

Abstract
Dextrocardia is a rare cardiac anomaly in which the heart is located in the right chest along with the cardiac long axis directing to the right and inferiorly. Although, it is a rare clinical phenomenon, coronary artery disease with dextrocardia is presumed to be of similar frequency as in the general population. Percutaneous coronary intervention has some technical difficulties in these patients. We hereby report a male patient with dextrocardia who was previously treated with coronary artery bypass graft surgery.
Keywords: coronary angiography, chronic total occlusion, coronary artery disease, dextrocardia
Clinical Presentation and Intervention
A 70-year-old man was admitted to our hospital with intermittent retrosternal chest pain radiating to the right shoulder and lasting for a few weeks. He was a known case of situs inversus with dextrocardia and had undergone coronary artery bypass graft (CABG) surgery 3 years ago. His initial clinical examination was consistent with the findings of dextrocardia. Routine biochemistry was normal. A 12 lead electrocardiogram showed a negative P wave in the I and aVL limb leads, a positive P wave in aVR limb leads, a prominent S wave in the left-sided chest leads, and a prominent R wave in the right-sided chest leads, which is suggestive of situs inversus with dextrocardia. Transthoracic echocardiography revealed mild hypokinesia in the inferior wall and the left ventricular ejection fraction was 55%. After a positive exercise stress test, the patient underwent coronary angiography which was performed via the right femoral artery. Selective coronary cannulation of left coronary sinus was performed by Judkins left (JL-4) catheter rotation, and selective cannulation of right coronary artery (RCA), saphenous vein, and internal mammary artery grafts was performed by Judkins right (JR-4) catheter. Counterclockwise rotation with slight withdrawal was required for the cannulation of RCA and saphenous vein grafts.
Coronary angiography showed that the left anterior descending (LAD) coronary artery was totally occluded after giving off the first diagonal artery branch; the left circumflex (LCX) coronary artery was nondominant and the right internal mammary artery graft was occluded (Fig. 1). Coronary angiography also demonstrated a total occlusion of the ostium of the RCA, and the saphenous vein—RCA and saphenous vein—diagonal artery grafts were patent. Percutaneous coronary intervention for the chronic totally occluded LAD was planned. The left main coronary artery was selectively cannulated with an extra backup guiding catheter (6 French extra backup [EBU] 3.5, Medtronic, Inc, Launcher 6F (EBUS 3.5) guiding catheter, MN) with ease. The lesion was crossed with a guidewire (ASHAI Fielder XT, Abbott Vascular, CA) and dilated with a 1.5 × 20 mm balloon. A 2.25 × 28 mm drug eluting stent (Xience, Abbott Vascular, CA) was deployed at 12 atmosphere (atm) (Fig. 2). The stent was postdilated with a 2.5 × 20 mm noncompliant balloon at 12 atm, and TIMI 3 flow was achieved (Fig. 3).
Fig. 1.
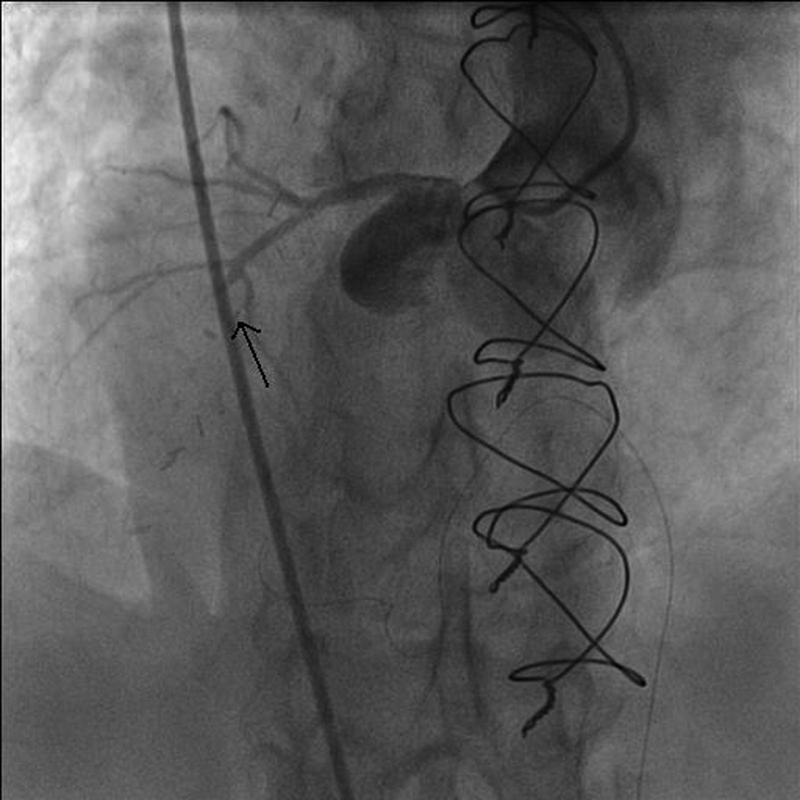
Coronary angiography (posteroanterior view) showing total occlusion of left anterior descending coronary artery.
Fig. 2.
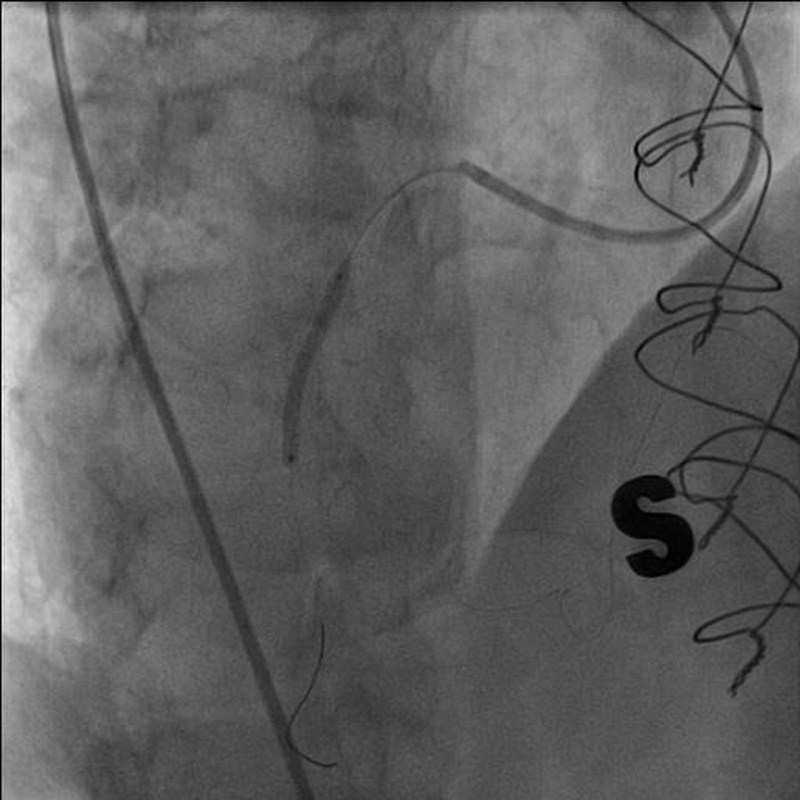
Angiography showing the stenting of left anterior descending coronary artery after crossing with guidewire.
Fig. 3.
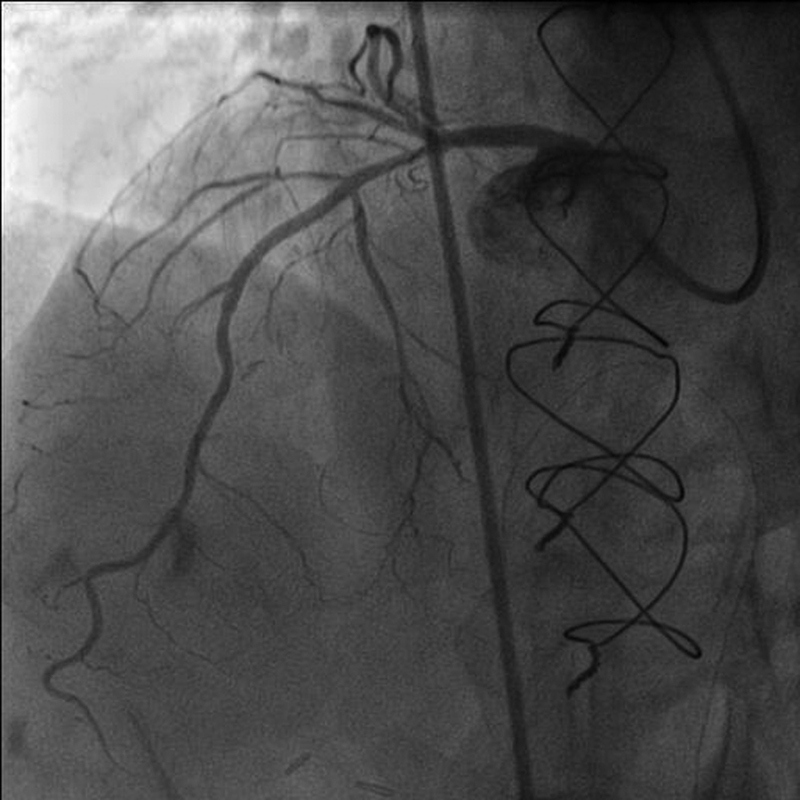
Coronary angiography (LAO cranial) after stenting showing TIMI 3 flow.
The patient's hospital course was uneventful and he was discharged on clopidogrel, acetylsalicylic acid, atorvastatin, metoprolol, and amlodipine.
Discussion
Dextrocardia is a rare anomaly occurring with a frequency of 1/10,000 in the general population.1 This anomaly can occur in isolation as situs solitus or in association with situs inversus or situs ambiguous.2 In situs inversus, all the visceral organs, including the heart and liver, are located on the opposite side as compared with normal, whereas in situs solitus only the heart is located in the right chest. The life expectancy of patients with dextrocardia is considered to be normal and the incidence of coronary artery disease is thought to be similar to that of the general population.3
Coronary angiography for dextrocardia was first reported in 1974.4 Coronary artery bypass surgery in a patient with dextrocardia was first reported in 1982.5 Percutaneous coronary intervention in dextrocardia with situs inversus was first reported in 1987.6 A few cases, including percutaneous coronary intervention for patients with dextrocardia, have been reported up to date previously.7 8 9 To our knowledge, our patient is the only patient with dextrocardia and coronary bypass grafts undergoing percutaneous coronary intervention for a chronic totally occluded coronary artery.
It is thought that regular coronary catheters are difficult to use because of the mirror image of the coronary arteries.6 However, we did not experience any difficulty during the cannulation of either the coronary arteries or grafts. Only a counterclockwise rotation with slight withdrawal was required for the cannulation of the RCA and saphenous vein grafts. The selective left coronary angiograms were obtained in the right anterior oblique, cranial, posteroanterior cranial, and left anterior oblique caudal views. The selective RCA and saphenous graft angiograms were obtained in the right anterior oblique caudal, posteroanterior cranial, and left anterior oblique cranial views. A visualization of a mirror image will help to visualize the anatomy of the coronary arteries and rotation and withdrawal of routine coronary artery catheters in an opposite direction to that of normal theoretically assist the cannulation of the coronary arteries during coronary angiograms. Also, a well-engaged guiding catheter is essential for the success of the percutaneous coronary procedures. In our case, chronic total occlusion of the culprit artery was difficult for intervention. However, a cannulation with an EBU catheter resulted in cannulation of the occluded coronary artery.
In summary, our case shows that even patients with previous CABG and dextrocardia may be suitable cases for coronary angiography and percutaneous coronary intervention.
References
- 1.Rosenberg H N, Rosenberg I N. Simultaneous association of situs inversus, coronary heart disease and hiatus hernia; report of a case and review of literature. Ann Intern Med. 1949;30(4):851–859. doi: 10.7326/0003-4819-30-4-851. [DOI] [PubMed] [Google Scholar]
- 2.Maldjian P D Saric M Approach to dextrocardia in adults: review. AJR Am J Roentgenol 2007188(6, Suppl):S39–S49, quiz S35–S38 [DOI] [PubMed] [Google Scholar]
- 3.Hynes K M, Gau G T, Titus J L. Coronary heart disease in situs inversus totalis. Am J Cardiol. 1973;31(5):666–669. doi: 10.1016/0002-9149(73)90341-x. [DOI] [PubMed] [Google Scholar]
- 4.Ettinger P O, Brancato R, Penn D. Dextrocardia, anteroseptal infarction, and fascicular block. Chest. 1975;68(2):229–230. doi: 10.1378/chest.68.2.229. [DOI] [PubMed] [Google Scholar]
- 5.Irvin R G, Ballenger J F. Coronary artery bypass surgery in a patient with situs inversus. Chest. 1982;81(3):380–381. doi: 10.1378/chest.81.3.380. [DOI] [PubMed] [Google Scholar]
- 6.Moreyra A E, Saviano G J, Kostis J B. Percutaneous transluminal coronary angioplasty in situs inversus. Cathet Cardiovasc Diagn. 1987;13(2):114–116. doi: 10.1002/ccd.1810130208. [DOI] [PubMed] [Google Scholar]
- 7.Menozzi M, Guiducci V, Pignatelli G, Giacometti P, Manari A. Coronary stenting using the radial approach in two women with situs viscerum inversus and acute myocardial infarction. Cardiovasc Revasc Med. 2012;13(2):128–132. doi: 10.1016/j.carrev.2010.06.006. [DOI] [PubMed] [Google Scholar]
- 8.Aksoy S, Cam N, Gurkan U, Altay S, Bozbay M, Agirbasli M. Primary percutaneous intervention: for acute myocardial infarction in a patient with dextrocardia and situs inversus. Tex Heart Inst J. 2012;39(1):140–141. [PMC free article] [PubMed] [Google Scholar]
- 9.Munawar M, Hartono B, Iskandarsyah K, Nguyen T N. Successful percutaneous coronary intervention for chronic total occlusion of right coronary artery in patient with dextrocardia. Cardiovasc Interv Ther. 2013;28(3):303–306. doi: 10.1007/s12928-013-0166-z. [DOI] [PubMed] [Google Scholar]