

Abstract
Introduction:
Given the importance of fracture healing on patient outcome in clinical practice, it is critical to assess fracture healing.
Aim:
The aim of this study was to evaluate the feasibility of the Radiographic Union Score Hip fracture after treatment with intramedullary nail of stable hip fractures.
Patients and Methods:
We retrospectively collected the data from the clinical records of our institution of the 47 patientswho had undergone intertrochanteric hip fracture treatment using an intramedullary nail. Pain visual analogic score (VAS) was collected the same day that X-rays were taken. Plain hip X-rays were performed, in two radiographic views, at 40 and 90 days after the surgical procedure. The correlation between the RUSH and VAS score was evaluated.
Results:
Mean RUSH and VAS scores showed a strong statistical improvement between the 40 and 90 day follow-ups. RUSH value at 40 days fitted an inverse linear regression with VAS, p-value of 0.0063 and r2 of 0.15. At 90 days the regression between RUSH and VAS scores was not significant.
Conclusion:
RUSH could be proposed as an objective system to evaluate union in hip fractures treated with intramedullary nail.
Keywords: Radiographic Value, RUSH, Intramedullary Nail, Stable Hip Fractures, Union, Non Union, Delay Union
1. INTRODUCTION
Hip fractures (HF) have high rates of morbidity and mortality (1-3), and are prone to delayed unions and non-unions (4). HF accounts for a significant part of direct medical costs to the community and are usually associated with osteoporosis (5) although pathological fractures associated withbreast, prostatic or renal tumors metastasis arealso frequent (6-9).
Given the importance of fracture healing on patient outcome in both clinical practice and in guiding patients’ follow-up decisions, it is critical to ensure assessments of fracture healing are reliable and valid. The assessment of fracture healing is highly subjective and lacks a gold standard, resulting in the absence of a univocal definition of fracture union (10).
The lack of consensus with regard to the definition of fracture-healing in the current orthopedic and radiological literature, haslead to the development of union scores that can be applied when reading plain X-rays (11). The RUST scoring system appeared to be a reliable tool for the evaluation of clinical outcomes and in the management of tibial fractures (11). Similarly, the RUSH score was applied in HF increasing the agreement between orthopedic surgeons and radiologists with regard to fracture healing assessment, and offering a systematic approach which may aid in the treatment and clinical practice used with patients suffering from HF (12, 13).
2. AIMS
The aims of this study were therefore: to evaluate the feasibility of the RUSH score in hip fractures treated with intramedullary nail;and to evaluate the correlation of the RUSH score to the clinical outcome.
3. PATIENTS AND METHODS
Between May and December 2015, a total of 250 patients were surgically treated in our institution for intertrochanteric fractures. Only those patients with stable fractures according to Evans classification were enrolled; in addition, enrolment required the availability of plain hip X-rays, in two radiographic views, at 40 and 90 days after the surgical procedure.
We retrospectively collected the data from the clinical records of our institution of the 47 patients who had undergone intertrochanteric hip fracture treatmentwhich provided the positioningof an intramedullary nail (Supernail GT, Lima Corporate, Italy). Patient ages ranged from 56-94, with a mean of 83; 9patients were male and 38 were female.
Two readers utilized the RUSH score provided by Chiavaras et al (12) and derived from the RUST scoring system. RUSH provides four component scores of cortical bridging, cortical disappearance, trabecularconsolidation, and trabecular disappearance. Each component can be scored from 1 to 3. Similarly, the two trabecular indices were scored from1 to 3, each based on consolidation for one of the indices, and fractureline disappearance for the other. The overall RUSHscore therefore ranged from a minimum of 10 to a maximum of 30.
Images were reviewed separately and consensus was achieved after a second look in cases of scoring disagreement. Pain visual analogic score (VAS) was collected the same day that the X-rays were taken.
Descriptive statistics were calculated for all variables evaluated at CT-E, reporting raw numbers, frequencies and averages. The T Student’s test were used to test for significant differences between continuous variables. Regression between VAS and RUSH was evaluated. MedCalc Statistical Software version 14.8.1 (MedCalc Software bvba, Ostend, Belgium) was used for statistical analysis.
4. RESULTS
All 47 patients underwent intramedullary nail positioning. Thirty patients had a right intertrochanteric fracture, while 17 were left sided. Mean Rush at 40 days was 19.8 points and 23.9 at 90 days; the difference was statistically significant with a p value of less than 0.0001 (Figure 1). As well, the difference of mean VAS score at 40 and 90 days was statistically significant with a p value of less than 0.0001 (Figure 2), and a mean respectively of 6.6 and 5.2 (Table 1).
Figure 1.
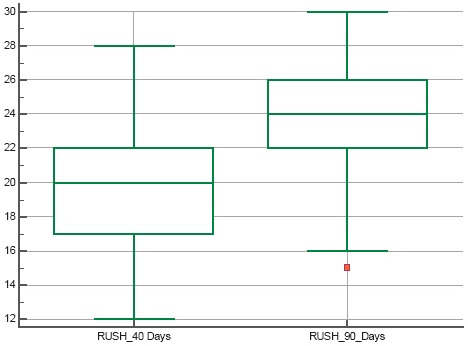
Mean RUSH score at 40 and 90 days after intramedullary nail positioning
Figure 2.
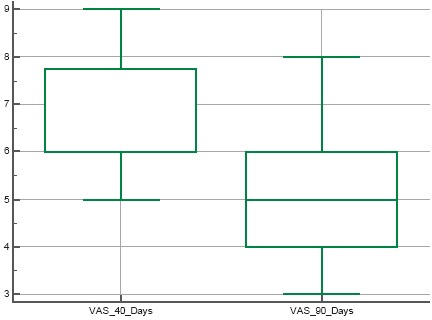
Mean VAS score at 40 and 90 days after intramedullary nail positioning
Table 1.
The difference of mean VAS score at 40 and 90 days

RUSH value at 40 days fitted an inverse linear regression with VAS, p-value of 0.0063 and r2 of 0.15 (Figure 3). At 90 days the regression between RUSH and VAS scores showed a p value of 0.059.
Figure 3.
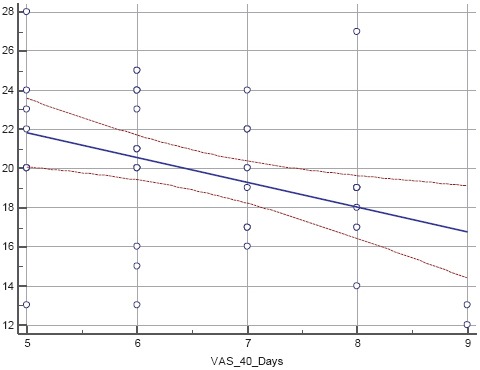
Regression between RUSH and VAS score at 40 days after intramedullary nail positioning.
5. DISCUSSION
Intertrochanteric fractures represent a major concern in elderly people, especially in women. The development of fixating toolshas significantly improved the outcome of such patients in the last century. Nevertheless, there is still a significant variability in the assessment of fracture-healing in orthopedic trauma studies (10). Fracture healing is a frequented point outcome in orthopedic research trials; therefore, differing and subjective accounts of fracture healingcan dramatically affect the perceived efficacy of a treatment (14).
The RUSH checklist improves the consistency and reliability of plain X-ray interpretation, as well it increases the utility of hip fracture radiographs.
RUSH appeared to be a feasible scoring system when applying it to intertrochanteric hip fractures treated with intramedullary nail. Actually, thecortical/trabecular bridging and disappearance were easy to assess in both the radiographic views. The only case where there may be difficulty is the evaluation of the lateral cortical bone;in this type of case the cephalic screw can hide the bridging and the fracture line. In such cases we suggest to lean for an intermediate value (2 points in the RUSH score). The significant improvement of RUSH during follow-up seemed to reflect the union of fractures (12).
The significant correlation between RUSH and VAS scoresconfirms the efficacy and feasibility ofthe RUSH scoring system in predicting bone healing during patient follow-up. Moreover, this study, form the basis for further studies confirming the clinical value of such radiographic scoring systems, which could be used to predict patients’ outcome giving to the orthopaedic surgeon a new tool in pain evaluation and follow-up. RUSH could be proposed as an objective system to evaluate union in many different fractures, including in cases that are treated with metallic fixating devices.
6. CONCLUSION
This study has several limitations: the small number of patients enrolled at one institution; and the retrospective natureof the study. The small number of patients does not allow for aproper evaluation of correlation. Moreover, the VAS scoring system is not validated to represent fracture healing. For all these reasons, further studies are required to define the correct role of RUSH.
This leads us to conclude that increasing the use of blinded assessment of outcomes and improved reporting of reliability of subjective end points will improve the quality of inferences derived from clinical studies. In the future, there will be a need to incorporate objective, quality-of-life, and functional parameters into the development of a more standardized definition for fracture union that better characterizes the chronological process of healing.
Footnotes
• Author’s contribution: Daniele Maiettini, Michele Bisaccia, Auro Caraffa, Giuseppe Rinonapoli, Luigi Piscitelli, Olga Bisaccia, Giuseppe Rollo, Luigi Meccariello, Paolo Ceccarini and Alberto Rebonato disclose any financial and personal relationships with otherpeople or organisations that could in appropriately influence (bias) their work. Examples of potential conflicts of interest include employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registrations, and grants or other funding.
• Conflict of interest statement: All authors disclose any financial and personal relationships with other people or organisations that could inappropriately influence (bias) their work. Examples of potential conflicts of interest include employment, consultancies, stock ownership, honoraria, paid expert testimony, patent applications/registrations, and grants or other funding.
• Human and animal rights: For this type of study no statement relating to studies on humans and animals is required.
REFERENCES
- 1.Liporace FA, Egol KA, Tejwani N, Zuckerman JD, Koval KJ. What’s new in hipfractures? Current concepts. Am J Orthop. 2005;34(2):66–74. [PubMed] [Google Scholar]
- 2.Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. OsteoporosInt. 2004;15(11):897–902. doi: 10.1007/s00198-004-1627-0. [DOI] [PubMed] [Google Scholar]
- 3.Gullberg B, Johnell O, Kanis JA. World-wide projections for hip fracture. OsteoporosInt. 1997;7(5):407–413. doi: 10.1007/pl00004148. [DOI] [PubMed] [Google Scholar]
- 4.Blomfeldt R, Tornkvist H, Ponzer S, Soderqvist A, Tidermark J. Comparison of internal fixation with total hip replacement for displaced femoralneck fractures. Randomized, controlled trial performed at four years. J Bone Joint Surg Am. 2005;87:1680–8. doi: 10.2106/JBJS.D.02655. [DOI] [PubMed] [Google Scholar]
- 5.Leal J, Gray AM, Prieto-Alhambra D, Arden NK, Cooper C, Javaid MK, Judge A. REFReSH study group. Impact of hip fracture on hospital care costs: apopulation-based study. Osteoporos Int. 2016;27(2):549–58. doi: 10.1007/s00198-015-3277-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Çaypınar B, Erol B, Topkar M, Başçı O. Biomechanical determination of therelationship between femoral neck lesion size and the risk of pathologicalfracture. Hip Int. 2016;26(2):158–63. doi: 10.5301/hipint.5000309. [DOI] [PubMed] [Google Scholar]
- 7.Rebonato A, Vannini E, Giganti M, Volterrani L, Fonio P, Piscioli I, Scialpi M. Small renal oncocytoma (≤4 cm):enhancement patterns on triphasic spiralcomputed tomography. Recenti Prog Med. 2012;103(11):477–82. doi: 10.1701/1166.12892. [DOI] [PubMed] [Google Scholar]
- 8.Dibekoglu C, Turanli S, Karaman N, Ozcelik KC, Erdogan O. Bone fracture inbreast cancer patients with isolated bone metastasis. Chirurgia (Bucur) 2015;110(1):43–8. [PubMed] [Google Scholar]
- 9.Rebonato A, Pierotti L, Barberini F, Rosi G, Macarini L, Scialpi M. Smallrenalcell carcinoma (≤4 cm): enhancementpatterns on triphasicspiral CT. Recent Prog Med. 2012;103(11):471–6. doi: 10.1701/1166.12891. [DOI] [PubMed] [Google Scholar]
- 10.Corrales LA, Morshed S, Bhandari M, Miclau T., 3rd Variability in the assessment of fracture-healing in orthopaedic trauma studies. J Bone Joint Surg Am. 2008;90(9):1862–8. doi: 10.2106/JBJS.G.01580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Cekiç E, Alıcı E, Yeşil M. Reliability of the radiographic union score for tibial fractures. Acta OrthopTraumatol Turc. 2014;48(5):533–40. doi: 10.3944/AOTT.2014.14.0026. [DOI] [PubMed] [Google Scholar]
- 12.Chiavaras MM, Bains S, Choudur H, Parasu N, Jacobson J, Ayeni O, Petrisor B, Chakravertty R, Sprague S, Bhandari M. The Radiographic Union Score for Hip (RUSH): the use of a checklist to evaluate hip fracture healing improves agreement between radiologists and orthopedic surgeons. Skeletal Radiol. 2013;42(8):1079–88. doi: 10.1007/s00256-013-1605-8. [DOI] [PubMed] [Google Scholar]
- 13.Bhandari M, Chiavaras MM, Parasu N, Choudur H, Ayeni O, Chakravertty R, Bains S, Hak A, Sprague S, Petrisor B. Radiographic union score for hip substantially improves agreement between surgeons and radiologists. BMC Musculoskelet Disord. 2013;25:14–70. doi: 10.1186/1471-2474-14-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Davis BJ, Roberts PJ, Moorcroft CI, Brown MF, Thomas PBM, Wade RH. Reliability of radiographs in defining union of internally fixed fractures. Injury. 2004;35(6):557–61. doi: 10.1016/S0020-1383(03)00262-6. [DOI] [PubMed] [Google Scholar]