

Abstract
Self-efficacy, denoting the degree of confidence an individual has in carrying out a specific activity, was initially discussed in the 1970s as a potential correlate of disease outcomes. Drawn from 35 years of related research, this review provides an updated understanding of the concept of self-efficacy and its relevance for arthritis management. There is a consistent link between self-efficacy, arthritis pain and disability, and adherence to recommended therapeutic strategies. A wide variety of intervention strategies improve arthritis self-efficacy, as well as outcomes. Steps to assess and intervene thoughtfully to maximize self-efficacy beliefs are likely to impact arthritis disability outcomes quite favorably and significantly, regardless of disease type, duration, or sociodemographic factors.
Keywords: arthritis, disability, outcomes, pain, self-efficacy
Introduction
Over 35 years ago, Albert Bandura (1977) proposed that the psychological variable of self-efficacy, a construct denoting one’s belief in his or her ability to successfully organize and implement a specific task, was a significant mediator of behavior. Bandura also proposed self-efficacy beliefs, which can be strengthened, potentially explained the discrepancy between having knowledge about a skill and the actual performance of this skill. Over the years, he and others have strongly supported the view that self-efficacy beliefs are predictive of motivation levels, thought patterns, moods, emotional reactions, and attitudes that can mediate the capacity and willingness to elicit behaviors that promote health (Bandura, 1977, 1986a, 1986b, 1997; Van der Bijl and Shortridge-Baggett, 2001), despite disconfirming experiences. Moreover, Bandura’s (1986a, 1994) research has supported the view that self-efficacy judgments can determine the extent to which a person will perform the adaptations needed to deal with chronic illness and its treatment.
In addition, this work points to how much effort will be expended on a task—and for how long—in the face of obstacles and aversive experiences (Bandura, 1997; O’Leary, 1985). Accordingly, in 1997, Bandura argued that because they are fundamental to many health-related behaviors and practices, self-efficacy beliefs were likely to be of immense importance in the context of influencing health outcomes among people with chronic illnesses such as arthritis. This is not only because self-efficacy beliefs predict the amount of effort and perseverance expended in reaching a goal, but they specifically influence the selection of goal-directed behaviors, in addition to the development of realistic goals (Berarducci and Lengacher, 1998).
The arthritic diseases, comprising over 100 forms of joint- and muscle-related disorders, continue to pose an immense burden on both the affected individual and the society (Baruth et al., 2013). Commonly associated with intractable pain, fatigue, weakness, functional and psychosocial limitations, plus progressive physical disability, and affecting millions of people worldwide, these conditions can be extremely debilitating. Moreover, several forms of arthritis, such as rheumatoid arthritis, systemic lupus erythematosis, and juvenile rheumatoid arthritis, are commonly associated with systemic problems that can severely magnify the extent of the prevailing disability and can challenge the affected individual’s coping capacity quite substantively (Arthritis and Related Conditions, 2011). The absence of a cure for any form of arthritis, the harmful side-effects of commonly used pharmaceutical strategies, the unpredictable waxing and waning of one or more physical aspects of the disease, and the immense psychological impact of all of these disabling conditions render the successful management of all forms of arthritis extremely challenging (Marks and Allegrante, 2007).
To this end, current researchers in the field emphasize the importance of minimizing disability and maximizing independence and life quality of the affected individual by assessing and treating both the biological as well as the psychological consequences of these conditions (e.g. Orengo et al., 2001; Somers et al., 2009a). In particular, given the link between a variety of human behaviors and several prevalent disease consequences of arthritis (Gaines et al., 2002; Harrison, 2004; Makelainen et al., 2009; Maly et al., 2005; Pells et al., 2008), and between self-efficacy and behaviors (Arnstein, 2000), Sharma et al. (2003) strongly supported a key role for continuing to examine the role of self-efficacy and its application in the context of strategies to optimize arthritis outcomes, such as modifying their activity levels and following complex medication regimens (Taal et al., 1993b).
However, even though self-efficacy has become a strong explanatory factor in efforts to help people deal with a variety of chronic diseases such as arthritis (Larkin and Kennedy, 2013; Rapley and Fruin, 1999; Sperber et al., 2013) and having the confidence to exercise, a crucial behavior among others for managing most arthritis conditions significantly improves the physical, social, as well as the health status of persons with arthritis (e.g. Der Ananian et al., 2008; Wright et al., 2008), very few current arthritis-related publications focus on the possible important assessment and treatment opportunities afforded by the insightful application of self-efficacy and its theoretical principles.
In light of the increasing role of health behaviors as mediators of health status, and the fact that adults with arthritis are required to often carry out highly complex novel behaviors, but may not be confident to do so, it was felt a comprehensive updated exploration of this topic could thus be very useful, first for extending our understanding of how this body of literature might be applied to better understand a variety of arthritis-related clinical features, and second, for guiding a more successful and efficacious clinical care process for people with arthritis, to manage their illness, in general. This review thus specifically focuses on examining some relevant past and current research concerning the link between behavior specific self-efficacy beliefs and one or more aspects of arthritis disability as reported over the past 35 years since Bandura brought his ideas to our attention, including the various attributes or dimensions of self-efficacy assessed in the context of arthritis. It also describes actual processes for enhancing self-efficacy directly, as well as what approaches may work to enhance self-efficacy indirectly. Although quite diverse, it was felt this information would be particularly helpful in efforts to better comprehend how certain confidence perceptions can explain the persistence of various symptoms, as well as suboptimal self-management behaviors that can negatively influence arthritis morbidity (see Tables 1 and 2). Some management strategies commonly recommended for minimizing the physiological, physical, or psychosocial consequences of arthritis where perceived confidence to carry out one or more of these tasks might make a significant difference to health outcomes are described in Table 3. Finally, tasks and behaviors people with arthritis may need to learn (Table 4) and the related implications of this research are discussed.
Table 1.
Some important physical and psychosocial manifestations of arthritis that may impact self-efficacy perceptions.
| Physical manifestations |
| Pain in one or more joints, muscle, soft tissue, bone |
| Diminished joint range of motion |
| Diminished muscle strength and endurance |
| Impaired balance capacity |
| Difficulties performing tasks of daily living (De Boer et al., 2009) |
| Problems related to the presence of one or more chronic comorbid conditions, such as heart disease, diabetes, cancer, and respiratory conditions that may further limit the ability of the patient to function physically and confidently (Braden et al., 1993) |
| Psychosocial manifestations |
| Depression and/or anxiety |
| Limitations in social, work, and recreational activities |
| Sleep disturbances (Davis, 2003) |
| Diminished life quality |
Table 2.
Some medical and nonmedical factors that may influence arthritis morbidity adversely if not remediated.
| Medical factors |
| Persistent pain, resulting in avoidance behaviors |
| Muscle weakness |
| Reduced aerobic capacity |
| Limited flexibility of joints and muscles |
| Obesity or malnourishment |
| Stress, fatigue, sleep disturbances, and lack of energy |
| Mood fluctuations |
| Nonmedical factors |
| Poor psychological adjustment due to fear or anxiety |
| Lack of confidence in prevailing abilities to function, control pain |
| Inaccurate outcome expectations |
| Poor pain coping skills |
| Low self-esteem and self-worth |
| Limited knowledge about the disease |
| A feeling of helplessness and affective distress, in general |
| Poor physician or provider communication skills |
| Poor adherence to long-term treatment regimens |
| Deficient social support, including instrumental, emotional, and informational support |
Table 3.
Management strategies commonly recommended for people with arthritis.
| Joint range of motion, strengthening, and aerobic exercises |
| Weight loss or weight normalization |
| Joint protection and energy conservation strategies |
| Use of assistive devices or aids |
| A variety of medication regimens |
| Surgery |
| Home and workplace modifications |
| Occupational and physical therapy |
| Psycho-educational interventions to improve knowledge and self-management skills and to strengthen self-efficacy beliefs and outcome expectations |
Table 4.
Behaviors or tasks people with arthritis may need to learn to effectively self-manage their condition.
| Use medication(s) correctly |
| Reduce their symptoms/slow disease progression |
| Interpret and report their symptoms accurately |
| Adjust to their condition socially and economically |
| Cope with the emotional consequences of their disease |
| Participate in decisions concerning prescribed treatments |
| Communicate effectively with physicians, other care-givers |
| Modify work, recreational, home environments effectively |
| Manage their condition postoperatively, if and when required |
This specific approach was implemented in light of the immense disease burden experienced by people with disabling arthritis worldwide, which shows no abatement despite modern technologies, and the fact that only one review paper on this potentially useful set of understandings could be located on PubMed, and this was published in 2001. Among six other reviews, retrieved using the key words arthritis and self-efficacy, two focused solely on osteoarthritis, and three on chronic illness or disability, and no current experimental reports were forthcoming on how building self-efficacy strategically can influence arthritis outcomes. There is currently no body of work consolidating the available research related to self-efficacy and arthritis, and its utility, despite the potential importance of revisiting and consolidating the research in this area. Consequently, this review specifically attempted to fill this gap by examining
the various self-efficacy attributes or dimensions that have been studied among arthritis samples over the past 35 years and their implications for practice and/or future research;
whether there have been consistent associations between these various self-efficacy attributes and arthritis symptoms and outcomes over the past 35 years;
whether there is any evidence of a dose–response effect between specific self-efficacy perceptions related to pain control, coping, management behaviors, and arthritis outcomes, and
whether it is possible to increase arthritis self-efficacy, and if so, what are possible best practice approaches.
Methods
To achieve the aims of this review, all relevant publications located in the Cumulative Index to Nursing and Allied Health Literature (CINAHL), Medline, PubMed, PsychINFO, Science Direct, Web of Knowledge, and Social Science Citation databases covering the years 1980–2014 were sought. To be included in the present review, only English language publications concerning arthritis disability and self-efficacy were deemed acceptable. The specific studies retrieved were categorized as either descriptive correlation or prospective studies with either theoretical or nontheory-based intervention protocols. The key search terms used were “arthritis” and “self-efficacy.” Studies detailing instrumentation processes related to the topic, those discussing diseases other than arthritis and those focused on chronic diseases, in general, were excluded (see Figure 1).
Figure 1.
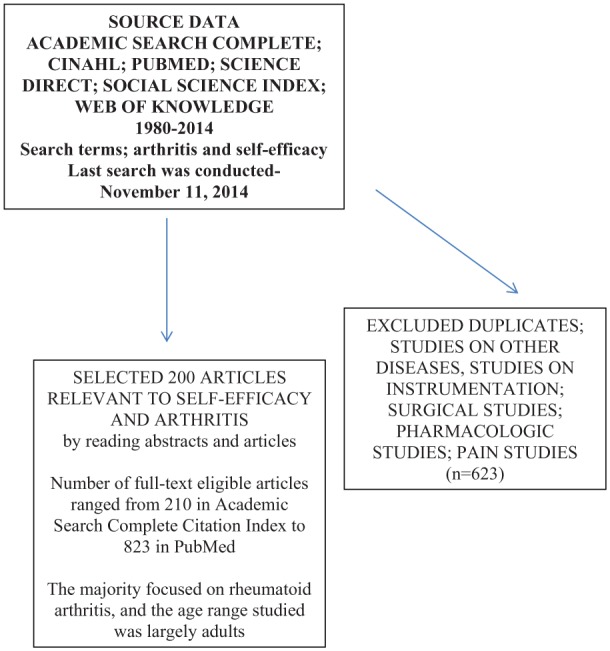
Literature review strategy summary.
Although the desired information was extracted from the available documents in a systematic way, no systematic review was conducted, given the many varied tools or approaches used to assess and/or estimate self-efficacy, the varied domains of self-efficacy assessed, the varied diseases studied, and their varied sampling strategies and research designs. Instead, in accordance with Bandura’s (1977, 1986b) belief that self-efficacy is an important behavioral mediator and may predict future behaviors (Jensen et al., 1991), this review examined whether this body of collective research constituted largely by cross-sectional data supports the view that arthritis disability may be impacted negatively by low self-efficacy perceptions and positively by efforts that enhance self-efficacy perceptions.
Since self-efficacy is a psychological attribute amenable to intervention, support for the efficacy of implementing theoretical as well as nontheoretical self-efficacy enhancing interventions to improve the performance ability of people with arthritis as outlined in Figure 2 was sought.
Figure 2.

Hypothetical model of possible intermediate, primary, and secondary outcomes of utilizing self-efficacy enhancing strategies in the conservative management of arthritis.
Results
Among the articles that matched the search criteria, 873 related articles were found listed in PubMed, 625 in Web of Science, 700 in Science Direct, 312 in PsychINFO were listed, 213 were listed in CINAHL, 254 papers were listed in the Science Citation Index, and 210 related papers were listed in Academic Search Complete. Many listings overlapped and some were excluded if they were listed, but did not address the topic in question. Among the 200 articles employed for this review extracted from the various databases, articles that addressed issues related to arthritis management were included as required to provide a context for the challenges people with arthritis face and are required to deal with and adapt to (see Tables 3 and 4).
The specific studies detailing self-efficacy and some form of arthritis or arthritis symptom were divided into those that were cross-sectional in nature, and those that were prospective. Among those that were prospective were several clinical observational studies, and intervention studies, classified as theoretically based if they followed explicit recommendations for enhancing self-efficacy, and nontheoretical if self-efficacy was not specifically the target intervention.
Clinical studies linking arthritis self-efficacy to arthritis outcomes
In terms of evaluating the contribution of self-efficacy beliefs to one or more key arthritis outcomes, the literature reveals a broad array of 25 cross-sectional studies dating back to the 1980s that have examined the magnitude and direction of the theorized association between the concept of self-efficacy and arthritis functioning across several diverse domains, and among an array of arthritis sufferers (e.g. Gaines et al., 2002; Harrison, 2004; Maly et al., 2005). Others such as Taal et al. (1993a) have examined whether adherence to self-management strategies is related in part to their self-efficacy beliefs, whether there is a dose–response between self-efficacy magnitudes and symptom presentation, and the relationship of self-efficacy to arthritis symptoms (see Table 5).
Table 5.
Selected studies demonstrating statistically significant relationships between self-efficacy levels and key variables of importance in the management of arthritis, regardless of sample, or self-efficacy attribute assessed.
| Study | Sample | Results |
|---|---|---|
| Dose–response–related studies | ||
| aBarlow et al. (2002) | 82 RA cases | Lower arthritis self-efficacy scale scores predicted greater physical impairment, pain, fatigue, a more depressed and anxious mood and less positive mood |
| aBaruth et al. (2013) | 396 arthritis cases | Among other variables, lower arthritis self-efficacy was associated with greater disability |
| Blamey et al. (2009) | 218 attendees | Low arthritis self-efficacy was associated with greater pain; rheumatology clinic self-efficacy and analgesic use were negatively related |
| Symptom-related studies | ||
| Alok et al. (2014) | 100 FM cases | Patients had significantly lower arthritis self-efficacy; higher self-efficacy was positively associated with life quality |
| 100 controls | ||
| Benka et al. (2014) | 146 cases of RA | Coping self-efficacy was uniquely related to distress in early RA |
| 102 cases of early RA | ||
| aBrekke et al. (2001) | 815 patients with RA | Baseline self-efficacy levels for pain and other symptoms seemed to influence 2-year changes in these health status measures |
| Dirik and Karanci (2009) | 117 RA cases | Arthritis self-efficacy is a significant predictor of depression |
| Marcum et al. (2014) | 190 patients with knee OA | Arthritis self-efficacy correlated with gait speed |
| Orengo et al. (2001) | 45 men with RA | Self-efficacy accounted for over one-third of the predicted variance in disablement |
| aPackham et al. (2002) | 246 adults with long-standing JIA | Pain self-efficacy and pain were inversely correlated (p < .001). Pain self-efficacy was weakly related to inflammation (p < .005) |
| Pells et al. (2008) | 174 cases of overweight adults with knee OA | Pain self-efficacy accounted for 14% variance in pain; function self-efficacy accounted for 10% of the variance in disability; and self-efficacy for resisting eating predicted eating practices |
| Porter et al. (2008) | 38 patients with OA | Among patients, higher self-efficacy for pain communication was associated with lower pain levels, physical and psychological disability, and pain catastrophizing |
| aRayahin et al. (2014) | 212 patients with knee OA | Higher self-efficacy and good 2-year knee pain outcomes were found |
| Somers et al. (2010) | 263 arthritis cases | Self-efficacy for pain control and function accounted for 32%–42% of disease severity’s effect on their respective outcomes |
| Van Liew et al. (2013) | 363 older persons with OA | Quality of life was significantly related to self-efficacy |
| aWallis et al. (2014) | 20 adults with severe OA | Failure to improve self-efficacy was associated with lack of improvements in pain and activity limitations |
| Program adherence studies | ||
| Gyurcsik et al. (2003) | 216 adults with arthritis | Task self-efficacy for aquatic exercise was predictive of attendance. High attendees had higher task and scheduling self-efficacy than low attendees |
| aGyurcsik et al. (2013) | 56 adults with arthritis | Greater self-regulatory efficacy was associated with better adherence to managing disease barriers |
| Loucks-Atkinson (2007) | 224 cases with FM | Higher self-efficacy for negotiation scores was associated with higher levels of motivation and effort to negotiate and a higher level of participation |
RA: rheumatoid arthritis; FM: fibromyalgia; OA: osteoarthritis; JIA: Juvenile Idiopathic Arthritis.
Prospective study.
Cases studied have predominantly included adults diagnosed as having varying degrees of disabling rheumatoid arthritis, osteoarthritis, and fibromyalgia, and the attributes of self-efficacy, predominantly studied as a behavior specific construct, have been assessed most consistently by the instrument developed by Lorig et al. (1989) that focuses on pain self-efficacy, self-management, and functional self-efficacy. However, self-efficacy for exercise, task self-efficacy, coping self-efficacy, self-efficacy for negotiation, scheduling self-efficacy, and mobility-related self-efficacy, as well as self-efficacy for weight reduction are among other domains that have been examined.
Despite this highly heterogeneous collection of research issues, instruments, samples, and design, among other factors outlined in Table 5, a consistent theme that emerges is that the level of perceived confidence in one or more behavioral domains is strongly associated with the magnitude of one or more disease-associated features, regardless of sample studied or instrument applied. Self-efficacy also correlates consistently with adherence to behaviorally oriented regimens, and appears to produce a variety of dose–response–related health outcomes. That is, notwithstanding the limitations of interpreting this broad array of cross-sectional and prospective data, a less than optimal level of confidence to carry out one or more essential behaviors related to the self-management process appears consistently related to an arthritis sufferers’ pain (Pells et al., 2009; Sinikallio et al., 2014), regardless of arthritis diagnosis (Brekke et al., 2001; Buckelew et al.,1994; Buescher et al., 1991; Keefe et al., 1997a; Packham et al., 2002).
The strength of an arthritis patient’s self-efficacy perceptions also consistently correlates with measures of functional status in a linear manner (Maly et al., 2006; Rejeski et al., 2001; Sinikallio et al., 2014), regardless of disease type, study sample, or sampling methods, or when differences in disease-associated variables and personality are controlled for (Benka et al., 2014). According to Somers et al. (2010), self-efficacy also clearly mediates the relationship between disease severity and pain and functioning, and in cases of older adults with knee osteoarthritis, functional self-efficacy explained the greatest amount of variance in all physical performance measures as determined by step-wise linear regressions (Maly et al., 2005).
In other studies, self-efficacy levels also explained differential disease responses (Bolen et al., 2010), as recently discussed by Allen et al. (2010) and Greene et al. (2006); health status (Cross et al., 2006); depression levels (Broderick et al., 2011; Dirik and Karanci, 2009); fatigue (Van Hoogmoed et al., 2010); life quality (Broderick et al., 2011); problems with medication adherence (Spruill et al., 2013); coping capacity (Gyurcsik et al., 2009); and adjustment efforts among people with rheumatoid arthritis (Lowe et al., 2008).
Additional correlations exist between prevailing levels of self-efficacy and extent of activity participation (Baruth et al., 2014; Dekker et al., 2009; Huffman et al., 2014; Hutton et al., 2009; Leveille et al., 2003), an essential component of arthritis management.
Self-efficacy for exerting control over stressors, and for effectively mobilizing the social network, also influences arthritis outcomes such as anxiety and depression (Dirik and Karanci, 2009; Lowe et al., 2008). Other research shows that fatigue, commonly associated with inflammatory arthritis (Riemsma et al., 1998); coping ability (Benka et al., 2014); and resilience, an important factor in predicting pain and physical functioning in people with arthritis, are consistently impacted by the nature of a person’s self-efficacy appraisals (Wright et al., 2008). Other data reveal that arthritis self-efficacy beliefs can affect the extent of analgesic usage (Blamey et al., 2009), participation in leisure time physical activities (Reinseth et al., 2011), adaptation or adjustment to one’s condition (Packham et al., 2002; Wright et al., 2008), the ability to resist excessive eating (Pells et al., 2008; Somers et al., 2014), and the ability to communicate about pain (Porter et al., 2008).
In short, even though Benyon et al. (2010) found no relationship between self-efficacy and pain as predictors of osteoarthritis outcomes in a systematic review, arthritis disability and the magnitude of an individual’s self-efficacy perceptions for managing their health condition appear to be consistently related in a dose dependent manner when taking all forms of arthritis and domains of self-efficacy. This cumulative body of ongoing research thus continues to support the view that efforts to both monitor and strengthen a patient’s self-efficacy appraisals (Brassington et al., 2002), which are amenable to change through various education programs and other strategies (Cross et al., 2006), may offer a potentially important, but often overlooked channel of opportunity for ameliorating the pervasive negative effects of arthritis on the affected adults’ physiological, emotional, occupational, and social well-being, as outlined recently by McKnight et al. (2010) and Benka et al. (2014).
Conversely, careful examination of self-efficacy perceptions and attempts to minimize the impact of low self-efficacy appraisals may specifically foster heightened psychological well-being (Benka et al., 2014) and better adjustment to the disease (Wright et al., 2008). Furthermore, thoughtful application of the self-efficacy concept can produce higher activity levels (Leveille et al., 2003), better exercise adherence (Gecht et al., 1996), improved performance ability (Gaines et al., 2002; Mendes de Leon et al., 1996; Strahl et al., 2000), more favorable self-reported pain task difficulty ratings (Rejeski et al., 1996), while fostering psychological thriving (Sirois and Hirsch, 2013) and general perceptions about functional ability (Mendes de Leon et al., 1996) among people with arthritis, regardless of level of physical function.
Consequently, efforts to help optimize self-efficacy for a variety of behaviors are arguably highly salient in efforts to yield more favorable outcomes for people with an arthritic condition than those attained when ignoring such efforts. Since the self-efficacy concept does not seem to have impacted the design of arthritis treatments as consistently as one might expect given its importance as a predictor of arthritis outcomes, the next section of this review examines the extent to which efforts to enhance arthritis self-efficacy directly as well as vicariously can indeed heighten the self-efficacy beliefs of arthritis sufferers, and if so, whether these are accompanied by positive changes in health outcomes believed to be associated with self-efficacy beliefs in selected cross-sectional studies outlined in Table 5 or in the above discussion.
Intervention studies linking self-efficacy to arthritis outcomes
In terms of prospective evidence linking perceived self-efficacy beliefs and arthritis outcomes, there are currently approximately 20 studies which have reported on interventions designed to improve self-efficacy among arthritis cases or on self-efficacy outcomes following interventions. Initiating this body of research was the work performed by Holman et al. (1989) who developed a comprehensive arthritis self-management intervention known as the Arthritis Self-Management Program (ASMP) where participants exhibited consistent significant early and sustained clinical improvements that seemed closely linked to changes in the participant’s self-efficacy scores for pain and managing fatigue. Strong support for self-efficacy as a salient outcome predictor was forthcoming after that, given that program participation not only heightened self-efficacy test scores but also reduced medical services usage and related health-care costs (Lorig et al., 1993), a finding later supported by several independent researchers (e.g. Barlow and Barefoot, 1996; Barlow et al., 1999; Braden et al., 1993; Cross et al., 2006, Davis et al., 1994; Leung et al., 2014; Nuñez et al., 2009; Taal et al., 1993b; Yip et al., 2008).
In accord with study results of Braden et al. (1993), Lorig and Gonzalez (1992) and Lorig and Holman (1993), 12 years after implementing the ASMP, Allegrante et al. (1993) who conducted a comprehensive hospital-based patient education program for people with knee osteoarthritis based on self-efficacy theory found that taking steps to specifically enhance the patient’s self-efficacy for walking produced significant and clinically meaningful improvements in the patient’s functional status without an increase in pain.
As part of this randomized controlled study, 47 patients with moderate to severe knee osteoarthritis, ages 40–89 years, participated in an 8-week walking education program conducted for 90 minutes three times per week for groups of 10–15 patients. Each session included direct instruction by a trained interventionist or a guest speaker on a topic of special interest, social support, light physical activity, and walking. Participants also received a manual describing exercises to be learned, a videotape and audiocassette about walking, and a diary in which they were asked to record their physical activity levels during the study. To enhance self-efficacy and task mastery, experimental group participants were exposed to the four strategies recommended by Bandura (1977, 1986b) for increasing behavioral competence, namely
facilitation of task mastery;
exposure to direct or vicarious walking experiences;
social and verbal encouragement and persuasion;
assistance in dealing with emotions believed to potentially impede adherence to walking.
Carefully organized into four successive phases that incorporated well-established methods for fostering the desired behaviors, including shaping and guiding, contracting, maintenance, and relapse prevention strategies, the results of this study strongly supported the beneficial application of self-efficacy theory in enhancing short-term outcomes for persons with disabling knee osteoarthritis.
In another study of patients with rheumatoid arthritis, Taal et al. (1993b) attempted to help participants adjust to their exercise, rest and medication regimens, and to the varying nature of the disease. They did this by helping them make the right decisions about required adjustments to their treatment regimens and how to carry out desired “self-management” behaviors. Based on Bandura’s (1977, 1986b) Social Cognitive Theory and the ASMP developed by Lorig and Holman (1993), the program goal was to strengthen the individual’s perceived self-efficacy, outcome expectations, and self-management behaviors and ultimately to better their health status. The program, which was evaluated prospectively, established significant positive effects for the group for functional disability, joint tenderness, the practice of relaxation and physical exercises, self-management behaviors, outcome expectations, self-efficacy for overall function, and knowledge. Positive results of the intervention for the practice of exercise, self-efficacy for function, and knowledge were still evident 14 months after implementation.
Hammond et al. (1999) similarly applied the self-efficacy construct to the design of an educational–behavioral joint protection program for 35 people with rheumatoid arthritis. The strategies this group used to maximize joint protection adherence, which were partly similar to those advocated by Jensen and Lorish (1994), included goal setting, contracting, modeling, homework programs, motor learning theory, recall enhancing methods, and mental practice. Although no significant changes in pain, functional disability, grip strength, self-efficacy, or helplessness were reported post-education, joint protection strategy usage was significantly increased at the 12- and 24-week follow-up. The sample was quite small, however, and the study may also have been too short in duration to demonstrate anticipated functional improvements. This is supported by a more recent study reported by Hammond and Freeman (2001) that detailed outcomes of a similar joint protection program for 65 people with rheumatoid arthritis after 1 year. In the latter study, as in the first study in 1999, the positive findings that adherence to the learned joint protection techniques was facilitated by the cognitive-behavioral strategies employed suggested that these strategies were effective for facilitating performances of the recommended behaviors.
In another study, after combining the principles of self-management, adult learning, case management, and self-efficacy enhancement in an interdisciplinary program that integrated group and individualized treatment, Alderson et al. (1999) reported significant increases in self-efficacy among 57 persons diagnosed as having arthritis who participated in such a program. These improvements were noted immediately following the program and were sustained for up to 6 months after the program. Disability and pain also decreased over the follow-up period.
Similarly, Brekke et al. (2003) who conducted a longitudinal observational study of 306 patients with rheumatoid arthritis over a 5-year period showed that changes in self-efficacy regarding pain as well as other symptoms were positively related to changes in perceived health status as outlined in Figure 2. This study also revealed that high levels of self-efficacy at baseline were positively related to improved pain perception after 5 years and that mental distress at baseline was related to reduced self-efficacy after 5 years.
Piyakhachornrot et al. (2011) who developed an integrated health education program including exercise based on self-efficacy theory that aimed to enhance self-efficacy expectations among patients with knee osteoarthritis showed positive results in a recent quasi experimental study. In terms of mastery experiences, patients were trained to precisely carry out their exercise regimens. They received demonstrations on how to do this and watched a patient with a similar condition carry this out. They were specifically encouraged to engage in exercise or perform activities related to reducing knee symptoms they had learned. To reduce emotional arousal, they discussed and shared strategies for reducing barriers to exercise and participants were trained until they felt confident to exercise.
Other interventions studied prospectively and found to impact arthritis self-efficacy and symptoms indirectly and favorably and that support a self-efficacy disease presentation link include the following: aquatic programs (Guo et al., 2009), cognitive-behavioral self-help interventions (Garnefski et al., 2013; Shigaki et al., 2013), exercise and dietary weight loss interventions (Focht et al., 2005), exercise and education interventions (Grønning et al., 2012; Hopman-Rock and Westhoff, 2000), tai-chi (Waite-Jones et al., 2013), and yoga (Evans et al., 2013) (see Table 6).
Table 6.
Selected intervention methods found to impact arthritis self-efficacy and symptoms vicariously and positively in prospective studies.
| Study | Methods | Key self-efficacy–related results |
|---|---|---|
| Focht et al. (2005) | The Arthritis, Diet, and Activity Promotion Program was applied for 18 months to 316 overweight or obese older adults with symptomatic knee OA | Mobility-related self-efficacy increased significantly |
| Callahan et al. (2011) | 463 adults with self-reported arthritis were assigned to walking program either in a group or in a self-directed mode and assessed before and after 6 weeks of the program | Both programs improved arthritis self-efficacy at 6 weeks and at 1 year as regards pain and symptom management |
| Deng and Hu (2013) | 16 patients with RA received six 1-hour structure educational sessions | Participants showed significantly improved arthritis self-efficacy for pain scores, as well as self-efficacy for other symptoms at the 1-month follow-up |
| Guo et al. (2009) | Aquatic program was applied to six arthritis cases over age 80 years for 3 months | The program increased the participants’ arthritis self-efficacy scale scores and reduced the negative impact of arthritis |
| Hammond and Freeman (2006) | 183 cases with fibromyalgia participated in a community patient-education–exercise program, using a cognitive-behavioral approach in a randomized controlled trial | At 4 months, arthritis self-efficacy scores were significantly higher in the patient education group as well as total fibromyalgia impact; these changes were not sustained at 8 months |
| Hewlett et al. (2011) | Two-arm parallel randomized controlled trial of 168 adults with RA of a program of self-management for fatigue consisting of six weekly 2-hour sessions, consolidated in week 14 | At 18 weeks, fatigue impact scores were better in active group, as were secondary measures including self-efficacy as measured on the RA self-efficacy scale |
| Hopman-Rock and Westhoff (2000) | Exercise and education applied to cases with either hip or knee OA for 6 weeks | Moderate increases in self-efficacy were noted and lasted up to 6 months |
| Knittle et al. (2011) | 271 cases with RA were randomly selected to receive a questionnaire assessing pain, a 4-item goal efficacy subscale of the Self-Regulation Skills Battery in relation to that self-set physical activity goals, physical activity, life quality; 129 did a follow-up questionnaire; 109 remained in final sample | The first mediation model revealed significant indirect effects of self-efficacy upon arthritis pain, through the achievement of physical activity goals |
| It was concluded that higher levels of self-efficacy for physical activity increase the likelihood patients will achieve their physical activity goals | ||
| Lee et al. (2013) | Applied a tai-chi program plus acupressure or tai-chi alone to a nonrandom sample of 21 patients with RA for 12 weeks | Arthritis pain self-efficacy improvements were observed, regardless of group allocation |
| Niederman et al. (2011) | Joint Protection Education for 53 adults with RA in a randomized controlled trial measured at 6 and 12 months | At 12 months, self-efficacy for joint protection was greater in experimental than control group, along with grip strength |
| Lamb et al. (2008) | Chronic Disease Management Program for 121 cases waiting for surgery with severe OA carried out over six weekly sessions | Pain and function self-efficacy increased among other factors at 6 and 122 weeks using the arthritis self-efficacy pain and function scales |
| Landa-Gonzalez and Molnar (2012) | Carried out an occupational therapy intervention among older Hispanic females | For the occupational intervention, the task specific self-efficacy scores were higher for the intervention than the control group |
| Manning et al. (2014) | 52 cases with RA underwent four 1-hour group sessions of a brief supervised education, self-management, and global upper extremity exercise training program, in addition to a home exercise regimen of 12 weeks’ duration and compared to 66 cases who received standard care | Self-efficacy improved to a greater extent in the group with supplementary exercises |
| McCarron (2014) | 23 cases with RA attended 1-hour six monthly support groups | There was an improvement in quality of life and this was linked to empowerment improvements attributed to increases in self-efficacy |
| Pariser and O’Hanlon (2005) | 85 elders with arthritis received standard education or education supplemented by telephone over a 6-week period | Arthritis self-efficacy improved in both groups |
| Rejeski et al. (1998) | Aerobic or resistance training programs were applied to older adults with OA over an 18-month period | Both exercise treatments increased self-efficacy for stair climbing; self-efficacy mediated the stair walking time variable |
| Schoster et al., (2005) | The People with Arthritis Can Exercise (PACE) Program, a community-based program was applied for 347 arthritis cases for 8 weeks | Participants reported improved exercise self-efficacy |
| Unetzer et al. (2008) | Care Management Program for 60 cases of older patients with depression and OA was provided over a 6-month period | Patients experienced improvements in depression self-efficacy on a 0–10 scale among other factors |
OA: osteoarthritis; RA: rheumatoid arthritis.
Table 7.
Recommended approaches for promoting arthritis self-efficacy.
| Employ a variety of cognitive strategies including the following: lectures, discussions, brainstorming, demonstrations, goal setting, contracting, modeling, mental practice, homework, recall enhancing methods, and mutual aid and support |
| Involve significant others, such spouses/family members, as well as health-care providers deemed trustworthy and credible in patient derived goal setting and management processes |
| Employ graduated behavioral interventions to promote ability to self-manage fear, stress, pain, depression, and anxiety, as well as to exercise, control weight, protect joints, and carry out self-monitoring strategies |
| Apply encouragement, persuasion and direct or indirect support so as to maximize mastery experiences and subjective for the desired changes (Jerome et al., 2002) |
| Promote decision-making skills, plus the necessary knowledge, skills, and problem-solving ability to deal with challenging unpredictable disease-related situations |
| Use multi-component instructional strategies such as pamphlets, lectures, audiotapes, and videotaped instructions |
| Use appropriately staged instructional strategies (Keefe et al., 2000) |
| Integrate both individual and group intervention approaches |
| Practice activities that approximate those to be performed in the home, worksite or community |
| Set desirable, but achievable short-term, rather than long-term goals |
| Build self-efficacy of care-givers if indicated |
| When planning follow-up care, focus on continuity, easy access to knowledgeable providers, and an effective interpersonal relationship |
| Consider using nursing consultations following patient education |
Source: Adapted from Allegrante et al. (1993), Hammond et al. (1999), Lorig et al. (1993), Primdahl et al. (2011a, 2012), and Reinseth et al. (2011).
Table 8.
Anticipated impact of heightened self-efficacy beliefs on arthritis outcomes.
| May foster the initiation, achievement, and maintenance of successful disease-associated coping and self-management strategies (Weiner et al., 2013) |
| May increase time and effort expended on a task in the face of obstacles |
| May reduce the extent to which individuals with arthritis become disabled |
| May influence the degree of hope experienced versus the degree of despair experienced |
| May heighten the sense of control people with arthritis can have over their lives (Heye et al., 2002) |
| May promote physical activity participation (Mielenz et al., 2013) |
| May heighten life quality (Cramm et al., 2013; Seid et al., 2014) |
| May foster the degree to which the doctor–patient relationship can be maximized (Barlow, 1998) |
| May enhance the outlook of the caregiver, which predicts physical outcomes (Beckham et al., 1995) |
In addition, self-management programs, combined with adaptive pain coping skills training interventions and social emotional support to strengthen self-efficacy expectations (Taal et al., 1993a), may further enhance self-efficacy cognitions, plus the physical and psychological status of individuals with arthritis (Keefe et al., 1997a). Educating spouses, significant family members, and care-givers may also impact favorably upon a patient’s expectancies about their ability to control arthritis-related symptoms, such as pain and functional limitation (Beckham et al., 1995; Keefe et al., 1996, 1997b; Martire et al., 2003). However, very few studies have been designed to specifically impact self-efficacy directly, and to test whether this systematic theory-based self-efficacy enhancement approach is superior to that attained through nonspecific treatment approaches. Consequently, it is also unclear as to whether self-efficacy improvements observed in relation to a range of different interventions actually have a significant effect on or mediate the changes in the behaviors or symptoms that were observed in these studies.
Practical programmatic approaches and suggestions
In terms of seeking to apply self-efficacy theory to maximize arthritis outcomes, the literature on this topic strongly suggests that a direct focus on the development of self-efficacy or enhancing the patient’s prevailing self-efficacy in one or more domains will prove more valuable than not, even if indirect methods can heighten self-efficacy. Among the different methods for enhancing task or behavior specific self-efficacy, Bandura (1986b, 1997) and Strecher et al. (1986) originally suggested that clinicians try to: (1) identify and reinforce the patient’s past and present successful accomplishments, (2) direct the patient to observe successful behaviors of others, (3) provide positive feedback for the patient’s efforts or encourage people in the patient’s social network to do this, and (4) try to ensure their patients interpret their feelings correctly.
For example, if a patient in pain feels anxious about undertaking a new behavior such as exercising, the clinician might explain that their anxiety is justified, given what the patient is being asked to undertake, but that once the requisite skill is acquired, their pain will abate. They could also direct the patient to observe others similar to them carrying out the activity and experiencing a successful outcome. Because self-efficacy is strengthened by actually performing the task in question, rather than just discussing this (Blazer, 2002), the clinician may want to adopt a skills-based learning approach and help the novice patient to carry out the actual task requirements in a step by step fashion. The clinician can also offer timely and positive reinforcement and encouragement as the new skill is practiced and learned.
This approach of employing several principle sources of efficacy information successively to promote self-efficacy as outlined by Bandura (1977), including performance attainments, vicarious learning, verbal persuasion, and physiological feedback, was successfully employed by Kovar et al. (1992) who designed a multipronged intervention to heighten the well-being of older adults with knee osteoarthritis. To this end, this group employed a variety of learning activities that included lectures, discussions, brainstorming, demonstrations, goal setting, modeling, and mutual aid and support using a team approach, discussions, demonstrations, an exercise component, and a social component to provide an array of strategies believed to foster self-efficacy. Patients were also encouraged to work collaboratively with their leader and with each other to achieve their goals, and positive achievements were duly rewarded and reinforced.
Hammond et al. (1999), who attempted to enhance adherence to a joint protection program for people with arthritis, believed to be enhanced by fostering self-efficacy for this task, similarly included goal setting, contracting, modeling, homework programs, and recall enhancing methods in the implementation of that program. As supported by motor learning principles, these joint protection strategies were carried out incrementally, which is an important concept in building self-efficacy. As proposed by Bandura (1977), the learning process employed to build the patient’s confidence also involved a composite of verbal, visual, and kinesthetic instructions, supported by extrinsic feedback on performance achievements. In addition, subjects used mental imagery techniques and practiced in pairs or threes to improve skill acquisition. Finally, to promote generality of the motor learning experiences and self-efficacy expectations—the belief that the outcome of the behaviors will yield a specific result—attained under supervision in the investigator’s laboratory to the home environment, self-management and self-monitoring strategies were used. In agreement with the acknowledged role of encouragement and persuasion in enhancing self-efficacy beliefs, support for the desired changes was enhanced by inviting patient’s partners or significant others to attend the classes. The partners or significant others were asked by the investigator to help promote the patient’s use of the recommended novel practices at home and to assist with any required home modifications. The program and follow-up measures were implemented for only a short duration, however, and hence more powerful effects that might have accrued in the long-term might have been overlooked, in light of the challenges experienced on a day-to-day basis by this patient group, and the ability to learn a new skill in the face of pain, numerous task demands, and physical disablement.
More recently, Hammond and Freeman (2001) extended their ideas to helping their patients to acquire confidence in hand-joint protection methods by providing participants with a range of options for task performance, so that patients could select those methods they felt would work best for them. Again, a step-by-step approach was used, whereby practice started with blocked repetitions of single actions and progressed to sequences of activities requiring multiple joint protection methods. Mental rehearsal was included, as were contracting and goal-setting strategies designed to promote practice of joint protection at home between meetings. Participants were encouraged to write their goals in workbooks, and feedback was given on progress and problems at the beginning of each meeting. Individual’s practical problems were also discussed and group members used problem-solving methods to generate solutions.
In previous research, Alderson et al. (1999) developed an equally successful integrated group education and individualized treatment program using principles of self-management, adult learning, case management, and self-efficacy enhancement. The outcomes of the program suggested this combined approach is a very potent one.
Resnick (2002a) who conducted research to better understand the factors that can influence the efficacy beliefs of older adults as regards being motivated to participate in a rehabilitation program identified 11 major themes amenable to intervention. These included the following: motivation and verbal encouragement, having exposure to positive role models, being able to deal effectively with patient’s past experiences, and current aversive physical sensations.
Additional research has shown that for purposes of enhancing pain self-efficacy, a problem of major concern to all patients who suffer from arthritis: (1) the clinician should assess the extent of pain experienced by a patient during a demanding activity; (2) they should train the individual in pain reduction skills through relaxation, distraction, or imagery; (3) they should have the patient repeat the demanding activity while applying the acquired pain reduction skills and monitor the improvements in pain that result (O’Leary et al., 1988). In addition to educating patients to better manage pain, educating them to cope with disease flares and any disease progression, helping them to understand why and how emotional reactions can affect their disease status, may be of additional value in helping to increase a patient’s repertoire of coping responses (Barlow et al., 2002). Moreover, structuring exercise treatments in such a way that mastery experiences and positive feedback are maximized is recommended (Jerome et al., 2002).
Furthermore, cognitive-behavioral interventions designed to affect the perceptions of control and the individual’s coping patterns (Hammond and Freeman, 2006; Sinclair et al., 1998), along with coping skills training and related educational interventions, are found to enhance arthritis self-efficacy with respect to mood and fatigue, physical capacity, pain, disability, and function (Keefe et al., 1996; Lorig et al., 1989; Smarr et al., 1997; Stenstrom, 1994).
Additional evidence suggests, a sound patient–therapist relationship that permits mutual inquiry, information-giving, problem solving, and the negotiation of activity goals may foster a patient’s sense of confidence, as may setting short-term, rather than long-term goals for some desired achievement (Bandura and Schunk, 1981; Jensen and Lorish, 1994). That is, implementing a series of modest progressive behavioral changes over short time periods is more likely to result in observable increases in task self-efficacy than unrealistic long-term goals that do not incorporate well-designed successive action steps (Bandura and Simon, 1977; Jensen and Lorish, 1994), and achievable sub-goals. Starting with the easiest task or the task most likely to be successful is also indicated here, as are mastery aids that can be gradually withdrawn, plus role plays and homework (Lorig, 1986). Furthermore, practicing activities in venues and situations that closely approximate the actual activities patients need to perform in their daily lives may be helpful (Gage and Polatajko, 1994).
However, because an individual is less likely to perform an activity if they feel less than confident of achieving success, the role of prior negative experiences should be addressed early on, and a constructive plan of action developed to permit the patient to overcome any perceived barriers in this respect (Barlow et al., 1998).
In sum, many practical strategies exist to assist the clinician in raising the self-efficacy beliefs of individuals with various forms of arthritis. One or more of these approaches if thoughtfully applied have been found to foster better health outcomes than those achieved with standard practices of care.
Discussion
Self-efficacy, contextualized in this review as personal beliefs likely to be of immense importance in the context of influencing health outcomes among people with chronic illnesses such as arthritis and representing the strength to which one has the confidence to undertake a specific task, under a variety of conditions, is a well-accepted theme in the psychology literature. Given the accepted understanding that arthritis has both physical and psychological ramifications, this present review was undertaken to validate whether self-efficacy beliefs can either help to explain a significant degree of the overall attendant disability experienced by a person diagnosed as having arthritis, regardless of pathology, and if heightening self-efficacy perceptions is consistently accompanied by related improvements in disability outcomes, regardless of type of arthritis condition studied. In this respect, specifically examined were past and recent evidence linking the magnitude of the perceived self-efficacy scores of a variety of arthritis patient sub-groups and related disease manifestations, both those physical and cognitive, as well as functional and behavioral.
Although much of the related research remains cross-sectional, and thus no cause–effect relationship can be deduced despite findings that denote there is significant association between the extent of one’s self-efficacy beliefs and selected arthritis manifestations, prospective studies strongly support the view that regardless of numbers of affected joints, joint sites, or arthritis diagnosis, the role that self-efficacy perceptions or beliefs may play in mediating or moderating arthritis outcomes should not be ignored. In this respect, the present findings also concur with those of Primdahl et al. (2011b) who concluded self-efficacy scores assessed using the arthritis self-efficacy scale seem to be highly associated with physical disease-related variables in people with arthritis, regardless of study approach, evaluation tool, or sample studied. They also support the view of Dekker et al. (2009) that low self-efficacy is a risk factor for functional declines in cases with hip osteoarthritis.
Furthermore, several reports specifically indicate a strong relationship between levels of perceived self-efficacy and self-management behaviors (Prior and Bond, 2004), and adherence with exercise regimens (Brus et al., 1997; McAuley et al., 2003; Oliver and Cronan, 2002; Stenstrom, 1994), management approaches of great import to the preservation of joint health and general well-being of people with arthritis, regardless of form. Other findings show levels of perceived self-efficacy are negatively correlated with several commonly debilitating arthritis-related outcomes, such as fatigue and pain, and depression (see Table 5), but that bolstering a patient’s self-efficacy may help them to maintain an optimal level of physical function, despite the progressive nature of most of these diseases (Belza et al., 2002; Bent et al., 2001; Brassington et al., 2002; Oliver and Cronan, 2002). In particular, enhancing exercise self-efficacy, which is associated with exercise adherence (Gecht et al., 1996; McAuley et al., 2003; Oliver and Cronan, 2002) appears important for sustaining initial program benefits (Stenstrom, 1994) and physical activity goal achievement (Knittle et al., 2011).
Other research shows efforts to impact self-efficacy that lead to improvements in physical functioning are likely to yield significant early and sustained treatment benefits including the ability to manage arthritis pain and improved psychological well-being (Barlow et al., 1998; Holman et al., 1989). Importantly, these observed improvements are likely to be commensurate with those obtained by arthritis medications, while reducing utilization of, and dependency upon, health-care services (Lorig et al., 1993). Such outcomes, could in turn, reduce individual suffering as well as the collective societal burden of the disease, improve an affected individual’s life quality quite positively, and lessen current demands on an already overburdened health-care system. Tailored in light of an individual’s age, gender, ethnicity, health condition, socioeconomic status, and personal goals, carefully designed and implemented self-efficacy building interventions could permit people with arthritis to continue to be actively employed and independent, rather than dependent. In addition to the far-reaching economic consequences of this outcome, being able to work, which has enormous emotional health, physical health, and social implications, would in all likelihood prove highly efficacious (see Figure 2).
By contrast, arthritis patients with low perceived self-efficacy are likely to experience poor health outcomes, especially excessive pain (Daltroy 1993; Heiberg and Kvien, 2002; Somers et al., 2009a), physical disability, psychological disability (Shelby et al., 2008), and deleterious eating behaviors that lead to overeating and overweight (Pells et al., 2008). Furthermore, one can expect higher health-care costs (Walen et al., 2001).
It should be noted, though, that to be most efficacious, efforts to enhance self-efficacy among people with arthritis may need to be implemented over a long period of time, rather than a short period of time, and include different strategies for fostering different categories and degrees of task-related and symptom management confidence perceptions. Although it is unclear what specific approach is likely to prove optimal in heightening an individual’s arthritis self-efficacy level, the clinician should carefully select the intervention method(s) that will most closely achieve the desired outcomes for a given individual, in light of their disease presentation, and self-efficacy perceptions, and concentrate on those patients whose self-efficacy is weak in specific key self-management areas (Makelainen et al., 2009).
Conclusion
Arthritis, in any of its forms, is an extremely debilitating disease that requires a considerable degree of personal management. In this regard, a large volume of research strongly implies that optimally enhancing an individual patient’s perceived self-efficacy beliefs can be highly influential in fostering behaviors critical to an efficacious self-management process. Although no definitive conclusions can be reached in respect to either the frequency, duration, and intensity of interventions that will foster self-efficacy among people with arthritis, this review strengthens the basic support for this approach, and highlights the variety of ways Albert Bandura’s research can be applied to improve arthritis outcomes.
In the counseling domain, the present findings suggest that routinely assessing self-efficacy, which is easy to measure, and intervening accordingly thereafter, as indicated, is strongly recommended prior to simply communicating directives for a progressive series of weight reduction and dietary changes, as well as exercise and related health recommendations. To this end, making the importance of basic self-efficacy estimates in the context of arthritis treatment more visible in guidelines for standard care practices designed to enhance arthritis outcomes is also indicated. To foster confidence needed to achieve optimal arthritis health outcomes, careful assessment of factors influencing self-efficacy perceptions, such as prior experiences, extent of disease, availability of resources, and social support, followed by appropriately tailored self-efficacy enhancing strategies as outlined in this review to achieve mastery may be helpful, as indicated. Periodic re-assessments and a long-term, rather than a short-term, therapeutic relationship are deemed highly desirable in this respect, as is a mutual decision-making and communication process between the provider and patient.
Due to the very diverse nature of this body of literature, future research to examine the role of self-efficacy in mediating or moderating functional, social, emotional, and physical outcomes in specific arthritis sub-groups using random sampling, well-defined inclusion criteria, and validated instruments along with well-designed long-term prospective studies would be most helpful. Well-controlled intervention study comparisons testing whether theory-based approaches are more useful than nontheoretical approaches using validated outcome measures are also strongly indicated.
Footnotes
Declaration of conflicting interests: The author declares that there is no conflict of interest.
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
- Alderson M, Starr L, Gow S, et al. (1999) The program for rheumatic independent self-management: A pilot evaluation. Clinical Rheumatology 18: 283–292. [DOI] [PubMed] [Google Scholar]
- Allegrante JP, Kovar PA, Mackenzie CR, et al. (1993) A walking education program for patients with osteoarthritis of the knee: Theory and intervention strategies. Health Education Quarterly 20: 63–81. [DOI] [PubMed] [Google Scholar]
- Allen KD, Oddone EZ, Coffman CJ, et al. (2010) Racial differences in osteoarthritis pain and function: Potential explanatory factors. Osteoarthritis and Cartilage 18(2): 160–167. [DOI] [PubMed] [Google Scholar]
- Alok R, Das SK, Agarwal GG, et al. (2014) Problem-focused coping and self-efficacy as correlates of quality of life and severity of fibromyalgia in primary fibromyalgia patients. Journal of Clinical Rheumatology 20(6): 314–316. [DOI] [PubMed] [Google Scholar]
- Arnstein P. (2000) The mediation of disability by self efficacy in different samples of chronic pain patients. Disability and Rehabilitation 20: 794–801. [DOI] [PubMed] [Google Scholar]
- Arthritis and Related Conditions (2011) Chapter 4. Available at: http://www.boneandjointburden.org/pdfs/BMUS_chpt4_arthritis.pdf (accessed 9 November 2014).
- Bandura A. (1977) Social Learning Theory. Englewood Cliffs, NJ: Prentice Hall. [Google Scholar]
- Bandura A. (1986a) Self-efficacy mechanism in physiological activation and health promoting behavior. In: Madden J, Matthysse S, Barchas J. (Eds.). Adaptation, Learning and Affect. New York: Raven Press. [Google Scholar]
- Bandura A. (1986b) Social Foundations of Thought and Action: A Social Cognitive Theory. Englewood Cliffs, NJ: Prentice Hall. [Google Scholar]
- Bandura A. (1994) Social cognitive theory and exercise of control over HIV infection. In: DiClemente R, Peterson JL. (eds) Preventing AIDS: Theories and Methods. New York: Plenum Press, pp. 25–59. [Google Scholar]
- Bandura A. (1997) Self-Efficacy: The Exercise of Control. New York: W.H. Freeman and Company, p. 3. [Google Scholar]
- Bandura A, Schunk DH. (1981) Cultivating competence, self-efficacy, and intrinsic interest through proximal self-motivation. Journal of Personality and Social Psychology 41: 586–598. [Google Scholar]
- Bandura A, Simon KM. (1977) The role of proximal intentions in self-regulation of refractory behavior. Cognitive Therapy and Research 1: 177–198. [Google Scholar]
- Barlow JH. (1998) Understanding exercise in the context of chronic disease: An exploratory investigation of self-efficacy. Perceptual and Motor Skills 87: 439–446. [DOI] [PubMed] [Google Scholar]
- Barlow JH, Barefoot J. (1996) Group education for people with arthritis. Patient Education and Counseling 27: 257–267. [DOI] [PubMed] [Google Scholar]
- Barlow JH, Cullen LA, Rowe IF. (2002) Educational preferences, psychological well-being and self-efficacy among people with rheumatoid arthritis. Patient Education and Counseling 46: 11–19. [DOI] [PubMed] [Google Scholar]
- Barlow JH, Turner AP, Wright CC. (1998) Long-term outcomes of an arthritis self-management programme. British Journal of Rheumatology 37: 1315–1319. [DOI] [PubMed] [Google Scholar]
- Barlow JH, Williams B, Wright CC. (1999) ‘Instilling the strength to fight the pain and get on with life’: Learning to become an arthritis self-manager through an adult education programme. Health Education Research 14: 533–544. [DOI] [PubMed] [Google Scholar]
- Baruth M, Wilcox S, Schoffman DE, et al. (2013) Factors associated with disability in a sample of adults with arthritis. Disability and Health Journal 6(4): 377–384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baruth M, Wilcox S, Sharpe PA, et al. (2014) Baseline predictors of physical activity in a sample of adults with arthritis participating in a self-directed exercise program. Public Health 128: 834–841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beckham JC, Burker EJ, Rice JR, et al. (1995) Patient predictors of caregiver burden, optimism and pessimism in rheumatoid arthritis. Behavioral Medicine 20: 171–178. [DOI] [PubMed] [Google Scholar]
- Belza B, Topolski T, Kinne S, et al. (2002) Does adherence make a difference? Results from a community-based aquatic exercise program. Nursing Research 51: 285–291. [DOI] [PubMed] [Google Scholar]
- Benka J, Nagyova I, Rosenberger J, et al. (2014) Is coping self-efficacy related to psychological distress in early and established rheumatoid arthritis patients? Journal of Developmental and Physical Disabilities 26(3): 285–297. [Google Scholar]
- Bent N, Jones A, Molley I, et al. (2001) Factors determining participation in young adults with a physical disability: A pilot study. Clinical Rehabilitation 15: 552–561. [DOI] [PubMed] [Google Scholar]
- Benyon K, Hill S, Zadurian N, et al. (2010) Coping strategies and self-efficacy as predictors of outcome in osteoarthritis: A systematic review. Musculoskeletal Care 8: 224–236. [DOI] [PubMed] [Google Scholar]
- Berarducci A, Lengacher CA. (1998) Self-efficacy: An essential component of advanced-practice nursing. Nursing Connections 11: 55–67. [PubMed] [Google Scholar]
- Blamey R, Jolly K, Greenfield S, et al. (2009) Patterns of analgesic use, pain and self-efficacy: A cross-sectional study of patients attending a hospital rheumatology clinic. BMC Musculoskeletal Disorders 10: 137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blazer DG. (2002) Self-efficacy and depression in late life: A primary prevention proposal. Aging & Mental Health 6: 315–324. [DOI] [PubMed] [Google Scholar]
- Bolen J, Schieb L, Hootman JM, et al. (2010) Differences in the prevalence and impact of arthritis among racial/ethnic groups in the United States, National Health Interview Survey, 2002, 2003, and 2006. Prevention and Chronic Disease 7(3): A64. [PMC free article] [PubMed] [Google Scholar]
- Braden CJ, McGlone K, Pennington F. (1993) Specific psychosocial and behavioral outcomes from the systemic lupus erythematosus self-help course. Health Education Quarterly 20: 29–41. [DOI] [PubMed] [Google Scholar]
- Brassington GS, Atienza AA, Perczek RE, et al. (2002) Intervention-related cognitive versus social mediators of exercise adherence in the elderly. American Journal of Preventive Medicine 23(2 Suppl.): 80–86. [DOI] [PubMed] [Google Scholar]
- Brekke M, Hjortdahl P, Kvien TK. (2001) Self-efficacy and health status in rheumatoid arthritis: A two-year longitudinal observational study. Rheumatology 40: 387–392. [DOI] [PubMed] [Google Scholar]
- Brekke M, Hjortdahl P, Kvien TK. (2003) Changes in self-efficacy and health status over 5 years: A longitudinal observational study of 306 patients with rheumatoid arthritis. Arthritis Rheumatism 15: 342–348. [DOI] [PubMed] [Google Scholar]
- Broderick JE, Junghaenel DU, Schneider S, et al. (2011) Treatment expectation for pain coping skills training: Relationship to osteoarthritis patients’ baseline psychosocial characteristics. Clinical Journal of Pain 27: 315–322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brus H, van de Laar M, Taal E, et al. (1997) Determinants of compliance with medication in patients with rheumatoid arthritis: The importance of self-efficacy expectations. Patient Education and Counseling 36: 57–64. [DOI] [PubMed] [Google Scholar]
- Buckelew SP, Parker JC, Keefe FJ, et al. (1994) Self-efficacy and pain behavior among subjects with fibromyalgia. Pain 59: 377–384. [DOI] [PubMed] [Google Scholar]
- Buescher KL, Johnston JA, Parker JC, et al. (1991) Relationship of self-efficacy to pain behavior. Journal of Rheumatology 18: 968–972. [PubMed] [Google Scholar]
- Callahan LF, Shreffler JH, Altpeter M, et al. (2011) Evaluation of group and self-directed formats of the Arthritis Foundation’s Walk With Ease Program. Arthritis Care and Research 63(8): 1098–1107. [DOI] [PubMed] [Google Scholar]
- Cramm JM, Strating MM, Nieboer AP. (2013) The importance of general self-efficacy for the quality of life of adolescents with diabetes or juvenile rheumatoid arthritis over time: A longitudinal study among adolescents and parents. Frontiers in Pediatrics 20(1): 40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cross MJ, March LM, Lapsley HM, et al. (2006) Patient self-efficacy and health locus of control: Relationships with health status and arthritis-related expenditure. Rheumatology 45(1): 92–96. [DOI] [PubMed] [Google Scholar]
- Daltroy LH. (1993) Doctor-patient communication in rheumatological disorders. Ballieres Clinical Rheumatology 7: 221–239. [DOI] [PubMed] [Google Scholar]
- Davis GC. (2003) Improved sleep may reduce arthritis pain. Holistic Nursing Practice 17: 128–135. [DOI] [PubMed] [Google Scholar]
- Davis P, Busch A, Lowe J, et al. (1994) Evaluation of a rheumatoid arthritis education program: Impact on knowledge and self-efficacy. Patient Education and Counseling 24: 55–61. [DOI] [PubMed] [Google Scholar]
- De Boer IG, Peeters AJ, Ronday HK, et al. (2009) Assistive devices: Usage in patients rheumatoid arthritis. Clinical Rheumatology 28: 119–928. [DOI] [PubMed] [Google Scholar]
- Dekker J, Van Dijk GM, Veenhof C. (2009) Risk factors for functional decline in osteoarthritis of the hip or knee. Current Opinion in Rheumatology 21: 520–524. [DOI] [PubMed] [Google Scholar]
- Deng W, Hu J. (2013) The effects of a pilot intervention for community-dwelling adults with rheumatoid arthritis in Wuhan, China. Frontiers of Public Health 10(1): 43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Der Ananian C, Wilcox S, Watkins K, et al. (2008) Factors associated with exercise participation in adults with arthritis. Journal of Aging and Physical Activity 16: 125–143. [DOI] [PubMed] [Google Scholar]
- Dirik G, Karanci AN. (2009) Psychological distress in rheumatoid arthritis patients: An evaluation within the conservation of resources theory. Psychology & Health 25(5): 617–632. [DOI] [PubMed] [Google Scholar]
- Dwyer KA. (1997) Psychosocial factors and health status in women with rheumatoid arthritis: Predictive models. American Journal of Preventive Medicine 13: 66–72. [PubMed] [Google Scholar]
- Evans S, Moieni M, Lung K, et al. (2013) Impact of iyengar yoga on quality of life in young women with rheumatoid arthritis. Clinical Journal of Pain 29(11): 988–997. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Focht BC, Rejeski WJ, Ambosius WT, et al. (2005) Exercise, self-efficacy, and mobility performance in overweight and obese older adults with knee osteoarthritis. Arthritis & Rheumatism 53: 659–665. [DOI] [PubMed] [Google Scholar]
- Gage M, Polatajko H. (1994) Enhancing occupational performance through an understanding of perceived self-efficacy. American Journal of Occupational Therapy 48: 452–461. [DOI] [PubMed] [Google Scholar]
- Gaines JM, Talbot LA, Metter EJ. (2002) The relationship of arthritis self-efficacy to functional performance in older men and women with osteoarthritis of the knee. Geriatric Nursing 23: 167–170. [DOI] [PubMed] [Google Scholar]
- Garnefski N, Kraaij V, Benoist M, et al. (2013) Effect of a cognitive behavioral self-help intervention on depression, anxiety, and coping self-efficacy in people with rheumatic disease. Arthritis Care and Research 65(7): 1077–1084. [DOI] [PubMed] [Google Scholar]
- Gecht MR, Connell KJ, Sinacore JM, et al. (1996) A survey of exercise beliefs and exercise habits among people with arthritis. Arthritis Care and Research 9: 82–88. [DOI] [PubMed] [Google Scholar]
- Greene BL, Haldeman GF, Kaminski A, et al. (2006) Factors affecting physical activity behavior in urban adults with arthritis who are predominantly African-American and female. Physical Therapy 86: 510–519. [PubMed] [Google Scholar]
- Grønning K, Skomsvoll JF, Rannestad T, et al. (2012) The effect of an educational programme consisting of group and individual arthritis education for patients with polyarthritis—A randomised controlled trial. Patient Education and Counseling 88(1): 113–120. [DOI] [PubMed] [Google Scholar]
- Guo L, Yang H, Malkin MM. (2009) Self-efficacy and arthritis impact on health: The effect of an Arthritis Foundation Aquatic Program. American Journal of Recreational Therapy 8: 9–19. [Google Scholar]
- Gyurcsik NC, Brawley LR, Sprink KS, et al. (2009) Physical activity in women with arthritis: Examining perceived barriers and self-regulatory efficacy to cope. Arthritis and Rheumatism 61: 1087–1094. [DOI] [PubMed] [Google Scholar]
- Gyurcsik NC, Brawley LR, Spink KS, et al. (2013) Meeting physical activity recommendations: Self-regulatory efficacy characterizes differential adherence during arthritis flares. Rehabilitation Psychology 58(1): 43–50. [DOI] [PubMed] [Google Scholar]
- Gyurcsik NC, Estabrooks PA, Frahm-Templar MJ. (2003) Exercise-related goals and self-efficacy as correlates of aquatic exercise in individuals with arthritis. Arthritis and Rheumatism 49: 306–313. [DOI] [PubMed] [Google Scholar]
- Hammond A, Freeman K. (2001) One-year outcomes of a randomized controlled trial of an educational-behavioral joint protection programme for people with rheumatoid arthritis. Rheumatology 40: 1044–1051. [DOI] [PubMed] [Google Scholar]
- Hammond A, Freeman K. (2006) Community patient education and exercise for people with fibromyalgia: A parallel group randomized controlled trial. Clinical Rehabilitation 20: 835–846. [DOI] [PubMed] [Google Scholar]
- Hammond A, Lincoln N, Sutcliffe L. (1999) A crossover trial evaluating an educational-behavioral joint protection programme for people with rheumatoid arthritis. Patient Education and Counseling 37: 19–32. [DOI] [PubMed] [Google Scholar]
- Harrison AL. (2004) The influence of pathology, pain, balance, and self-efficacy on function in women with osteoarthritis of the knee. Physical Therapy 84: 822–831. [PubMed] [Google Scholar]
- Heiberg T, Kvien TK. (2002) Preferences for improved health examined in 1,024 patients with rheumatoid arthritis: Pain has highest priority. Arthritis and Rheumatism 15: 391–397. [DOI] [PubMed] [Google Scholar]
- Hewlett S, Ambler N, Almeida C, et al. (2011) Self-management of fatigue in rheumatoid arthritis: A randomised controlled trial of group cognitive-behavioural therapy. Annals of the Rheumatic Diseases 70: 1060–1067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heye ML, Foster L, Bartlett MK, et al. (2002) A preoperative intervention for pain reduction, improved mobility, and self-efficacy. Applied Nursing Research 15: 174–183. [DOI] [PubMed] [Google Scholar]
- Holman H, Mazonson P, Lorig K. (1989) Health education for self-management has significant early and sustained benefits in chronic arthritis. Transactions of the Association of American Physicians 102: 204–208. [PubMed] [Google Scholar]
- Hopman-Rock M, Westhoff MH. (2000) The effects of a health educational and exercise program for older adults with osteoarthritis of the hip or knee. Journal of Rheumatology 27: 1947–1954. [PubMed] [Google Scholar]
- Huffman K, Pieper C, Hall K, et al. (2014) Self-efficacy for exercise, more than disease-related factors, is associated with objectively assessed exercise time and sedentary behaviour in rheumatoid arthritis. Scandinavian Journal of Rheumatology 15: 1–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hutton I, Gamble G, McLean G, et al. (2009) What is associated with being active in arthritis? Analysis from the Obstacles to Action study. Internal Medicine Journal. Epub ahead of print 21 May. DOI: 10.1111/j.1445-5994.2009.01989.x. [DOI] [PubMed] [Google Scholar]
- Jensen GM, Lorish CDP. (1994) Promoting patient cooperation with exercise programs. Linking research, theory and practice. Arthritis Care and Research 7: 181–189. [DOI] [PubMed] [Google Scholar]
- Jensen MP, Turner JA, Romano JM, et al. (1991) Coping with chronic pain: A critical review of the literature. Pain 47: 249–283. [DOI] [PubMed] [Google Scholar]
- Jerome GJ, Marquez DX, McAuley E, et al. (2002) Efficacy effects on feeling states in women. International Journal of Behavioral Medicine 9: 139–154. [DOI] [PubMed] [Google Scholar]
- Keefe FJ, Caldwell DS, Baucom D, et al. (1996) Spouse assisted coping skills training in the management of osteoarthritic knee pain. Arthritis Care and Research 9: 279–291. [DOI] [PubMed] [Google Scholar]
- Keefe FJ, Lefebvre JC, Kerns RD, et al. (2000) Understanding the adoption of arthritis self-management: Stages of change profiles among arthritis patients. Pain 87: 303–313. [DOI] [PubMed] [Google Scholar]
- Keefe FJ, Lefebvre JC, Maixner W, et al. (1997a) Self-efficacy for arthritis pain: Relationship to perception of thermal laboratory pain stimuli. Arthritis Care and Research 10: 177–184. [DOI] [PubMed] [Google Scholar]
- Keefe FJ, Susmita KZ, Robinson E, et al. (1997b) Pain coping strategies that predict patients’ and spouses’ ratings of patients’ self-efficacy. Pain 73: 191–199. [DOI] [PubMed] [Google Scholar]
- Knittle KP, De Gucht V, Hurkmans EJ, et al. (2011) Effect of self-efficacy and physical activity goal achievement on arthritis pain and quality of life in patients with rheumatoid arthritis. Arthritis Care Research 63: 1613–1619. [DOI] [PubMed] [Google Scholar]
- Kovar PA, Allegrante JP, MacKenzie CR, et al. (1992) Supervised fitness walking in patients with osteoarthritis of the knee: A randomized, controlled trial. Annals of Internal Medicine 116: 529–534. [DOI] [PubMed] [Google Scholar]
- Lamb SE, Toye F, Barker KL. (2008) Chronic disease management programme in people with severe knee osteoarthritis: Efficacy and moderators of response. Clinical Rehabilitation 22: 169–178. [DOI] [PubMed] [Google Scholar]
- Landa-Gonzalez B, Molnar D. (2012) Occupational therapy intervention: Effects on self-care, performance, satisfaction, self-esteem/self-efficacy, and role functioning of older Hispanic females with arthritis. Occupational Therapy and Health Care 26(2–3): 109–119. [DOI] [PubMed] [Google Scholar]
- Larkin L, Kennedy N. (2013) Correlates of physical activity in adults with rheumatoid arthritis: A systematic review. Journal of Physical Activity and Health. Epub ahead of print 19 August. DOI: 10.1123/jpah.2012-0194. [DOI] [PubMed] [Google Scholar]
- Lee HY, Hale CA, Hemingway B, et al. (2013) Tai Chi exercise and auricular acupressure for people with rheumatoid arthritis: An evaluation study. Journal of Clinical Nursing 21(19–20): 2812–2822. [DOI] [PubMed] [Google Scholar]
- Leung YY, Kwan J, Chan P, et al. (2014) A pilot evaluation of Arthritis Self-Management Program by lay leaders in patients with chronic inflammatory arthritis in Hong Kong. Clinical Rheumatology. Epub ahead of print 8 October. DOI: 10.1007/s10067-014-2791-z. [DOI] [PubMed] [Google Scholar]
- Leveille SG, Cohen-Mansfield J, Guralnik JM. (2003) The impact of chronic musculoskeletal pain on exercise attitudes, self-efficacy, and physical activity. Journal of Aging and Physical Activity 11: 275–283. [Google Scholar]
- Lorig K. (1986) A short guide to self-efficacy. Arthritis Health Professional Association 21st annual scientific meeting, New Orleans, LA, 3–7 June. [Google Scholar]
- Lorig K, Gonzalez V. (1992) The integration with practice: A 12-year case study. Health Education Quarterly 19: 355–368. [DOI] [PubMed] [Google Scholar]
- Lorig K, Holman H. (1993) Arthritis self-management studies: A twelve year review. Health Education Quarterly 20: 17–28. [DOI] [PubMed] [Google Scholar]
- Lorig K, Chastain RL, Ung E, et al. (1989) Development and evaluation of a scale to measure perceived self-efficacy in people with arthritis. Arthritis and Rheumatism 32: 37–44. [DOI] [PubMed] [Google Scholar]
- Lorig K, Gonzalez VM, Laurent DD, et al. (1998) Arthritis self-management program variations: Three studies. Arthritis Care and Research 11: 448–454. [DOI] [PubMed] [Google Scholar]
- Lorig K, Mazonson PD, Holman H. (1993) Evidence suggesting that health education for self-management in patients with chronic arthritis has sustained health benefits while reducing health care costs. Arthritis and Rheumatism 36: 439–446. [DOI] [PubMed] [Google Scholar]
- Loucks-Atkinson A. (2007) Role of self-efficacy in the constraints negotiation process: The case of individuals with Fibromyalgia syndrome. Leisure Sciences 29: 19–36. [Google Scholar]
- Lowe R, Cockshott Z, Greenwood R, et al. (2008) Self-efficacy as an appraisal that moderates the coping-emotion relationship: Associations among people with rheumatoid arthritis. Psychology & Health 23: 155–174. [DOI] [PubMed] [Google Scholar]
- McAuley E, Jerome GJ, Elavsky S, et al. (2003a) Predicting long-term maintenance of physical activity in older adults. Preventive Medicine 37: 110–118. [DOI] [PubMed] [Google Scholar]
- McCarron A. (2014) An exploration of the perceived effects of a support group for individuals with rheumatoid arthritis. Journal of the American Association of Nurse Practitioners. Epub ahead of print 2 July. DOI: 10.1002/2327-6924.12146. [DOI] [PubMed] [Google Scholar]
- McKnight PE, Afram A, Kashdan TB, et al. (2010) Coping self-efficacy as a mediator between catastrophizing and physical functioning: Treatment target selection in an osteoarthritis sample. Journal of Behavioral Medicine 33: 239–249. [DOI] [PubMed] [Google Scholar]
- Makelainen P, Vehvilaainen-Julkunen K, Pietil A. (2009) Change in knowledge and self-efficacy of patients with rheumatoid arthritis: A six-month follow-up study. International Journal of Nursing Practice 15: 368–375. [Google Scholar]
- Maly M, Costigan P, Olney S. (2005) Contribution of psychosocial and mechanical variables to mobility outcome measures in knee osteoarthritis. Physical Therapy 85: 1318–1328. [PubMed] [Google Scholar]
- Maly MR, Costigan PA, Olney SJ. (2006) Determinants of self-efficacy for physical tasks in people with knee osteoarthritis. Arthritis & Rheumatism 55: 94–101. [DOI] [PubMed] [Google Scholar]
- Manning VL, Hurley MV, Scott DL, et al. (2014) Education, self-management, and upper extremity exercise training in people with rheumatoid arthritis: A randomized controlled trial. Arthritis Care and Research 66(2): 217–227. [DOI] [PubMed] [Google Scholar]
- Marcum ZA, Zhan HL, Perera S, et al. (2014) Correlates of gait speed in advanced knee osteoarthritis. Pain Medicine 15(8): 1334–1342. [DOI] [PubMed] [Google Scholar]
- Marks R, Allegrante JP. (2007) Prevalence and impact of arthritis: Opportunities for prevention. Health Education Journal 66: 3–21. [Google Scholar]
- Martire LM, Schulz R, Keefe FJ, et al. (2003) Feasibility of a dyadic intervention for management of osteoarthritis: A pilot study with older patients and their spousal caregivers. Aging and Mental Health 7: 53–60. [DOI] [PubMed] [Google Scholar]
- Mendes de Leon CF, Seeman TE, Baker DI, et al. (1996) Self-efficacy, physical decline, and change in functioning in community-living elders: A prospective study. Journals of Gerontology Series B: Psychological Sciences and Social Sciences 51: S183–S190. [DOI] [PubMed] [Google Scholar]
- Mielenz TJ, Kubiak-Rizzone KL, Alvarez KJ, et al. (2013) Association of self-efficacy and outcome expectations with physical activity in adults with arthritis. Arthritis 2013(2013): 621396 (8 pp.). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Niedermann K, Buchi S, Ciurea A, et al. (2011) Six and 12 months’ effects of individual joint protection education in people with rheumatoid arthritis: A randomized controlled trial. Scandinavian Journal of Occupational Therapy. Epub ahead of print 22 September. DOI: 10.3109/11038128.2011.611820. [DOI] [PubMed] [Google Scholar]
- Nuñez DE, Keller C, Ananian CD. (2009) A review of the efficacy of the self-management model on health outcomes in community-residing older adults with arthritis. Worldviews Evidence Based Nursing 6: 130–148. [DOI] [PubMed] [Google Scholar]
- O’Leary A. (1985) Self-efficacy and health. Behavior Research and Therapy 23: 437–461. [DOI] [PubMed] [Google Scholar]
- O’Leary A, Schoor S, Lorig K, et al. (1988) A cognitive-behavioral treatment for rheumatoid arthritis. Health Psychology 7: 527–544. [DOI] [PubMed] [Google Scholar]
- Oliver K, Cronan T. (2002) Predictors of exercise behaviors among fibromyalgia patients. Preventive Medicine 35: 383–389. [DOI] [PubMed] [Google Scholar]
- Orengo CA, Wei SH, Molinari VA, et al. (2001) Functioning in rheumatoid arthritis: The role of depression and self-efficacy. Clinical Gerontologist 23: 45–56. [Google Scholar]
- Packham JC, Hall MA, Pimm TJ. (2002) Long-term follow-up of 246 adults with juvenile idiopathic arthritis: Predictive factors for mood and pain. Rheumatology 41: 1444–1449. [DOI] [PubMed] [Google Scholar]
- Pariser D, O’Hanlon A. (2005) Effects of telephone intervention on arthritis self-efficacy, depression, pain, and fatigue in older adults with arthritis. Journal of Geriatric Physical Therapy 28: 67–73. [PubMed] [Google Scholar]
- Pells JJ, Shelby RA, Keefe FJ, et al. (2008) Arthritis self-efficacy and self-efficacy for resisting eating: Relationships to pain, disability, and eating behavior in overweight and obese individuals with osteoarthritic knee pain. Pain 136: 340–347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piyakhachornrot N, Aree-Ue S, Putwatana P, et al. (2011) Impact of an integrated health education and exercise program in middle-aged Thai adults with osteoarthritis of the knee. Orthopedic Nursing 30: 134–142. [DOI] [PubMed] [Google Scholar]
- Porter LS, Keefe FJ, Wellington C, et al. (2008) Pain communication in the context of osteoarthritis: Patient and partner self-efficacy for pain communication and holding back from discussion of pain and arthritis related concerns. Clinical Journal of Pain 24: 662–668. [DOI] [PubMed] [Google Scholar]
- Primdahl J, Wagner L, Horselev-Petersen K. (2011a) Being an outpatient with rheumatoid arthritis-a focus group study on patient’s self-efficacy and experiences from participation in a short course and one of three different outpatient setting. Scandinavian Journal of Caring Sciences 25: 394–403. [DOI] [PubMed] [Google Scholar]
- Primdahl J, Wagner L, Hørslev-Petersen K. (2011b) Self-efficacy as an outcome measure and its association with physical disease-related variables in persons with rheumatoid arthritis: A literature review. Musculoskeletal Care. Epub ahead of print 10 June. DOI: 10.1002/msc.210. [DOI] [PubMed] [Google Scholar]
- Primdahl J, Wagner L, Holst R, et al. ; AMBRA Study Group (2012) The impact on self-efficacy of different types of follow-up care and disease status in patients with rheumatoid arthritis—A randomized trial. Patient Education and Counseling 88(1): 121–128. [DOI] [PubMed] [Google Scholar]
- Prior KN, Bond MJ. (2004) The roles of self-efficacy and abnormal illness behaviour in osteoarthritis self-management. Psychology Health & Medicine 9(2): 177–192. [Google Scholar]
- Rapley P, Fruin DJ. (1999) Self-efficacy in chronic illness: The juxtaposition of general and regimen-specific efficacy. International Journal of Nursing Practice 5(4): 209–215. [DOI] [PubMed] [Google Scholar]
- Rayahin JE, Chmiel JS, Hayes KW, et al. (2014) Factors associated with pain experience outcome in knee osteoarthritis. Arthritis Care and Research. Epub ahead of print 21 July. DOI: 10.1002/acr.22402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinseth L, Uhlig T, Kjeken I, et al. (2011) Performance in leisure-time physical activities and self-efficacy in females with rheumatoid arthritis. Scandinavian Journal of Occupational Therapy 18: 210–218. [DOI] [PubMed] [Google Scholar]
- Rejeski WJ, Craven T, Ettinger WH, Jr, et al. (1996) Self-efficacy and pain in disability with osteoarthritis of the knee. Journals of Gerontology Series B: Psychological Sciences and Social Sciences 51: 24–29. [DOI] [PubMed] [Google Scholar]
- Rejeski WJ, Ettinger WH, Martin K, et al. (1998) Treating disability in knee osteoarthritis with exercise therapy: A central role for self-efficacy and pain. Arthritis Care and Research 11: 94–101. [DOI] [PubMed] [Google Scholar]
- Rejeski WJ, Miller ME, Foy C, et al. (2001) Self-efficacy and the progression of functional limitations and self-reported disability in older adults with knee pain. Journals of Gerontology Series B: Psychological Sciences and Social Sciences 56: S261–S265. [DOI] [PubMed] [Google Scholar]
- Resnick B. (2002a) Geriatric rehabilitation: The influence of efficacy beliefs and rehabilitation. Rehabilitation Nursing 27: 152–159. [DOI] [PubMed] [Google Scholar]
- Resnick B. (2002b) Testing the effect of the WALC intervention on exercise adherence in older adults. Journal of Gerontology Nursing 28: 40–49. [DOI] [PubMed] [Google Scholar]
- Riemsma RP, Rasker JJ, Taal E, et al. (1998) Fatigue in rheumatoid arthritis: The role of self-efficacy and problematic social support. British Journal of Rheumatology 37: 1042–1046. [DOI] [PubMed] [Google Scholar]
- Schoster B, Callahan LF, Meier A, et al. (2005) The People with Arthritis Can Exercise (PACE) program: A qualitative evaluation of participant satisfaction. Preventing Chronic Disease 2: A11. [PMC free article] [PubMed] [Google Scholar]
- Seid M, Huang B, Niehaus S, et al. (2014) Determinants of health-related quality of life in children newly diagnosed with juvenile idiopathic arthritis. Arthritis Care Research 66(2): 263–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharma L, Cahue S, Song J, et al. (2003) Physical functioning over three years in knee osteoarthritis: Role of psychosocial, local mechanical, and neuromuscular factors. Arthritis and Rheumatism 48: 3359–3370. [DOI] [PubMed] [Google Scholar]
- Shelby RA, Somera TJ, Keefe FJ, et al. (2008) Domain specific self-efficacy mediates the impact of pain catastrophizing on pain and disability in overweight and obese adults. Pain 9: 912–919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shigaki CL, Smarr KL, Siva C, et al. (2013) RAHelp: An online intervention for individuals with rheumatoid arthritis. Arthritis Care and Research 65(10): 1573–1581. [DOI] [PubMed] [Google Scholar]
- Sinclair VG, Wallston KA, Dwyer KA, et al. (1998) Effects of a cognitive-behavioral intervention for women with rheumatoid arthritis. Research Health Nursing 21: 315–326. [DOI] [PubMed] [Google Scholar]
- Sinikallio SH, Helminen EE, Valjakka AL, et al. (2014) Multiple psychological factors are associated with poorer functioning in a sample of community-dwelling knee osteoarthritis patients. Journal of Clinical Rheumatology 20(5): 261–267. [DOI] [PubMed] [Google Scholar]
- Sirois FM, Hirsch JK. (2013) Associations of psychological thriving with coping efficacy, expectations for future growth, and depressive symptoms over time in people with arthritis. Journal of Psychosomatic Research 75((3): 279–286. [DOI] [PubMed] [Google Scholar]
- Smarr KL, Parker JC, Wright GE, et al. (1997) The importance of enhancing self-efficacy in rheumatoid arthritis. Arthritis Care and Research 10: 18–26. [DOI] [PubMed] [Google Scholar]
- Somers TJ, Keefe FJ, Godiwala N, et al. (2009a) Psychosocial factors and the pain experience of osteoarthritis patients: New findings and new directions. Current Opinion in Rheumatology 21: 501–506. [DOI] [PubMed] [Google Scholar]
- Somers TJ, Keefe FJ, Pells JJ, et al. (2009b) Pain catastrophizing and pain-related fear in osteoarthritis patients: Relationships to pain and disability. Journal of Pain Symptom Management 37: 863–872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Somers TJ, Shelby RA, Keefe FJ, et al. (2010) Disease severity and domain-specific arthritis self-efficacy: Relationships to pain and functioning in patients with rheumatoid arthritis. Arthritis Care and Research 62(6): 848–856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Somers TJ, Wren AA, Blumenthal JA, et al. (2014) Pain, physical functioning, and overeating in obese rheumatoid arthritis patients: Do thoughts about pain and eating matter? Journal of Clinical Rheumatology 20(5): 244–250. [DOI] [PubMed] [Google Scholar]
- Sperber N, Hall KS, Allen K, et al. (2013) The role of symptoms and self-efficacy in predicting physical activity change among older adults with arthritis. Journal of Physical Activity and Health. Epub ahead of print 8 February. DOI: 10.1123/jpah.2012-0030. [DOI] [PubMed] [Google Scholar]
- Spruill TM, Ogedegbe G, Harrold LR, et al. (2013) Association of medication beliefs and self-efficacy with adherence in urban Hispanic and African-American rheumatoid arthritis patients. Annals of the Rheumatic Diseases. Epub ahead of print 31 July. DOI: 10.1136/annrheumdis-2013-203560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stenstrom CH. (1994) Home exercise in rheumatoid arthritis functional class II: Goal setting versus pain attention. Journal of Rheumatology 21: 627–634. [PubMed] [Google Scholar]
- Strahl C, Kleinecht RA, Dinnel DL. (2000) The role of pain anxiety, coping, and pain self-efficacy in rheumatoid arthritis patient functioning. Behavior Research and Therapy 38: 863–873. [DOI] [PubMed] [Google Scholar]
- Strecher VJ, DeVellis BM, Becker MH, et al. (1986) The role of self-efficacy in achieving health behavior change. Health Education Quarterly 13: 73–92. [DOI] [PubMed] [Google Scholar]
- Taal E, Rasker JJ, Seydel ER, et al. (1993a) Health status, adherence with health recommendations, self-efficacy and social support in patients with rheumatoid arthritis. Patient Education and Counseling 20: 63–76. [DOI] [PubMed] [Google Scholar]
- Taal E, Riemsma R, Brus H, et al. (1993b) Group education for patients with rheumatoid arthritis. Patient Education and Counseling 20: 177–187. [DOI] [PubMed] [Google Scholar]
- Unützer J, Hantke M, Powers D, et al. (2008) Care management for depression and osteoarthritis pain in older primary care patients: A pilot study. International Journal of Geriatric Psychiatry 23: 1166–1171. [DOI] [PubMed] [Google Scholar]
- Van der Bijl JJ, Shortridge-Baggett LM. (2001) The theory and measurement of the self-efficacy construct. Scholarly Inquiry in Nursing Practice 15: 189–207. [PubMed] [Google Scholar]
- Van Hoogmoed D, Fransen J, Bleijenberg G, et al. (2010) Physical and psychosocial correlates of severe fatigue in rheumatoid arthritis. Rheumatology. Epub ahead of print 29 March. DOI: 10.1093/rheumatology/keq043. [DOI] [PubMed] [Google Scholar]
- Van Liew C, Santoro MS, Chalfant AK, et al. (2013) The good life: Assessing the relative importance of physical, psychological, and self-efficacy statuses on quality of well-being in osteoarthritis patients. Arthritis 2013(2013): 914216 (9 pp.). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waite-Jones JM, Hale CA, Lee HY. (2013) Psychosocial effects of Tai Chi exercise on people with rheumatoid arthritis. Journal of Clinical Nursing 22(21–22): 3053–3061. [DOI] [PubMed] [Google Scholar]
- Walen HR, Cronan PA, Bigatti SM. (2001) Factors associated with healthcare costs in women with fibromyalgia. American Journal of Managed Care 25: SP39–SP47. [PubMed] [Google Scholar]
- Wallis JA, Webster KE, Levinger P, et al. (2014) A pre-operative group rehabilitation programme provided limited benefit for people with severe hip and knee osteoarthritis. Disability and Rehabilitation. Epub ahead of print 6 March. DOI: 10.3109/09638288.2014.895428. [DOI] [PubMed] [Google Scholar]
- Weiner DK, Moore CG, Morone NE, et al. (2013) Efficacy of periosteal stimulation for chronic pain associated with advanced knee osteoarthritis: A randomized, controlled clinical trial. Clinical Therapeutics 35: 1703–1720.e5. [DOI] [PubMed] [Google Scholar]
- Wright LJ, Zautram A, Goingm S. (2008) Adaptation to early knee osteoarthritis: The role of risk, resilience, and disease severity on pain and physical functioning. Annals of Behavioral Medicine 36: 70–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yip YB, Sit JW, Wong DY, et al. (2008) A 1-year follow-up of an experimental study of a self-management arthritis programme with an added exercise component of clients with osteoarthritis of the knee. Psychology Health Medicine 13: 402–414. [DOI] [PubMed] [Google Scholar]