

Abstract
Background
Rice is known to be high in arsenic, including in infant rice cereal. Although arsenic in drinking water is currently regulated, there are currently no US regulations regarding arsenic concentrations in food.
Objective
We used published values to estimate arsenic exposure via rice cereal relative to breast milk or formula for 6- to 12-month-old infants in the general US population.
Results
We found that arsenic exposure from 3 servings of rice cereal exceeded that of formula made with water containing arsenic at 10 mg/L, the US Environmental Protection Agency maximum contaminant level.
Conclusions
Our findings suggest that rice cereal can markedly increase arsenic exposure among US infants relative to breast milk and formula.
Keywords: arsenic, environmental exposure, infant formula, rice cereal
Introduction
Arsenic is a known carcinogen and suspected immunotoxicant.1 We previously reported that infant formula can be an important source of arsenic exposure, especially when reconstituted with arsenic-contaminated water.2 However, solid foods are also a potential source of arsenic, especially those containing rice.3-5 Infant rice cereal, often the first solid food an infant recieves, has been reported to contain elevated concentrations of arsenic.6-8 This is potentially of concern because early life is a period of both heighted vulnerability to arsenic9 and high dietary intake relative to adults.10
Although arsenic in drinking water is currently regulated at concentrations >10 μg/L, the maximum contaminant level (MCL) set by the US Environmental Protection Agency (EPA),11 there are currently no US regulations regarding arsenic concentrations in food.12 We therefore developed exposure models using published data to compare infant arsenic exposure from rice cereal versus formula prepared with water at and below the MCL.
Methods
Rice Cereal
We estimated the per-serving exposure to arsenic by multiplying the mean serving size13 by the concentration of total or inorganic arsenic in rice cereal reported by the US Food and Drug Administration8 and then dividing by the body weight recommended by the US EPA.3 We estimated exposure using both central tendency and upper bound inputs. For central tendency inputs, we used the median concentration of arsenic in rice cereal (total arsenic: 0.20 μg/g; inorganic arsenic: 0.12 μg/g)8 and mean body weight (3-6 months: 7.4 kg; 6-12 months: 9.2 kg).10 Upper bound inputs included the maximum concentration of arsenic in rice cereal (total arsenic: 0.37 μg/g; inorganic arsenic 0.25 μg/g)8 and fifth percentile body weight (3-6 months: 5.7 kg; 6-12 months: 7.1 kg).10 Both models used the mean serving size (3-6 months: 11.6 g; 6-12 months: 17 g or ∼4 tablespoons) because no upper bound was available.13 The water used to reconstitute the cereal was assumed to be free of arsenic.
Although water contains primarily inorganic forms of arsenic (AsIII and AsV), rice typically contains organic forms, including dimethylarsinic acid (DMA), a metabolite of inorganic arsenic.8 The toxicity of the organic forms is less understood; however, the trivalent forms of DMA appear to be toxic.11 Therefore, we calculated exposures for both total and inorganic arsenic and relied on total arsenic for our comparisons.
Infant Formula
We estimated central tendency and upper bound arsenic exposure (μg/kg/d) for infants fed exclusively with formula prepared using tap water containing arsenic at 3 target concentrations: 1, 5, and 10 μg/L. The total concentration of arsenic in formula included the target concentration of arsenic in tap water plus the concentration of arsenic in formula powder. The total concentration of arsenic in formula was then multiplied by the age-specific body weight–adjusted ingestion rate.10 For central tendency inputs we used the target concentration of arsenic in tap water (1, 5, or 10 μg/L), the median concentration of arsenic in formula powder (1.1 μg/L),4 and the mean body weight adjusted ingestion rate (L/kg/d; birth–1 month: 0.15; 1-3 months: 0.14; 3-6 months: 0.11; 6-12 months: 0.08).10 Upper bound inputs used the target concentration of arsenic in tap water (1, 5, or 10 μg/L), the maximum concentration of arsenic in formula powder (1.8 μg/L),4 and the upper percentile body weight–adjusted ingestion rate, defined by the US EPA as the mean plus 2 standard deviations (L/kg/d; birth–1 month: 0.22; 1-3 months: 0.19; 3-6 months: 0.15; 6-12 months: 7.1).10
Results
Estimated exposure as a result of rice cereal was elevated (Table 1, Fig. 1). Two servings of rice cereal per day resulted in higher total arsenic exposure for 6- to 12-month-old infants than formula made with water containing 5 μg/L. The estimated 1.11 μg/kg/d from 3 servings of rice cereal per day exceeded exposure from formula mixed with water at the MCL and was 6.5 times higher than exposure for a 60-kg adult ingesting 1 L/d of water at the MCL (0.17 μg/kg/d).6
Table 1. Central Tendency (Upper Bound) Estimated Daily Exposure (μg/kg/d) for Infants During the First Year of Life as A Result of Formula Mixed with Tap Water Containing Arsenic at 1, 5, or 10 μg/l Versus 1-4 Servings of Infant Rice Cereal.
| Infant Age (mo) | ||||
|---|---|---|---|---|
|
| ||||
| Birth to <1 | 1 to <3 | 3 to <6 | 6 to <12 | |
| Infant formula, tap water arsenic | ||||
| 1 μg/L | 0.32 (0.62) | 0.29 (0.53) | 0.23 (0.42) | 0.17 (0.36) |
| 5 μg/L | 0.92 (1.5) | 0.85 (1.29) | 0.67 (1.02) | 0.51 (0.88) |
| 10 μg/L | 1.67 (2.6) | 1.55 (2.24) | 1.22 (1.77) | 0.92 (1.53) |
| Servings of infant rice cereal | ||||
| 1 serving/d | NE | NE | 0.32 (0.76) | 0.37 (0.89) |
| 2 servings/d | NE | NE | 0.63 (1.52) | 0.74 (1.77) |
| 3 servings/d | NE | NE | 0.95 (2.28) | 1.11 (2.66) |
| 4 servings/d | NE | NE | 1.27 (3.04) | 1.48 (3.55) |
NE, not estimated because rice cereal is not recommended at this age.
Figure 1.
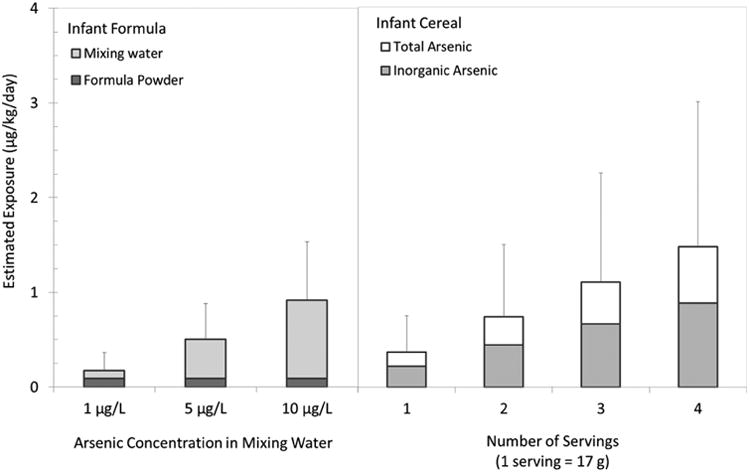
Estimated daily exposure to arsenic via formula (left) or rice cereal (right) for 6- to 12-month-old infants. Columns represent central tendency estimates and error bars represent upper bound estimates.
Discussion
Our results indicate that infant rice cereal can be an important source of arsenic exposure for US infants during weaning, consistent with reports from Europe.6,7 Infants consuming both formula mixed with arsenic-containing water and rice cereal can have especially high exposures. Although we used the MCL as a point of comparison, it is based on chronic, adult-onset disease11 and was not explicitly designed to protect infants.9 According to the American Academy of Pediatrics, rice cereal provides no advantage over other grains as a first solid food,14 and both the the American Academy of Pediatrics and US
Food and Drug Administration suggest that infants would benefit from an array of grain cere-als.14,15 Future research should investigate how effective a no- or low-rice cereal intervention could be at reducing infant exposure to arsenic.
Acknowledgments
This publication was supported in part by grants P01 ES022832 and P20 ES018175 from the National Institute of Environmental Health Sciences (NIEHS) and RD83459901 and RD83544201 from the Environmental Protection Agency (EPA). Contents are solely the responsibility of the grantee and do not necessarily represent the official views of the US EPA. Further, the US EPA does not endorse the purchase of any commercial products or services mentioned in the publication.
Footnotes
The authors have no financial relationships relevant to this article to disclose. The authors have no conflicts of interest to disclose.
All authors had access to the data and a role in writing the manuscript.
References
- 1.Naujokas MF, Anderson B, Ahsan H, et al. The broad scope of health effects from chronic arsenic exposure: update on a worldwide public health problem. Environ Health Perspect. 2013;121:8. doi: 10.1289/ehp.1205875. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Carignan CC, Cottingham KL, Jackson BP, et al. Estimated exposure to arsenic in breastfed and formula-fed infants in a United States cohort. Environ Health Perspect. 2015;123:600–6. doi: 10.1289/ehp.1408789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Abedin MJ, Cresser MS, Meharg AA, Feldmann J, Cotter-Howells J. Arsenic accumulation and metabolism in rice (Oryza sativa L) Environ Sci Technol. 2002;36:962–8. doi: 10.1021/es0101678. [DOI] [PubMed] [Google Scholar]
- 4.Jackson BP, Taylor VF, Punshon T, Cottingham KL. Arsenic concentration and speciation in infant formulas and first foods. Pure Appl Chem. 2012;84:215–23. doi: 10.1351/PAC-CON-11-09-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Meharg A. Arsenic in rice— understanding a new disaster for South-East Asia. Trends Plant Sci. 2004;9:415–7. doi: 10.1016/j.tplants.2004.07.002. [DOI] [PubMed] [Google Scholar]
- 6.Meharg A, Sun G, Williams PN, et al. Inorganic arsenic levels in baby rice are of concern. Environ Pollut. 2008;152:746–9. doi: 10.1016/j.envpol.2008.01.043. [DOI] [PubMed] [Google Scholar]
- 7.Hernandez-Martinez R, Navarro-Blasco I. Survey of total mercury and arsenic content in infant cereals marketed in Spain and estimated dietary intake. Food Control. 2013;30:423–32. [Google Scholar]
- 8.US Food and Drug Administration. Analytical results from inorganic arsenic in rice and rice products sampling. Washington, DC: U.S. Food and Drug Administration; 2013. [Accessed April 9, 2015]. Available at: http://www.fda.gov/downloads/Food/FoodborneIllnessContaminants/Metals/UCM352467.pdf. [Google Scholar]
- 9.Farzan SF, Karagas MR, Chen Y. In utero and early life arsenic exposure in relation to long-term health and disease. Toxicol Appl Pharmacol. 2013;272:384–90. doi: 10.1016/j.taap.2013.06.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.US Environmental Protection Agency. Child-Specific Exposure Factors Handbook (Final Report) 2008. Washington, DC: EPA; 2008. EPA/600/R-06/096F. [Google Scholar]
- 11.Abernathy CO, Thomas DJ, Calderon RL. Health effects and risk assessment of arsenic. J Nutr. 2003;133:1536S–8S. doi: 10.1093/jn/133.5.1536S. [DOI] [PubMed] [Google Scholar]
- 12.Schmidt CW. In search of “just right”: the challenge of regulating arsenic in rice. Environ Health Perspect. 2015;123:A16–9. doi: 10.1289/ehp.123-A16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fox MK, Reidy K, Karwe V, Ziegler P. Average portions of foods commonly eaten by infants and toddlers in the United States. J Am Diet Assoc. 2006;106:66–76. doi: 10.1016/j.jada.2005.09.042. [DOI] [PubMed] [Google Scholar]
- 14.American Academy of Pediatrics. AAP offers advice for parents concerned about arsenic in food. Elk Grove, IL: American Academy of Pediatrics; 2013. [Accessed April 9, 2015]. Available at: https://www.aap.org/en-us/about-the-aap/aap-press-room/pages/AAP-Offers-Advice-For-Parents-Concerned-About-Arsenic-in-Food.aspx. [Google Scholar]
- 15.US Food and Drug Administration. Questions & answers: arsenic in rice and rice products. Washington, DC: FDA; 2013. [Accessed April 9, 2015]. http://www.fda.gov/Food/FoodborneIllnessContaminants/Metals/ucm367263.htm. [Google Scholar]