

Abstract
Aims and Objectives:
The objective of the present investigation is to evaluate patients’ pain perception and discomfort, the duration of pain and the level of self-medication over time during tooth separation, and the effectiveness of elastomeric and spring types of orthodontic separators in Saudi population.
Materials and Methods:
The study group consisted of 30 female adolescent patients who had elastomeric/spring separators as part of their orthodontic treatment. A self-administrated questionnaire comprising 16 multiple choice questions and another with visual analog scale were used to record the patient's pain perceptions at 4 hours, 24 hours, 3 days, 5 days, and 7 days from the time of insertion. The level of pain and discomfort during these time periods were assessed by a visual analog scale. After a separation period of 7 days, the amount of separation was measured with a leaf gauge. Type and frequency of analgesic consumption was also recorded. The Statistical Package for the Social Sciences (SPSS) version 20 (IBM SPSS -Chicago, IL: SPSS Inc.,) was used for statistical analysis.
Results:
The data showed significant increase in the level of pain at 4 hours, 24 hours, and 3 days from separator placement. The elastomeric separators produced significantly more separation than the spring separators and also caused maximum pain during the first 3 days after insertion. However, there was no significant difference between the score of pain between two separators at all time intervals.
Conclusion:
Both elastomeric and spring separators showed comparative levels of pain and discomfort during the early phase of separation. Elastomeric separators were found to be more effective in tooth separation than spring separators. However, further studies are necessary to substantiate this preliminary observation.
Keywords: Analgesics, orthodontic separators, pain perception, periodontal ligament cells
INTRODUCTION
Patients undergoing orthodontic treatment experience varying degrees of pain during different stages of treatment. Placement of separators induces pain which increases to a peak level after 24 hours.[1] Separators are used to create space for placement of band that later anchors the fixed orthodontic appliance.[2] The different types of separators vary in the amount of pain they cause during separation, the effectiveness in separating teeth, and maintenance of the separation gained.[3] The two types that are most commonly used are the elastomeric and spring-type stainless steel separators.[4]
Studies have shown that the pain perception accompanied with orthodontic procedures includes a combination of pressure, tension, soreness, and pain.[5,6] The pain experienced is due to the constant pressure, ischemia, inflammation, and edema in the periodontal ligaments of the teeth that are moved during orthodontic movements. Therefore, pain has been the prime reason for discontinuation of orthodontic treatment.[7,8] Pain is usually initiated 4 hours after the application of the separator and increases over 24 hours, which then decreases within a 7-day period.[9,10,11] Literature revealed that pain is usually aggravated by functions such as eating, eventually leading the patients to modify their eating habits as a coping mechanism and/or force them to use analgesics as a preventive measure when pain arises.[12,13]
Few studies in the past have compared pain perception based on gender, age, and cultural background. Females often complained of more severe pain than males.[14,15] In contrast, other studies reported no difference in pain perception among both the genders.[16,17,18] A study by Brown and Moerenhout[19] showed that adults are more likely to suffer from pain when compared to pre-adolescents and adolescents. Cultural background and customs may influence the perception and expression of pain.[12] Only limited data is available on the pain perception and tolerance subsequent to the application of elastomeric and spring separators in Saudi patients undergoing orthodontic treatment.[10] Hence, the present study is undertaken to compare the pain perception associated with the two most common types of separators (elastomeric and the spring type separators) used in adolescent patients.
MATERIALS AND METHODS
Thirty female adolescent patients were included in this study. The sample size was calculated using the G Power software (www.psycho.uniduesseldorf.de/aap/projects/gpower/). The significance level, power, and magnitude of the expected difference were taken into consideration to derive the sample size. Baseline values were obtained from similar studies[11,20] conducted in the past to test similar hypothesis. The suggested inclusive criteria indicated that all participants should fulfill the following: initiating treatment for the first time with fixed orthodontic appliance at College of Dentistry/King Saud University, contact with adjacent teeth (second premolars and second molars) and age range of 14 to 21 years. The study was conducted from October 2015 to April 2016. All patients were informed that their participation in the study will be voluntary and confidential; all participants or their guardians were given a consent form that documented their agreement in participation after receiving written explanatory information regarding the study procedure and the questionnaire that they should fill. Ethical approval for this study was granted by the College of Dentistry Research Center at King Saud University (CDRC-IR0045). Two different types of separators were tested. A spring-type and an elastomeric-type separator were placed on the mesial and distal aspects of the upper and lower first molars [Figure 1]. Equal number of separators were placed on the left or the right quadrant to avoid right/left bias.
Figure 1.

The elastomeric and spring separators in the patient's mouth
Investigation of patient pain perception
Following the placement of the separators, the patients were given the questionnaire. The patients were asked to answer each questionnaire after a proposed timing, i.e., 4 hours, 24 hours, 3 days, 5 days, and 7 days from the insertion time. The questionnaire was adopted and modified from earlier studies.[9,11,21] A visual analog scale (VAS) was included in the questionnaire [Figure 2]. The VAS was used to measure the severity of the pain. The patients were given two 1 cm long scales scoring 1–10 from no pain to severe pain; each scale representing one side, i.e., right/left. Majority of the patients had an understanding of VAS and could immediately formulate the measurement. VAS has shown increased sensitivity over verbal descriptive scales with respect to measuring the successive response to treatment.[22]
Figure 2.
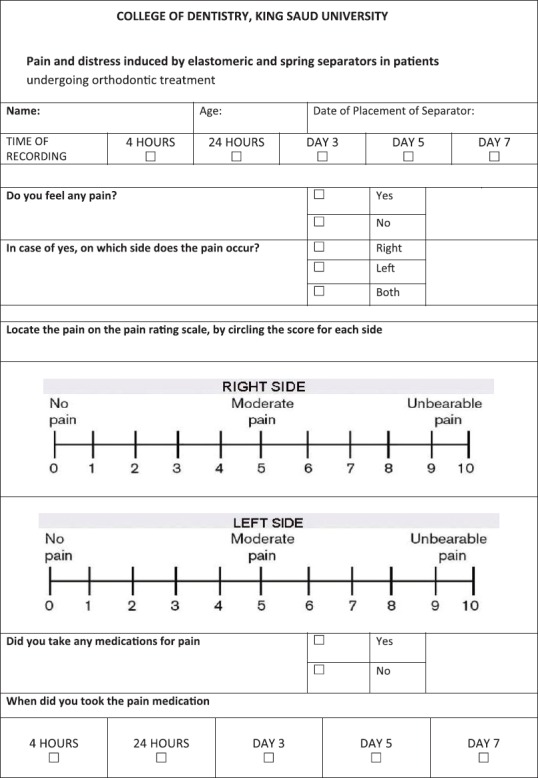
The questionnaire used in the study
Measuring the separation effect
After the 7th day of separator insertion, the remaining separators (in case some were lost) were removed and the area was rinsed and dried for evaluation. The amount of separation was measured with a leaf gauge mesially and distally to the first upper and lower molars by 1 examiner. For intraexaminer reliability, the examiner replaced the separators for 5 randomly selected patients after 2 months from the first placement to ensure space closure from the previous separator placement.
Statistical procedures
In this study, patients’ pain perception output variables and the separating effect of the two separators applied were measured. The Statistical Package for the Social Sciences version 20 (IBM SPSS -Chicago, IL: SPSS Inc.,) was used. The results were presented with descriptive statistical tables, mean, standard deviation, and percentages to describe the study data. t-test was also conducted to compare the amount of space generated by two separators, as well as the correlation between space sizes created by both separators on either side.
RESULTS
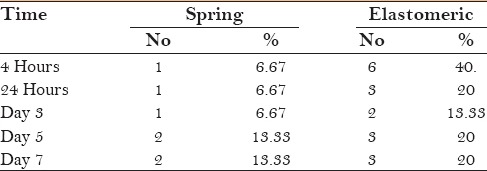
The study investigated the tooth separation and pain perception associated with two types of tooth separators during orthodontic treatment. The observations showed that the elastomeric separators produced significantly more space compared to the spring separators [Table 1]. The pain perception measured using a VAS showed that elstomeric separators have relatively higher pain perception during all time points. However, it was not statistically significant from the elastomeric separators [Table 2; Figure 3]. The peak for pain intensity was recorded on day 1 in both separator groups and started to decline after day 3. Descriptive data on the analgesics used by both group of patients is presented in Table 3. There is not much variation in the use of analgesics between the participants in the elastomeric and spring separators. A higher percentage of analgesic usage was observed during the first 4 hours to 24 hours.
Table 1.
The space achieved by the application of the separators
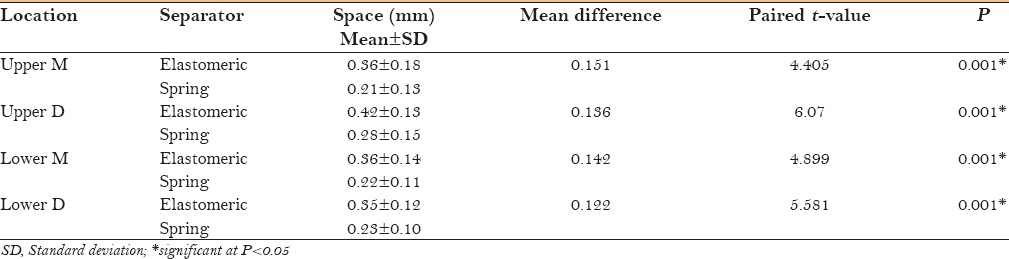
Table 2.
Pain perceived (VAS scale) by the separators at different intervals
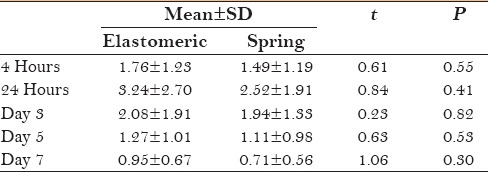
Figure 3.
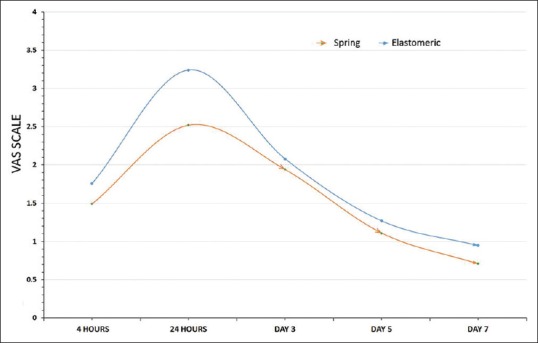
The pain experienced with the elastomeric and spring separators over time
Table 3.
The percentage of participants who used painkillers during the first 7 days of tooth separation
DISCUSSION
Pain and discomfort experienced by patients during orthodontic tooth separation can vary widely, and are the major patient concerns that discourage some patients from seeking treatment and others from discontinuing with their treatment.[11] Adolescents are the prevalent age group pursuing orthodontic treatment because occlusal condition is considerably allied to the tolerability of their general physical mien. However, pain and discomfort is concerning for many potential adolescent patients undergoing orthodontic treatment.[23] Several studies have revealed that the patients’ reaction to the early movement of the teeth differs, and it is difficult for the orthodontist to react precisely to forthcoming patients’ query concerning the degree and duration of distress that might be encountered. Response to these sensations differs between subjects and can rely on previous experiences, cultural background, and other modes of psychologic input that provide gist to a condition in which pain ensued. Pain is generally a consequence of pressure, ischemia, inflammation, and edema developing in periodontal ligament ascribable to the applied orthodontic forces.[24] Pain may be associated with the interactions of inflammatory mediators, and control of these inflammatory mediators may be important to relieve the pain that accompanies tooth movement.[25]
There are various types of separators used in orthodontics, namely, latex elastics, brass wires, spring-type steel, and elastomeric separators. The present study was performed on 30 adolescent female patients who were asked to complete a questionnaire concerning pain after the insertion of elastomeric separators and spring separators in the right and left molar areas. The evaluation of pain initiated from the fourth hour after placement of both the separators was persistent until the seventh day. It was noted that a majority of the patients delineated continuous pain after 4 hours from separators placement, which continued to the third day. Then, intermittent pain was noticed to be associated with a reduced number of participants revealing pain in the subsequent days to arrive the least on the seventh day. This is in agreement with the findings of Ngan et al.[26] who reported that pain was worst during the 24-hour period and completely subsided on the seventh day. The perceived pain was more intense during the second day and virtually declined thereafter.[20]
Bondemark et al.,[9] in their study, compared pain perception to elastomeric and spring type of separators; they did not find any differences in pain effect of both types of separators. In the present study, although not statistically significant, the data showed higher pain scores for elastomeric separators than spring separators; however, the intensity and score of pain are not significantly different between both the separators. Although Scheurer et al.[27] found a correlation between pain experience and analgesics consumption, we found no correlation between pain experience and analgesic consumption, which is in agreement with an earlier report.[28] We also found that spaces obtained with elastomeric separators were significantly greater than spring separators at all locations.
The findings from the current study and the supported literature indicates that the pain and discomfort encountered by the participants following separator placement may be associated with noxious agents such as substance P and the level of prostaglandins in the periodontal ligament. This study highlights the subtlety of the VAS. This is in concordance with the study conducted by Ngan et al.,[18] which signified the susceptibility of VAS to minor treatments, and substantiates the benefit of VAS over verbal rating scales in instituting the importance of some type of treatment.
In general, the observations of the study conclude that elastomeric separators are superior in tooth separation. The pain and discomfort levels did not show any significant differences between the two separators. However, elastomeric separators seem to be better tolerated. The limitation of the study is that it was conducted only among females and the limited number of participants included in this cross-sectional study.
CONCLUSION
Pain is one of the cardinal signs of inflammation, as well as nearly inevitable and for the patient, it is an unpleasant reaction to orthodontic therapy. Within the limitations of the study, we can conclude that pain and discomfort is experienced with both type of tooth separators. However, elastomeric separators were found to be superior in tooth separation than spring separators.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Bergius M, Berggren U, Kiliaridis S. Experience of pain during an orthodontic procedure. Eur J Oral Sci. 2002;110:92–8. doi: 10.1034/j.1600-0722.2002.11193.x. [DOI] [PubMed] [Google Scholar]
- 2.Steen Law SL, Southard KA, Law AS, Logan HL, Jakobsen JR. An evaluation of preoperative ibuprofen for treatment of pain associated with orthodontic separator placement. Am J Orthod Dentofacial Orthop. 2000;118:629–35. doi: 10.1067/mod.2000.110638. [DOI] [PubMed] [Google Scholar]
- 3.Malagan MA, P PB, Muddaiah S, Reddy R, Shetty BK, Preetham J, et al. Comparison between efficacy of four different types of orthodontic separators. J Clin Diagn Res. 2014;8:ZC41–4. doi: 10.7860/JCDR/2014/9963.4755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Beck VJ, Farella M, Chandler NP, Kieser JA, Thomson WM. Factors associated with pain induced by orthodontic separators. J Oral Rehabil. 2014;41:282–8. doi: 10.1111/joor.12144. [DOI] [PubMed] [Google Scholar]
- 5.Farronato G, Giannini L, Galbiati G, Cannalire P, Martinelli G, Tubertini I, et al. Oral tissues and orthodontic treatment: Common side effects. Minerva Stomatol. 2013;62:431–46. [PubMed] [Google Scholar]
- 6.Shi Q, Yang S, Jia F, Xu J. Does low level laser therapy relieve the pain caused by the placement of the orthodontic separators?--A meta-analysis. Head Face Med. 2015;11:28. doi: 10.1186/s13005-015-0085-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bukhari OM, Sohrabi K, Tavares M. Factors affecting patients’ adherence to orthodontic appointments. Am J Orthod Dentofacial Orthop. 2016;149:319–24. doi: 10.1016/j.ajodo.2015.07.040. [DOI] [PubMed] [Google Scholar]
- 8.Cioffi I, Michelotti A, Perrotta S, Chiodini P, Ohrbach R. Effect of somatosensory amplification and trait anxiety on experimentally induced orthodontic pain. Eur J Oral Sci. 2016;124:127–34. doi: 10.1111/eos.12258. [DOI] [PubMed] [Google Scholar]
- 9.Bondemark L, Fredriksson K, Ilros S. Separation effect and perception of pain and discomfort from two types of orthodontic separators. World J Orthod. 2004;5:172–6. [PubMed] [Google Scholar]
- 10.Asiry MA, Albarakati SF, Al-Marwan MS, Al-Shammari RR. Perception of pain and discomfort from elastomeric separators in Saudi adolescents. Saudi Med J. 2014;35:504–7. [PubMed] [Google Scholar]
- 11.Nalbantgil D, Cakan DG, Oztoprak MO, Arun T. Perception of pain and discomfort during tooth separation. Aust Orthod J. 2009;25:110–5. [PubMed] [Google Scholar]
- 12.Bergius M, Kiliaridis S, Berggren U. Pain in orthodontics. A review and discussion of the literature. J Orofac Orthop. 2000;61:125–37. doi: 10.1007/BF01300354. [DOI] [PubMed] [Google Scholar]
- 13.Erdinc AM, Dincer B. Perception of pain during orthodontic treatment with fixed appliances. Eur J Orthod. 2004;26:79–85. doi: 10.1093/ejo/26.1.79. [DOI] [PubMed] [Google Scholar]
- 14.Unruh AM. Gender variations in clinical pain experience. Pain. 1996;65:123–67. doi: 10.1016/0304-3959(95)00214-6. [DOI] [PubMed] [Google Scholar]
- 15.Kazanci F, Aydogan C, Alkan O. Patients’ and parents’ concerns and decisions about orthodontic treatment. Korean J Orthod. 2016;46:20–6. doi: 10.4041/kjod.2016.46.1.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jones M, Chan C. The pain and discomfort experienced during orthodontic treatment: A randomized controlled clinical trial of two initial aligning arch wires. Am J Orthod Dentofacial Orthop. 1992;102:373–81. doi: 10.1016/0889-5406(92)70054-e. [DOI] [PubMed] [Google Scholar]
- 17.Fernandes LM, Ogaard B, Skoglund L. Pain and discomfort experienced after placement of a conventional or a superelastic NiTi aligning archwire. A randomized clinical trial. J Orofac Orthop. 1998;59:331–9. doi: 10.1007/BF01299769. [DOI] [PubMed] [Google Scholar]
- 18.Ngan P, Kess B, Wilson S. Perception of discomfort’ by patients undergoing orthodontic treatment. Am J Orthod Dentofacial Orthop. 1989;96:47–53. doi: 10.1016/0889-5406(89)90228-x. [DOI] [PubMed] [Google Scholar]
- 19.Brown DF, Moerenhout RG. The pain experience and psychological adjustment to orthodontic treatment of preadolescents, adolescents, and adults. Am J Orthod Dentofacial Orthop. 1991;100:349–56. doi: 10.1016/0889-5406(91)70073-6. [DOI] [PubMed] [Google Scholar]
- 20.Sandhu SS, Sandhu J. Effect of physical activity level on orthodontic pain perception and analgesic consumption in adolescents. Am J Orthod Dentofacial Orthop. 2015;148:618–27. doi: 10.1016/j.ajodo.2015.04.037. [DOI] [PubMed] [Google Scholar]
- 21.Sandhu GPS, Kanase A, Naik C, Pupneja P, Sudan S. Separation Effect and Perception of Pain and Discomfort from Three Types of Orthodontic Separators. J Indian Orthod Soc. 2013;47:6. [Google Scholar]
- 22.Huskisson EC. Measurement of pain. Lancet. 1974;2:1127–31. doi: 10.1016/s0140-6736(74)90884-8. [DOI] [PubMed] [Google Scholar]
- 23.Vishwanath AE, Sharmada BK, Pai SS, Nandini N, Roopa T. Tooth separation potential problems. Int J Orthod Milwaukee. 2014;25:35–7. [PubMed] [Google Scholar]
- 24.Spalj S, Katic V, Vidakovic R, Slaj M, Slaj M. History of Orthodontic Treatment, Treatment Needs and Influencing Factors in Adolescents in Croatia. Cent Eur J Public Health. 2016;24:123–7. doi: 10.21101/cejph.a4117. [DOI] [PubMed] [Google Scholar]
- 25.Yamaguchi M, Kasai K. Inflammation in periodontal tissues in response to mechanical forces. Arch Immunol Ther Exp. 2005;53:388–98. [PubMed] [Google Scholar]
- 26.Ngan P, Wilson S, Shanfeld J, Amini H. The effect of ibuprofen on the level of discomfort in patients undergoing orthodontic treatment. Am J Orthod Dentofacial Orthop. 1994;106:88–95. doi: 10.1016/S0889-5406(94)70025-7. [DOI] [PubMed] [Google Scholar]
- 27.Scheurer PA, Firestone AR, Burgin WB. Perception of pain as a result of orthodontic treatment with fixed appliances. Eur J Orthod. 1996;18:349–57. doi: 10.1093/ejo/18.4.349. [DOI] [PubMed] [Google Scholar]
- 28.Feinmann C, Ong M, Harvey W, Harris M. Psychological factors influencing post-operative pain and analgesic consumption. Br J Oral Maxillofac Surg. 1987;25:285–92. doi: 10.1016/0266-4356(87)90067-2. [DOI] [PubMed] [Google Scholar]