

Abstract
Diffuse large B-cell lymphoma (DLBCL) patients with high Ki-67 expression receive limited benefits from R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) therapy. This study aims to compare the R-EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin) and R-CHOP regimens as first-line therapy in DLBCL patients with high Ki-67 expression. Data from 44 untreated DLBCL patients with high Ki-67 expression receiving R-EPOCH therapy were matched with those from 132 untreated DLBCL patients with high Ki-67 expression receiving R-CHOP therapy based on the International Prognostic Index (IPI: age, Ann Arbor stage, performance status, LDH level, number of extranodal sites), gender, and Ki-67 expression. In the R-EPOCH group, 42/44 patients were eligible for response evaluation. A total of 35 patients (83.3%) achieved complete remission (CR); 6 patients (14.3%) achieved partial remission (PR); and one patient (2.4%) exhibited progressive disease (PD) after 2 cycles of therapy. Patients in the R-EPOCH group presented better survival outcomes than those in the R-CHOP group (3-year overall survival [OS]: 89.9% vs. 70.2%, p = 0.041; 3-year progression-free survival [PFS]: 86.6% vs. 59.7%, p = 0.024). The survival superiority of the R-EPOCH over the R-CHOP regimen persisted when considering only patients of low-to-intermediate IPI risk, but it was not observed in those of high IPI risk. Our data suggest that R-EPOCH could be superior to R-CHOP as a first-line regimen in DLBCL patients with high Ki-67 expression, especially in those of low-to-intermediate IPI risk.
Keywords: R-EPOCH, DLBCL, Ki-67 expression, R-CHOP
INTRODUCTION
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma (NHL), accounting for 30%–40% of all NHL patients [1–3]. DLBCL is considered to be a heterogeneous entity based on its biological characteristics and clinical outcomes [3–5]. R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) is the first-line standard treatment for DLBCL because the addition of rituximab to CHOP chemotherapy notably improves survival outcomes [6, 7]. However, some DLBCL patients continue to present an inferior prognosis under standard R-CHOP therapy. Therefore, many studies have been performed in an attempt to improve the current treatment for DLBCL with a poor prognosis [8–10].
For tumors with high proliferation, the EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin) regimen is based on the concept that the extension of drug exposure may yield better antitumor efficacy than a bolus regimen, such as CHOP [11–13]. Ki-67, a useful prognostic factor in various neoplasms, is considered to be a proliferation index [14, 15]. In a previous study, we found that DLBCL patients with high Ki-67 expression received limited survival benefits from R-CHOP therapy [16]. Hence, the present study aimed to investigate whether R-EPOCH is superior to R-CHOP in untreated DLBCL patients with high Ki-67 expression.
RESULTS
Patient characteristics
A total of 44 DLBCL patients with high Ki-67 expression in the study group treated with R-EPOCH and 132 DLBCL patients with high Ki-67 expression in the control group treated with R-CHOP were compared via matched-pair analysis. The clinical characteristics of all patients in both groups are shown in Table 1. The median age of the study group was 46 years (range: 19–69 years) and 48 years (range: 21–74) in the control group. An elevated LDH level and advanced disease (Ann Arbor stage III–IV) were found in 45% and 43% of the patients in the two groups, respectively. IPI score of 0–3 was observed in 82% of the patients in both groups. Bulky disease was present in 8 patients (18%) from the study cohort and 23 patients (17.4%) from the control cohort. The main clinical features of the patients were comparable in the study and control groups.
Table 1. Patient characteristics in the R-EPOCH and R-CHOP groups.
| Characteristics | Total (N = 176) | R-EPOCH group (N = 44) | R-CHOP group (N = 132) | P-value |
|---|---|---|---|---|
| Age (years) | ||||
| ≤ 60 | 148 | 37 | 111 | 1.0 |
| ≥ 60 | 28 | 7 | 21 | |
| Gender | ||||
| Male | 80 | 20 | 60 | 1.0 |
| Female | 96 | 24 | 72 | |
| Ann Arbor Stage | ||||
| I–II | 76 | 19 | 57 | 1.0 |
| III–IV | 100 | 25 | 75 | |
| B symptoms | ||||
| Absent | 115 | 29 | 86 | 0.927 |
| Present | 61 | 15 | 46 | |
| ECOG performance status | ||||
| 0–1 | 144 | 36 | 108 | 1.0 |
| ≥ 2 | 32 | 8 | 24 | |
| LDH level | ||||
| Normal | 80 | 20 | 60 | 1.0 |
| Elevated | 96 | 24 | 72 | |
| Bulky disease | ||||
| No | 144 | 36 | 109 | 0.909 |
| Yes | 32 | 8 | 23 | |
| IPI score | ||||
| 0–3 | 144 | 36 | 108 | 1.0 |
| 4–5 | 32 | 8 | 24 |
Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; LDH, lactate dehydrogenase;IPI, International Prognostic Index.
All patients and control subjects included in the study exhibited high Ki-67 expression (≥ 80%). The Ki-67 expression status (80%–90% vs. > 90%) was one of the matching variables in both the study group and the control group. A total of 75% of all patients in the R-EPOCH group (33 cases) and in the R-CHOP group (99 cases) exhibited Ki-67 expression, ranging from 80%–90%. Approximately three-fourths (26 cases, 76%) of the patients in the study group showed positive bcl-2 expression. The non-GCB subtype was found in 16 patients (18/34, 53%) and 45 patients (58/103, 56%) in the R-EPOCH and R-CHOP groups, respectively. The immunohistochemical expression of biomarkers in the R-EPOCH and R-CHOP groups is summarized in Table 2. No significant difference in the unmatched clinical features and biomarker expression was observed in the R-EPOCH and R-CHOP groups.
Table 2. Biomarkers in the R-EPOCH and R-CHOP groups.
| Biomarkers | Total (No. evaluated) | R-EPOCH group (No. evaluated) | R-CHOP group (No. evaluated) | P-value |
|---|---|---|---|---|
| Ki-67 | 176 | 44 | 132 | 1.0 |
| ≤ 90% | 132 | 33 | 99 | |
| > 90% | 44 | 11 | 33 | |
| BCL-2 | 149 | 34 | 115 | 0.690 |
| Negative | 39 | 8 | 31 | |
| Positive | 110 | 26 | 84 | |
| DLBCL subtype | 137 | 34 | 103 | 0.732 |
| GCB | 61 | 16 | 45 | |
| Non-GCB | 76 | 18 | 58 | |
| BCL-6 | 139 | 36 | 103 | 0.627 |
| Negative | 51 | 12 | 39 | |
| Positive | 88 | 24 | 64 | |
| CD10 | 151 | 36 | 115 | |
| Negative | 93 | 21 | 72 | 0.645 |
| Positive | 58 | 15 | 43 | |
| Mum-1 | 131 | 32 | 99 | |
| Negative | 40 | 10 | 30 | 0.919 |
| Positive | 91 | 22 | 69 |
Treatment outcomes and toxicity in the R-EPOCH group
In the R-EPOCH group, 42 patients (95.5%) were eligible for response evaluation. Complete remission (CR) was achieved in 35 patients (83.3%), and partial remission was achieved in 6 patients (14.3%). One patient exhibited disease progression after 2 cycles of R-EPOCH therapy. Within a median follow-up of 30.6 months (range, 7.3–71.4 months), 3 patients died of progressive lymphoma, and one patient died of cardiovascular disease.
A total of 218 cycles of R-EPOCH therapy were administered, with a median of 4 cycles (range: 2 to 8 cycles). The major side effect of the R-EPOCH regimen was hematologic toxicity. Grade 3/4 neutropenia, anemia and thrombocytopenia were observed in 32.2% (70 cycles), 4.6% (10 cycles), and 9.2% (20 cycles) of the cycles, respectively. Neutropenic fever developed in 13.8% of the cycles (30 cycles). Mild peripheral neuropathy was present in approximately one-third of the patients (13 patients, 29.5%) but was mild and controllable. The observed gastrointestinal toxicity, which included vomiting, mucositis and constipation, was mild to moderate and manageable. Cardiac toxicity from epirubicin (EPI) or pirarubicin (THP) did not exhibit any significant impact on R-EPOCH administration. No patients exhibited a decrease in the cardiac ejection fraction leading to a discontinuation of EPI (or THP) or the development of congestive heart failure. No treatment-related deaths were observed in the R-EPOCH group.
Survival outcomes and prognostic factors
In the R-CHOP group, the 3-year OS and PFS rates were 70.2% and 59.7%, respectively. The patients in the R-EPOCH group presented superior survival outcomes over those in the R-CHOP group (3-year OS: 89.9% vs. 70.2%, p = 0.041; 3-year PFS: 86.6% vs. 59.7%, p = 0.024), as shown in Figure 1. The survival superiority of the R-EPOCH regimen over the R-CHOP regimen remained in patients who showed Ki-67 expression of 80%–90% (3-year OS: 86.7% vs. 63.1%, p = 0.036; 3-year PFS: 83.6% vs. 57.4%, p = 0.019, as indicated in Figure 2), but not in patients who showed Ki-67 expression > 90% (p = 0.719 in OS, and p = 0.745 in PFS). Figure 3 shows the comparison of survival outcomes in the R-EPOCH and R-CHOP groups according to IPI risk. In patients with a low-to-intermediate-risk IPI (IPI score of 0–3), the R-EPOCH regimen resulted in better survival outcomes than did the R-CHOP regimen (3-year OS: 100% vs. 81.1%, p = 0.017; 3-year PFS: 97.1% vs. 74.3%, p = 0.010). However, no survival benefit was found in patients with a high-risk IPI (IPI score: 4–5) treated with the R-EPOCH regimen compared with those with a high-risk IPI treated with the R-CHOP regimen (3-year OS: 37.5% vs. 35.5%, p = 0.604; 3-year PFS: 33.3% vs. 25.1%, p = 0.483).
Figure 1. Survival outcomes in the R-EPOCH and R-CHOP groups.
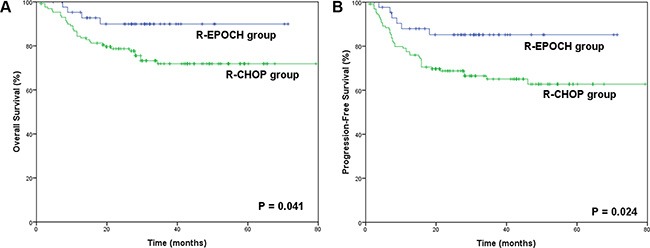
(A) Overall survival (OS) in the R-EPOCH and R-CHOP groups. (B) Progression-free survival (PFS) in the R-EPOCH and R-CHOP groups.
Figure 2. Survival outcomes in the R-EPOCH and R-CHOP groups according to the Ki-67 expression status.

(A) Overall survival (OS) in the R-EPOCH and R-CHOP groups with Ki-67 expression of 80%–90%. (B) Progression-free survival (PFS) in the R-EPOCH and R-CHOP groups with Ki-67 expression greater than 90%.
Figure 3. Survival outcomes in the R-EPOCH and R-CHOP groups according to the International Prognostic Index (IPI).
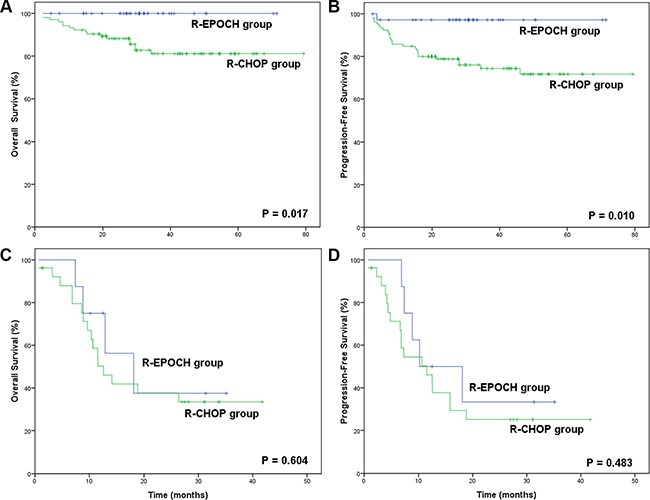
(A) Overall survival (OS) in the R-EPOCH and R-CHOP groups with low-to-intermediate IPI risk. (B) Progression-free survival (PFS) in the R-EPOCH and R-CHOP groups with low-to-intermediate IPI risk. (C) Overall survival (OS) in the R-EPOCH and R-CHOP groups with high IPI risk. (D) Progression-free survival (PFS) in the R-EPOCH and R-CHOP groups with high IPI risk.
Table 3 lists the results of the univariate analysis of prognostic factors for survival outcomes in the R-EPOCH group. The following variables were found to have an adverse impact on survival outcomes: high-risk IPI (p < 0.001 in both OS and PFS), bulky disease (p < 0.001 in both OS and PFS) and B symptoms (p = 0.002 in OS, and p = 0.019 in PFS). Due to the limited sample size of the R-EPOCH group, multivariate analysis was not performed further.
Table 3. Univariate analysis of prognostic factors for survival in the R-EPOCH group.
| Parameters | Overall survival (OS) P-value | Progression-free survival (PFS) P-value |
|---|---|---|
| IPI score (0–3 vs. 4–5) | < 0.001 | < 0.001 |
| Bulky disease | < 0.001 | < 0.001 |
| B symptoms | 0.002 | 0.019 |
| Bcl-2 expression status | 0.256 | 0.203 |
| CD10 expression status | 0.534 | 0.317 |
| Bcl-6 expression status | 0.526 | 0.209 |
| Mum-1 expression status | 0.915 | 0.590 |
| DLBCL subtype | 0.385 | 0.202 |
Abbreviations: IPI, International Prognostic Index; DLBCL, diffuse large B-cell lymphoma.
DISCUSSION
Rituximab, which targets the CD20 antigen, was the first monoclonal antibody approved for use in patients with lymphoma [7]. The combination of rituximab and CHOP chemotherapy showed additional benefits in DLBCL patients in randomized controlled trials [17–20]. R-CHOP has been adopted as the standard first-line therapy for DLBCL [6]. However, DLBCL is an entity that presents heterogeneous biological characteristics and clinical behaviors [5]. Patients who exhibit poor clinical outcomes under standard R-CHOP therapy pose a difficult challenge. Many studies have made attempts to explore novel biological markers for identifying the patients who would receive limited benefits from R-CHOP therapy [16, 21–23].
Ki-67, a surrogate marker of proliferation, has been investigated in various neoplasms and found to be a powerful prognostic factor for survival outcomes [14, 16, 24–26]. Patients with highly proliferative tumors show much poorer survival than those with tumors characterized by low proliferation [24]. In a previous study, we investigated Ki-67 expression in DLBCL patients in the era of rituximab treatment. Our results indicated that high Ki-67 expression was associated with adverse clinical behaviors. Patients with a non-GCB subtype with high Ki-67 expression receive limited survival benefits from R-CHOP therapy [16]. Therefore, determining the optimal treatment for DLBCL patients with high Ki-67 expression remains a challenge.
The EPOCH regimen was designed based on experimental findings showing that continuous low-concentration exposure to drugs could enhance the effectiveness of cell-killing in malignant cells with high proliferation [11, 27, 28]. In addition, in vitro studies suggested that prolonged low-dose drug exposure could overcome the resistance mediated by MDR-1 in tumor cells [29]. The EPOCH regimen has shown promising results and safe profiles in relapse or refractory non-Hodgkin lymphomas [29–32]. The combination of the EPOCH regimen (or the dose-adjusted regimen) and rituximab has also been evaluated in several clinical trials [23–25]. Here, we administered R-EPOCH as a first-line regimen in DLBCL patients with high Ki-67 expression and compared the treatment efficacy of R-EPOCH and R-CHOP therapy in this subgroup using matched-pair controls. Our results suggested that patients treated with the R-EPOCH regimen exhibited better survival than those administered the R-CHOP regimen. The superiority of the R-EPOCH regimen persisted in patients showing Ki-67 expression of 80%–90% but not in patients exhibiting Ki-67 expression > 90%. The main reason for this result lies in the small sample size of patients showing Ki-67 expression > 90% (25%, 11 cases). Whether the R-EPOCH regimen shows better efficacy than the R-CHOP regimen in DLBCL patients with Ki-67 expression > 90% needs to be evaluated in a much larger population. When patients were stratified by IPI risk, it was found that the patients with a low-to-intermediate IPI risk received better survival benefits from the R-EPOCH regimen than the R-CHOP regimen. There were only 8 cases in the high-risk IPI group, and no significant difference in survival outcomes was found in the R-EPOCH and R-CHOP groups. The limited number of patients in the high-risk group might be one of the reasons for these negative results. The efficacy of R-EPOCH regimen in high-risk DLBCL patients is still uncertain [10, 36], which needs to be explored in the prospective studies. A phase III randomized study of comparison R-CHOP and R-EPOCH regimen in treating DLBCL in the US is still ongoing, and we are expecting the final results.
Certain biomarkers have been assessed to determine their relationship with survival outcomes in DLBCL patients treated with a dose-adjusted R-EPOCH regimen, such as bcl-2, bcl-6, and the GCB subtype [33, 35, 37]. However, the results have been controversial [33, 35, 37]. In the present study, common pathological biomarkers were also evaluated through univariate analysis, but no association with survival was found.
In conclusion, R-EPOCH could be superior to R-CHOP as a first-line regimen in DLBCL patients with high Ki-67 expression, particularly in those of low-to-intermediate IPI risk. Further prospective studies are warranted to confirm our findings and to identify possible prognostic biomarkers for use in association with R-EPOCH therapy.
MATERIALS AND METHODS
Patients and study design
Our cohort included 44 patients with untreated de novo DLBCL diagnosed at Sun Yat-Sen University Cancer Center, China, from May 2005 to October 2012. The patients included in this study fulfilled the following criteria: (1) histologically proven diagnosis of DLBCL with positive expression of CD20, according to the WHO classification of Tumours of Haematopoietic and Lymphoid Tissues [38]; (2) Ki-67 immunohistochemical expression ≥ 80%; (3) no previous treatment; (4) no previous neoplasm or second malignancy; (5) no severe coincident disease; and (6) available clinical information and follow-up data. Patients with primary central nervous system lymphoma and those with human immunodeficiency virus infection or DLBCL secondary to low-grade lymphoma were excluded from this cohort. Grey zone lymphoma and composite lymphoma were also excluded from this study. Antibodies to the following antigens were evaluated for immunophenotype analysis: CD10, Bcl-6, MUM1/IRF4, Bcl-2, CD20, CD79α, and CD3. Germinal center B-cell (GCB) and non-GCB DLBCL subtypes were classified based on the algorithm proposed by Hans et al. [39]. This study was performed in accordance with the Declaration of Helsinki, and it was approved by the Institutional Review Board (IRB) of Sun Yat-Sen University Cancer Center. Written informed consent was obtained from all patients before the collection of patients' information. The clinical available data included patient demographics, physical examination results, Eastern Cooperative Oncology Group (ECOG) performance status (PS), B symptoms, serum lactate dehydrogenase (LDH) levels, bone marrow examination results, and computed tomography (CT) or positron emission tomography/CT (PET/CT) scans. All patients were staged according to the Ann Arbor Staging system and analyzed using the International Prognostic Index (IPI: age, PS, stage, LDH level, and extranodal sites).
In the matched-pair analysis performed in this study, patients treated with R-EPOCH were matched to those receiving R-CHOP therapy during the same period at a ratio of 1:3. The source of the matching control group was 836 consecutive de novo DLBCL patients treated with R-CHOP as a first-line therapy at Sun Yat-Sen University between May 2005 and October 2012. The patients were matched for the following variables: gender (male vs. female), age (± 5 years), Ann Arbor stage (I–II vs. III–IV), ECOG PS (0–1 vs. 2–3), LDH levels (normal vs. elevated), extranodal sites (0–1 vs. ≥ 2), and Ki-67 expression (80%–90% vs. > 90%). All of the study cohort and the control group in the matched-pair analysis exhibited high Ki-67 expression (≥ 80%). All of the above factors were fully matched among the study cases and the three controls. If a case could be matched with more than 3 controls, the 3 controls were selected randomly.
Treatment and response criteria
All 44 patients in the study cohort received an EPOCH regimen combined with rituximab as first-line chemotherapy for 2 to 8 cycles (median, 6 cycles). Rituximab was administered on day 1 at a dose of 375 mg/m2. The EPOCH regimen included doxorubicin (10 mg/m2, continuous intravenous infusion, days 2 to 5), etoposide (50 mg/m2, continuous intravenous infusion, days 2 to 5), vincristine (0.4 mg/m2, continuous intravenous infusion, days 2 to 5), cyclophosphamide (750 mg/m2, intravenous bolus, day 6), and prednisone (60 mg/m2, orally, days 2 to 6). The R-EPOCH regimen was administered every 21 days.
In the matching control group, all patients were treated with R-CHOP as first-line therapy for 2 to 8 cycles (median 6 cycles). The administration of rituximab was as described above in the R-EPOCH regimen. The CHOP regimen included cyclophosphamide (750 mg/m2, day 2), doxorubicin (50 mg/m2, day 2), vincristine (1.4 mg/m2, at a maximal dose of 2 mg, day 2) and prednisone (60 mg/m2, days 2 to 6). The treatment schedule was repeated every 21 days.
In both the study cohort and the matching control group, involved field radiation (30–56 Gy) was delivered to the residual disease, extranodal sites, or previous bulky disease via a conventional fractionation scheme (daily fraction of 2 Gy, 5 fraction per week) after the chemotherapy.
The response to treatment was assessed according to the International Working Group Recommendation for Response Criteria for non-Hodgkin lymphoma [40, 41]. The evaluation of adverse effects after chemotherapy was based on the National Cancer Institute (NCI) criteria [42].
Immunohistochemistry for Ki-67
Immunohistochemical analysis of Ki-67 was carried out using a mouse monoclonal anti-Ki-67 antibody (1:100; Invitrogen, Carlsbad, CA, USA). Formalin-fixed, paraffin-embedded sections (4 μm thick) were deparaffinized and rehydrated through a graded series of alcohols. The immunohistochemical method for Ki-67 detection was performed as previously reported [16]. Ki-67 expression was detected in the nucleus of tumor cells. The proportion of cells showing Ki-67 expression was evaluated based on the number of lymphoma cells with nuclear immunoreactivity and the total number of tumor cells in the highest labeling field at high magnification (400 ×). High Ki-67 expression was considered to be present in this study when antibody staining for Ki-67 in the nucleus was observed in 80% or more of the lymphoma cells. Evaluation of the immunostaining and cell counts was performed independently at diagnosis by two pathologists who were blinded to the clinical outcomes of the patients.
Statistical analysis
The primary aim of this study was to compare the treatment efficacy of R-EPOCH and R-CHOP therapy as first-line regimens in DLBCL patients with high Ki-67 expression. Overall survival (OS) and progression-free survival (PFS) were the primary end points of this study. OS was calculated from the date of diagnosis to the date of death due to any cause or to the date of the last follow-up. PFS was calculated from the date of first progression, relapse, death, or the last follow-up. The Pearson's Chi-squared test was used to compare the categorical variables. Survival curves and univariate analysis were performed via the Kaplan-Meier method. Differences were determined using a two-tailed log-rank test, and p < 0.05 was considered statistically significant. Statistical analysis was carried out with SPSS 16.0 software.
Acknowledgments
We thank all the pathologists, oncologists, radiologists, surgeons and nurses who contributed.
Footnotes
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
GRANT SUPPORT
This work was supported by National Natural Science Foundation of China (NO. 81071950, 81301903), Guangdong Natural Science Foundation (NO. S2013010016331), Guangzhou science and technology project (NO. 2014J4100163), Fundamental Research Funds for the Central Universities (NO. 10ykpy36), National-Eleventh Five Technology Major Project (NO. 2008ZX09312-002, 2012ZX09301), and Research Award Funds for Outstanding Young Researchers in Sun Yat-Sen Cancer Center.
REFERENCES
- 1.Pileri SA, Agostinelli C, Sabattini E, Bacci F, Sagramoso C, Pileri A., Jr Falini B, Piccaluga PP. Lymphoma classification: the quiet after the storm. Semin Diagn Pathol. 2011;28:113–23. doi: 10.1053/j.semdp.2011.02.001. [DOI] [PubMed] [Google Scholar]
- 2.Moskowitz C. Diffuse large B cell lymphoma: how can we cure more patients in 2012? Best Pract Res Clin Haematol. 2012;25:41–7. doi: 10.1016/j.beha.2012.01.008. [DOI] [PubMed] [Google Scholar]
- 3.Abid MB, Nasim F, Anwar K, Pervez S. Diffuse large B cell lymphoma (DLBCL) in Pakistan: an emerging epidemic? Asian Pac J Cancer Prev. 2005;6:531–4. [PubMed] [Google Scholar]
- 4.Song CG, Huang JJ, Li YJ, Xia Y, Wang Y, Bi XW, Jiang WQ, Huang HQ, Lin TY, Li ZM. Epstein-Barr Virus-Positive Diffuse Large B-Cell Lymphoma in the Elderly: A Matched Case-Control Analysis. PLoS One. 2015;10:e0133973. doi: 10.1371/journal.pone.0133973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Harris NL, Jaffe ES, Diebold J, Flandrin G, Muller-Hermelink HK, Vardiman J. Lymphoma classification—from controversy to consensus: the R.E.A.L. and WHO Classification of lymphoid neoplasms. Ann Oncol. 2000;11:3–10. [PubMed] [Google Scholar]
- 6.Sehn LH1, Berry B, Chhanabhai M, Fitzgerald C, Gill K, Hoskins P, Klasa R, Savage KJ, Shenkier T, Sutherland J, Gascoyne RD, Connors JM. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood. 2007;109:1857–61. doi: 10.1182/blood-2006-08-038257. [DOI] [PubMed] [Google Scholar]
- 7.Coiffier B. Rituximab therapy in malignant lymphoma. Oncogene. 2007;26:3603–13. doi: 10.1038/sj.onc.1210376. [DOI] [PubMed] [Google Scholar]
- 8.Kirschey S, Flohr T, Wolf HH, Frickhofen N, Gramatzki M, Link H, Basara N, Peter N, Meyer RG, Schmitz N, Weidmann E, Banat A, Schulz A, et al. Rituximab combined with DexaBEAM followed by high dose therapy as salvage therapy in patients with relapsed or refractory B-cell lymphoma: mature results of a phase II multicentre study. Br J Haematol. 2015;168:824–34. doi: 10.1111/bjh.13234. [DOI] [PubMed] [Google Scholar]
- 9.Mytelka DS, Li L, Stafkey-Mailey D, Liepa AM, Hess LM, Farrelly E, Eaddy M. Treatment patterns and outcomes among patients with high-intermediate/high-risk diffuse large B-cell lymphoma in the USA. Hematology. 2014 Dec 31; doi: 10.1179/1607845414Y.0000000228. [DOI] [PubMed] [Google Scholar]
- 10.Purroy N, Bergua J, Gallur L, Prieto J, Lopez LA, Sancho JM, García-Marco JA, Castellví J, Montes-Moreno S, Batlle A, de Villambrosia SG, Carnicero F, Ferrando-Lamana L, et al. Long-term follow-up of dose-adjusted EPOCH plus rituximab (DA-EPOCH-R) in untreated patients with poor prognosis large B-cell lymphoma. A phase II study conducted by the Spanish PETHEMA Group. Br J Haematol. 2015;169:188–98. doi: 10.1111/bjh.13273. [DOI] [PubMed] [Google Scholar]
- 11.Wilson WH, Teruya-Feldstein J, Fest T, Harris C, Steinberg SM, Jaffe ES, Raffeld M. Relationship of p53, bcl-2, and tumor proliferation to clinical drug resistance in non-Hodgkin's lymphomas. Blood. 1997;89:601–9. [PubMed] [Google Scholar]
- 12.Broyde A, Boycov O, Strenov Y, Okon E, Shpilberg O, Bairey O. Role and prognostic significance of the Ki-67 index in non-Hodgkin's lymphoma. Am J Hematol. 2009;84:338–43. doi: 10.1002/ajh.21406. [DOI] [PubMed] [Google Scholar]
- 13.Miller TP, Grogan TM, Dahlberg S, Spier CM, Braziel RM, Banks PM, Foucar K, Kjeldsberg CR, Levy N, Nathwani BN. Prognostic significance of the Ki-67-associated proliferative antigen in aggressive non-Hodgkin's lymphomas: A prospective Southwest Oncology Group trial. Blood. 1994;83:1460–6. [PubMed] [Google Scholar]
- 14.Dziegiel P, Salwa-Zurawska W, Zurawski J, Wojnar A, Zabel M. Prognostic significance of augmented metallothionein (MT) expression correlated with Ki-67 antigen expression in selected soft tissue sarcomas. Histol Histopathol. 2005;20:83–9. doi: 10.14670/HH-20.83. [DOI] [PubMed] [Google Scholar]
- 15.Urruticoechea A, Smith IE, Dowsett M. Proliferation marker Ki-67 in early breast cancer. J Clin Oncol. 2005;23:7212–20. doi: 10.1200/JCO.2005.07.501. [DOI] [PubMed] [Google Scholar]
- 16.Li ZM, Huang JJ, Xia Y, Zhu YJ, Zhao W, Wei WX, Jiang WQ, Lin TY, Huang HQ, Guan ZZ. High Ki-67 expression in diffuse large B-cell lymphoma patients with non-germinal center subtype indicates limited survival benefit from R-CHOP therapy. Eur J Haematol. 2012;88:510–7. doi: 10.1111/j.1600-0609.2012.01778.x. [DOI] [PubMed] [Google Scholar]
- 17.Coiffier B, Lepage E, Briere J, Herbrecht R, Tilly H, Bouabdallah R, Morel P, Van Den Neste E, Salles G, Gaulard P, Reyes F, Lederlin P, Gisselbrecht C. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002;346:235–42. doi: 10.1056/NEJMoa011795. [DOI] [PubMed] [Google Scholar]
- 18.Feugier P, Van Hoof A, Sebban C, Solal-Celigny P, Bouabdallah R, Fermé C, Christian B, Lepage E, Tilly H, Morschhauser F, Gaulard P, Salles G, Bosly A, et al. Long-term results of the R-CHOP study in the treatment of elderly patients with diffuse large B-cell lymphoma: a study by the Groupe d'Etude des Lymphomes de l'Adulte. J Clin Oncol. 2005;23:4117–26. doi: 10.1200/JCO.2005.09.131. [DOI] [PubMed] [Google Scholar]
- 19.Habermann TM, Weller EA, Morrison VA, Gascoyne RD, Cassileth PA, Cohn JB, Dakhil SR, Woda B, Fisher RI, Peterson BA, Horning SJ. Rituximab-CHOP versus CHOP alone or with maintenance rituximab in older patients with diffuse large B-cell lymphoma. J Clin Oncol. 2006;24:3121–7. doi: 10.1200/JCO.2005.05.1003. [DOI] [PubMed] [Google Scholar]
- 20.Pfreundschuh M, Trümper L, Osterborg A, Pettengell R, Trneny M, Imrie K, Ma D, Gill D, Walewski J, Zinzani PL, Stahel R, Kvaloy S, Shpilberg O, et al. CHOP-like chemotherapy plus rituximab versus CHOP-like chemotherapy alone in young patients with good-prognosis diffuse large-B-cell lymphoma: a randomised controlled trial by the MabThera International Trial (MInT) Group. Lancet Oncol. 2006;7:379–91. doi: 10.1016/S1470-2045(06)70664-7. [DOI] [PubMed] [Google Scholar]
- 21.Evens AM, Sehn LH, Farinha P, Nelson BP, Raji A, Lu Y, Brakman A, Parimi V, Winter JN, Schumacker PT, Gascoyne RD, Gordon LI. Hypoxia-inducible factor-1 {alpha} expression predicts superior survival in patients with diffuse large B-cell lymphoma treated with R-CHOP. J Clin Oncol. 2010;28:1017–24. doi: 10.1200/JCO.2009.24.1893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bari A, Marcheselli L, Sacchi S, Marcheselli R, Pozzi S, Ferri P, Balleari E, Musto P, Neri S, Aloe Spiriti MA, Cox MC. Prognostic models for diffuse large B-cell lymphoma in the rituximab era: a never-ending story. Ann Oncol. 2010;21:1486–91. doi: 10.1093/annonc/mdp531. [DOI] [PubMed] [Google Scholar]
- 23.Copie-Bergman C, Gaulard P, Leroy K, Briere J, Baia M, Jais JP, Salles GA, Berger F, Haioun C, Tilly H, Emile JF, Banham AH, Mounier N, et al. Immuno-fluorescence in situ hybridization index predicts survival in patients with diffuse large B-cell lymphoma treated with R-CHOP: a GELA study. J Clin Oncol. 2009;27:5573–9. doi: 10.1200/JCO.2009.22.7058. [DOI] [PubMed] [Google Scholar]
- 24.Klapper W, Hoster E, Determann O, Oschlies I, van der Laak J, Berger F, Bernd HW, Cabeçadas J, Campo E, Cogliatti S, Hansmann ML, Kluin PM, Kodet R, et al. Ki-67 as a prognostic marker in mantle cell lymphoma-consensus guidelines of the pathology panel of the European MCL Network. J Hematop. 2009;2:103–11. doi: 10.1007/s12308-009-0036-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gerdes J, Lemke H, Baisch H, Wacker HH, Schwab U, Stein H. Cell cycle analysis of a cell proliferation-associated human nuclear antigen defined by the monoclonal antibody Ki-67. J Immunol. 1984;133:1710–5. [PubMed] [Google Scholar]
- 26.Szczuraszek K, Mazur G, Jeleń M, Dziegiel P, Surowiak P, Zabel M. Prognostic significance of Ki-67 antigen expression in non-Hodgkin's lymphomas. Anticancer Res. 2008;28:1113–8. [PubMed] [Google Scholar]
- 27.Moskowitz CH, Schöder H, Teruya-Feldstein J, Sima C, Iasonos A, Portlock CS, Straus D, Noy A, Palomba ML, O'Connor OA, Horwitz S, Weaver SA, Meikle JL, et al. Risk-adapted dose-dense immunochemotherapy determined by interim FDG-PET in Advanced-stage diffuse large B-Cell lymphoma. J Clin Oncol. 2010;28:1896–903. doi: 10.1200/JCO.2009.26.5942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lai GM, Chen YN, Mickley LA, Fojo AT, Bates SE. P-glycoprotein expression and schedule dependence of adriamycin cytotoxicity in human colon carcinoma cell lines. Int J Cancer. 1991;49:696–703. doi: 10.1002/ijc.2910490512. [DOI] [PubMed] [Google Scholar]
- 29.Jermann M, Jost LM, Taverna Ch, Jacky E, Honegger HP, Betticher DC, Egli F, Kroner T, Stahel RA. Rituximab-EPOCH, an effective salvage therapy for relapsed, refractory or transformed B-cell lymphomas: results of a phase II study. Ann Oncol. 2004;15:511–6. doi: 10.1093/annonc/mdh093. [DOI] [PubMed] [Google Scholar]
- 30.Martelli M, Di Rocco A, Russo E, Perrone S, Foà R. Primary mediastinal lymphoma: diagnosis and treatment options. Expert Rev Hematol. 2015;8:173–86. doi: 10.1586/17474086.2015.994604. [DOI] [PubMed] [Google Scholar]
- 31.Sparano JA, Lee JY, Kaplan LD, Levine AM, Ramos JC, Ambinder RF, Wachsman W, Aboulafia D, Noy A, Henry DH, Von Roenn J, Dezube BJ, Remick SC, et al. Rituximab plus concurrent infusional EPOCH chemotherapy is highly effective in HIV-associated B-cell non-Hodgkin lymphoma. Blood. 2010;115:3008–16. doi: 10.1182/blood-2009-08-231613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Dunleavy K, Pittaluga S, Maeda LS, Advani R, Chen CC, Hessler J, Steinberg SM, Grant C, Wright G, Varma G, Staudt LM, Jaffe ES, Wilson WH. Dose-adjusted EPOCH-rituximab therapy in primary mediastinal B-cell lymphoma. N Engl J Med. 2013;368:1408–16. doi: 10.1056/NEJMoa1214561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wilson WH, Jung SH, Porcu P, Hurd D, Johnson J, Martin SE, Czuczman M, Lai R, Said J, Chadburn A, Jones D, Dunleavy K, Canellos G, et al. A Cancer and Leukemia Group B multi-center study of DA-EPOCH-rituximab in untreated diffuse large B-cell lymphoma with analysis of outcome by molecular subtype. Haematologica. 2012;97:758–65. doi: 10.3324/haematol.2011.056531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.García-Suárez J, Flores E, Callejas M, Arribas I, Gil-Fernández JJ, Olmedilla G, Curto N, Guillén H, Casco CR, Martín Y, Burgaleta C. Two-weekly dose-adjusted (DA)-EPOCH-like chemotherapy with high-dose dexamethasone plus rituximab (DA-EDOCH14-R) in poor-prognostic untreated diffuse large B-cell lymphoma. Br J Haematol. 2013;160:510–4. doi: 10.1111/bjh.12144. [DOI] [PubMed] [Google Scholar]
- 35.Wilson WH, Dunleavy K, Pittaluga S, Hegde U, Grant N, Steinberg SM, Raffeld M, Gutierrez M, Chabner BA, Staudt L, Jaffe ES, Janik JE. Phase II study of dose-adjusted EPOCH and rituximab in untreated diffuse large B-cell lymphoma with analysis of germinal center and post-germinal center biomarkers. J Clin Oncol. 2008;26:2717–24. doi: 10.1200/JCO.2007.13.1391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.García-Suárez J, Bañas H, Arribas I, De Miguel D, Pascual T, Burgaleta C. Dose-adjusted EPOCH plus rituximab is an effective regimen in patients with poor-prognostic untreated diffuse large B-cell lymphoma: results from a prospective observational study. Br J Haematol. 2007;136:276–85. doi: 10.1111/j.1365-2141.2006.06438.x. [DOI] [PubMed] [Google Scholar]
- 37.Wilson WH, Grossbard ML, Pittaluga S, Cole D, Pearson D, Drbohlav N, Steinberg SM, Little RF, Janik J, Gutierrez M, Raffeld M, Staudt L, Cheson BD, et al. Dose-adjusted EPOCH chemotherapy for untreated large B-cell lymphomas: a pharmacodynamic approach with high efficacy. Blood. 2002;99:2685–93. doi: 10.1182/blood.v99.8.2685. [DOI] [PubMed] [Google Scholar]
- 38.Chan JK. The new World Health Organization classification of lymphomas: the past, the present and the future. Hematol Oncol. 2001;19:129–50. doi: 10.1002/hon.660. [DOI] [PubMed] [Google Scholar]
- 39.Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, Müller-Hermelink HK, Campo E, Braziel RM, Jaffe ES, Pan Z, Farinha P, Smith LM, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103:275–82. doi: 10.1182/blood-2003-05-1545. [DOI] [PubMed] [Google Scholar]
- 40.Cheson BD, Pfistner B, Juweid ME, Gascoyne RD, Specht L, Horning SJ, Coiffier B, Fisher RI, Hagenbeek A, Zucca E, Rosen ST, Stroobants S, Lister TA, et al. Revised response criteria for malignant lymphoma. J Clin Oncol. 2007;25:579–86. doi: 10.1200/JCO.2006.09.2403. [DOI] [PubMed] [Google Scholar]
- 41.Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Connors JM, Lister TA, Vose J, Grillo-López A, Hagenbeek A, Cabanillas F, Klippensten D, Hiddemann W, et al. Report of an international workshop to standardize response criteria for non-Hodgkin's lymphomas. NCI Sponsored International Working Group. J Clin Oncol. 1999;17:1244. doi: 10.1200/JCO.1999.17.4.1244. [DOI] [PubMed] [Google Scholar]
- 42.Ajani JA, Welch SR, Raber MN, Fields WS, Krakoff IH. Comprehensive criteria for assessing therapy-induced toxicity. Cancer Invest. 1990;8:147–59. doi: 10.3109/07357909009017560. [DOI] [PubMed] [Google Scholar]