

Abstract
Background:
Patients have to acquire information to support their decision on choosing a suitable healthcare provider. But in developing countries like Vietnam, accessibility issues remain an obstacle, thus adversely affect both quality and costliness of healthcare information. Vietnamese use both sources from health professionals and friends/relatives, especially when quality of the Internet-based cheaper sources appear to be still questionable. The search of information from both professionals and friends/relatives incurs some cost, which can be viewed as low or high depending low or high accessibility to the sources. These views potentially affect their choices.
Aim and Objectives:
To investigate the effects that medical/health services information on perceived expensiveness of patients’ labor costs. Two related objectives are a) establishing empirical relations between accessibility to sources and expensiveness; and, b) probabilistic trends of probabilities for perceived expensiveness.
Results:
There is evidence for established relations among the variables “Convexp” and “Convrel” (all p’s < 0.01), indicating that both information sources (experts and friends/relatives) have influence on patients perception of information expensiveness. The use of experts source tends to increase the probability of perceived expensiveness.
Conclusion:
a) Probabilistic trends show Vietnamese patients have propensity to value healthcare information highly and do not see it as “expensive”; b) The majority of Vietnamese households still take non-professional advices at their own risks; c) There is more for the public healthcare information system to do to reduce costliness and risk of information. The Internet-based health service users communities cannot replace this system.
Keywords: Healthcare provider, Quality of information, Health data, Consumer behavior, Vietnam
1. BACKGROUND
Prior to making a decision on where to go for their healthcare treatment, most patients would to a certain extent like to acquire information regarding a propsective healthcare provider’s quality, reputation and suitability with respect to their needs. Therefore, quality information will play an important role in helping patients to make more informed decisions (1). In fact, the extant literature has confirmed that the question of whether one could have access to healthcare information and data remains unanswered and a major problem in numerous developing countries (2). Having faced the same issue, Vietnamese patients have long had to accept the uncertainty caused by asymmetric information phenomenon, and to bear the risk of making non-optimal decisions (3).
There is a wide range of sources where patients can find information from, such as their relatives, health experts, and media (e.g. newspapers, advertisements, Internet, etc.). These sources can overlap or supplement one another; and they may also be used with different degrees of trust (4). When a patient is not satisfied with the information provided by health experts, due to issues of quality or sufficiency, he/she can now seek more data thanks to the existence of the Internet and other ICT-based facilities (5). One the other hand, the practice of providing medical advice by health experts has for long been proposed in order to increase public access to primary health services (6).
Nonetheless, there has been a limitation in the use of the Internet as well as other free health information sources: reliability (7, 8). The plethora of information and even contradicting advices may become confusing and difficult for patients to make a decision (9). As a consequence, many patients have to rely on their families, friends or health profesionals for confirmation (10).
As acquiring opinions from health professionals is not always easy, and often seen as time-consuming and financially costly by many (11), a substantial portion of patients and their relatives would accept to act as voluntary health workers for themselves or for their friends, by spending time, energy and even some money to acquire useful information and data which can enable them to provide a feasible solution (3). These services albeit voluntary reflect a kind of labor cost, which can be felt costly as well. They may potentially influence patients’ choices (12).
For understanding patient behaviors in making decision on healthcare provider’s choice, both empirical data and statistical evidence are needed with respect to effects that information, coming from different sources, may exert on a patient’s perception.
2. AIM AND OBJECTIVES
This short article aims to investigate the effects that medical/health services information that patients receive from their major sources (friends/relatives versus healthcare experts) may have on perceived expensiveness of their labor costs during the process of collecting information/data for their decision on healthcare provider’s choice. This overall aim is specified by closely related objectives of: a) establishing empirical relations between possible variables representing a dataset obtained from a healthcare information survey; and, b) estimating/presenting conditional probabilities for the abovementioned labor costs “paid” by patients. Logically, policy implications follow.
3. MATERIAL AND METHODS
The study investigates a dataset that contains 1,459 observations collected from over 30 hospitals in the Hanoi region of Vietnam by a community-based cross-section survey starting in the fourth quarter of 2015, ending the first quarter 2016. The dataset is deposited at (13) and open to public examination and reuse.
The sampling is random and does not have any discriminations against or in favor of any cases. Data collection was undertaken by Hanoi-based Vuong & Associates, with ethical standards beign based on an institutional regulation and clearance, numbered V&A/15#01 (dated October 19, 2015). Written approvals by survey respondents have been obtained from participants by the survey team.
Statistical Analysis
Data were entered using MS Excel; and then the raw data file were converted to tables in CSV format. The R statistical package (3.2.3) has then been used to process and structure categorical data. Subsequent statistical investigations have been performed using baseline category logit (BCL) procedures for multinomial logistic regression analysis, with technical details provided in (14). The regression analysis enables us to obtain estimated coefficiens, which are required for computing empirical probabilities, upon satisfactory statistical significance of the predictor variables in the estimated model shown by z-values and corresponding p-values. p < 0.05 is considered statistically significant. For an example of real-world treatments, refer to (3).
Dataset
Tthe dataset provided in Table 1 shows responses of respondents to survey questions regarding the level of accessibility to information sources, namely friends/relatives and healthcare professionals/experts.
Table 1.
Distribution of patients against factors “Labor”, “Convrel” and “Convexp”
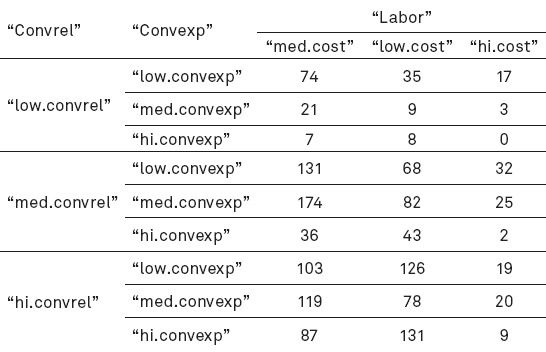
From this dataset, the first predictor variable (coded “Convrel”) has three distinct categorical values, which imply different levels of labor costs incurred:
“hi.convrel”: high convenience and easy access to friends/relatives medical advice;
“med.convrel”: relatively convenient; and,
“low.convrel”: mostly inconvient, uneasy access.
Three categorical values of the second predictor (“Convexp”) are defined similarly:
“hi.convexp”;
“med.convexp”; and,
“low.convexp”.
The one response variable is “Labor”, which has three levels of perceived expensiveness of labor costs patients “pay” for seeking healthcare information:
“low.cost”;
“med.cost”;
“hi.cost”.
The majority of respondents (>88%) report that they had not encountered problems in obtaining useful medical information and data from friends/relatives. On the other hand, nearly 58% report reasonably easy access to professional sources such as health experts. About 8.7% of patients encounter a great deal of difficulty in gathering information for making decisions.
4. RESULTS
The statistical estimation results are provided in Table 2, with the first estimation referring to Eq.1, and the second to Eq.2.
Table 2.
Estimation results

From Table 2, the estimated coefficients among two above predictor variables and the response variable are reported to be highly significant, with all p-values < 0.01. Therefore, there is evidence for established relations among the variables.
Generally speaking, almost all coefficients of “Convexp” are larger than those of “Convrel”. Consequently, information from experts appear to have had a stronger influence on patients rather than which from friends/relatives.
Especially, as it is illustrated in Eq.1, the largest coefficient is β3=1.418 (p<0.0001) suggesting that difficulty in acquiring health information from experts/professionals appears to incur the highest “labor cost” to patients while seeking health and medical information.
From Eqs.1-2, empirical probabilities are computed and provided in Table 3.
Table 3.
Probabilities of perceived expensiveness, with respect to “Convexp” / “Convrel”
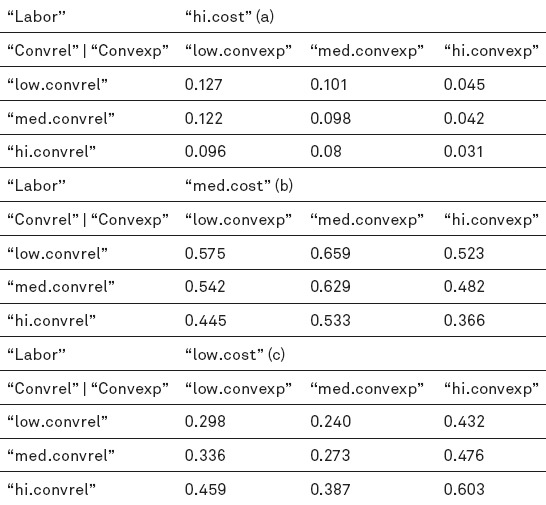


The set of higher empirical probabilities as reported in Table 3 is found in the case of “med.cost”, especially when the condition of reasonably easy access to health experts applies.
5. DISCUSSION
The likelihood of high labor costs for patients in acquiring healthcare information is reported to be reasonably low, for all both sources of data. When difficulty is reproted, the probability computed is as low as 12.7%:
When encountering shortage of healthcare information from friends/relatives, patients will need to rely on healthcare professionals. Figure 1 considers the changing probabilities of “labor costs” following changing levels of access to experts’ advice (from “low” to “high”). The downward trend of “hi.cost” line implies that if a patients finds it reasonably easy to acquire data from health experts, the probability of expensiveness decreases.
Figure 1.
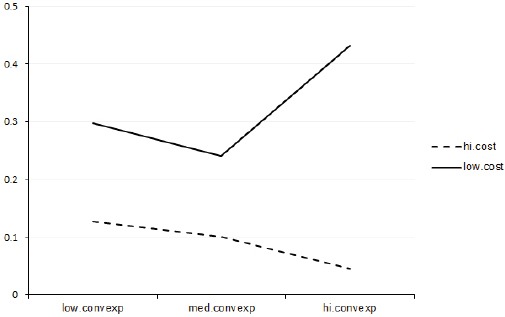
Changing probabilities of perceived expensiveness given difficult access to medical information from friends/relatives
On the other hand, the “low.cost” lines tells that when access to health experts source improves, the probability for a patient to view healthcare information as “inexpensive” increases significantly, from 29.8% to 24.0% to 43.2%.
The trends in Fig. 2 unveil different insights since we now control for situation where access to health experts/professionals is limited and/or difficult, in which case patients count on friends/relatives (“Convrel”) for information. (Naturally, the two probabilistic trends (i.e., “hi&med.cost” and “low.cost”) are symmetric over the line of 50%. The easier a patient’s access to this source of information, the higher the chance of “inexpensiveness” is.
Figure 2.
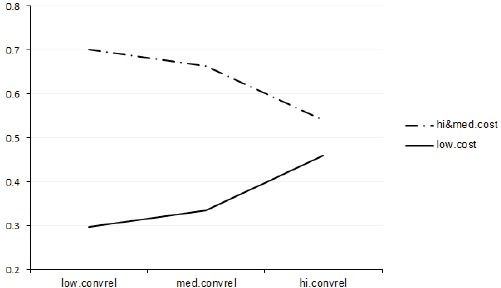
Changing probabilities of perceived expensiveness given difficult access to medical information from health experts
6. CONCLUSION
Firstly, Vietnamese patients’ perception about costliness of health information for making decision of health service provider shows a clearer trend for two opposite states of low and high accessibility.
Secondly, general probabilistic trends show that Vietnamese patients have propensity to value healthcare information highly and therefore do not see it as “expensive” especially when access to friends/relatives is available. This suggests that the majority of Vietnamese households still believe in value of alternative sources to health experts, and taking non-professional advices at their own risks.
The situation suggests that perhaps there will be more room for the public healthcare system to improve regarding mitigating both costliness and risk of information use with public-funded information services, without leaving the lower-cost functions to the Internet-based health service users communities.
Recommendation: The trend of continuous reliance on friends/relatives exhibits a long-standing habit of seeking the most “convenient” sources of information instead of “reliable” and “responsible”. Further investigations into the latter should shed light on patients’ psychology that underscores their preference in their behavior of information search.
Limitation of the study: Although the sample size is reasonable, the study is by far limited to the region of Hanoi and its vicinity; and as a consequence, a generalization at this stage is impossible. In addition, this analysis does not consider the Internet sources, which is generally free, due to its questionable quality and difficulty to be verified.
Author’s contribution: Quan-Hoang Vuong, as sole author in this article, designing the research program, making research questions, acquiring and processing data, writing, checking and approving the manuscript.
Footnotes
• Conflict of interest: none declared.
REFERENCES
- 1.Charnock D, Shepperd S, Needham G, Gann R. DISCERN: an instrument for judging the quality of written consumer health information on treatment choices. Journal of Epidemiology and Community Health. 1999;53(2):105–11. doi: 10.1136/jech.53.2.105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.O'Donnell O. Access to health care in developing countries: breaking down demand side barriers. Cadernos de Saúde Pública. 2007;23(12):2820–34. doi: 10.1590/s0102-311x2007001200003. [DOI] [PubMed] [Google Scholar]
- 3.Vuong QH, Nguyen TK. Vietnamese patients’ choice of healthcare provider: in search of quality information. Int J Behavioural and Healthcare Research. 2015;5(3-4):184–212. doi:10.1504/IJBHR.2015.077678. [Google Scholar]
- 4.Tu HT, Cohen GR. Striking jump in consumers seeking health care information. Center for Studying Health System Change. 2008. Tracking Report No. 20. URL:< http://www.hschange.org/CONTENT/1006/1006.pdf. >. [PubMed]
- 5.Fogel J, Albert SM, Schnabel F, Ditkoff BA, Neugut AI. Use of the Internet by women with breast cancer. J Med Internet Res. 2002;4(2):e9. doi: 10.2196/jmir.4.2.e9. doi:10.2196/jmir.4.2.e9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Widman LE, Tong DA. Requests for medical advice from patients and families to health care providers who publish on the World Wide Web. Archives of Internal Medicine. 1997;157(2):209–12. [PubMed] [Google Scholar]
- 7.McMullan M. Patients using the Internet to obtain health information: how this affects the patient–health professional relationship. Patient Education and Counseling. 2006;63(1):24–8. doi: 10.1016/j.pec.2005.10.006. [DOI] [PubMed] [Google Scholar]
- 8.Hesse BW, Nelson DE, Kreps GL, Croyle RT, Arora NK, Rimer BK, Viswanath K. Trust and sources of health information: the impact of the Internet and its implications for health care providers: findings from the first Health Information National Trends Survey. Archives of Internal Med. 2005;165(22):2618–24. doi: 10.1001/archinte.165.22.2618. [DOI] [PubMed] [Google Scholar]
- 9.Damman OC, Hendriks M, Rademakers J, Delnoij DM, Groenewegen PP. How do healthcare consumers process and evaluate comparative healthcare information? A qualitative study using cognitive interviews. BMC Public Health. 2009;9(1) doi: 10.1186/1471-2458-9-423. Art. #423. doi:10.1186/1471-2458-9-423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Longo DR, Schubert SL, Wright BA, LeMaster J, Williams CD, Clore JN. Health information seeking, receipt, and use in diabetes self-management. The Annals of Family Medicine. 2010;8(4):334–40. doi: 10.1370/afm.1115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Nguyen T, Hai VU, Webster J, Nimunkar A. A Web-based electronic medical records and hospital information system for developing countries. Journal of Health Informatics in Developing Countries. 2011;5(1):155–70. [Google Scholar]
- 12.Isaacs SL. Consumer’s information needs: results of a national survey. Health Affairs. 1996;15(4):31–41. doi: 10.1377/hlthaff.15.4.31. [DOI] [PubMed] [Google Scholar]
- 13.Vuong QH. Data on Vietnamese patients’ behavior in using information sources, perceived data sufficiency and (non)optimal choice of health care provider. Data in Brief. 2016;7:1687–95. doi: 10.1016/j.dib.2016.04.066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Agresti A. Categorical Data Analysis. 3rd ed. New Jersey: Wiley, Hoboken; 2013. [Google Scholar]
- 15.Pistolis J, Zimeras S, Chardalias K, Roupa Z, Fildisis G, Diomidous M. Investigation of the impact of extracting and exchanging health information by using Internet & social networks. Acta Inform Med. 2016;24(3):156–60. doi: 10.5455/aim.2016.24.197-201. doi:10.5455/aim.2016.24.197-201. [DOI] [PMC free article] [PubMed] [Google Scholar]