

Description
A 68-year-old woman was transplanted pre-emptively with a kidney from a deceased donor in May 2012. Her immunosuppressive treatment included thymoglobulin, and tacrolimus, mycophenolate mofetyl (MMF), methylprednisolone. Ten months later, a positive urinalysis for decoy cells (figure 1) preceded a rise in creatinine to 2 mg/dL. Blood PCR for BK DNA detected 45 915 copies/mL. Kidney biopsy disclosed BK virus nephropathy (BKVN; figure 2). MMF was withdrawn and tacrolimus decreased to 4 ng/mL trough level. Three months later, the virus was undetectable. Creatinine remained stable over the following years (2 mg/dL). Donor-specific anti-HLA antibodies remained negative.
Figure 1.
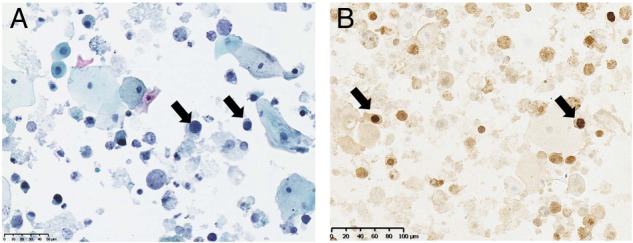
Urine cytology shows decoy cells corresponding to tubular epithelial cells infected with BK virus and shed in the urine. (A) Some epithelial cells have enlarged nuclei with ground glass appearance (arrows). (B) Immunohistochemistry staining using antibody against simian virus 40 large T antigen revealing infected cells.
Figure 2.
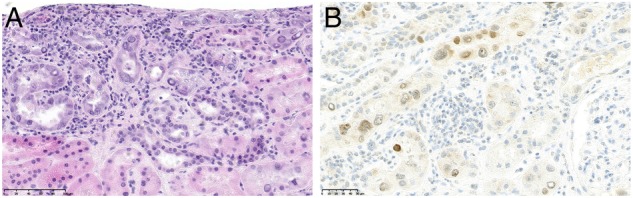
Kidney graft biopsy showing BKVN. (A) H&E stain shows interstitial inflammation located around infected tubules. Infected tubular cells have enlarged nuclei with intranuclear viral inclusion. (B) Immunohistochemical staining for SV40-T antigen showing positively stained nuclei in tubular epithelial cells. BKVN, BK virus nephropathy.
BKVN has emerged as a cause of graft loss. BK virus is a polyomavirus prevalent in 60–80% of the general population. It colonises mainly the renourinary tract where it remains latent. The intensity of immunosuppression is the main risk factor for BKVN. BK virus appears first in the urine, then in the blood, and ultimately progresses to the graft.1 Antiviral therapies are lacking. Thus, screening is essential, and recommended during the first post-transplant year. A kidney graft biopsy should be performed when plasma BKV DNA loads is >4 log 10 copies/mL.2 Since BKVN can be focal in distribution, negative results cannot rule out the diagnosis. The primary treatment is reducing the intensity of immunosuppression, by discontinuing the antimetabolite and reducing calcineurin inhibitor trough level.3 Graft failure occurs in 30–60% of patients, but outcomes have improved since screening has permitted prompt decrease of immunosuppression. Retransplantation is possible in virologically quiescent patients, but requires close monitoring of BK viremia.2
Learning points.
Polyomavirus nephropathy is a cause of kidney graft dysfunction and graft failure.
The intensity of immunosuppression is the main risk factor.
Reduction of immunosuppression is the primary treatment.
Screening allows early diagnosis and better outcomes.
Footnotes
Contributors: BS and NK took care of the patient and wrote the manuscript. MDM performed the biopsy. SA interpreted and provided the images.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Randhawa P, Brennan DC. BK virus infection in transplant recipients: an overview and update. Am J Transplant 2006;6:2000–5. 10.1111/j.1600-6143.2006.01403.x [DOI] [PubMed] [Google Scholar]
- 2.Hirsch HH, Vincenti F, Friman S et al. Polyomavirus BK replication in de novo kidney transplant patients receiving tacrolimus or cyclosporine: a prospective, randomized, multicenter study. Am J Transplant 2013;13:136–45. 10.1111/j.1600-6143.2012.04320.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dall A, Hariharan S. BK virus nephritis after renal transplantation. Clin J Am Soc Nephrol 2008;3(Suppl 2):S68–75. 10.2215/CJN.02770707 [DOI] [PMC free article] [PubMed] [Google Scholar]