

Abstract
Background and Aims:
Sepsis is a complex rapidly progressive infectious disease that remain a major cause of morbidity and mortality in surgical patients and trauma victims. Edaravone a novel free radical scavenger was approved in 2001 in Japan for treatment of acute cerebral and myocardial infarction. Hence, in this work we attempt to evaluate its role in cases of septic peritonitis (SP).
Material and Methods:
This is a prospective randomized observer-blinded study carried out in surgical Intensive Care Unit (ICU) after approval by Hospital Ethical Committee. After admission to ICU patients were randomly divided into two groups of thirty patients each-Group (C): Control group managed according to the routine protocol of sepsis and Group (E): Edaravone treated SP managed according to the routine protocol of sepsis + edaravone at dose of 30 mg/12 h intravenous infusion for 2 weeks. All patients were monitored for invasive blood pressure, central venous pressure, heart rate, temperature, urine output, total fluid balance, and routine investigation. Blood sample was taken weekly for 2 weeks to measure the following parameters: Nuclear transcription factor kappa B activity (NFKB), mitogen-activated protein kinase (MAPK), heat shock protein 72 (HSP 72) and total antioxidant capacity (TAC).
Results:
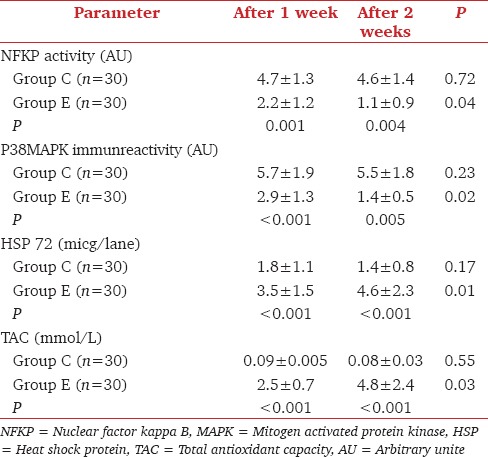
There was significant decrease (P < 0.05) in serum level of NFKB, MAPK in Group E in comparison with Group C. While serum level of HSP 72 and TAC showed significant increase (P < 0.05) in Group E compared with Group C with better outcome.
Conclusion:
SP treatment with edaravone could significantly improve the inflammatory and oxidative states with better patient outcomes.
Key words: Chemical markers, edaravone, Intensive Care Unit, septic peritonitis
Introduction
Sepsis is a clinical syndrome that results from complex interaction between host and infectious agents and is characterized by systemic activation of multiple inflammatory pathways.[1] The pathophysiology of sepsis could be initiated by the outer membrane components of Gram-negative and Gram-positive organisms. Signaling by these mediators occurs via a family of transmembrane receptors known as toll like receptors.[2] Within the monocyte, nuclear factor kappa B (NFKP) and mitogen activated protein kinase (MAPK) are activated which lead to production of proinflammatory cytokines.[3]
It is thought that edaravone has antioxidant action, inhibits lipid peroxidation and causes quenching of active oxygen leading to protection of various cells against damage by reactive oxygen species.[4] Some studies have shown beneficial effect of edaravone on postischemic reperfusion injury in cardiac, cerebral and hepatic tissues.[5] However the putative mechanisms underlying the beneficial effect of edaravone are still not clear. So, in this work we attempt to evaluate its role in cases of septic peritonitis (SP).
Material and Methods
This is a prospective observer-blinded study carried out in surgical Intensive Care Unit (ICU) during the period from March 2014 to April 2015 in 60 patients with SP after approval by Hospital Ethical Committee. The CONSORT 2010 statement was followed in reporting this study.
Inclusion criteria included American Society of Anesthesiologists physical status I or II having SP after gastrointestinal perforation (perforated peptic ulcer, traumatic intestinal perforation or postcorrection of intestinal anastomosis leakage).
Exclusion criteria included patients in septic shock, on vasopressor or with one or more organ dysfunction.
Criteria of sepsis according to American College of Chest Physician/Society of Critical Care Medicine definitions which include strongly suspected infection or positive blood culture plus two or more of the following: Temperature >38°C or <36, heart rate (HR) >90 b/min, respiratory rate >20 C/min, PCO2<32 mmHg and white blood cells >12000 mm3 or <4000 mm3.[6]
All patients were treated with antibiotics according to culture and sensitivity test and received intravenous (IV) fluids to keep central venous pressure (CVP) ≥12 Cm H2O and mean arterial pressure ≥65 mmHg.
Randomization was performed using a random number list generated by means of the QuickCalcs (GraphPad Software Inc., La Jolla, CA, USA). The group assignment numbers were sealed in an envelope and kept by the study supervisor. After admission to ICU a written informed consent was obtained from each patient. Patients were randomly divided into two groups of thirty patients each-Group (C): Control group managed according to the routine protocol of sepsis and Group (E): Edaravone treated SP managed according to the routine protocol of sepsis + edaravone at dose of 30 mg/12 h IV infusion for 2 weeks.[7]
Edaravone was supplied from Sigma Company (license from Mitsubishi pharmaceutical, Inc.). Each ampoule of 20 ml contained 30 mg of the drug diluted in saline.
All patients were monitored for invasive blood pressure, HR, CVP, temperature, urine output, total fluid balance and routine investigations (complete blood cell count, arterial blood gases, serum electrolytes, liver, and kidney function tests).
Blood sample were taken weekly for 2 weeks to measure the following parameters:
Nuclear transcription factor kappa B activity (NFKB) was measured in activated monocyte macrophage by ELISA based kits assay against P50 and P65 (Trans AM. NFKB P56 from active motif Rixensart Belgium).[8]
MAPK was measured in activated monocyte/macrophage by nonradioactive assay kits (western blot analysis kits) from cell signaling technology Inc., U.S.A).[9]
Heat shock protein 72 (HSP 72), an indicator for intracellular response to stress, was measured by immunoblotting.[10]
Total antioxidant capacity (TAC) was measured by ferric reducing ability of plasma method, comparing absorbance changes at 593 nm which will be linear over a wide concentration range of antioxidant mixtures.[11]
Statistical analysis
Sample size of thirty patients was calculated for 90% power, α = 0.05, β = 0.1, and anticipated effect size = 0.40 using sample size software (G*Power Version 3.00.10, Germany). Analytic statistics was performed on IBM compatible computer using SPSS 11.5 software (SPSS Inc., Chicago, IL) package under Windows XP operating system. All results are presented in the form of mean ± standard deviation. Data was compared using unpaired Student's t-test; P < 0.05 was considered statistically significant.
Results
30 patients in each group completed the study [Figure 1]. There was significant decrease (P < 0.05) in serum level of NFKB, MAPK in Group E in comparison with Group C. While serum level of HSP 72 and TAC showed significant increase (P < 0.05) in Group E in comparison with Group C. Mortality rate was lower in Group E than in Group C. The number of patients developed septic shock was lower in Group E than in Group C [Tables 1 and 2].
Figure 1.

The randomized trial flow diagram, including enrollment, intervention allocation, and analysis
Table 1.
Patients’ demographic data and outcome
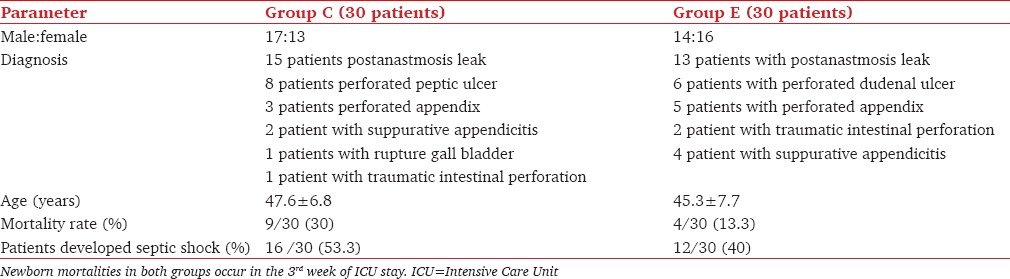
Table 2.
Effect of edaravone on blood level of nuclear factor kappa B, P38 mitogen activated protein kinase, heat shock protein 72 and total antioxidant capacity
Discussion
This work demonstrated that the edaravone treated SP group recorded significant improvement in the inflammatory and oxidative processes in comparison with control group manifested by a significant decrease in serum level of P38 MAPK and NFKB.
Septic shock can initiate an inflammatory response which is characterized by up regulation of cytokine expression and neutrophil accumulation in a variety of tissues.[12]
The cytokine expression is mediated by two separate signal pathways: P38 MAPK and NFKB in activated monocyte/macrophages which are activated by several incoming signals from cell surface including the reactive oxidative intermediates and lipopolysaccharides of most clinically relevant Gram-negative organisms found in septic infection.[1]
The expression of several inflammatory cytokines as tumor necrosis factor alpha (TNF-α) and interleukin 6 bind to their receptors in various cell types resulting in functional impairment.[13]
Edaravone is a free radical scavenger quenching of reactive oxygen and hence attenuating the oxidative process and inhibiting subsequent injurious inflammation by reducing expression of inflammatory cytokines and adhesion molecules.[5]
Yoshida et al., 2008[14] stated that edaravone has an anti-inflammatory effect by inhibiting induction of Inducible nitric oxide synthase (iNOS) as well as pro-inflammatory cytokines TNF-α and this is mediated by the inhibiting activity of transcription factor NFK-B which is an essential signal for iNOS production. Also, edaravone could decrease the stability of iNOS mRNA and hence decreasing expression of iNOS. The inhibition of NO production will subsequently inhibit production of perioxynitrite and hence attenuat lipid peroxidation.[15]
Higashi et al.,[5] stated that edaravone could inhibit lipoxygenase metabolism of arachidonic acid by trapping hydroxyl radicals. Also it could inhibit alloxan induced lipid peroxidation and hence prevent cellular damage.
Moreover, Suzuki et al.[16] demonstrated that the antioxidant action of edaravone could be attributed partly to the enhancement of prostacyclin production leading to protection of various cells.
In addition, this work demonstrated a significant increase in serum level of cytoprotective HSP 72 in edaravone treated SP group in comparison with control one. Although the mechanism of HSP production is still unclear, it may be attributed to activation of adenosine monophosphate-activated protein kinase and MAPKs.[17] Activation of these intracellular signaling pathways cause quiescent cells to enter the cell cycle and initiate regenerative response inducing HSP as sort of stress adaptation.[18] Heat shock 72 are intracellular proteins (named according to their molecular weight) which present in small amount in normal cells and a larger amount in cells subjected to a variety of stressful stimuli as a sort of cellular defense mechanism protecting cells from excessive stress damage. Also, they play a role in protein-protein interaction stabilizing the protein conformation and preventing the unwanted protein aggregation.[19]
This study elucidated that edaravone induced a significant increase in TAC of plasma in comparison with a control group which could be attributed partly to the significant increase in serum level of HSP 72 induced by edaravone. Zhi et al.,[10] stated that HSP 72 could increase the antioxidant capacity of cells.
Tamamura et al.,[20] elucidated that edaravone could reduce the oxidative stress by enhancing the production of HSP, which could limit cellular injury by refolding the disrupted protein stabilizing cell membrane and hence attenuating neutrophil infiltration.
Conclusion
In cases of SP treatment with edaravone could significantly improve the inflammatory and oxidative states with better patient outcomes. However, further investigation is needed to clarify other possible underlying mechanisms.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Ulloa L, Brunner M, Ramos L, Deitch EA. Scientific and clinical challenges in sepsis. Curr Pharm Des. 2009;15:1918–35. doi: 10.2174/138161209788453248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Navneet K, Lui F. Sepsis- guidelines, treatment and novel approach. Crit Care. 2008;12:120–8. doi: 10.1186/cc6836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Barnato AE, Alexander SL, Linde-Zwirble WT, Angus DC. Racial variation in the incidence, care, and outcomes of severe sepsis: Analysis of population, patient, and hospital characteristics. Am J Respir Crit Care Med. 2008;177:279–84. doi: 10.1164/rccm.200703-480OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Xu JZ, Shen BZ, Li Y, Zhang T, Xu WH, Liu XW, et al. Edaravone attenuates ischemia-reperfusion injury by inhibiting oxidative stress in a canine lung transplantation model. Chin Med J (Engl) 2008;121:1583–7. [PubMed] [Google Scholar]
- 5.Higashi Y, Jitsuiki D, Chayama K, Yoshizumi M. Edaravone (3-methyl-1-phenyl-2-pyrazolin-5-one), a novel free radical scavenger, for treatment of cardiovascular diseases. Recent Pat Cardiovasc Drug Discov. 2006;1:85–93. doi: 10.2174/157489006775244191. [DOI] [PubMed] [Google Scholar]
- 6.Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31:1250–6. doi: 10.1097/01.CCM.0000050454.01978.3B. [DOI] [PubMed] [Google Scholar]
- 7.Li H, Xu K, Wang Y, Zhang H, Li T, Meng L, et al. Phase I clinical study of edaravone in healthy Chinese volunteers: Safety and pharmacokinetics of single or multiple intravenous infusions. Drugs R D. 2012;12:65–70. doi: 10.2165/11634290-000000000-00000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kevin A, Adleina H, Michel K, Steven F. A method for measuring multiple cytokines from small samples. Brain Behav Immun. 2004;18:274–80. doi: 10.1016/j.bbi.2003.09.009. [DOI] [PubMed] [Google Scholar]
- 9.Nick J, Advic N, Gerwi SP, Uorthen G. Activation of P38 MAPK in human neutrophil by lipopolysaccharide. J Immunol. 1996;156:4867–75. [PubMed] [Google Scholar]
- 10.Zhi J, Cong J, Mua W. Expression of HSP 72 in lung tissues of acute paraquat poisoned rats. World J Emerg Med. 2010;1:229–33. [PMC free article] [PubMed] [Google Scholar]
- 11.Benzie IF, Strain JJ. The ferric reducing ability of plasma (FRAP) as a measure of “antioxidant power”: The FRAP assay. Anal Biochem. 1996;239:70–6. doi: 10.1006/abio.1996.0292. [DOI] [PubMed] [Google Scholar]
- 12.Rosas B, Olofssan P, Ochani M, Valdes S, Levine Y. Neural circuits regulate cytokine production to prevent potentially damaging inflammation. Science. 2011;334:98–101. [Google Scholar]
- 13.Marial I, Apostolos P, Jlias K, Andreas C, George Z. Redox state and the potential role of antioxidant compounds in liver ischemia reperfusion injury. Int J Med Med Sci. 2010;2:200–9. [Google Scholar]
- 14.Yoshida H, Kwon A, Masaki K, Yasuo K, Seije T, Okumura T. Edaravone prevents iNOS expression by inhibiting its promoter transactivation and mRNA stability in cytokine stimulated hepatocytes. Nitric oxide. 2008;18:105–12. doi: 10.1016/j.niox.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 15.Hamaishi M, Orihashi K, Isaka M, Kumagai H, Takahashi S, Okada K, et al. Low-dose edaravone injection into the clamped aorta prevents ischemic spinal cord injury. Ann Vasc Surg. 2009;23:128–35. doi: 10.1016/j.avsg.2008.05.010. [DOI] [PubMed] [Google Scholar]
- 16.Suzuki Y, Nakao A, Fujita T, Noiri E. Radical scavenger edaravone developed for clinical use ameliorates ischemia/reperfusion injury in rat kidney. Kidney Int. 2004;65:1714–23. doi: 10.1111/j.1523-1755.2004.00567.x. [DOI] [PubMed] [Google Scholar]
- 17.Narberhaus F. Translational control of bacterial heat shock and virulence genes by temperature-sensing mRNAs. RNA Biol. 2010;7:84–9. doi: 10.4161/rna.7.1.10501. [DOI] [PubMed] [Google Scholar]
- 18.Salinthone S, Tyagi M, Gerthoffer WT. Small heat shock proteins in smooth muscle. Pharmacol Ther. 2008;119:44–54. doi: 10.1016/j.pharmthera.2008.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chao L, Zhen L, Makoto K, Yuzo Y, Yoshio Y. HSP 72 normothermic ischemia and the impact of congested portal blood reperfusion on rat liver. World J Gastroenterol. 2001;7:415–8. doi: 10.3748/wjg.v7.i3.415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tamamura M, Motokair S, Yukakok, Saton K. Protective effect of edaravone on ischemia reperfusion injury in rat testis. BJU Int. 2010;105:870–6. doi: 10.1111/j.1464-410X.2009.08798.x. [DOI] [PubMed] [Google Scholar]