

Abstract
Background
Hospitals are currently admitting an increasing number of older people, and more than one-third could have an underlying mental health problem. The existing Older Adult Mental Health (OAMH) liaison service was increasingly unable to meet the escalating needs of older and frail patients. Therefore, the service was modernized and enhanced on an “invest-to-save” principle to provide a prompt holistic assessment for older adults with mental health problems. The objective of this study was a service evaluation to appraise clinical outcome, minimize the length of stay, and measure the predictors of adverse outcomes to streamline this enhanced service.
Materials and methods
Patient demographics, social care needs, comorbidity burden (Charlson comorbidity index, CCI), and functional status (Barthel index, BI) were recorded from November 2014 to February 2015. Frailty status (frailty index, FI) was measured by an index (Rockwood index) of accumulated deficits. The outcomes were compared with the previous OAMH liaison service data over the same period a year earlier.
Results
The new Rapid Assessment Interface and Discharge service assessed 339 patients compared to 179 by the previous liaison team over the 4-month period. Mean age was 82.18±8.04 years, with 60% women; preadmission BI was 14.96±4.35, and admission BI was 11.38±5.73 (P<0.001, paired t-test); mean CCI was 1.66±1.53, and mean FI was 0.34±0.99, and 80% were on polypharmacy. The direct discharges from front door were increased by 7%. The mean hospital stay reduced from 35 to 20 days in acute site and from 108 to 47 days in long-stay wards. The cost benefits were based on the mean reduction in hospital stay (41.8 days) and admission reduction (2.2 days), leading to a total annualized bed savings of 44 days. FI was the most highly significant factor between patient groups with a good and poor outcome (P=0.00003, independent groups t-test, t=−4.38, df 98).
Conclusion
Prompt mental health assessments for acutely unwell frail older people are not only cost effective but also improve clinical outcomes.
Keywords: older people, frailty index, mental health, mortality, critical illness, hospitals
Introduction
The population of the UK is aging, with the fastest increase in the oldest old, particularly centenarians. Currently, three million people are over the age of 80 years, and around half a million people are aged 90 years and over (0.8% of the total population).1 By 2031, a 77% increase is expected in the number of those aged 75 years and over and a 131% increase in those aged 85 years and over.2 These demographic changes have influenced the structure of social and health services for older people. In Wales, compared to other countries in the UK, there is an increased demand for services for the oldest old where frailty, dementia, and the effects of multiple chronic conditions are more prevalent.3
The prevalence of mental health and psychological problems in older people is higher in the general hospital as compared to the community. Forty percent of patients older than 70 years with acute medical admissions have dementia, but only half of these patients have been diagnosed.4 Patients with dementia have poorer health outcomes, longer hospital stays, and higher rates of readmissions and institutionalization.4–6 Two-thirds of patients admitted to any district general hospital are aged more than 65 years,4 and two-thirds of whom could have an underlying mental health need due to dementia, depression, or delirium.7,8 Additional mental health illnesses are associated with poorer clinical outcomes.9–11 Key reasons for poor outcome are delayed or under-recognition of the mental health problem or inadequate treatment by the medical staff.11–15
There are several consultant-led psychiatric liaison service models in European countries which mainly deliver comprehensive emergency psychiatric services.16 Such models could be slow in response due to lack of capacity, thus becoming essentially a reactive model of care. Systematic reviews favor the liaison model being more effective at improving clinical outcomes in older people compared to the consultant-led model but fail to identify strong evidence to guide service provision.17–19 There is little evidence to support that psychiatric liaison models for acute older people admitted to hospitals during normal working hours (9 am to 5 pm) are cost effective and beneficial.18,20,21 Therefore, the primary objective of this study was to evaluate the proposed enhanced mental health liaison service model during working hours and describe clinical outcomes comprehensively. The secondary objective of the study was to compare the various factors in predicting adverse outcomes for patients. The rationale was based on prudent health care principles to care for those with the greatest health needs first, making the most effective use of all skills and resources.
Materials and methods
Study design
This was a service evaluation using a prospective observational cohort study of patients admitted acutely to Royal Gwent Hospital (RGH), Newport, within Aneurin Bevan University Health Board (ABUHB) between November 2014 and February 2015. However, patients admitted over the same 4-month period a year before (November 2013 to February 2014) were studied retrospectively to measure the impact of the enhanced service.
Setting
The existing nurse-led Older Adult Mental Health (OAMH) psychiatric liaison service was a 2.4 whole-time equivalent (WTE) nurse-led psychiatric liaison service and was not only insufficient to meet the rising need but also working in a reactive rather than proactive manner. The existing service was expanded to provide an enhanced multidisciplinary input by increasing nurse provision, and introducing therapists, social worker input, and a dedicated old age psychiatry consultant on weekdays between 9 am and 5 pm. The funding for £250,000 was granted by the Welsh Assembly Intermediate Care Fund on an “invest-to-save” basis.
The funding was used to pay clinical and administrative staff over a period of 4 months. The new team included a WTE team lead (Band 7), 4 WTE liaison nurses (2 Band 7, 2 Band 6), 1 WTE occupational therapist (Band 6), 1 WTE social worker (Band 6), 2 WTE secretaries (team and project – Band 4), and 1 WTE project manager (Band 7). The medical support was provided by 0.5 WTE consultant psychiatrist and 0.2 WTE old age psychiatry registrar. In addition, a consultant geriatrician (0.1 WTE) was part of the Rapid Assessment Interface and Discharge (RAID) team to lead the service evaluation.
The objective of the new enhanced service was to improve the mental health care of older people admitted to all the departments (acute, medical, surgical, and trauma wards) of a 750-bedded general hospital. The key principle was to see the patients promptly with a target response rate of 4 hours of receiving a referral for patients admitted to acute services and within 24 hours for the general medical and surgical ward referrals. All patients referred received multidisciplinary input during their hospital stay, and active follow-up was arranged with the community psychiatry teams if needed.
The included patients were those above 65 years who had mental health issues or cognitive problems at the time of their admission and those under 65 years with cognitive problems not caused by delirium or acute intoxication. The new service was available to all relevant patients admitted to the RGH but could not be offered in other ABUHB district general hospitals because of finite resources.
It is essential when introducing service developments in the National Health Service (NHS) to undertake robust service evaluation to ensure effective implementation of the new services and to demonstrate the improvements achieved.
Measurements
Detailed comprehensive data were recorded to describe the population studied between November 2014 and February 2015. This included patient demographics and social care needs. The medical comorbidity burden was measured using Charlson comorbidity index (CCI).22 In this study, 17 modified categories were used in an electronic application to generate the CCI scores.23 A new International Classification of Diseases, Tenth Revision, version of the CCI was used to predicted in-hospital mortality.23 The higher the score, the more likely the predicted outcome, which showed a strong association between increasing index scores and mortality. A score of zero indicated that no comorbidities were found.23 The performance status of ten basic items of activities of daily living was measured using the Barthel index (BI) before admission to hospital and on admission to hospital.24 A higher score is associated with a greater likelihood of being able to live independently. A modified version of the BI has been introduced.25 The modified scale gives a maximum score of 20. The BI has demonstrated high inter-rater reliability (0.95) and test–retest reliability (0.89).26 BI has also shown high correlations (0.74–0.8) with other measures of physical disability.26 Frailty status (frailty index, FI) was measured by an index (Rockwood) of accumulated deficits.27,28 The mean FI is expressed as a ratio, giving a potential score from 0 (no deficits) to 1.0 (all 40 deficits). The value of 0.25 or above indicates that the person involved is approaching a “frail” state, and the maximum value for institutionalized or palliative patients is 0.67.29–31 The outcomes were compared with the previous OAMH liaison service data over the same period in 2014 (November 2013 to February 2014).
Data and statistical analyses
The performance of the service was recorded based on the referral rates and response timings. The clinical outcomes including discharge destination, the length of stay (LoS), and mortality were recorded. Twenty-eight days readmission rates and inpatient mortality rates were determined for all patients. Mortality data of all patients for 6 months were also collected following completion of recruitment. The outcomes were also compared retrospectively with the previous OAMH liaison service data over the same period in the previous year (November 2013 to February 2014).
The primary working clinical diagnosis made by the RAID team was considered for sub-analysis. The outcomes were arbitrarily defined as following three categories to evaluate predictors of adverse outcomes.32
Good outcome: discharged to original residence within 28 days.
Intermediate outcome: discharged to the original residence but the LoS was more than 28 days.
Poor outcome: new care home placement or inpatient mortality.
The description of the study cohort was completed, and data were presented as mean ± standard deviation. The level of statistical significance at which the null hypothesis was rejected was chosen as 0.05. All statistical analyses were conducted using Statistica version 9.1 (StatSoft, Inc., Tulsa, OK, USA). The correlation was used to examine the linear association between continuous two variables and Spearman’s correlation to assess monotonic relationship (whether linear or not) in nonparametric variables. Analysis of variance (ANOVA) was used to analyze differences among groups. The Tukey honest significant difference (HSD) test was used post hoc to enumerate differences between groups. The estimated cost savings were based on the analysis of administrative data on patient admissions and discharge.
Ethics
Ethical approval was not required for this service evaluation as this work does not constitute a research study according to the Health Research Authority decision tool; however, all questions and forms required to carry out the study were sent to the research and development (R&D) – ABUHB, Wales, to assess risks to patient identification and the health board. The study was approved by the R&D of ABUHB, Wales. The patient written informed consent is deemed not required by the ABUHB as patients’ service evaluation were not directly interviewed and no identifiable patient data were recorded.
Results
The RAID team assessed 339 older adults (mean age 82.12±8.04 years; median 83.09 years, range 55–101, 60% females) over a 4-month period. Seventy-eight percent (263/339) were seen and assessed, and only 20% (68/339) were considered inappropriate referrals. Eight patients (2%) required re-referral following discharge from RAID service due to either relapse or new mental health need. The average number of referrals assessed was 16 per week. In comparison, 179 patients were assessed before introducing RAID over a similar period, a year before, suggesting 47% increased assessment rate.
The details of referrals and timings of assessments were recorded on 251 forms. One hundred percent referrals from accident and emergency unit, medical assessment unit, and surgical assessment unit were assessed within 4 hours, and 93% ward referrals were assessed within the target time of 24 hours. Sixty-seven percent (167/251) of total referrals were assessed within 4 hours. In addition to the improved response rate from RAID service, patient’s mental health needs were acknowledged by non-psychiatric teams on admission, and 31% (105/339) of patients were referred to RAID within 24 hours. The previous limited liaison team had only 10% patients referred within 24 hours.
The most common primary mental health diagnosis was dementia followed by delirium (Table 1). The mean BI while in the hospital (11.38±5.73) was significantly lower as compared to the mean preadmission BI of 14.96±4.35 (P<0.001, paired t-test, t=9.35, df 145, n=146). The mean CCI was 1.66±1.53, and the mean FI was 0.34±0.99 (range 0.11–0.58). The majority (80%) were on polypharmacy including antipsychotics (15%), antidepressants (36%), and benzodiazepines (7%).
Table 1.
Details of the primary mental health diagnoses
| Diagnosis on admission | n (%) |
|---|---|
| Dementia | 82 (36) |
| Delirium | 74 (33) |
| Depression | 41 (18) |
| Acute or chronic confusion | 18 (8) |
| Anxiety | 6 (3) |
| Psychosis | 3 (1) |
| Other mood disorders | 2 (1) |
Eighty-seven percent (215/246) of patients were admitted from the community including their homes (houses, bungalows, or flats), 11% (26/246) were admitted from residential-type care homes, and 2% were admitted from nursing homes. Forty-nine percent of patients were discharged home, 14% of patients required nursing home, and 10% required a residential home. Four percent were still in hospital at the time of data analysis. Twenty-three percent (55 patients) died in the hospital. The 30-day and 6-month post-discharge mortality rates were 2% and 5%, respectively. The overall 6-month mortality rate was 28%.
The mean LoS for RAID-assessed patients on the acute site (RGH) was 21.54±19.77 days; overall LoS for the health board was 33.99±34.92 days. The mean LoS for liaison-assessed patients on the acute site before introducing RAID was 35 days, and LoS for patients in long-stay wards was 108 days (standard deviations unavailable – data provided by the previous service). Annual bed days savings were calculated based on the reduction of LoS. The benefits were only calculated based on the bed days saved from the reduction in the LoS and admission avoidance. These analyses were completed by the Assistant Director of Planning, and the annualized bed savings were calculated as 44 days.
The sub-analysis was done for 225 patients to evaluate the predictors of the adverse outcome. We excluded 114 patients for sub-analysis for the following reasons: present in the hospital at the time of the analysis, some form of data was missing, and discharged to temporary accommodation or transferred to another hospital.
Category 1: 42% (n=94/225) of patients were discharged to their original residence within 28 days – good clinical outcome category.
Category 2: 17% (n=39/225) of patients were discharged to their original residence after staying in the hospital for more than 28 days – intermediate clinical outcome category.
Category 3: 16% (n=36/225) of patients were discharged to new care homes, and 24% (n=55/225) died as inpatients (totally 40%) (91/225) – poor outcome.
Age was not a significant predictor of good or poor outcome (ANOVA, P=0.40, F=0.925, df 2). Similarly, gender, the original place of residence, and final diagnosis did not show any statistically significant association with outcome predictors. Polypharmacy showed a weak correlation in predicting the outcome.
The mean CCI was significantly higher for patients in the intermediate (2.1±1.7) and poor (2.0±1.7, ANOVA, P=0.001, F=6.75, df 2) outcome categories as compared to those with a good outcome (1.2±1.2). CCI was a significant predictor of a good outcome (P=0.003) but could not predict an intermediate or a poor outcome (Tukey HSD test: good:intermediate groups, P=0.02; good:poor groups, P=0.002; intermediate:poor groups, P=0.98). This is illustrated in the Box and Whisker plot in Figure 1. The mean preadmission BI for patients in good, intermediate, and poor outcome categories was 16.7±3.6, 13.4±4.9, and 14.4±3.9, respectively. Preadmission level of independence was also a significant predictor of a good outcome as compared to an intermediate and a poor outcome (ANOVA, P=0.005, F=5.6, df 2) (Tukey HSD: good:intermediate groups, P=0.011; good:poor groups, P=0.019) (Figure 2).
Figure 1.
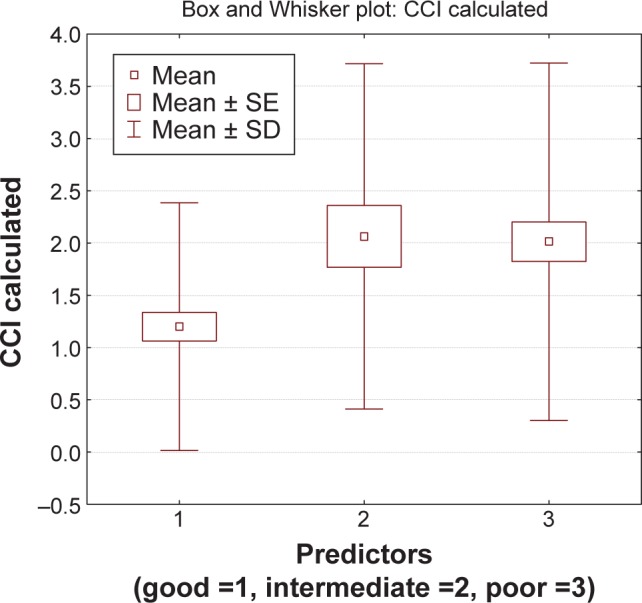
Box and Whisker plot between good (1), intermediate (2), and poor (3) outcome predictors and CCI on admission.
Abbreviations: CCI, Charlson comorbidity index; SE, standard error; SD, standard deviation.
Figure 2.
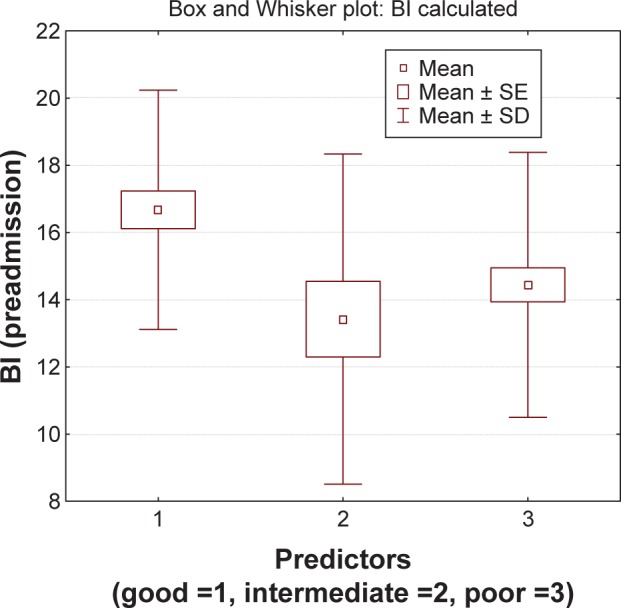
Box and Whisker plot between good (1), intermediate (2), and poor (3) outcome predictors and preadmission BI.
Abbreviations: BI, Barthel index; SE, standard error; SD, standard deviation.
The mean FI for patients with good, intermediate, and poor outcomes was 0.288±0.1, 0.373±0.1, and 0.378±0.1, respectively. FI was the most highly significant factor between patient groups with a good and poor outcome (P=0.00003, independent groups t-test, t=−4.38, df 98). FI was also significantly different between groups with a good and an intermediate outcome (independent groups t-test, P=0.0016, t=3.31, df 58). However, FI was not significantly different between groups with an intermediate or a poor outcome (independent groups t-test, P=0.834, t=−0.21, df 80). A Lowess smoothing curve demonstrates the relationship between the FI and outcome predictors (Figure 3). The FI values at the two ends of the curve represent the better association. No subjects from poor outcome predictor had an FI below 0.25.
Figure 3.
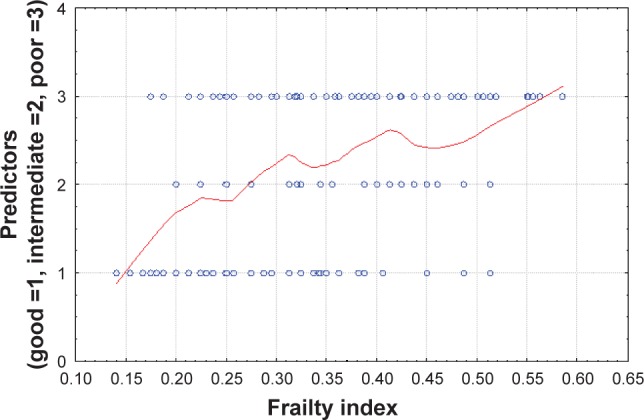
Lowess smoothing plot of predictors of clinical outcomes according to FI.
Abbreviation: FI, frailty index.
Discussion
The NHS is the publicly funded health care system for the UK over the last 65 years. It is the largest and the oldest single-payer health care system in the world, helping the people recover from acute illness and live an independent life. The NHS is facing demographic changes due to an aging population and higher number of people with long-term conditions, resulting in huge economic challenges to deliver safe and high-quality services. The way forward is the most effective use of available resources, putting a greater emphasis on keeping people healthy, particularly those with both physical and mental health illnesses. There is a need to introduce high-quality enhanced services employing new ways of working collectively to improve productivity and value for money spent. This will possibly minimize the threat to the financial stability and sustainability of the NHS.
The modern psychiatric liaison service in the UK is defined as the subspecialty that provides mental health care to patients being admitted to general hospitals, aiming to bridge the gap between physical and mental services.13 According to the most recent evidence based on all ages, the 24-hour multidisciplinary psychiatric liaison team model is not only cost effective by reduced LoS and reduced readmission but also improves patient care.33 The greatest benefit was for older people with dementia, and a very positive impact on discharge to original place of residence was noted.33,34 Therefore, rapid response and the comprehensive psychiatric team integrated into an acute hospital can lead to significant savings. There is existing evidence that appropriate multidisciplinary treatment and prevention of delirium improved perioperative outcomes.35–39 The “Who cares wins” report from the Royal College of Psychiatrists concluded that
There is evidence to suggest that preventative interventions can improve clinical outcome particularly in the incidence of delirium, which carries a poor prognosis.4
Comorbid mental disorders affecting older people in general hospitals are amenable to prevention and treatment. In this study, we have observed this in terms of reduced LoS, better recovery, more successful rehabilitation, and less transfer to institutional care, leading to an overall annualized bed savings of 44 days. This study highlights that improved outcomes can be achieved in routine clinical practice by an enhanced partnership with acute front door teams and psychiatric liaison services. There are several liaison service models to provide comprehensive mental health assessment to patients above the age of 16 years. Considering aging population and financial constraints, service models need to be modified to meet the needs of the local population. Newport RAID model was adapted from a 24 hours a day, seven days a week, Birmingham RAID model.33 The enhanced Newport RAID service has been shown to meet escalating needs of the acutely unwell older people and has shown improved outcomes during working hours, 9 am to 5 pm, Monday to Friday.
In this study, in spite of the rate of the referrals to the new service doubling, all acute admissions were assessed within 4 hours to meet the challenging mental health needs of the older patients, and a clear care plan was agreed. The timeliness of the referral rate was also increased by the non-psychiatry team by 67%. This is likely to be related to both an increase in the awareness of the non-psychiatry staff of concurrent mental health problems and the daily presence of the RAID team in the front door wards which affords informal education across the specialties. A low admission BI, an intermediate FI (0.34), and a high inpatient mortality rate (23%) support the fact that the rise in the referral rate did not represent reduced complexity of the patients included in the study. The patient’s cohort studied represented a predominance of dementia, delirium, and depression as expected (95%).
Given the clinical burden, it can be challenging for the liaison service to take the ownership and provide appropriate care to all the acutely unwell patients. Considering multiple comorbidities and associated mental health problem, prognosis could be guarded in few patients. In this study, we have observed 23% inpatient mortality rate, and the overall 6-month mortality rate was 28%. Patients with high FI had poor outcomes. FI should not be justified for therapeutic nihilism or restrict mental health team input. The FI is not intended to replace clinical judgment and expertise. The accurate risk stratification remains difficult in older frail patients. However, if medical and psychiatry teams can predict poor prognosis on the basis of clinical experience, other interventions such as optimization of nutrition, medication review, pain control, good nursing care, communication and education of carers, and tailored exercise programs could be more appropriate. This could not only avoid “refer-on approach” but also result in effective use of the liaison service staff time.
Our study has numerous strengths. We achieved complete follow-up of inpatient outcomes and mortality up to 6 months after enrollment. The study population was well defined using a comprehensive and standard battery of tests including BI, comorbidity, drug burden, and FI to increase generalizability of the study. The funding was solely granted to develop an enhanced psychiatric liaison service. However, effective team working between service providers, service evaluation staff, and research and development team resulted in comprehensive service evaluation, which was properly completed and explored various predictors of adverse outcomes to augment clinical decisions. As a result, Welsh Government has approved £4.05 million annual funding for all the other health boards across Wales to provide similar services, including £761,000 for ABUHB.
Our study has several limitations. Although this is a non-randomized prospective study based on existing data, a comparison was done retrospectively, and detailed data were not available to compare all the variables. We acknowledge that this results in reduced ability to allow for all relevant differences or biases in the comparison, particularly those associated with the passage of time. We did not measure post-discharge functional status, impact on quality of life, and patient/carer satisfaction as part of this study. We also acknowledge that other confounding variables, including differences in the characteristics of individual patients, differences in wider contextual or environmental variables, the severity of acute illness, an impact of hospitalization like infection, and inpatient falls, were not studied. This study was done during winter months, and usually, a higher number of patients with complex care needs are admitted to the hospital. We have not studied if any other measures like extra nursing support were employed by the health board during the study period. We also did not measure the impact of new community services like reablement teams or community resource teams that could have been introduced at the same time which may have resulted in observed improved outcomes. A further evaluation on similar services in South Wales (UK) is being proposed to study and measure the impact of these variables.
This study supports that psychiatric liaison service needs to be enhanced and expanded to meet the mental health needs of the frail older people admitted with an acute illness. Psychiatric liaison services operate in a wide range of hospital settings. Services could vary in quality and clinical settings based on the demographics and demand of the local population. The resources available for a particular service can only describe the structure of that service, which in turn will define the delivery of care and clinical activity. Therefore, similar outcomes and performance measures may not be applicable for service improvement in every setting. The key clinical outcome used to measure performance in this study was the LoS, but there is a wide variety of metrics that can be used to measure the effectiveness of the service. This includes patient satisfaction, carer burden, quality of life, readmission rates, or mortality. This paper describes a service evaluation project, and this was never designed with a meticulous research methodology. It may lack the rigor needed for inclusion in a systematic review, but we feel that its results may stimulate and inform a future research-based study of the observations made in this service evaluation.
Therefore, we propose systematic and structured service evaluation of various psychiatric liaison service models in order to benchmark outcome and performance measures.
Conclusion
Prompt mental health assessments for acutely unwell frail older people are not only cost effective but also improve clinical outcomes including LoS. Coproduction and integrated work with old age psychiatry teams improve patient flow and enable more patients to return to their original place of residence.
Acknowledgments
The authors are grateful to all the members of the department of old age psychiatry, nursing, and medical teams of the RGH. The authors are also grateful to the Department of Geriatric Medicine, Ysbyty Ystrad Fawr, and Research and Development Department, ABCi Team and Informatics, ABUHB, Wales, UK, for their continued support for research activities. They also appreciate the support from Mrs Salma Zabaneh, Education Centre, Ysbyty Ystrad Fawr, and all the faculty of masters course (Aging, Health and Disease), Cardiff University. There was no external funding for the study, but the ABUHB has received funding from the Intermediate Care Fund (£250,000) through Welsh Government to enhance and improve the existing old age psychiatric liaison services.
Footnotes
Author contributions
IS was responsible for the study concept and designed the evaluation. PF and JG contributed to data collection. KW and PC led the service modernization. IS wrote the first draft. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
An oral research presentation was given by IS at British Geriatrics Society (BGS) 2016 Spring Scientific Meeting on May 11–13, 2016, at ACC, Liverpool, and the abstract has been published in British Geriatrics Society, Page 10. None of the authors has any financial or any other kind of personal conflicts with this article. The authors report no other conflicts of interest in this work.
References
- 1.Office for National Statistics Population estimates for UK, England and Wales, Scotland and Northern Ireland, mid-2015. 2015. [Accessed August 22, 2016]. Available from: http://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/bulletins/annualmidyear-populationestimates/mid.
- 2.Bayliss J, Sly F. ‘Ageing across the UK’, Reg Trends. 2010. [Accessed December 7, 2016]. Available from: http://link.springer.com/article/10.1057/rt.2010.2.
- 3.Head of Integrated Services Social Care & Health Integrated pathway for older people. [Accessed August 22, 2016]. (Community Planning & Development Scrutiny Committee report 2014). Available from: https://democracy.newport.gov.uk/Data/Community%20Planning%20and%20Development%20Scrutiny%20Committee/20140910/Agenda/$996231%20-%20CONT727702.doc.pdf.
- 4.Who care wins. Improving the outcome for older people admitted to the general hospital: guidelines for the development of Liaison Mental Health Services for older people Report of a working group for the faculty of Old Age Psychiatry. Royal College of Psychiatrists; 2005. [Accessed August 22, 2016]. Available from: http://www.rcpsych.ac.uk/PDF/WhoCaresWins.pdf. [Google Scholar]
- 5.Singh I, Edwards C, Okeke J. Impact of cognitive impairment on inpatient falls in single room setting and its adverse outcomes. J Gerontol Geriatr Res. 2015;S4:S4-001. [Google Scholar]
- 6.Knight S, Singh I. Profile of inpatient falls in patients with dementia: a prospective comparative study between 100% single rooms and traditional multibedded wards. J Clin Gerontol Geriatr. 2016;7(3):87–92. [Google Scholar]
- 7.Goldberg SE, Whittamore KH, Harwood RH, Bradshaw LE, Gladman JRF, Jones RG. The prevalence of mental health problems among older people admitted as an emergency to a general hospital. Age Ageing. 2012;41(1):80–86. doi: 10.1093/ageing/afr106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lindesay J. Delirium in the elderly. In: Gelder MG, Lopez-Ibor J, Andreasen NC, Geddes J, editors. New Oxford Text Book of Psychiatry. 2nd ed. Oxford: Oxford University Press; 2000. pp. 1530–1534. [Google Scholar]
- 9.O’Keeffe S, Lavan J. The prognostic significance of delirium in older hospital patients. J Am Geriatr Soc. 1997;45(2):174–178. doi: 10.1111/j.1532-5415.1997.tb04503.x. [DOI] [PubMed] [Google Scholar]
- 10.Nightingale S, Holmes J, Mason J, House A. Psychiatric illness and mortality after hip fracture. Lancet. 2001;357(9264):1264–1265. doi: 10.1016/S0140-6736(00)04421-4. [DOI] [PubMed] [Google Scholar]
- 11.Holmes J, House A. Psychiatric illness predicts poor outcome after surgery for hip fracture: a prospective cohort study. Psychol Med. 2000;30(4):921–929. doi: 10.1017/s0033291799002548. [DOI] [PubMed] [Google Scholar]
- 12.Gustafson Y, Brannstrom B, Berggren D, et al. A geriatric-anaesthesiologic program to reduce acute confusional states in elderly patients treated for femoral neck fractures. J Am Geriatr Soc. 1991;39(7):655–662. doi: 10.1111/j.1532-5415.1991.tb03618.x. [DOI] [PubMed] [Google Scholar]
- 13.Holmes J, Bentley K, Cameron I. A UK survey of psychiatric services for older people in general hospitals. Int J Geriatr Psychiatry. 2003;18(8):716–721. doi: 10.1002/gps.911. [DOI] [PubMed] [Google Scholar]
- 14.Balestrieri M, Bisoffi G, Tansella M, Martucci M, Goldberg DP. Identification of depression by medical and surgical general hospital physicians. Gen Hosp Psychiatry. 2002;24(1):4–11. doi: 10.1016/s0163-8343(01)00176-1. [DOI] [PubMed] [Google Scholar]
- 15.Prudent M, Dramé M, Jolly D, et al. Potentially inappropriate use of psychotropic medications in hospitalized elderly patients in France: cross-sectional analysis of the prospective, multicentre SAFEs cohort. Drugs Aging. 2008;25(11):933–946. doi: 10.2165/0002512-200825110-00004. [DOI] [PubMed] [Google Scholar]
- 16.Huyse FJ, Herzog T, Lobo A, et al. Consultation-liaison psychiatric service delivery: results from a European study. Gen Hosp Psychiatry. 2001;23(3):124–132. doi: 10.1016/s0163-8343(01)00139-6. [DOI] [PubMed] [Google Scholar]
- 17.Draper B. The effectiveness of old age psychiatry services. Int J Geriatr Psychiatry. 2000;15(8):687–703. doi: 10.1002/1099-1166(200008)15:8<687::aid-gps181>3.0.co;2-k. [DOI] [PubMed] [Google Scholar]
- 18.Holmes J, Montana C, Powell G, et al. Liaison mental health services for older people: a literature review, service mapping and in-depth evaluation of service models. National Institute for Health Research Service Delivery and Organisation; 2010. [Accessed August 22, 2016]. Available from: http://www.nets.nihr.ac.uk/__data/assets/pdf_file/0016/81412/ES-08-1504-100.pdf. [Google Scholar]
- 19.Callaghan P, Eales S, Coates T, Bowers L. A review of research on the structure, process and outcome of liaison mental health services. J Psychiatr Ment Health Nurs. 2003;10(2):155–165. doi: 10.1046/j.1365-2850.2003.00300.x. [DOI] [PubMed] [Google Scholar]
- 20.Cole MG, Fenton FR, Engelsmann F, Mansouri I. Effectiveness of geriatric psychiatry consultation in an acute care hospital: a randomised clinical trial. J Am Geriatr Soc. 1991;39(12):1183–1188. doi: 10.1111/j.1532-5415.1991.tb03572.x. [DOI] [PubMed] [Google Scholar]
- 21.Grover S, Sarkar S, Avasthi A, et al. Consultation-liaison psychiatry services: difference in the patient profile while following different service models in the medical emergency. Indian J Psychiatry. 2015;57(4):361–366. doi: 10.4103/0019-5545.171854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi: 10.1016/0021-9681(87)90171-8. [DOI] [PubMed] [Google Scholar]
- 23.Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative database. J Clin Epidemiol. 1992;45(6):613–619. doi: 10.1016/0895-4356(92)90133-8. [DOI] [PubMed] [Google Scholar]
- 24.Mahoney FI, Barthel DW. Functional evaluation: the Barthel index. Md State Med J. 1965;14:61–65. [PubMed] [Google Scholar]
- 25.Colin C, Wade DT, Davis S, Home V. The Barthel ADL index: a reliability study. Int Disabil Stud. 1988;10(2):61–63. doi: 10.3109/09638288809164103. [DOI] [PubMed] [Google Scholar]
- 26.Granger CV, Albrecht GL, Hamilton BB. Outcome of comprehensive medical rehabilitation: measurement by PULSES profile and the Barthel index. Arch Phys Med Rehabil. 1979;60(4):145–154. [PubMed] [Google Scholar]
- 27.Searle SD, Mitnitski AB, Gahbauer EA, Gill MA, Rockwood K. A standard procedure for creating a frailty index. BMC Geriatr. 2008;8:24. doi: 10.1186/1471-2318-8-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rockwood K, Mitnitski A. Frailty in relation to the accumulation of deficits. J Gerontol A Biol Sci Med Sci. 2007;62(7):722–727. doi: 10.1093/gerona/62.7.722. [DOI] [PubMed] [Google Scholar]
- 29.Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489–495. doi: 10.1503/cmaj.050051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rockwood K, Andrew M, Mitnitski A. A comparison of two approaches to measuring frailty in elderly people. J Gerontol A Biol Sci Med Sci. 2007;62(7):738–743. doi: 10.1093/gerona/62.7.738. [DOI] [PubMed] [Google Scholar]
- 31.Rockwood K, Mitnitski A. Limits to deficit accumulation in elderly people. Mech Ageing Dev. 2006;127(5):494–496. doi: 10.1016/j.mad.2006.01.002. [DOI] [PubMed] [Google Scholar]
- 32.Singh I, Gallacher J, Davis K, Johansen A, Eeles E, Hubbard RE. Predictors of adverse outcomes on an acute geriatric rehabilitation ward. Age Ageing. 2012;41(2):242–246. doi: 10.1093/ageing/afr179. [DOI] [PubMed] [Google Scholar]
- 33.Tadros G, Salama RA, Kingston P, et al. The impact of an integrated rapid response psychiatric liaison team on quality improvement and cost savings: Birmingham RAID model. Psychiatrist. 2013;37(1):4–10. [Google Scholar]
- 34.Singh I, Ramakrishna S, Williamson K. The Rapid Assessment Interface and Discharge service and its implications for patients with dementia. Clin Interv Aging. 2013;8:1101–1108. doi: 10.2147/CIA.S36398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Marcantonio ER, Flacker JM, Wright RJ, Resnick NM. Reducing delirium after hip fracture: a randomised trial. J Am Geriatr Soc. 2001;49(5):516–522. doi: 10.1046/j.1532-5415.2001.49108.x. [DOI] [PubMed] [Google Scholar]
- 36.Singh I, Varanasi A, Williamson K. Assessment and management of dementia in the general hospital setting. Rev Clin Gerontol. 2014;24(3):205–218. [Google Scholar]
- 37.Huusko TM, Karppi P, Avikainen V, Kautiainen H, Sulkava R. Randomised clinically controlled trial of intensive geriatric rehabilitation in patients with hip fracture: subgroup analysis of patients with dementia. BMJ. 2000;321(7269):1107–1111. doi: 10.1136/bmj.321.7269.1107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Singh S. Assessment and management of older people in the general hospital setting. In: Zawada ET Jr, editor. Challenges in Elder Care. InTech; 2016. [Google Scholar]
- 39.Zhang H, Lu Y, Liu M, et al. Strategies for prevention of postoperative delirium: a systematic review and meta-analysis of randomized trials. Crit Care. 2013;17(2):R47. doi: 10.1186/cc12566. [DOI] [PMC free article] [PubMed] [Google Scholar]