

Abstract
Möbius syndrome is an extremely rare congenital disorder. We report a case of Möbius syndrome in a 2-year-old girl with bilateral convergent squint and left-sided facial weakness. The characteristic magnetic resonance imaging (MRI) findings of Möbius syndrome, which include absent bilateral abducens nerves and absent left facial nerve, were noted. In addition, there was absence of left anterior inferior cerebellar artery (AICA) and absence of bilateral facial colliculi. Clinical features, etiology, and imaging findings are discussed.
Keywords: Abducens nerve, anterior inferior cerebellar artery, convergent squint, facial nerve, Möbius syndrome
Introduction
Möbius syndrome is a rare congenital neuromuscular disorder. It is characterized by unilateral or bilateral paralysis of the sixth and seventh cranial nerves, manifested clinically as external ophthalmoplegia and weakness of facial muscles.[1] Even though von Graaefe[2] described a case of congenital facial diplegia in 1880, it was Paul Julius Möbius, a German neurologist, who drew attention to the association of congenital facial diplegia with other malformations in 1888 and 1892.[3,4] The estimated incidence of this entity is 2–20 per million live births.[5] Only about 300 cases have been reported in the literature,[6] and very few cases of this syndrome have been reported in the radiology literature.
Case Report
A 2-year-old girl was referred to our department for plain magnetic resonance imaging (MRI) scan of the brain. The child's parents noticed facial asymmetry in the child with deviation of the angle of mouth to the right side on smiling, watering and incomplete closure of the left eye since birth. The child's birth and developmental history were normal.
On physical examination, facial asymmetry, bilateral convergent squint, prominent everted upper and lower lips were noted. Left facial nerve paralysis and bilateral abducent nerve paralysis were noted on neurological examination [Figures 1a and b].
Figure 1 (A and B).

(A) Picture showing bilateral convergent squint secondary to bilateral abducens nerve paralysis. Mild ptosis on left side is also seen (B) Picture demonstrating left-sided facial paralysis causing deviation of angle of mouth to right side on smiling
MR examination was performed using a 1.5 Tesla MRI scanner (Avanto; Siemens Medical Solutions, Erlangen, Germany). Axial and sagittal T1-weighted, axial T2-weighted, fluid-attenuated inversion recovery (FLAIR), and three-dimensional (3D) constructive interference in steady state (CISS) sequences (0.7-mm slice thickness) were evaluated.
MRI brain showed the following findings:
Absent cisternal and canalicular segments of left facial nerve [Figures 2 and 3]
Nonvisualization of cisternal segments of bilateral abducens nerves [Figures 2a and c]
Flattened floor of fourth ventricle with absence of bilateral facial colliculi [Figure 4].
Figure 2 (A-D).
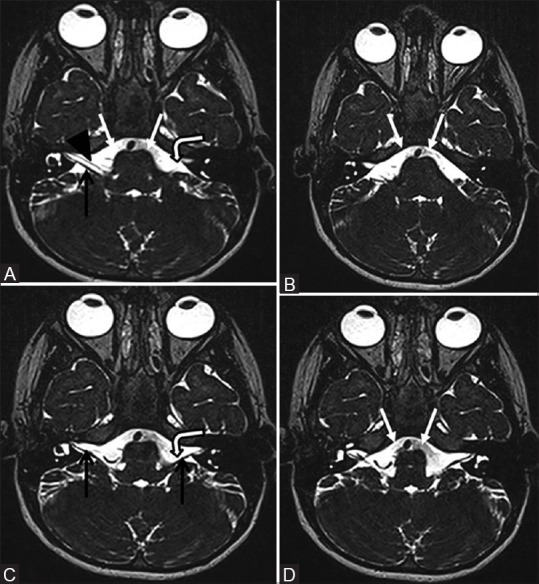
Four (A–D) contiguous 0.7-mm thick axial 3D CISS MR images of brain showing the absence of left facial nerve in cerebellopontine angle cistern (A and C, bent arrows). Right facial nerve (A, black arrow head) and bilateral vestibulocochlear nerves (A and C, black arrows) are visualized. In addition, there is absence of bilateral abducens nerves (A, B, and D, white arrows) in prepontine cisterns, the expected position of bilateral abducens nerves (A–D images are cranial to caudal sections)
Figure 3.
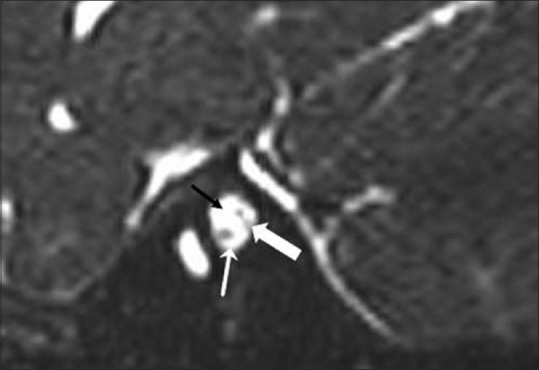
Parasagittal CISS MR image of left internal auditory canal (IAC) showing absent facial nerve in anterosuperior part of left IAC (black arrow). Vestibular (thick white arrow) and cochlear nerves (thin white arrow) are visualized in posterior and anteroinferior parts of left IAC respectively. (Anterior is to the left of image and posterior is to the right)
Figure 4.

Axial T1W MR image at the level of middle cerebellar peduncles showing flattened floor of fourth (black arrow) ventricle secondary to absence of bilateral facial colliculi
The left anterior inferior cerebellar artery (AICA) flow void was absent, and mild prominence of the right AICA was noted [Figure 5].
Figure 5.
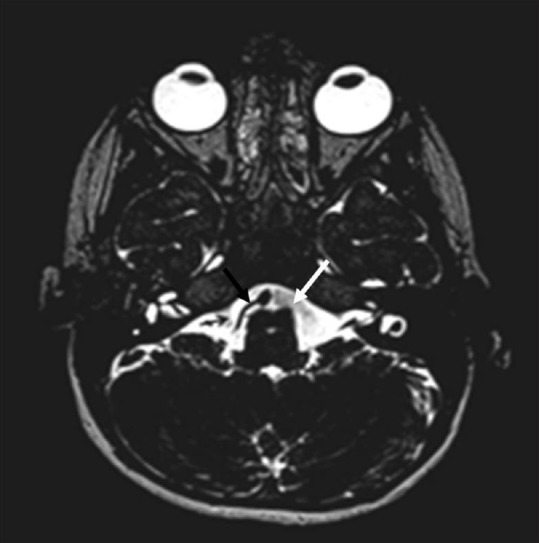
Axial CISS MR image showing right AICA (black arrow) and absent left AICA (white arrow)
Discussion
Möbius syndrome is rare disorder, which is characterized by congenital complete or partial facial nerve paralysis with or without paralysis of other cranial nerves.[7]
The definition and criteria for diagnosis of Möbius syndrome vary among authors. Based on previously published reviews, Kumar[7] used the following criteria for diagnosis of this syndrome: (a) Complete or partial facial nerve paralysis is an essential criterion for the diagnosis of Möbius syndrome, (b) Limb malformations (syndactyly, brachydactyly, absent digits, talipes) are often present, (c) Bilateral or unilateral cranial nerve palsies (commonly VI, XII, also IX, X) may be seen, (d) Orofacial malformations, ear deformities, and musculoskeletal deformities may also be seen. Recently, Verzijl et al.,[8] suggested facial palsy with impairment of ocular abduction as the primary criterion for Möbius syndrome, with or without association of other cranial nerve paralysis, musculoskeletal defects, or orofacial malformations.
Möbius syndrome manifests soon after birth with inability to close the eyelids during sleep, drooling of saliva, difficulty in sucking, and mask-like facies. Paralysis of the sixth cranial nerve results in impaired abduction of eyes. The hypoglossal nerve is the third most common nerve to be involved, causing paralysis and hypoplasia of the tongue. The oculomotor and trigeminal nerves are occasionally involved.[9]
Although neither the etiology nor the pathogenesis of Möbius syndrome has yet been elucidated, Verzijl et al.[10] proposed two theories based on previous published reviews: (a) a developmental rhombomeric defect including facial cranial nerve nuclei due to a genetic cause, or (b) an interruption in the vascular supply of the brainstem secondary to an environmental, mechanical, or genetic cause resulting in ischemia in the region of facial cranial nerve nuclei. An association of absent AICA with Möbius syndrome is not described in the literature; however, an association of the ischemic process resulting from an interruption of vascular supply to the brainstem in early fetal development was proposed.[7,10] Absent left AICA with mildly prominent contralateral AICA, observed in our case, may be an incidental finding and an anatomic variant. At times, either the posterior inferior cerebellar artery or the AICA is absent and one artery supplies the usual territories of both arteries.[11]
Möbius syndrome is mainly a clinical diagnosis. However, MRI is useful in demonstrating the abnormalities of the cranial nerves and orbital structures.[12]
Absence of facial and abducens nerves can be considered as characteristic features on MRI.[12] Other computed tomography (CT) and MR imaging findings include brainstem hypoplasia with straightening of floor of the fourth ventricle, indicating absence of the facial colliculus; calcification in pons in the region of abducens nuclei; absence of hypoglossal eminence at the medulla; and cerebellar hypoplasia.[1,13] Marked hypoplasia of extraocular muscles can occur.[12]
Based on history and clinicoradiological examinations (3D CISS), our case was diagnosed as Möbius syndrome. Craniofacial syndrome with asymmetric crying facies, congenital heart disease, and other factors may be confused with Möbius syndrome. Other neuromuscular disorders such as Melkersson–Rosenthal syndrome, muscular dystrophy, congenital facial muscular atrophy, cerebral palsy, and congenital myopathies may overlap with Möbius syndrome.[7,14] The Poland anomaly is found in 15% of Möbius syndrome patients.[7] The seventh nerve palsy in Möbius syndrome primarily affects the upper face, which is differentiated from other lower motor neuron palsies affecting both upper and lower portions of the face. Additionally, this can also be differentiated from supranuclear lesions, which only affect the lower half of the face.[7]
Since the disease is congenital and nonprogressive, no definitive and established treatment has been described. Ocular care and careful monitoring of complications that might set in, patient education, and a multidisciplinary approach by health professionals help to reduce the morbidity.
Conclusion
We herein reported a case of Möbius syndrome with absent left facial and bilateral abducens nerves. It is an irreversible condition that causes not only physical abnormalities but also social and psychological disturbances. CT and MR imaging may depict abnormalities in the brainstem, extraocular muscle hypoplasia, and other associated abnormalities. MR imaging, particularly 3D CISS sequence, is very useful in evaluating cisternal and cavernous segments of the cranial nerves.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
We have no conflicts of interest to disclose.
References
- 1.Kuhn MJ, Clark HB, Morales A, Shekar PC. Group III Möbius syndrome: CT and MR findings. AJNR Am J Neuroradiol. 1990;11:903–4. [PMC free article] [PubMed] [Google Scholar]
- 2.Von Graefe A. In: Handbuch der Gesamten Augenheilkunde. (Handbook of Ophthalmology) Von Graefe A, Saemisch T, editors. Vol. 6. Leipzig: W Engelmann; 1880. pp. 60–67. [Google Scholar]
- 3.Möbius PJ. Über angeboren doppelseitige Abducens-Facialis-Làhmung. Münch Med Wschr. 1888;35:91. [Google Scholar]
- 4.Möbius PJ. Uber infantile hernschwund. Müch Med Wschr. 1892;39:17. [Google Scholar]
- 5.Kuklík M. Poland-Möbius syndrome and disruption spectrum affecting the face and extremeties: A review paper and presentation of five cases. Acta Chir Plast. 2000;42:95–103. [PubMed] [Google Scholar]
- 6.Kulkarni A, Madhavi MR, Nagasudha M, Bhavi S. A rare case of Moebius sequence. Indian J Ophtalmol. 2012;60:558–60. doi: 10.4103/0301-4738.103798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kumar D. Moebius syndrome. J Med Genet. 1990;27:122–126. [PMC free article] [PubMed] [Google Scholar]
- 8.Verzijl HT, van der Zwaag B, Cruysberg JR, Padberg GW. Möbius syndrome redefined: A syndrome of rhombencephalic maldevelopment. Neurology. 2003;61:327–33. doi: 10.1212/01.wnl.0000076484.91275.cd. [DOI] [PubMed] [Google Scholar]
- 9.Walsh FB, Hoyt WF. Clinical Neuro-Ophthalmology. 3rd ed. Baltimore: Williams and Wilkins; 1969. pp. 1008–9. [Google Scholar]
- 10.Verzijl HT, Padberg GW, Zwarts MJ. The spectrum of Mobius syndrome: An electrophysiological study. Brain. 2005;128:1728–36. doi: 10.1093/brain/awh502. [DOI] [PubMed] [Google Scholar]
- 11.Akgun V, Battal B, Bozkurt Y, Oz O, Hamcan S, Sari S, et al. Normal anatomical features and variations of the vertebrobasilar circulation and its branches: An analysis with 64-detector row CT and 3T MR angiographies. Scientific World Journal 2013. 2013:620162. doi: 10.1155/2013/620162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wu SQ, Man FY, Jiao YH, Xian JF, Wang YD, Wang ZC. Magnetic resonance imaging findings in sporadic Möbius syndrome. Chin Med J (Engl) 2013;126:2304–7. [PubMed] [Google Scholar]
- 13.Pedraza S, Gámez J, Rovira A, Zamora A, Grive E, Raguer N, et al. MRI findings in Möbius syndrome: Correlation with clinical features. Neurology. 2000;55:1058–60. doi: 10.1212/wnl.55.7.1058. [DOI] [PubMed] [Google Scholar]
- 14.Srinivasa MR, Suma GN, Prakash R, Goel S. Moebius syndrome: A rare case report. JIndian Acad Oral Med Radiol. 2011;23:267–70. [Google Scholar]