 19.Mitchell AJ, Rao S, Vaze A. Can general practitioners identify people with distress and mild depression? A meta-analysis of clinical accuracy. J Affect Disord 2011; 130:26–36. [DOI] [PubMed] [Google Scholar]
- 20.Olaya-Contreras P, Persson T, Styff J. Comparison between the Beck Depression Inventory and psychiatric evaluation of distress in patients on long-term sick leave due to chronic musculoskeletal pain. J Multidiscip Healthc 2010; 3:161–167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Knudsen AK, Harvey SB, Mykletun A, Overland S. Common mental disorders and long-term sickness absence in general working population: the Hordaland Health Study. Acta Psychiatr Scand 2013; 127:287–297. [DOI] [PubMed] [Google Scholar]
- 22.Martimo KP. Reducing sickness absenteeism at the workplace: what to do and how? [editorial]. Scand J Work Environ Health 2006; 32:253–255. [DOI] [PubMed] [Google Scholar]
- 23.Van der Klink J, Blonk R, Schene A, et al. Reducing long-term sickness absence by an activating intervention in adjustment disorders: a cluster randomized controlled design. Occup Environ Med 2003; 60:437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Willert MV, Thulstrup AM, Bonde JP. Effects of a stress management intervention on absenteeism, and return to work: results from a randomized wait-list controlled trial. Scand J Work Environ Health 2011; 37:186–195. [DOI] [PubMed] [Google Scholar]
- 25.Lexis MAS, Jansen NWH, Huibers MJH, et al. Prevention of long-term sickness absence and major depression in high-risk employees: a randomized controlled trial. Occup Environ Med 2011; 68:400–407. [DOI] [PubMed] [Google Scholar]
- 26.Linden M, Mushalla B, Hansmeier T, et al. Reduction of sickness absence by an occupational health care management program focusing on self-efficacy and self-management. Work 2013; 47:485–489. [DOI] [PubMed] [Google Scholar]
- 27.Wang W, Albert JM. Estimation of mediation effects for zero-inflated regression models. Stat Med 2012; 31:3118–3132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Buck R, Barnes MC, Cohen D, et al. Common health problems, yellow flags and functioning in a community setting. J Occup Rehabil 2010; 20:235–246. [DOI] [PubMed] [Google Scholar]
- 29.Akkermans J, Brenninkmeijer V, Schaufeli WB, Blonk RWB. It's all about careerskills: effectiveness of a career development intervention for young employees. Human Res Manag 2015; 54:533–551. [Google Scholar]
- 30.Lagerveld S, Blonk RWB, Brenninkmeijer V, et al. Work-focused treatment of common mental disorders and return to work: a comparative outcome study. J Occup Health Psychol 2012; 17:220–234. [DOI] [PubMed] [Google Scholar]
- 31.Ahola K, Virtanen M, Honkonen T, et al. Common mental health disorders and subsequent work disability: a population-based Health 2000 Study. J Affect Disord 2011; 134:365–372. [DOI] [PubMed] [Google Scholar]
- 32.Duijts SFA, Kant I, Swaen GMH, et al. A meta-analysis of observational studies identifies predictors of sickness absence. J Clin Epidemiol 2007; 60:1105–1115. [DOI] [PubMed] [Google Scholar]
- 33.van der Berg TI, Robroek SJ, Plat JF, Koopmanschap MA, Burdorf A. The importance of job control for workers with decreased work ability to remain productive at work. Int Arch Occup Environ Health 2011; 84:705–712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Virtanen M, Vahtera J, Pentti, et al. Job strain and psychological distress. Influence on sickness absence among Finnish employees. Am J Prevent Med 2007; 33:182–187. [DOI] [PubMed] [Google Scholar]