

Abstract
A 19-year-old woman underwent ASD closure with patch in the childhood. Fifteen years later, she presented with severe cyanosis and dyspnea on exertion. Clinical diagnostics revealed a dislocation of the patch resulting in a right-to-left shunt (RLS) that was compensated in the past years by a recurrent ASD allowing a left-to-right shunt (LRS). The existing balance between interatrial shunts vanished by the growth of the patient leading to the clinical deterioration. After successful redo surgery, the patient was discharged home 8 days postoperatively.
Keywords: congenital heart disease, reoperation, imaging
Case Report
The 19-year-old female patient underwent surgical closure of atrial septal defect (ASD). Repair included implantation of an autologous pericardial patch. Yearly follow-ups showed no abnormality.
After 15 years, she complained of weakness and shortness of breath on exertion. Physical examination showed pale discoloration of the skin and acrocyanotic fingers with clubbing.
The transthoracic echocardiography demonstrated turbulent flow of unknown origin at the left atrial roof (Fig. 1).
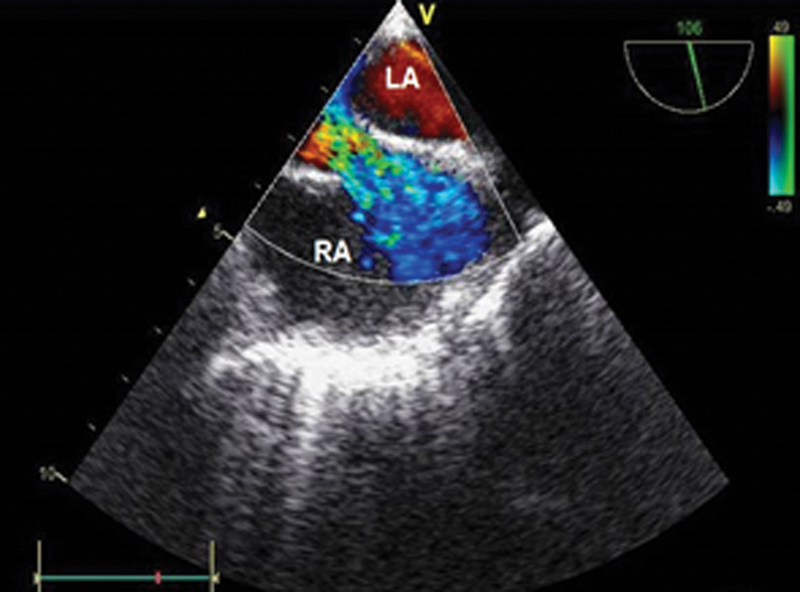
Fig. 1.
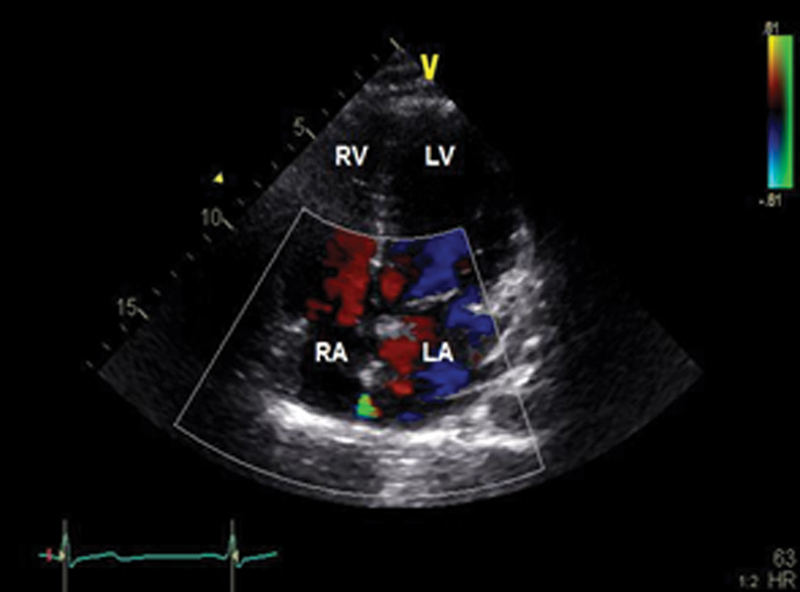
Color-coded transthoracic echocardiography showing a turbulent inflow of unknown origin in the interatrial septum.
Computed tomography pulmonary angiography (Fig. 2) showed a prominent right inferior pulmonary vein (RIPV) with a diameter of 16 mm draining into the left atrium (LA) in a very close anatomical relation to the atrial septum. Furthermore, the inferior vena cava (IVC) drained into the left atrium instead of the right atrium.
Fig. 2.
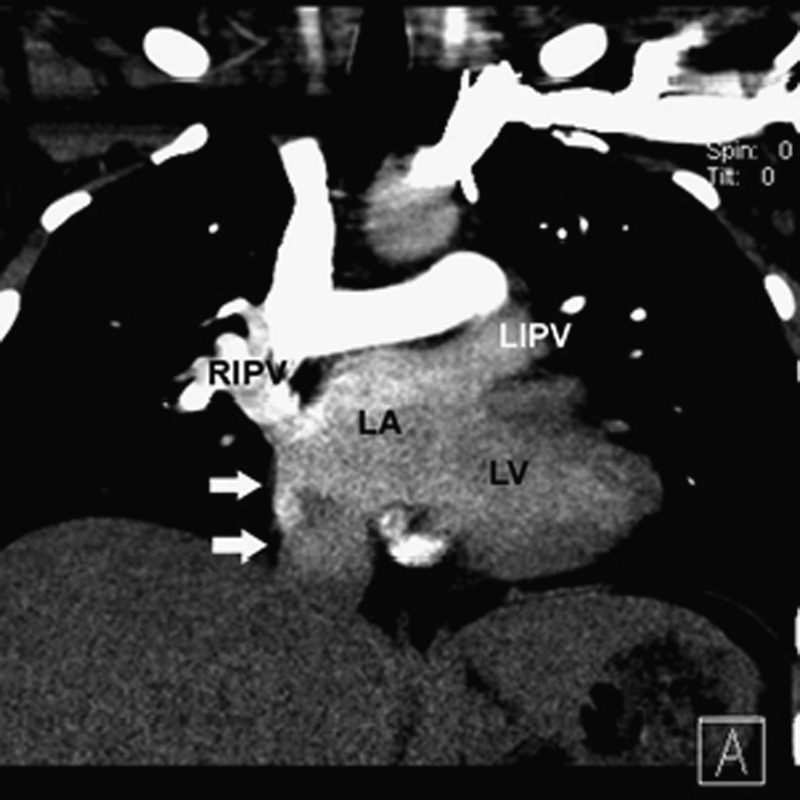
Computed tomography pulmonary angiography in paracoronal view. The direct junction of the IVC and the LA (white arrows). Noncontrast-enhanced blood from the IVC is mixing with slightly enhanced blood from the pulmonary veins.
Cardiac magnetic resonance imaging (Fig. 3) showed a central discontinuity of approximately 10 × 11 mm in the atrial septum. A double contour formation bulging toward the RA was found in this area. A discrete strain of dye from the right to the left atrium could be seen. However, phase-contrast flow measurements revealed a shunt volume of approximately 10 mL from the right to the left atrium.
Fig. 3.
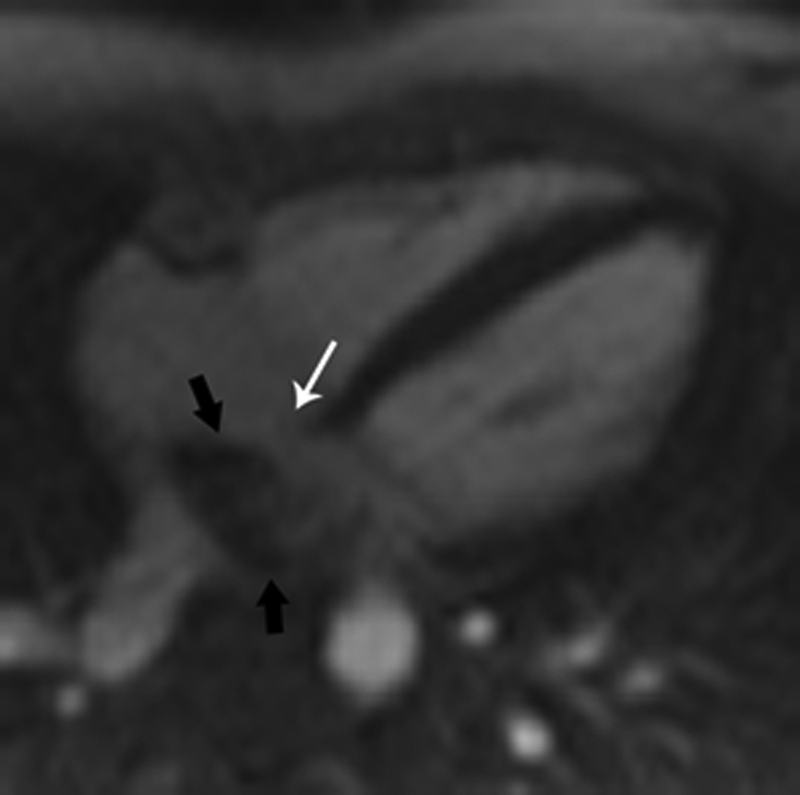
Cardiac magnetic resonance imaging rest perfusion of the heart in axial view. A small defect in the atrial septum can be delineated (white arrow). However, the small shunt volume, which was measured on phase-contrast series, was visually not detectable in the perfusion series. Also note the large area with low-signal intensity in the central portion of the LA (black arrows) representing noncontrast-enhanced inflowing venous blood from the IVC. On the other side, pulmonary veins, left ventricle, and aorta show high-signal intensity due to contrast-enhanced arterial blood.
Diagnostic tests showed that the original patch of the ASD closure caused a deviation of the IVC into the LA (Fig. 4), leading to a symptomatic RLS. Indication for reoperation was seen.
Fig. 4.
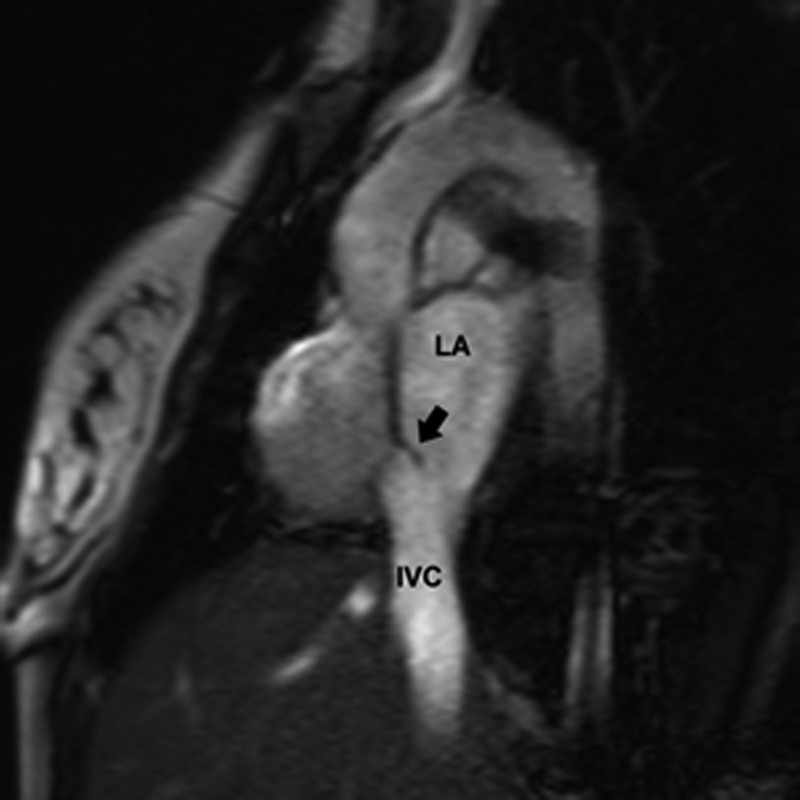
Cardiac magnetic resonance imaging cine in short-axis view cutting through the LA. Note the small flap arising from the region of the atrial septum and pointing toward the LA/IVC (black arrow). The direct junction of the IVC and the LA can be visualized.
After induction of general anesthesia, a transesophageal echocardiography confirmed the large RLS (Fig. 5). After performing median resternotomy and establishing the cardiopulmonary bypass, right atriotomy was performed. The atrial septum appeared intact with a small defect just above the RIPV orifice. The patch occluded the connection between IVC and the RA and deviated IVC as well as blood from the RIPV into the LA (Fig. 6). The old patch was partially dissected off the old suture line and resewn into correct position, augmented by a small new patch. The coronary sinus was clearly identified and routed into the RA. The ostium of the RIPV was very close to the proximal IVC, so the membrane between the RIPV and the IVC was incised to move the ostium more into the center of the LA. A small additional new patch was sutured to this incision, following the LA wall below the coronary sinus and the cut edge of the old patch on the right side, closing the small recurrent ASD. The IVC orifice was augmented with a small additional patch (Fig. 7). The weaning from extracorporeal circulation was uneventful. No shunt was noted in the postoperative transesophageal echocardiography (Fig. 8).
Fig. 5.
Preoperative color-coded transesophageal echocardiography showing the RLS.
Fig. 6.
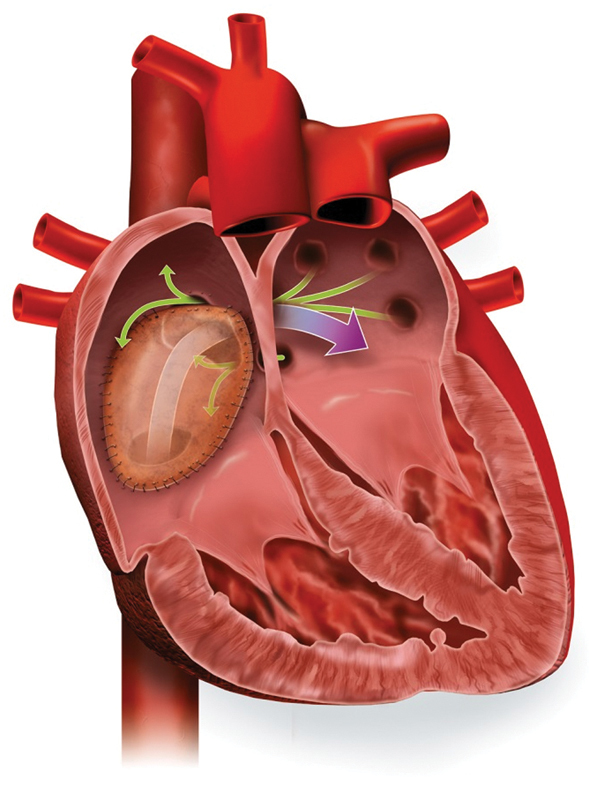
Preoperative illustration demonstrates the incorrect patch placement with a deviation of IVC flow into the LA corresponding to the flow of the RIPV and the recurrent ASD.
Fig. 7.
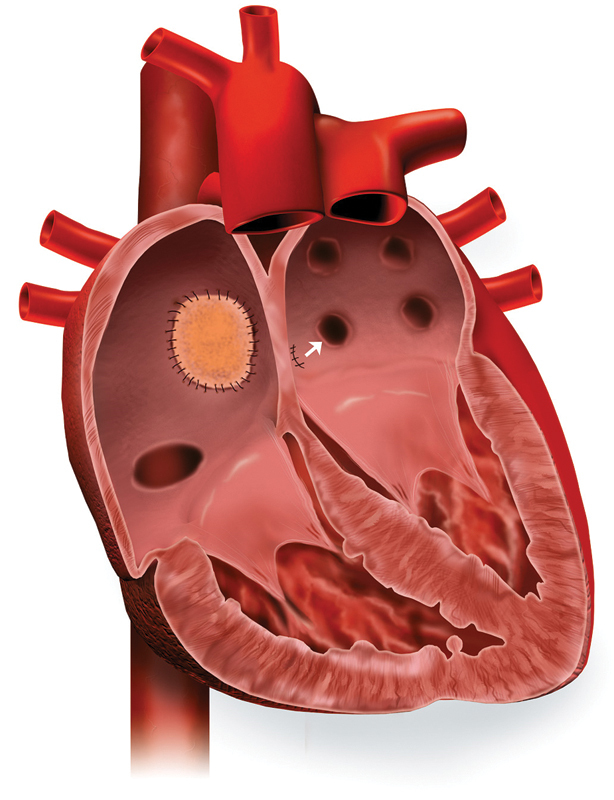
Postoperative illustration shows the closed ASD with a patch and the diversion of the RIPV into the center of the LA.
Fig. 8.
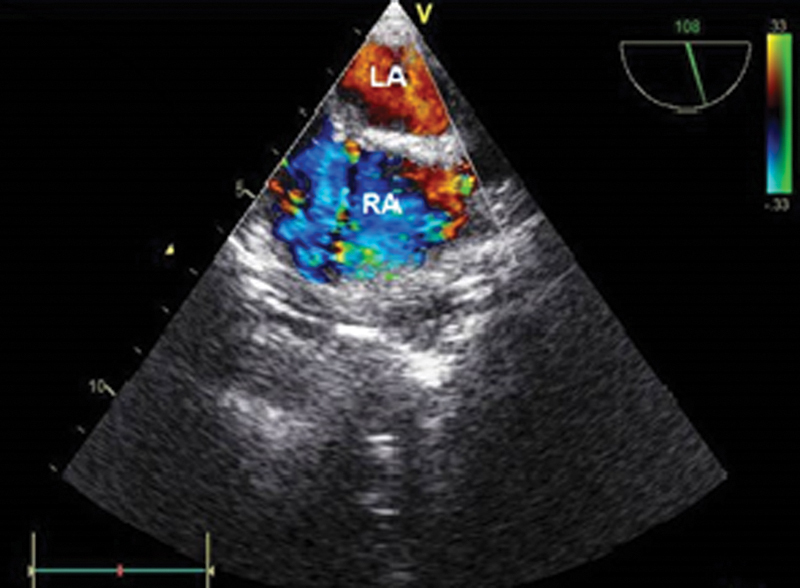
Postoperative color-coded transesophageal echocardiography on atrial level: no detectable shunt in the interatrial septum after surgical correction.
After an uneventful postoperative course, the patient was discharged home 8 days postoperatively.
Comment
Late complications following surgical closure of atrial ASD are very rare.1 Sellers et al. reported in a series of 275 patients with a history of operative treatment of ASD a recurrent shunt rate of 7%.2 Diversion of the IVC into the LA and residual RLS is a rare postoperative complication following surgical ASD closure.3 Because of the lack of clinical manifestations, reoperation rates for correction of residual LRS or recurrent ASD were very low, with a reported incidence of less than 2%.2
In our case, the very late development of clinical symptoms after 15 years of healthiness was a remarkable fact. Clinical examination and diagnostics confirmed only the presence of a minimal interatrial shunt that was not correlated with sudden progress of the symptoms. After a reevaluation of the diagnostic findings, we realized the incorrect patch placement with a deviation of IVC flow into the LA corresponding to the flow of the RIPV (Figs 4 and 6).
Over the past years, the patient was hemodynamically compensated by a recurrent ASD allowing LRS and ensuring a balance in the systemic circulation. This flow phenomenon exists physiologically in the fossa ovalis4 but is uncommon as a postoperative complication after surgical repair of ASD and has not been described in the literature yet.
We hypothesize that a rapid clinical deterioration after 15 years was caused by the growth of the patient: the remaining ASD possibly became restrictive, the existing balance between interatrial shunts vanished, cyanosis increased, and the patient became severely symptomatic.
The patient underwent a redo surgery. IVC was diverted into the RA, and the RIPV into the LA. The ASD was closed (Fig. 7). She was discharged home 8 days postoperatively. She remains symptom free 3 years later.
Acknowledgment
The authors would like to thank Mrs Charlotte Schmitz for the illustrations.
References
- 1.Meijboom F, Hess J, Szatmari A. et al. Long-term follow-up (9 to 20 years) after surgical closure of atrial septal defect at a young age. Am J Cardiol. 1993;72(18):1431–1434. doi: 10.1016/0002-9149(93)90192-f. [DOI] [PubMed] [Google Scholar]
- 2.Sellers R D, Ferlic R M, Sterns L P, Lillehei C W. Secundum type atrial septal defects: early and late results of surgical repair using extracorporeal circulation in 275 patients. Surgery. 1966;59(1):155–164. [PubMed] [Google Scholar]
- 3.Desnick S J, Neal W A, Nicoloff D M, Moller J H. Residual right-to-left shunt following repair of atrial septal defect. Ann Thorac Surg. 1976;21(4):291–295. doi: 10.1016/s0003-4975(10)64313-5. [DOI] [PubMed] [Google Scholar]
- 4.Lind J, Wegelius C. Atrial septal defects in children: an angiocardiographic study. Circulation. 1953;7(6):819–829. doi: 10.1161/01.cir.7.6.819. [DOI] [PubMed] [Google Scholar]