

Abstract
Successful surgical management of a case of congenital aneurysm of the left sinus of Valsalva involving the left main coronary artery has been reported. To our knowledge, this is the first report describing an unusual case of congenital aneurysm of the left sinus of Valsalva, which involves the left main coronary artery.
Keywords: left sinus of Valsalva, aneurysm, left main coronary artery, congenital
Congenital aneurysms of the sinus of Valsalva (SOV) are the most common sinus aneurysm. This results from the absence of aortic wall media where the aorta attaches to the valve tissue.1 The most common site of those aneurysms is the right sinus (94%), then the noncoronary (5%), and the least of all is the left sinus where only 1% is reported.2 Comprehensive review of the literature shows that the left main coronary artery (LMCA) is usually compressed by the aneurysm mass.3 4 5 In the current case, an aneurysm of the left SOV has been reported with no coronary artery compression, although the LMCA is part of the aneurysm. To our knowledge, we know of no prior case study of this nature in the literature.
Case Study
The patient was a 35-year-old female with a history of 2 years exertional dyspnea and a recent onset of chest discomfort. She denied cough, hemoptysis, fever, and chest pain at rest. Upon physical examination (P/E), she had blood pressure: 110/65 and pulse: 90 with no respiratory distress. She had a flat jugular venous pressure and the cardiovascular examination showed symmetrical normal pulses, a systolic murmur II/VI, and a diastolic murmur III/VI at the aortic area. Lungs and the rest of P/E were normal. The patient was married and had undergone a cesarean section 10 years earlier. The chest X-ray showed a normal cardiothoracic ratio with increased lung vascular marking. Pulmonary function tests and diffusing capacity of lung for carbon monoxide were normal. Electrocardiogram showed inverted T waves in leads V1–V4. Echocardiogram revealed normal left ventricle size and systolic function with left ventricular ejection fraction (EF) of 55%. Dilation of the LMCA and the left coronary sinus were reported with mild-to-moderate aortic insufficiency (AI) and aortic valve (AV) annulus of 2.2 cm. Ascending aorta was normal. Mild tricuspid regurgitation and mild mitral regurgitation (MR) were reported with normal pulmonary artery pressure (PAP) of 25 to 30 mm Hg. A small patent ductus arteriosus was also noted. Cardiac catheterization and aortography showed an aneurysmal left SOV involving the LMCA. Coronary branches were shown to arise from this aneurysm (Fig. 1a, b). Also, a moderate AI was noted.
Fig. 1.
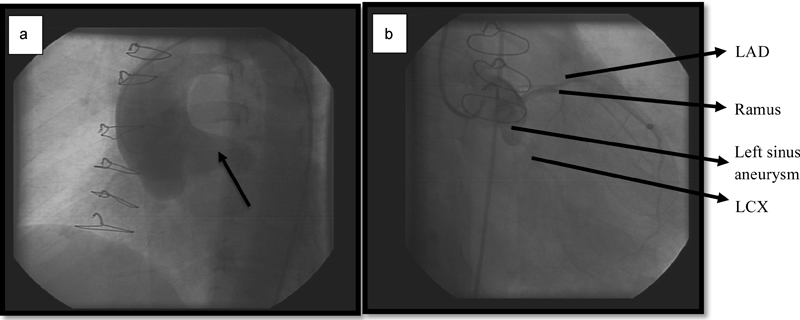
(a) Aortogram showing the aneurysm of the left sinus of Valsalva. (b) Attempted coronary angiography showing the left sinus aneurysm with coronary arteries at the end LAD and LCX arteries at the end. LAD, left anterior descending; LCX, left circumflex.
At Surgery
On cardiopulmonary bypass and under cardioplegic arrest, the back of the aorta was initially dissected. After the standard oblique aortotomy, a left sinus aneurysm that included the LMCA ostium was noted. Coronary artery branches seen at the base end of this aneurysm were probed and proved to be related to the left anterior descending, ramus, and the left circumflex arteries. To separate the aneurysm from the aorta, a circular incision around the LMCA ostium was made (Fig. 2a).
Fig. 2.
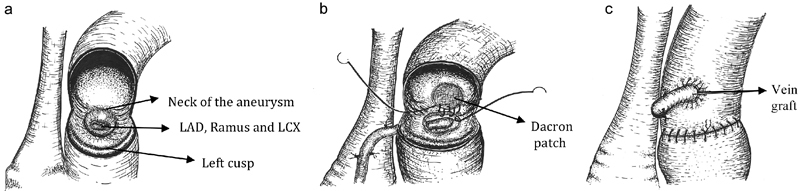
(a) Left sinus of Valsalva aneurysm, (b) circumferential excision of the aneurysm resection and the bypass of the left main branches and patch repair of the sinus. (c) Closed aorta and completed proximal anastomosis. LAD, left anterior descending; LCX, left circumflex.
The body of the aneurysm was resected. Both the aneurysmal sinus and the LMCA were excluded. The three coronary ostias at the end of the aneurysm were connected to the tailored end of a segment of reverse saphenous vein (RSV). Then the left sinus defect was repaired with a Dacron patch (GETINGE Group, MAQUET Cardiovascular LLC, San Jose, CA) (Fig. 2b). AV leaflets were healthy. Commissural repair was done using 4.0 pledgeted sutures. The aortotomy was closed and the proximal end of the RSV graft was anastomosed to the ascending aorta (Fig. 2c).
After Surgery
The postoperative course was uneventful. Echocardiogram showed a mild AI and MR, normal EF and a normal PAP. The myocardial perfusion scan was also normal. One year after the surgery, the patient expressed no chest discomfort or dyspnea. Additionally, aortography and coronary angiography showed normal graft and coronary functions (Fig. 3a, b). Follow-up at 2 and 4 years, respectively, on clinical and echocardiographic evaluations showed an unchanged mild AI with a normal EF and the patient remained symptom free.
Fig. 3.
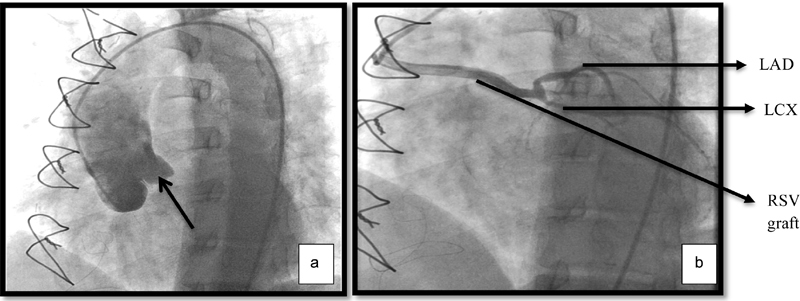
(a) One-year postoperation angiography, aortogram, showing the repaired left sinus of Valsalva. (b) Coronary angiography showing the saphenous vein and the coronary artery branches. LAD, left anterior descending; LCX, left circumflex; RSV, reverse saphenous vein.
Discussion
Congenital aneurysm of the left SOV is rare.2 Of the 20 cases reported by Lijoi et al in 2002 with coronary compression and angina, only 13 were congenital in origin.2 Since then, few additional congenital cases of the left SOV were reported with coronary compression symptoms, aneurysm rupture, or heart failure.4 5 6 7 8 A rare case of an aneurysm of the left SOV with an intramural LMCA presenting with angina was also reported.9 Our case is unique in that the patient had chest pain and exertional dyspnea without evidence of coronary compression. She had an aneurysm of the left SOV, which included the LMCA.
A recent increase in chest pain and evidence of a large aneurysm of the left sinus, which by itself has been reported as a cause of sudden death,2 as well as a mild-to-moderate AI, were the reasons why surgical intervention was indicated in the current case. Aneurysm of the LMCA is a rare condition and occurs in only approximately 0.1% of the population, and their managements have been previously reported.2 10 To our knowledge, a congenital aneurysm of the left SOV involving the LMCA has not been reported. This unique congenital aneurysm seems to differ from the usual congenital aneurysms in that it arises from the nadir of the sinus. These are thought to be due to the absence of the aortic media at the junction of the sinus and the AV.6 Our successful surgical repair consisted of direct patching of the sinus defect. We performed graft replacement of the LMCA to the base of the aneurysm containing the ostias of the three branches of the LMCA. A 1-year echocardiography follow-up showed mild AI that had not changed and coronary angiography demonstrated a well-functioning graft. At 4 years postsurgery, the patient was asymptomatic and the echocardiographic evaluations showed no change.
Conclusion
We have described a rare case with symptoms of cardiac ischemia proved to have a left SOV aneurysm, which also included the LMCA. Although rare, aneurysms of the coronary sinuses as well as their surgical management should be considered.
Declaration
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
References
- 1.Ring W. Oxford: Blackwell Publishing Ltd; 2013. Sinus of Valsalva aneurysm; pp. 704–714. [Google Scholar]
- 2.Lijoi A, Parodi E, Passerone G C, Scarano F, Caruso D, Iannetti M V. Unruptured aneurysm of the left sinus of Valsalva causing coronary insufficiency: case report and review of the literature. Tex Heart Inst J. 2002;29(1):40–44. [PMC free article] [PubMed] [Google Scholar]
- 3.Bjursten H, Harnek J, Cunha-Goncalves D, Koul B. Giant aneurysm in the sinus of Valsalva presenting as an acute coronary symptom. Interact Cardiovasc Thorac Surg. 2013;17(1):193–195. doi: 10.1093/icvts/ivt127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Imai A, Matsuzaki K, Imazuru T, Jikuya T. Myocardial angina due to compression of the left coronary artery by a large aneurysm in the left sinus of Valsalva. Jpn J Cardiovasc Surg. 2011;40(2):54–57. [Google Scholar]
- 5.Uchimuro T, Fukui T, Nakamichi T, Mihara W, Takanashi S. Coronary arterial compression caused by an aneurysm of the sinus of Valsalva with aortic prosthetic valve endocarditis. Gen Thorac Cardiovasc Surg. 2012;60(12):834–836. doi: 10.1007/s11748-012-0095-2. [DOI] [PubMed] [Google Scholar]
- 6.Hakami A, Stiller B, Hetzer R. Unruptured congenital aneurysm of the left sinus of Valsalva in an adult with complex left heart malformations. Heart. 2003;89(1):e3. doi: 10.1136/heart.89.1.e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hausinger P, Sasi V, Volford G. et al. Unruptured aneurysm of the left sinus of Valsalva compressing the left main coronary artery: successful percutaneous treatment. Herz. 2014;39(6):770–773. doi: 10.1007/s00059-013-3891-2. [DOI] [PubMed] [Google Scholar]
- 8.Vadivelu R, Rohit M K, Yadav M. Ruptured sinus of Valsalva aneurysm from left coronary sinus into right atrium: a rare anomaly with an odd presentation. BMJ Case Rep. 2013;2013:bcr2012007855. doi: 10.1136/bcr-2012-007855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Altarabsheh S E, Deo S V, Spitell P, Araoz P, Park S J. An intramural left main coronary artery with a left sinus of Valsalva aneurysm: a unique combination of congenital anomalies. Heart Surg Forum. 2013;16(1):E35–E37. doi: 10.1532/HSF98.20121076. [DOI] [PubMed] [Google Scholar]
- 10.Topaz O, DiSciascio G, Cowley M J. et al. Angiographic features of left main coronary artery aneurysms. Am J Cardiol. 1991;67(13):1139–1142. doi: 10.1016/0002-9149(91)90881-k. [DOI] [PubMed] [Google Scholar]