

Abstract
A prominent behavioral manifestation of impulsivity in children with attention-deficit/hyperactivity disorder (ADHD) is inappropriate language production, such as talking excessively, blurting out answers, and interrupting others.
Objective
In this study, we examined language production in ADHD and non-ADHD controls to determine whether these types of language production problems are apparent in adults with ADHD.
Method
Participants (18–35 years old, 53.3% male) were asked to describe networks of colored dots that contained two branches that differed in length and complexity. According to the Minimal-Load Principle (Levelt, 1989), participants should prefer to describe a shorter and less complex branch first, in order to minimize planning and memory demands when formulating a description of the network. The dependent measures focused on which branch participants chose to describe first and the fluency of the descriptions. Four types of disfluency were examined: filled pauses, silent pauses, repetitions, and repairs.
Results
There was no difference between ADHD participants and controls in the decisions they made when describing the networks (p > .10, η2 = .004). Participants in both groups preferred to describe a short branch before describing a long branch and decisions were unaffected by complexity. However, ADHD participants did produce more words overall, t(73) = −2.33, p < .05, η2 = .07, and they also produced more disfluencies, F(4, 70) = 2.98, p < .05, η2 = .15, even after adjusting for number of words produced.
Conclusions
These findings suggest less language efficiency and reduced fluency in ADHD, and that language production issues remain in adults with ADHD, similar to the issues commonly reported in children with ADHD.
Keywords: attention-deficit/hyperactivity disorder, language production, network task, disfluency production, disfluencies
Attention-deficit/hyperactivity disorder (ADHD) affects approximately 6% of children and has now been recognized as persisting into adolescence and adulthood in a substantial percentage of cases, with an estimated 4% of adults affected in the United States (Barkley, Fischer, Smallish, & Fletcher, 2002; Kessler et al., 2006). ADHD reflects impaired levels of hyperactivity, impulsivity, and/or inattention. The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM–IV; American Psychiatric Association, 2000) identifies three subtypes based on levels of presenting symptoms: primarily hyperactive/impulsive (ADHD-PH), primarily inattentive (ADHD-PI), and combined (ADHD-C). Extensive research has now demonstrated that at least one mechanism involved in ADHD is a breakdown in the deliberate suppression of motor and oculomotor responses (e.g., Carr, Nigg, & Henderson, 2006; Schachar, Tannock, Marriott, & Logan, 1995). These response inhibition deficits have figured into prominent theoretical accounts of this disorder (Barkley, 1997; Nigg, 2001, 2006).
Children with ADHD often have some co-occurring language problems, including both expressive and receptive language delays (August & Garfinkel, 1990; Beitchman & Young, 1997; Cohen, Davine, Horodezky, Lipsett, & Isaacson, 1992; Denckla, 1996; Hinshaw, 1992; Nigg, Hinshaw, Carte, & Treuting, 1998; Tirosh & Cohen, 1998). Estimates of the comorbidity between ADHD and language impairments vary quite widely (i.e., from 15%–75%), depending on whether the sample is clinically referred or community recruited. However, most reports fall in the 40%– 45% range (Beitchman, Hood & Inglis, 1990; Tirosh & Cohen, 1998). Formal learning disabilities are also common in ADHD, and the most prevalent of these is reading disability, which co-occurs at a rate of 15% to 30% with ADHD (Dykman & Ackerman, 1991; Willcutt & Pennington, 2000). General language impairments in children with ADHD can include delayed onset of words, poor performance on standardized tests, and pragmatic problems, such as difficulty in conversation (Cantwell, 1996; Johnson, Miller, Curtiss, & Tallal, 1993; Rashid, Morris, & Morris, 2001; Redmond, 2004; Scott & Windsor, 2000; Tannock, Purvis, & Schachar, 1993; Willcutt et al., 2001). These language-related difficulties contribute to wideranging detrimental effects on quality of life, such as poorer social functioning, lower academic achievement, and later in life, lower occupational attainment (Biederman et al., 2006; Mapou, 2009).
The focus of the current study was whether adults with ADHD experience breakdowns in the control of language output (i.e., speech production). Understanding language production problems in adults with ADHD has important implications for understanding the developmental mechanisms involved with ADHD. This is because speech production matures relatively early, but cognitive control matures relatively late, primarily because of ongoing myelination of brain networks into late adolescence and early adulthood (Giedd et al., 1999). Two language production possibilities exist. The first is that language production problems in childhood ADHD might simply be an epiphenomenon, or secondary consequence, of immature language and cognitive control processes. In this case, we expect language production issues to cease in adults, even when ADHD persists. This would suggest that problems in language output are not central to ADHD. The second possibility is that language production problems are more directly related to, or part of the core syndrome of ADHD, in which case, production issues should remain apparent in adults who continue to have the disorder.
Language Production in ADHD
Two common methods have been employed to assess language production abilities in children with ADHD. The first is story retelling. In this task, participants hear a story, and they are instructed to listen carefully so that they can repeat it back using their own words. Using this task, Purvis and Tannock (1997) found significant deficits in event sequencing, overall organization, and more misinterpretations in children with ADHD compared with controls. Participants with ADHD also made more ambiguous references (for similar findings, see Oram, Fine, & Tannock, 1999; Shaywitz et al., 1995; Tannock, Purvis & Schachar, 1993). However, other studies using a story retelling task have reported that children with ADHD produce age-appropriate mean length utterances and age-appropriate grammatical errors (Ludlow, Rapoport, Bassich, & Mikkelsen, 1980; Zentall, 1988).
The second method for assessing language production is to collect conversational samples and to analyze them for factors, such as number of interruptions, grammaticality mistakes, disfluencies, and so forth. Studies using this type of task have also produced mixed results. Barkley, Cunningham, and Karlsson (1983) reported similar numbers of utterances and syllables per utterance in ADHD children compared with controls. Redmond (2004), however, reported more and longer disfluencies for ADHD children. Tannock and Schachar (1996) reported that children with ADHD produced more off topic speech and made more interruptions compared with controls. Analyzing conversational samples has one advantage over story retelling, because with story retelling it is difficult to separate comprehension and memory deficits from production deficits (Engelhardt, Nigg, Carr, & Ferreira, 2008; Flory et al., 2006; Martinussen & Tannock, 2006; McInnes, Humphries, Hogg-Johnson, & Tannock, 2003). The tradeoff, of course, is that spontaneous conversation cannot be controlled and structured in the same manner as repeating a story. In summary, most, but not all studies of language production show that (1) the narrative speech of children with ADHD is characterized by disorganization and poor cohesion, and (2) that their conversations are characterized by poor topic maintenance, more interruptions, and a greater tendency to be disfluent.
Language production in adults with ADHD has received significantly less attention than language production in children with ADHD. However, Engelhardt, Ferreira, and Nigg (2009) investigated sentence-level language production in adolescents and adults with ADHD. Their results showed that the ADHD-C subtype was more likely to produce ungrammatical and disfluent utterances compared to control participants (see also Engelhardt, Corley, Nigg, & Ferreira, 2010; Rashid, Morris, & Morris, 2001). These findings suggest that inhibitory control and response suppression failures are persistent in ADHD, and adversely affect sentence formation throughout development. At this point, however, we do not know whether these problems also affect the ability to organize, plan, and execute larger linguistic units, such as discourse.
Discourse Production
To produce an extended description of an object or a procedure, a speaker must make decisions about the order in which the words and phrases should be articulated. Psycholinguists studying language production have investigated the factors that influence a speaker’s tendency to place certain words and phrases before others. Bock and colleagues showed that speakers have a tendency to place more salient and conceptually active concepts (or words) earlier in a sentence (Bock, 1987; Bock & Warren, 1985; Christianson & Ferreira, 2005; Ferreira, 1994; Tomlin, 1983). For example, if the word apple is made prominent for some reason, then speakers are more likely to produce a sentence, such as the apple was eaten by the boy. In this case, the more conceptually active word appears first, despite a strong general preference in speech for active sentences over passives. Compared with lexical ordering within a sentence, the factors affecting how speakers order clauses within a larger discourse have received considerably less empirical attention (cf. Levelt, 1981, 1982).
In many domains of discourse, the decision about how to order sentences is obvious. When describing one’s work history for example, the discourse would likely be organized temporally, beginning with early events and ending with more recent events or vice versa. A second common organizational principle in discourse structure is spatial. When describing a recent visit to the Louvre for example, it makes sense to take a listener on a mental tour. As Levelt (1989) points out, this organizational structure has the dual purpose of (1) allowing the speaker to keep track of what s/he has said, and (2) it makes the layout clearer to the listener. In this case, the listener has an easier time generating an abstract mental representation from a sequential (spatial) description, than if the speaker jumped from location to location with no spatial ordering (although a disorganized speaker might do so anyway).
The Network Task
In the current study, participants were asked to describe simple networks of colored dots (Figure 1), a task that has been used previously in the language production literature but not in individuals with ADHD. Each network consisted of two main branches one to the left and one to the right. Branches differed in length and complexity. We collected two dependent measures. The first was participants’ decision to describe the left or the right branch of the network first. The second was disfluencies, which are commonly thought to reflect various types of planning difficulty within the language production system (Clark & Fox Tree, 2002; Fox Tree, 1995).
Figure 1.
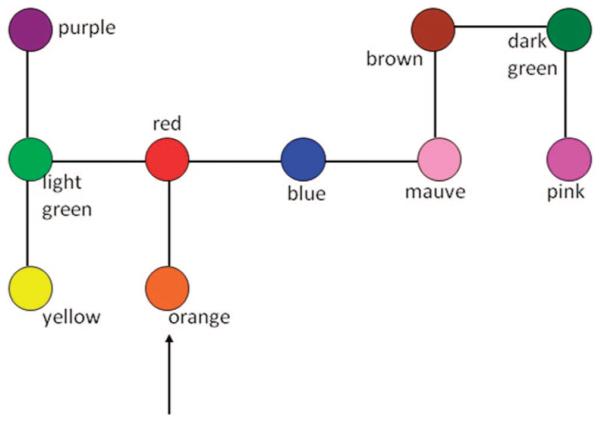
Example stimulus, the left branch has 3 dots and contains one choice point. The right branch contains 5 dots and is linear (i.e., no choice points). Note that the color labels were not presented during the experiment. They are presented here for readers convenience.
In each network, the speaker was required to start at the dot directly above the arrow. After the first dot, the speaker comes to a choice point (i.e., the red dot), and this is the point where the participant must decide whether to describe the left side or the right side first. Branches varied in two dimensions. The first was length. In critical trials, the branch lengths were either three or five dots. The second dimension was complexity, and complexity refers to whether there was a choice point. An example of a choice point is contained in the left branch of Figure 1 (i.e., the light green dot). For the remainder of this article, we will refer to branches as either linear or choice.
Previous studies using this task in nondisordered individuals have reported two main findings (Ferreira & Henderson, 1998; Levelt, 1981, 1982). The first is that shorter branches are described prior to longer branches, and the second is that linear branches are described before choice branches. On the basis of these results, Levelt proposed a Minimal-Load Principle, which assumes that speakers attempt to minimize the memory load they incur as they formulate a description of the network.
The Minimal-Load Principle predicts a preference for shorter branches over longer branches as this reduces the time that a speaker must hold the initial choice point (e.g., the red dot) in memory. The preference for a linear branch over a choice branch is explained using similar logic. If the speaker describes the left branch of Figure 1 first, then not only does the first choice point (the red dot) have to be maintained, but the light green dot will also have to be maintained as the speaker works his or her way through the left branch. Therefore, the memory load is two choice points if the left branch is described first. In contrast, if the right branch is described first, then only one choice point must be held in memory at a time. Previous results show that preferences with regard to planning in discourse production are primarily dependent on memory demands for the speaker (Ferreira & Henderson, 1998).
Current Study
In this study, we examined whether language production difficulties extend to a relatively macro- (or discourse) level of language production in adults with ADHD, in order to determine whether the production problems affecting children with ADHD also affect adults with ADHD. The research question we addressed was whether adults with ADHD show organizational problems in language production when planning and producing an extended multisentence description of a network of colored dots. If they do, then we expect participants with ADHD to rely less on organizational strategies for minimizing memory load, such as the Minimal-Load Principle (Levelt, 1989). We also expect that if ADHD participants have organizational and planning difficulties, then they should also be more disfluent in their descriptions. Based on analyses of naturalistic conversation in nondisordered individuals, it has been estimated that disfluencies occur approximately six times per 100 words, and as mentioned previously, reflect general planning difficulty when speaking (Maclay & Osgood, 1959; Shriberg, 2001).
We also expect differences between the two subtypes of ADHD that are frequent in adults (i.e., ADHD-PI and ADHD-C).1 The ADHD-PI subtype reflects elevated symptoms of inattention but not hyperactivity-impulsivity, whereas the ADHD-C subtype reflects elevated symptoms in both domains. If poorer organization and planning is attributable to inattention, then we expect both subtypes to perform worse than non-ADHD controls. In contrast, if problems in discourse-level language production arise due to a tendency to respond impulsively or to hyperactivity, then we expect the ADHD-C subtype to perform worse than both controls and ADHD-PI. The latter of these possibilities is indirectly supported by the symptoms descriptions in the DSM–IV (American Psychiatric Association, 2000). This is because one third of the symptoms in the hyperactive-impulsive symptom domain are specific to language output (i.e., talks excessively, blurts out answers before questions are completed, and interrupts or intrudes on conversation). Therefore, examining the subtypes separately should provide clues regarding the relationship between the two ADHD symptom domains and the ability to organize and plan a linguistic discourse.
In summary, the goal of this study was to examine discourse production in adults with ADHD. If the problems that affect children also affect adults, then we expect to see less effective planning and more disfluencies. On the other hand, if there are no differences between ADHD participants and typically developing controls, then it would suggest that language production problems do not affect discourse-level language production in adults with ADHD.
Method
Participants
Participants were 75 young adults between the ages of 18 and 35. Table 1 shows the demographic data for the ADHD group and controls. As can be seen in Table 1, the groups differed as expected with regard to the typical clinical profile of ADHD. Table 2 shows the breakdown of the ADHD group by subtype. Participants were recruited from the community via widespread public advertisements designed to access a broad and representative sample. Participants were evaluated in a multistage screening and diagnostic evaluation procedure to identify ADHD cases and controls meeting the study criteria. The procedures were as follows. Prospective participants contacted the project office, at which point key rule-outs were checked (i.e., no sensory-motor handicap, no neurological illness, no nonstimulant psychiatric medications). Eligible participants were then scheduled for an initial diagnostic visit wherein they completed a semistructured clinical interview and assessment of IQ and reading ability (Wechsler, 1997). IQ was estimated using a reliable and valid five subtest short form of the Wechsler Adult Intelligence Scale 3rd edition (Sattler, 2001). The subtests were picture completion, vocabulary, similarities, arithmetic, and matrix reasoning. Reading was assessed with the Wide Range Achievement Test (WRAT; Wilkinson, 1993). After this initial visit, participants were scheduled for a second visit (typically 3– 4 weeks later) where they completed several cognitive tasks, and these tasks were always administered in the same fixed order.
Table 1.
Sample Characteristics for the Two Main Diagnostic Groups
|
M (SD) |
|||
|---|---|---|---|
| Variable | Controls (31) | ADHD (44) | Significance df (73) |
| Age (years) | 24.77 (4.93) | 23.45 (4.50) | t = 1.20, p > .20 |
| Education (years) | 15.39 (1.84) | 13.31 (1.70) | t = 4.90, p < .05 |
| Full-scale IQ | 111.84 (9.77) | 111.79 (12.60) | t = 0.12, p > .90 |
| WRAT reading | 105.68 (6.99) | 100.33 (12.50) | t = 2.13, p < .05 |
| Conners’ (1) | 46.59 (9.23) | 68.19 (7.57) | t = 10.76, p < .05 |
| Conners’ (2) | 44.44 (6.67) | 63.68 (8.27) | t = 10.52, p < .05 |
Note. ADHD = attention-deficit/hyperactivity disorder; WRAT = Wide Range Achievement Text. Conners’ scores are t-scores; (1) is “cognitive problems,” which is closely related to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM–IV) inattentive symptoms; and (2) is hyperactive-impulsive symptoms. Values represent average of informant and self-report.
Table 2.
Sample Characteristics for the Three Attention-Deficit/Hyperactivity Disorder (ADHD) Subtypes
|
M (SD) |
|||
|---|---|---|---|
| Variable | ADHD-PH (6) | ADHD-PI (18) | ADHD-C (20) |
| Age (years) | 25.33 (2.58) | 23.11 (4.71) | 23.20 (4.77) |
| Education | 14.67 (3.08) | 13.21 (1.48) | 12.94 (1.08) |
| Full scale IQ | 109.33 (7.84) | 115.57 (15.66) | 109.79 (11.12) |
| WRAT reading | 104.67 (7.34) | 104.86 (11.30) | 95.63 (13.3) |
| Conners’ (1) | 63.25 (3.88) | 68.12 (7.81) | 69.82 (7.85) |
| Conners’ (2) | 68.29 (6.65) | 59.07 (8.39) | 65.63 (7.32) |
Note. ADHD-PH = primarily hyperactive/impulsive; ADHD-PI = primarily inattentive; ADHD-C = combined. Conners’ scores are t-scores; (1) is “cognitive problems,” which is closely related to Diagnostic and Statistical Manual for Mental Disorders, Fourth Edition (DSM–IV) inattentive symptoms; and (2) is hyperactive-impulsive symptoms. Values represent average of informant and self-report.
For adults, effective assessment of ADHD requires retrospective assessment of their childhood ADHD status to establish childhood onset, in turn, mandating the inclusion of informant interviews to verify symptoms (Wender, Wolf, & Wasserstein, 2001). Thus, in addition to self report, a retrospective Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS; Puig-Antich & Ryan, 1986) along with standardized rating scales were administered to a parent or, in some instances another relative who the participant stated knew them very well throughout their childhood. This interview was conducted by a masters-level clinician with extensive training, following previously published procedures for assessing adults (Biederman, Faraone, Keenan, Knee, & Tsuang, 1990). This procedure assessed the adult’s childhood ADHD, conduct disorder, and oppositional defiant disorder symptoms and impairment by collateral report.
Ongoing adult ADHD symptoms were assessed both by selfreport and by interview with a second collateral informant who the participant stated currently knew them very well (Wender et al., 2001), typically a spouse, roommate, or close friend who either lived with the participant or saw them in many settings. We again used K-SADS ADHD questions worded appropriately for current adult symptoms (Biederman et al., 1990). This interview was supplemented with Barkley and Murphy’s (2006) Current ADHD Symptoms rating scale (as recommended by Weiss, Hechtman, & Weiss, 1999). All informant interviews were conducted by clinically trained interviewers via telephone after appropriate consent procedures.
To ensure that ADHD participants currently exceeded normative cutoffs for ADHD symptoms, adult participants also completed the Conners, Erhardt, and Sparrow (1999) Young Adult ADHD Rating Scale, Achenbach (1991) Young Adult Self Report Scale, and the Brown (1996) Adult ADHD rating scale. Their peer informants completed the Conners et al. (1999) peer rating form, the Barkley and Murphy peer ratings on adult symptoms, a brief screen of antisocial behavior, and drug and alcohol use.
Best estimate diagnosis for ADHD
For all participants, a diagnostic team comprised of a licensed clinical psychologist and a board certified psychiatrist arrived at a “best estimate” diagnosis (Faraone et al., 2000). The same team evaluated all cases. Each member independently reviewed all available information from all self and informant (peer and parent) rating scales and all interview data (including staff notes and observations) to arrive at a clinical judgment about ADHD present or absent, ADHD lifetime and current subtype, and comorbid disorders. All participants in the ADHD group met DSM–IV criteria for ADHD both as children and as adults.
The diagnostic team considered the option of using an “or” algorithm to reach a count of six symptoms, in cases in which there were at least four symptoms from each informant and there was clear evidence of cross-situational impairment. This is similar to what was done in the DSM–IV field trials. Because there is no agreement on age-appropriate cutoffs for adolescents and adults, the team conservatively followed DSM–IV criteria by requiring the six symptoms that DSM–IV specifies, albeit with license to use the “or” algorithm when informants reported additional symptoms. This ensured minimal “false positives” in the ADHD group. False negatives (ADHD cases ending up in the control group) were minimized by requiring four or fewer symptoms of ADHD, no past history of ADHD diagnosis, and rating scale data not in the clinical range for any of the ADHD scales.
The DSM–IV criteria regarding comorbidity were carefully followed, so that although comorbid disorders were diagnosed when present, the participant was excluded from the study if the clinicians agreed that ADHD symptoms were better explained by another disorder (American Psychiatric Association, 1994). This provided some control against obtaining a sample with extreme levels of comorbid disorders while still representing true cases of ADHD. Clinical interviewers rated and noted evidence of impairment (i.e., a rating of at least “moderate” on the K-SADS rating scale), and the diagnostic team required such evidence to make the ADHD diagnosis.
Interclinician agreement on presence or absence of ADHD was satisfactory (k = .80), and agreement on ADHD subtype was also adequate, ranging from k = .74 to .90. Diagnostician reliability for comorbid disorders was excellent (past major depression, k = .96; any current anxiety disorder, k = 0.98; antisocial personality disorder, k = 0.93; substance or alcohol dependence, k = 0.97). Disagreements were handled by conference of the clinicians. It happened that consensus was readily achieved in all cases.
Exclusionary criteria
Potential participants were excluded from all groups if they had a current major depressive or manic/hypomanic episode; current substance dependence preventing sober testing; history of psychosis; history of autism; history of head injury with loss of consciousness greater than 1 minute; sensorymotor handicap; neurological illness; currently prescribed antipsychotic, antidepressant, or anticonvulsant medications. We also ruled out participants with an estimated full scale IQ < 75.
Medication washout
Participants prescribed psychostimulant medications (e.g., Adderall, Ritalin, Concerta, and Focalin) were tested after a minimum of 24 hr (for short acting preparations) and after 48 hr (for long acting preparations). This degree of washout is considered sufficient to minimize medication effects on results. Sixteen percent of the participants with ADHD were on medication prior to washout.
Materials
Twenty-four networks were created for display on the computer. The circles were 1.5 cm in diameter and were connected with 4-cm long lines. For each network, the color of the circles was always unique, that is, no network contained two dots of the same color. The colors used were: light green, dark green, light blue, dark blue, white, black, yellow, red, pink, orange, mauve, brown, and purple. The networks appeared in one of eight conditions, which varied by three factors. The first was the number of dots. One side contained three and the other side contained five. The second was whether the left side was linear or choice. The third was whether the right side was linear or choice.
For each of the eight conditions, three different networks were created (differing in branch configuration and the colors of the circles). The networks were designed so that linear branches contained a bend or two (depending on the length of the figure in order to make them visually similar to the choice branches). Ten filler networks were also created. The fillers were similar to the experimental networks except that the two branches contained an equal number of circles (4), and there were an equal number of linear and choice branches over all of the filler trials. The filler networks were intended to prevent the participants from expecting the same type of network on each trial of the experiment. The 34 (24 experimental and 10 filler) networks were arranged in three random orders, and approximately one third of participants received each order.
Apparatus
Experiments were programmed with E-Prime (Version 1.1) software and were run on a Dell Optiplex GX 400 computer with a 19-in (48.26 cm) monitor.
Procedure
The participants were tested individually in a quiet room. They were shown an example network similar to the fillers, and were told that their task was to describe a number of these types of networks. Participants were asked to describe the networks so that someone else could later draw them based on their descriptions. Participants were asked to refer to the circles by color and to call the circles “dots,” for example, “the yellow dot.” At the beginning of the experiment, the participant saw the instructions on the screen. The instructions indicated that the participant was to begin with the circle immediately above the arrow. Participants were instructed to proceed at their own pace and to speak as if they were in a normal conversation. After reading the instructions, the participant pushed a button to see the colors that would be used in the experiment. This was to familiarize participants with the color labels, which ensures that participants have a readily available term for each color, thereby minimizing the number of disfluencies related to word retrieval.
At this point, the participant was given three practice trials. For each trial, the participant pressed a button to see the network. After the description was completed, the participant pressed a button to clear the screen. Thus, the experiment was participant paced, and there was no set time limit for each trial. Trials were separated with a 2-s intertrial interval. Participants were free to take a break between trials. During the practice, the experimenter monitored the participant’s performance and corrected any deviations from the instructions (e.g., use of an incorrect color term). Participants were then allowed to ask questions. At this point the tape recorder was switched on, and participants completed the 34 experimental trials. Participant responses were transcribed in full by a trained undergraduate research assistant who was naïve with respect to the experimental hypotheses and was also blind to the diagnostic group.
There were two dependent measures. The first was the choice participants made (left vs. right) with respect to the side of the network participants described first. The second was disfluencies, which are commonly thought to reflect planning and/or more general difficulty within the language production system (Barr, 2001; Blackmer & Mitton, 1991; Bortfeld, Leon, Bloom, Schober, & Brennan, 2001; Clark, 1994; Clark & Fox Tree, 2002; Clark & Wasow, 1998; Ferreira & Bailey, 2004; Fox Tree, 1995; Levelt, 1983). We examined four types of disfluency: filled pauses (i.e., um, uh, and er), unfilled (or silent) pauses, repetitions, and repairs. Silent pauses were coded as a disfluency only when they occurred between connected dots, and if they lasted for longer than one second (to rule out ordinary prosodic pauses). If the participant jumped from the end of one branch back to a choice point, then this was not coded as an unfilled pause disfluency. Repetitions refer to unintended repeats of a word or a string of words (e.g., The … the red dot). Repairs occur when a speaker suspends articulation, and then starts over with some new word or phrase (e.g., Go up…go down at the green dot). If a filled pause occurred in the middle of a repetition or repair, then both were coded. However, this was a rare occurrence in our data. The entire experimental session lasted approximately 45 min.
Design
The design was 2 × 2 × 2 × 2 (diagnostic group: ADHD vs. control × number of dots: 3 vs. 5 × left side: linear vs. choice × right side: linear vs. choice). Diagnostic group was between subjects, and the other three variables were within subject. For all critical trials there were 3 dots on one side and 5 on the other. When both branches are linear, participants should be more likely to describe the shorter branch first. When both branches are choice, participants should begin with the shorter of the two branches. In addition, when the 3-dot branch is linear and 5-dot branch is choice, participants should also be more likely to described the short branch first. The key comparison concerns trials in which the 3-dot branch is choice and the 5-dot branch is linear. In this case, because of memory demands, participants should be more likely to describe the longer of the two branches first (Ferreira & Henderson, 1998). If participants with ADHD are less organized when formulating their descriptions, then they should be less likely to show this shift from short-to-long based on the presence of a choice point compared to nondisordered participants.
If a participant described the left branch first, the trial was scored as a 0, and if a participant described the right branch first, the trial was scored as a 1. Therefore, mean values below .5 in each of the eight within subjects conditions represent a bias to initially go left, and values above .5 represent a bias to initially go right. Disfluencies were summed by type (i.e., filled pause, unfilled pause, repetition, and repair), and then divided by the total number of words produced over the course of the experiment.
Results
For the analyses, we begin with a two group analysis comparing ADHD to controls, as this was our main interest. If there was an ADHD main effect, then we proceeded to look at whether subtypes differed (see Footnote 1). For the disfluencies, the data were screened for outliers prior to the analyses. One extreme outlier (4.5 SDs from the group mean) was replaced with the mean for that group in that condition. The proportions (number of disfluencies divided by the total number of words produced) were transformed to rationalized arcsine units prior to the analysis (Studebaker, 1985).2 Table 3 shows the correlations between the demographic variables, symptom cluster scores, and the disfluencies. The ADHD group produced significantly more words overall compared to controls t(73) = −2.33, p < .05, η2 = .07 (ADHD: M = 2137, SD = 1006 and control: M = 1666, SD = 599). The ADHD-PI group was not significantly different from controls ( p > .15), but the ADHD-C group produced marginally more words than did controls t(49) = −1.80, p = .078 (η2 = .06).
Table 3.
Correlations Between Demographic Variables and Dependent Variables
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Age | — | .50** | .06 | −.03 | −.11 | −.24* | −.05 | −.13 | .25* |
| 2. Education | — | .19 | −.33** | −.38** | −.20 | −.22 | .12 | −.20 | |
| 3. IQ | — | .04 | −.05 | −.06 | −.23# | −.01 | −.15 | ||
| 4. Conners’ (1) | — | .78** | .21 | .26* | −.03 | .39** | |||
| 5. Conners’ (2) | — | .28* | .20 | .10 | .29* | ||||
| 6. Repetitions | — | .44** | .34** | .19 | |||||
| 7. Repairs | — | .21 | .44** | ||||||
| 8. Filled pauses | — | .01 | |||||||
| 9. Unfilled pauses | — |
Note. N = 75.
p < .07.
p < .05.
p < .01.
Left Versus Right Decision
The results of a 2 (diagnostic group: ADHD vs. control) × 2 (number of dots: 3 vs. 5) × 2 (left side: linear vs. choice) × 2 (right side: linear vs. choice) mixed-model analysis of variance (ANOVA) showed only one significant main effect, and two significant two-way interactions. However, diagnostic group (ADHD vs. control) did not produce a significant main effect, and it did not interact with any of the other three variables. We have reported the results that were significant in the online supplementary materials for interested readers.
Disfluencies
We began the disfluency analysis by collapsing across the eight within-subject conditions. The proportions of disfluencies produced per word are shown in Figure 2. A two-Group multivariate analysis of variance (MANOVA) using each of the four disfluency types as a dependent variable revealed a significant effect, F(4, 70) = 2.98, p < .05 (η2 = .15). We therefore, followed up this analysis with four uncorrected, independent samples t tests for each of the disfluency types. The results showed two significant differences. Participants with ADHD, compared with controls, were more likely to make unfilled pauses, t(73) = −2.58, p < .05 (η2 = .08), and repetitions, t(73) = −2.28, p < .05 (η2 = .07). There were no differences between groups in the rate of filled pauses or repairs.
Figure 2.

Proportion of disfluencies produced in each of the two diagnostic groups, error bars show the standard error of the mean.
We next investigated subtype differences (ADHD-PI, ADHD-C, and controls) for unfilled pauses and repetitions (Figure 3). We began with a MANOVA to confirm that group effects held when three groups were assigned. The results showed that they did, F(4, 130) = 2.57, p < .05 (η2 = .07). We followed up this analysis with pairwise t tests in order to determine where the significant differences were. For unfilled pauses, the ADHD-PI group was significantly more disfluent than controls, t(48) = −2.64, p < .05 (η2 = .13), whereas the ADHD-C group was marginally more disfluent than controls, t(50) = −1.91, p = .06 (η2 = .07). The two ADHD groups were not different from one another ( p > .30).
Figure 3.

Proportion of disfluencies produced in controls and two subtypes of ADHD, error bars show the standard error of the mean.
For the proportion of repetitions, the pattern between subtypes was similar to unfilled pauses. The ADHD-PI group was significantly more disfluent than controls, t(48) = −2.07, p < .05 (η2 = .08), and the ADHD-C group was marginally more disfluent than controls, t(50) = −1.75, p = .087 (η2 = .06). The two ADHD groups were not different from one another ( p > .70). The subtype results show, consistent with the two group analysis, that participants with ADHD have a greater tendency to make unfilled pauses and repetitions. In both cases, there were significant differences between the inattentive subtype and controls, and marginal differences between the combined subtype and controls.
As a final analysis of the disfluency data, we looked at the number of both repetitions and unfilled pauses in a 2 × 2 × 2 × 2 (diagnostic group: ADHD vs. control × number of dots: 3 vs. 5 × left side: linear vs. choice × right side: linear vs. choice) mixedmodel ANOVA. For repetitions, none of the main effects or interactions were significant for the three within-subjects variables. There was, however, a main effect of diagnostic group, F(1, 73) = 5.72, p < .05 (η2 = .07), with the ADHD group making more repetitions than the control group. The analysis of unfilled pauses also showed a significant main effect of group, F(1, 73) = 12.71, p < .01 (η2 = .15). However, in contrast to repetitions, unfilled pauses revealed a significant three-way interaction between the three within-subjects variables, F(1, 73) = 7.54, p < .01 (η2 = .09). We have elected to report the details of this analysis in the supplementary materials, as they are tangential to main issues of the study (i.e., ADHD status) but may be of interest to specialists in psycholingustics.
Age, IQ, and Reading Ability
The purpose of the following analyses was to ensure that the effects reported above could not be explained by alternate variables. The first variable that we examined was age. It is interesting to note that the correlations in Table 3 reveal that age significantly correlates with both repetitions and unfilled pauses. With unfilled pauses, the correlation is positive, suggesting that as people get older they pause more, and with repetitions, the correlation is negative, suggesting that as people get older they tend to repeat less (for a similar result, see Engelhardt et al., 2010). When we included age as a covariate in the two MANOVAs that tested overall disfluency production, we found that age produced a significant effect in both the two group model (ADHD vs. control: F(4, 69) = 3.37, p < .05, η2 = .16), and the three group model (ADHD-PI, ADHD-C, and control: F(4, 62) = 3.52, p < .05, η2 = .19). However, in both cases, the relationship between diagnostic group and the dependent variables did not change. This suggests that age accounts for significant, yet independent, variance, and that the group effect is robust once age is controlled.
The other two variables that we examined were IQ and reading ability. When IQ was included as a covariate in the two MANOVAs that showed significant group differences, it did not produce a significant effect, and it did not change the pattern of results in any way. Finally, we examined reading ability. Reading ability, similar to IQ, did not produce a significant effect in either of the two models, and it did not affect the results in any way. Therefore, all ADHD effects remain with age, IQ, and reading ability covaried ( p < .05).
Summary
In summary, there was an effect of diagnostic group on disfluencies. Disfluencies occur when the production system encounters difficulty or makes an overt error. We examined disfluencies in this study as a secondary measure of planning and production difficulty over the multiclause network descriptions that were required in this task. With unfilled pauses and repetitions, we found that ADHD participants had a greater tendency to be disfluent compared with controls.
Discussion
In this study, we found that ADHD participants produced significantly more words overall compared with controls. This result coincides with one of the hallmark behavioral symptoms of childhood ADHD, which is excessive talking. There are several studies in the literature, which report that children with ADHD produce more words than are necessary for task demands (e.g., Tannock & Schacher, 1996). In our study, we found that adult ADHD participants produced, on average, 500 more words over the course of the experiment than did control participants. One consequence of these additional words is a lack of efficiency with regard to how long it took to complete the experiment. More specifically, speech rates in the upper midwest of the United States have been estimated at four and a half to five syllables per second in typically developed individuals (Jacewicz, Fox, O’Neill, & Salmons, 2009). If we multiply this out (estimating number of syllables per word), and factoring in disfluency time, we estimate that ADHD participants took 4 to 4.5 min longer to complete the experiment than did control participants. This finding suggests less efficiency in language production, similar to what has been reported in children with ADHD.
The first dependent measure in this study was whether participants chose to describe the left branch or the right branch of a network first. The predictions for this task were based on a general preference in language production to begin with the easy things first (Bock, 1987; Bock & Warren, 1985). This idea is based on an incremental production architecture, and the basic assumption is that the system starts with the easy things first so as to cut down on planning time before actually initiating speech (Bock & Levelt, 1994; Ferreira & Engelhardt, 2006). This then gives the system additional time to deal with more difficult things, and as a result, production and planning can to some extent take place in parallel. We found that participants had a preference to described short branches before long branches. However, our results showed no difference between the ADHD group and controls in the decisions that they made as they worked their way through the networks.
The second dependent measure was disfluencies, and the overall disfluency rate was approximately 1.5 per 100 words, which is somewhat lower than what typically occurs in naturalistic conversation with typically developing individuals (Fox Tree, 1995), perhaps because the social monitoring demands of the present experiment were considerably reduced versus naturalistic speech. In this measure, we observed several novel findings with respect to language production in ADHD. Here the results showed an effect of diagnostic group on both the number of repetitions and unfilled pauses. In both cases, there were significant differences between controls and the ADHD-PI subtype, and there were marginal differences between controls and the ADHD-C subtype.
To our knowledge, this is only the second study to investigate disfluency production in adults with ADHD. Engelhardt et al. (2010) looked at disfluencies in a sentence production task that involved priming. The main findings from that study showed that when participants were primed toward a certain word order, and when that word order conflicted with the verb bias, ADHD-C participants were more likely to produce a repair disfluency. For example, if participants were shown a picture of a girl followed by a picture of a bicycle and had to form a sentence using the verb ridden, then the ADHD-C participants were more likely to produce a repair compared to controls. This is because ridden typically goes with passive sentences (e.g., The bicycle was ridden by the girl.), so in this case, the picture order conflicts with the verb bias. The conclusion drawn on the basis of those data was that an inhibition deficit in ADHD results in an increased tendency to begin speaking (due to priming) without sufficient planning, and therefore, ADHD participants have a greater tendency to suspend articulation midstream and restart with a new word (Gorfein & MacLeod, 2007). In other words, they make an overt error.
The difference in task demands between that study and the current one likely precludes direct comparison. However, there are two interesting differences, which have to be addressed. The first is that we observed larger differences between the ADHD-PI subtype and controls compared to the ADHD-C subtype. This is an interesting and somewhat counterintuitive result because the combined subtype is typically more severe, and typically results in greater impairments. Our results suggest that ADHD-PI participants have greater difficulty managing the demands of this particular task. When we examine our data as a whole, it is not apparent why this might be the case. The demographic variables and Conners’ (1) scores in Table 2 contain only one significant difference between ADHD-PI and ADHD-C, and the ADHD-PI group was significantly *higher* than ADHD-C in reading ability, t(36) = 2.10, p < .05. At this point, it remains an open issue as to why the inattentive subtype would perform (at least) numerically worse than the combined subtype. However, this finding is interesting in terms of Milich, Balentine, and Lynam’s (2001) suggestion that the meaning of inattention symptoms in the ADHD-PI group may be different from the meaning of inattention symptoms in the ADHD-C group. It should also be noted that the general trends in the data suggest that the two ADHD groups patterned more similarly to one another than they do to controls.
The second unique finding in the current study is that we observed differences in unfilled pauses and repetitions, whereas the previous production study (i.e., Engelhardt et al., 2010) showed differences in repairs. We believe that this discrepancy is due to the fact that the previous study utilized a priming paradigm in a direct attempt to address planning processes prior to speaking, and so, it is not at all surprising that there were more repairs. The current study, in contrast, required participants to simply describe a network of dots, and group differences emerged in the number of unfilled pauses and repetitions. With these types of disfluencies, it is difficult to pinpoint the underlying source of difficulty that caused the speaker to be disfluent. However, because we did observe significant differences based on ADHD status and because the two ADHD subtypes patterned more similarly to each other compared to controls, we assume that the underlying nature of these disfluencies is due to lapses in focused attention, rather than to a tendency to respond impulsively.
The aim of this research was to determine whether adults with ADHD have difficulty with discourse-level language production. In the introduction, we outlined two possibilities with respect to adult ADHD status and presence/absence of production difficulties. The first was that language production problems are not directly related to ADHD, in which case, language production issues should cease, even when ADHD persists. The second possibility was that language production problems are part of the core syndrome of ADHD. In this case, language production difficulties should remain in adults who continue to have the disorder. Our results showed no differences in the organizational strategies that ADHD participants used when planning and executing their descriptions. We chose the Network Task because it allowed us to better delineate and isolate production difficulties compared to the story retelling task that has been used in several previous studies of ADHD in children. This is because story retelling requires participants to comprehend and then store the information prior to verbally repeating it back to the experimenter. Story retelling therefore, confounds comprehension, memory, and production processes, which may partially explain why there are discrepant findings in the literature focusing on language production in children with ADHD.
Conclusions
The purpose of this study was to examine discourse-level language production in adults with ADHD to determine whether language production issues persist or attenuate in adulthood. We found that ADHD participants produced more words overall in their descriptions, and we also found several key differences in the rates of disfluency production. Participants diagnosed with ADHD were more likely to make repetition and unfilled pause disfluencies. The increased tendency to produce disfluencies suggests some persistence of language production difficulty in adults with ADHD. These problems were somewhat more clearly linked with problems in behavioral inattention than hyperactivity/impulsivity. These findings indicate that inhibition control problems in language production negatively affect the efficiency and fluency of speech in individuals even into adulthood and thus, throughout development.
Acknowledgments
This research was supported by the National Institute of Mental Health Grant R01-MH63146 awarded to Joel T. Nigg and Fernanda Ferreira. We thank Laurie A. Carr and Elizabeth Davis for their help collecting the data.
Footnotes
Supplemental materials: http://dx.doi.org/10.1037/a0022436.supp
The ADHD-PH subtype was infrequently identified, as expected based on previous literature (Hart, Lahey, Loeber, Applegate, & Frick, 1995; Lahey, Pelham, Loney, Lee, & Willcutt, 2005; Willcutt, Pennington, & DeFries, 2000), and therefore, for the follow up subtype analyses, we exclude this group.
An arc-sine transformation is commonly used when conducting statistical analyses on proportions in order to make distributions more normal. This is especially important when proportions are either very high or very low, the latter of which are common in disfluency studies. The Rationalized Arc-sine Transformation (Studebaker, 1985) is similar to the standard arc-sine transformation, but retains values very close to the original proportion values over most of the range of scores.
Contributor Information
Paul E. Engelhardt, Department of Psychology, Northumbria University, Newcastle upon Tyne, United Kingdom
Fernanda Ferreira, Department of Psychology, University of Edinburgh, Edinburgh, United Kingdom.
Joel T. Nigg, Department of Psychiatry, Oregon Health & Science University, Portland, Oregon
References
- Achenbach T. Manual for the Young Adult Self-Report and Young Adult Behavior Checklist. University of Vermont; Burlington, VT: 1991. [Google Scholar]
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 4th Author; Washington, DC: 1994. [Google Scholar]
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 4th Author; Washington, DC: 2000. [Google Scholar]
- August GJ, Garfinkel BD. Comorbidity of ADHD and reading disability among clinic-referred children. Journal of Abnormal Child Psychology. 1990;18:29–45. doi: 10.1007/BF00919454. [DOI] [PubMed] [Google Scholar]
- Barkley RA. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin. 1997;1:65–94. doi: 10.1037/0033-2909.121.1.65. [DOI] [PubMed] [Google Scholar]
- Barkley RA, Murphy KR. Attention deficit hyperactivity disorder: A clinical workbook. 3rd Guilford Press; New York: 2006. [Google Scholar]
- Barkley RA, Cunningham CE, Karlsson J. The speech of hyperactive children and their mothers: Comparison with normal children and stimulant drug effects. Journal of Learning Disabilities. 1983;16:105–110. doi: 10.1177/002221948301600209. [DOI] [PubMed] [Google Scholar]
- Barkley RA, Fischer M, Smallish L, Fletcher K. The persistence of attention-deficit/hyperactivity disorder into young adulthood as a function of reporting source and definition of disorder. Journal of Abnormal Psychology. 2002;111:279–289. [PubMed] [Google Scholar]
- Barr DJ. Trouble in mind: Paralinguistic indices of effort and uncertainty in communication. In: Cavé C, Guaïtella I, Santi S, editors. Oralité et gestualité: Interactions et comportements multimodaux dans la communication. L’Harmattan; Paris: 2001. pp. 597–600. [Google Scholar]
- Beitchman JH, Young AR. Learning disorders with a special emphasis on reading disorder: A review of the past 10 years. Journal of the American Academy of Child and Adolescent Psychiatry. 1997;36:1020–1032. doi: 10.1097/00004583-199708000-00009. [DOI] [PubMed] [Google Scholar]
- Beitchman JH, Hood J, Inglis A. Psychiatric risk in children with speech and language disorders. Journal of Abnormal Child Psychology. 1990;18:283–296. doi: 10.1007/BF00916566. [DOI] [PubMed] [Google Scholar]
- Biederman J, Faraone SV, Keenan K, Knee D, Tsuang MT. Family-genetic and psychosocial risk factors in DSM–III attention deficit disorder. Journal of the American Academy of Child & Adolescent Psychiatry. 1990;29:526–533. doi: 10.1097/00004583-199007000-00004. [DOI] [PubMed] [Google Scholar]
- Biederman J, Faraone SV, Spencer TJ, Mick E, Monuteaux MC, Aleardi M. Functional impairments in adults with self-reports of diagnosed ADHD: A controlled study of 1001 adults in the community. Journal of Clinical Psychiatry. 2006;67:524–540. doi: 10.4088/jcp.v67n0403. [DOI] [PubMed] [Google Scholar]
- Blackmer ER, Mitton JL. Theories of monitoring and timing of repairs in spontaneous speech. Cognition. 1991;39:173–194. doi: 10.1016/0010-0277(91)90052-6. [DOI] [PubMed] [Google Scholar]
- Bock JK. An effect of the accessibility of word forms on sentence structures. Journal of Memory and Language. 1987;26:119–137. [Google Scholar]
- Bock JK, Levelt WJM. Language production: Grammatical encoding. In: Gernsbacher MA, editor. Handbook of psycholinguistics. Academic Press; San Diego, CA: 1994. pp. 945–984. [Google Scholar]
- Bock JK, Warren RK. Conceptual accessibility and syntactic structure in sentence formulation. Cognition. 1985;21:47–67. doi: 10.1016/0010-0277(85)90023-x. [DOI] [PubMed] [Google Scholar]
- Bortfeld H, Leon SD, Bloom JE, Schober MF, Brennan SE. Disfluency rates in spontaneous speech: Effects of age, relationship, topic, role, and gender. Language and Speech. 2001;44:123–147. doi: 10.1177/00238309010440020101. [DOI] [PubMed] [Google Scholar]
- Brown TE. Brown Attention-Deficit Disorder Scales. Psychological Corporation; San Antonio, TX: 1996. [Google Scholar]
- Cantwell DP. Attention deficit disorder: A review of the past 10 years. Journal of the American Academy of Child & Adolescent Psychiatry. 1996;35:978–987. doi: 10.1097/00004583-199608000-00008. [DOI] [PubMed] [Google Scholar]
- Carr LA, Nigg JT, Henderson JM. Attentional versus motor inhibition in adults with attention deficit hyperactivity disorder. Neuropsychology. 2006;20:430–441. doi: 10.1037/0894-4105.20.4.430. [DOI] [PubMed] [Google Scholar]
- Christianson K, Ferreira F. Conceptual accessibility and sentence production in a free word order language (Odawa) Cognition. 2005;98:105–135. doi: 10.1016/j.cognition.2004.10.006. [DOI] [PubMed] [Google Scholar]
- Clark HH. Managing problems in speaking. Speech Communication. 1994;15:243–250. [Google Scholar]
- Clark HH, Fox Tree JE. Using uh and um in spontaneous speaking. Cognition. 2002;84:73–111. doi: 10.1016/s0010-0277(02)00017-3. [DOI] [PubMed] [Google Scholar]
- Clark HH, Wasow T. Repeating words in spontaneous speech. Cognitive Psychology. 1998;37:201–242. doi: 10.1006/cogp.1998.0693. [DOI] [PubMed] [Google Scholar]
- Cohen NJ, Davine M, Horodezky N, Lipsett L, Isaacson L. Unsuspected language impairment in psychiatrically disturbed children: Prevalence, language, and behavioral characteristics. Journal of the American Academy of Child and Adolescent Psychiatry. 1992;32:595–603. doi: 10.1097/00004583-199305000-00016. [DOI] [PubMed] [Google Scholar]
- Conners CK, Erhardt D, Sparrow E. Adult ADHD Rating Scales: Technical manual. Multi-Health Systems; Toronto, Ontario, Canada: 1999. [Google Scholar]
- Denckla MB. Biological correlates of learning and attention: What is relevant to learning disability and attention-deficit hyperactivity disorder? Developmental and Behavioral Pediatrics. 1996;17:114–119. [PubMed] [Google Scholar]
- Dykman RA, Ackerman PT. ADD and specific reading disability: Separate but often overlapping disorders. Journal of Learning Disabilities. 1991;24:96–103. doi: 10.1177/002221949102400206. [DOI] [PubMed] [Google Scholar]
- Engelhardt PE, Corley M, Nigg JT, Ferreira F. The role of inhibition in the production of disfluencies. Memory & Cognition. 2010;38:617–628. doi: 10.3758/MC.38.5.617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engelhardt PE, Ferreira F, Nigg JT. Priming sentence production in adolescents and adults with attention-deficit/hyperactivity disorder. Journal of Abnormal Child Psychology. 2009;37:916–928. doi: 10.1007/s10802-009-9323-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engelhardt PE, Nigg JT, Carr LA, Ferreira F. Cognitive inhibition and working memory in attention-deficit/hyperactivity disorder. Journal of Abnormal Psychology. 2008;117:591–605. doi: 10.1037/a0012593. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faraone SV, Biederman J, Spencer T, Wilens T, Seidman LJ, Mick E, Doyle AE. Attention-deficit/hyperactivity disorder in adults: An overview. Biological Psychiatry. 2000;48:9–20. doi: 10.1016/s0006-3223(00)00889-1. [DOI] [PubMed] [Google Scholar]
- Ferreira F. Choice of passive voice is affected by verb type and animacy. Journal of Memory and Language. 1994;33:715–736. [Google Scholar]
- Ferreira F, Bailey KGD. Disfluencies and human language comprehension. Trends in Cognitive Science. 2004;8:231–237. doi: 10.1016/j.tics.2004.03.011. [DOI] [PubMed] [Google Scholar]
- Ferreira F, Engelhardt PE. Syntax and Production. In: Traxler M, Gernsbacher MA, editors. Handbook of psycholinguistics. Elsevier Inc; Oxford, United Kingdom: 2006. pp. 61–91. [Google Scholar]
- Ferreira F, Henderson JM. Linearization strategies during language production. Memory & Cognition. 1998;26:88–96. doi: 10.3758/bf03211372. [DOI] [PubMed] [Google Scholar]
- Flory K, Milich R, Lorch EP, Hayden AN, Strange C, Welsch R. Online story comprehension among children with ADHD: Which core deficits are involved? Journal of Abnormal Child Psychology. 2006;34:853–865. doi: 10.1007/s10802-006-9070-7. [DOI] [PubMed] [Google Scholar]
- Fox Tree JE. The effects of false starts and repetitions on the processing of subsequent words in spontaneous speech. Journal of Memory and Language. 1995;34:709–738. [Google Scholar]
- Giedd JN, Blumenthal J, Jefferies NO, Castellanos FX, Lui H, Zijdenbos A, et al. Brain development during childhood and adolescents: A longitudinal MRI study. Nature Neuroscience. 1999;2:861–863. doi: 10.1038/13158. [DOI] [PubMed] [Google Scholar]
- Gorfein DS, MacLeod CM. Inhibition in cognition. American Psychological Association; Washington, DC: 2007. [Google Scholar]
- Hart EL, Lahey BB, Loeber R, Applegate B, Frick PJ. Developmental change in attention-deficit hyperactivity disorder in boys: A four-year longitudinal study. Journal of Abnormal Child Psychology. 1995;23:729–749. doi: 10.1007/BF01447474. [DOI] [PubMed] [Google Scholar]
- Hinshaw SP. Academic underachievement, attention deficits, and aggression: Comorbidity and implications for intervention. Journal of Consulting and Clinical Psychology. 1992;60:893–903. doi: 10.1037//0022-006x.60.6.893. [DOI] [PubMed] [Google Scholar]
- Jacewicz E, Fox RA, O’Neill C, Salmons J. Articulation rate across dialect, age, and gender. Language Variation and Change. 2009;21:233–256. doi: 10.1017/S0954394509990093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson JR, Miller JF, Curtiss S, Tallal P. Conversations with children who are language impaired: Asking questions. Journal of Speech and Hearing Research. 1993;36:973–978. doi: 10.1044/jshr.3605.973. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Adler L, Barkley R, Biederman J, Conners CK, Demler O. The prevalence and correlates of adult ADHD in the United States: Results from the National Comorbidity Survey Replication. American Journal of Psychiatry. 2006;163:716–723. doi: 10.1176/appi.ajp.163.4.716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, Pelham WE, Loney J, Lee SS, Willcutt EG. Instability of the DSM–IV subtypes of ADHD from preschool through elementary school. Archives of General Psychiatry. 2005;62:896–902. doi: 10.1001/archpsyc.62.8.896. [DOI] [PubMed] [Google Scholar]
- Levelt WJM. The speaker’s linearization problem. Philosophical Transactions of the Royal Society of London: Series B. 1981;295:305–315. [Google Scholar]
- Levelt WJM. Linearization in describing spatial networks. In: Peters S, Saarinen E, editors. Processes, beliefs, and questions. D. Reidel; Dordrecht: 1982. pp. 199–220. [Google Scholar]
- Levelt WJM. Monitoring and self-repair in speech. Cognition. 1983;14:41–104. doi: 10.1016/0010-0277(83)90026-4. [DOI] [PubMed] [Google Scholar]
- Levelt WJM. Speaking: From intention to articulation. MIT; Cambridge, MA: 1989. [Google Scholar]
- Ludlow C, Rapoport J, Bassich C, Mikkelsen E. Differential effects of dextroamphetamine on language performance in hyperactive and normal boys. In: Knights R, Bakker D, editors. Treatment of hyperactive and learning disordered children. University Park Press; Baltimore: 1980. pp. 185–205. [Google Scholar]
- Maclay H, Osgood CE. Hesitation phenomenon in spontaneous English speech. Word. 1959;15:19–44. [Google Scholar]
- Mapou RL. Adult learning disabilities and ADHD: Research-informed assessment. Oxford University Press; New York: 2009. [Google Scholar]
- Martinussen R, Tannock R. Working memory impairments in children with attention-deficit hyperactivity disorder with and without comorbid language learning disorders. Journal of Clinical and Experimental Neuropsychology. 2006;28:1073–1094. doi: 10.1080/13803390500205700. [DOI] [PubMed] [Google Scholar]
- McInnes A, Humphries T, Hogg-Johnson S, Tannock R. Listening comprehension and working memory are impaired in attention-deficit hyperactivity disorder irrespective of language impairment. Journal of Abnormal Child Psychology. 2003;31:427–443. doi: 10.1023/a:1023895602957. [DOI] [PubMed] [Google Scholar]
- Milich R, Balentine AC, Lynam DR. ADHD combined type and ADHD predominantly inattentive type are distinct and unrelated disorders. Clinical Psychology: Science and Practice. 2001;8:463–488. [Google Scholar]
- Nigg JT. Is ADHD a disinhibition disorder? Psychological Bulletin. 2001;127:571–598. doi: 10.1037/0033-2909.127.5.571. [DOI] [PubMed] [Google Scholar]
- Nigg JT. What causes ADHD? Understanding what goes wrong and why. Guilford Press; New York: 2006. [Google Scholar]
- Nigg JT, Hinshaw SP, Carte ET, Treuting JJ. Neuropsychological correlates of childhood attention-deficit/hyperactivity disorder: Explainable by comorbid disruptive behavior or reading problems? Journal of Abnormal Psychology. 1998;107:468–480. doi: 10.1037/0021-843X.107.3.468. [DOI] [PubMed] [Google Scholar]
- Oram J, Fine J, Tannock R. Assessing the language of children with attention deficit hyperactivity disorder. American Journal of Speech-Language Pathology and Audiology. 1999;8:72–80. [Google Scholar]
- Puig-Antich J, Ryan N. Western Psychiatric Institute and Clinic; Pittsburg, PA: 1986. The Schedule for Affective Disorders and Schizophrenia for School-Age Children (Kiddie-SADS)—1986. [Google Scholar]
- Purvis K, Tannock R. Language abilities in children with attention deficit hyperactivity disorder, reading disabilities, and normal controls. Journal of Abnormal Child Psychology. 1997;25:133–144. doi: 10.1023/a:1025731529006. [DOI] [PubMed] [Google Scholar]
- Rashid FL, Morris MK, Morris R. Naming and verbal memory skills in adults with attention deficit hyperactivity disorder and reading disability. Journal of Clinical Psychology. 2001;57:829–838. doi: 10.1002/jclp.1052. [DOI] [PubMed] [Google Scholar]
- Redmond SM. Conversational profiles of children with ADHD, SLI, and typical development. Clinical Linguistics & Phonetics. 2004;18:107–125. doi: 10.1080/02699200310001611612. [DOI] [PubMed] [Google Scholar]
- Sattler JM. Assessment of children: Cognitive applications. 4th Author; San Diego, CA: 2001. [Google Scholar]
- Schachar R, Tannock R, Marriott M, Logan GD. Deficient inhibitory control and attention deficit hyperactivity disorder. Journal of Abnormal Child Psychology. 1995;23:411–437. doi: 10.1007/BF01447206. [DOI] [PubMed] [Google Scholar]
- Scott CM, Windsor J. General language performance measures in spoken and written narrative and expository discourse of school-aged children with language learning disabilities. Journal of Speech, Language, and Hearing Research. 2000;43:324–339. doi: 10.1044/jslhr.4302.324. [DOI] [PubMed] [Google Scholar]
- Shaywitz BA, Fletcher JM, Holahan JM, Shneider AE, Marchione KE, Stuebing KK. Interrelationships between reading disability and attention-deficit/hyperactivity disorder. Child Neuropsychology. 1995;1:170–186. [Google Scholar]
- Shriberg E. To “errrr” is human: Ecology and acoustics of speech disfluencies. Journal of the International Phonetic Association. 2001;31:153–169. [Google Scholar]
- Studebaker GA. A “rationalized” arcsine transform. Journal of Speech and Hearing Research. 1985;28:455–462. doi: 10.1044/jshr.2803.455. [DOI] [PubMed] [Google Scholar]
- Tannock R, Schachar R. Executive dysfunction as an underlying mechanism of behavior and language problems in attention deficit hyperactivity disorder. In: Beitchman J, Cohen N, Konstantearas MM, Tannock R, editors. Language, learning, and behavior disorders. University Press; Cambridge: 1996. pp. 128–155. [Google Scholar]
- Tannock R, Purvis K, Schachar R. Narrative abilities in children with attention deficit hyperactivity disorder and normal peers. Journal of Abnormal Child Psychology. 1993;21:103–117. doi: 10.1007/BF00910492. [DOI] [PubMed] [Google Scholar]
- Tirosh E, Cohen A. Language deficit with attention-deficit disorder: A prevalent comorbidity. Journal of Child Neurology. 1998;13:493–497. doi: 10.1177/088307389801301005. [DOI] [PubMed] [Google Scholar]
- Tomlin RS. On the interaction of syntactic subject, thematic information, and agent in English. Journal of Pragmatics. 1983;7:411–432. [Google Scholar]
- Wechsler D. Wecshler Adult Intelligence Scale. 3rd The Psychological Corporation; San Antonio, TX: 1997. [Google Scholar]
- Weiss M, Hechtman LT, Weiss G. ADHD in adulthood: A guide to current theory, diagnosis, and treatment. Johns Hopkins University Press; Baltimore: 1999. [Google Scholar]
- Wender PH, Wolf LE, Wasserstein J. Adults with ADHD: An overview. In: Wasserstein J, Wolf LE, LeFever FF, editors. Annals of the New York Academy of Sciences. Vol. 931. New York Academy of Sciences; New York: 2001. pp. 1–16. [PubMed] [Google Scholar]
- Wilkinson GS. The Wide Range Achievement Test administration manual. Wide Range; Wilmington, DE: 1993. [Google Scholar]
- Willcutt EG, Pennington BF. Comorbidity of reading disability and attention-deficit/hyperactivity disorder: Differences by gender and subtype. Journal of Learning Disabilities. 2000;33:179–191. doi: 10.1177/002221940003300206. [DOI] [PubMed] [Google Scholar]
- Willcutt EG, Pennington BF, DeFries JC. Etiology of inattention and hyperactivity/impulsivity in a community sample of twins with learning difficulties. Journal of Abnormal Child Psychology. 2000;28:149–159. doi: 10.1023/a:1005170730653. [DOI] [PubMed] [Google Scholar]
- Willcutt EG, Pennington BF, Boada R, Ogline JS, Tunick RA, Chabildas NA, Olson RK. A comparison of the cognitive deficits in reading disability and attention-deficit/hyperactivity disorder. Journal of Abnormal Child Psychology. 2001;110:157–172. doi: 10.1037//0021-843x.110.1.157. [DOI] [PubMed] [Google Scholar]
- Zentall SS. Production deficiencies in elicited language but not in the spontaneous verbalizations of hyperactive children. Journal of Abnormal Child Psychology. 1988;16:657–673. doi: 10.1007/BF00913476. [DOI] [PubMed] [Google Scholar]