

Abstract
Introduction
In 2011 the National Institute for Health and Care Excellence (NICE) published guidelines suggesting that clinicians offer total hip replacement (THR) to patients with displaced intracapsular hip fractures who could walk independently outside with no aids or one stick, who are not cognitively impaired and are ASA (American Society of Anesthesiologists) grade ≤2. They also stated that best practice is operating within 36 hours of presentation. This audit aimed to determine whether Scarborough Hospital was following these guidelines and compared the results with the national average.
Methods
Two years of data (January 2012 – December 2013) were collected retrospectively from Scarborough Hospital’s hip fracture database on all patients presenting with an intracapsular hip fracture. Data were analysed to determine whether patients who had a THR fulfilled NICE criteria. Furthermore, patients with hemiarthroplasties who were eligible for THRs were identified. Finally, the time to surgery was calculated to examine whether patients receiving THRs waited longer than patients receiving hemiarthroplasties.
Results
In 2012, 48.6% of all eligible patients received a THR while in 2013 the figure was 55.9%. These percentages are much higher than the national average. However, 36 (53.7%) of the 67 patients who received a THR did not fulfil all the NICE criteria, mainly owing to high ASA grade. The mean time from presentation to theatre for THR was 8 hours and 37 minutes longer for THR patients than for hemiarthroplasty in 2012. This difference was reduced to 2 hours and 12 minutes in 2013.
Conclusions
Small general hospitals can meet and even exceed the standards regarding treatment strategies for hip factures. However, there is still room for improvement. Departmental training may be useful in achieving this aim. The anaesthetic team should be involved at the earliest opportunity, to help optimise patients preoperatively and determine whether patients listed for THR with higher ASA grades are suitable for this surgery.
Keywords: Arthroplasty, Hemiarthroplasty, Hip replacement, Fracture, Hip
Fragility fractures involving the neck of femur (NOF) make up a high volume of patients presenting to orthopaedic departments. Research suggests that the national incidence is 76,000 per year in England; however, this number is expected to increase to 100,000 per year by 2033.1
In June 2011 the National Institute for Health and Care Excellence (NICE) issued a document outlining the management of hip fractures in adults.2 This guideline offers information regarding the management of this special group of patients from their presentation at hospital to discharge and subsequent follow-up review. In addition, the fragility hip fracture best practice tariff (BPT) was also introduced in April 2010.3 These clinical characteristics of best practice were chosen by a group of clinicians and service managers chaired by the National Clinical Director for Trauma. Factors such as optimisation of the time from presentation/diagnosis to theatre, falls prevention and postoperative geriatrician review were included. The BPT dictates that patients should have their surgery within 36 hours of arrival in an emergency department (or time of diagnosis if an inpatient). Together, these documents aimed to improve the level of compliance with defined elements of evidence-based best practice care.
Clear advice regarding surgical options for fractured NOF is available in the NICE guideline.2 This recommends that patients with a displaced intracapsular NOF fracture should have a replacement arthroplasty (hemiarthroplasty or total hip replacement [THR]). The document further states that THR should be offered to patients who were able to walk independently out of doors with no more than the use of a stick, are not cognitively impaired, and are medically fit for anaesthesia and the procedure. For the purpose of this study and following discussion with the departmental multidisciplinary team, this included patients with an ASA (American Society of Anesthesiologists) grade of ≤2 and an abbreviated mental test score (AMTS) of ≥9 at the time of presentation/diagnosis.
The aim of this study was to determine whether a small hospital trust can adhere to NICE guidelines and offer eligible patients THRs. Data were also examined to discover the number of patients who may have been eligible for a THR but who received a hemiarthroplasty instead. These data were compared with those detailed in the National Hip Fracture Database annual report published in 2014.4 A secondary aim was to examine whether there was an increase in time to theatre if patients were waiting for a dedicated hip surgeon to perform their THR, resulting in potentially not meeting the 36-hour benchmark as dictated in the BPT document.3
Methods
A retrospective review was undertaken of data collected over a two-year period (January 2012 – December 2013) from the National Hip Fracture Database for patients who had their surgery performed in Scarborough Hospital, a small general hospital on the east coast of England serving a relatively elderly population (21.9% aged over 65 years).5 The data were analysed by two researchers working in the orthopaedic department. Data collected included type of surgery, time to surgery, ASA grade, AMTS and preoperative mobility status.
Results
During the study period, 614 patients had surgery performed for a fractured NOF or proximal femoral fracture. This included many different fixation devices: hemiarthroplasty (n=262), THR (n=67), intramedullary nails (n=28), cannulated hip screws (n=9) and dynamic hip screws (n=248) (Fig 1).
Figure 1.
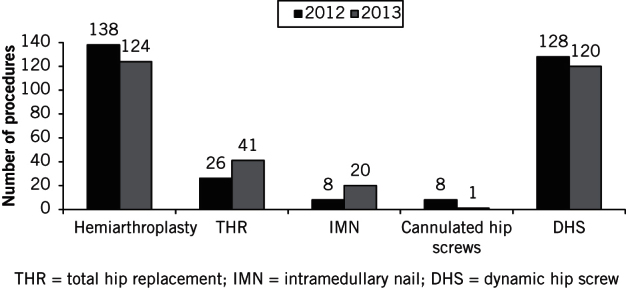
Procedures performed during the study period
In 2012, 26 patients had a THR and 138 had a hemiarthroplasty for fractured NOF. In 2013 the figures were 41 and 124 respectively (Table 1). The increase in the proportion of patients receiving THR for a fracture was statistically significant (p=0.04).
Table 1.
Numbers of arthroplasty procedures performed
| 2012 | 2013 | |
| Total number of arthroplasty procedures (hemiarthroplasty and THR) | 164 | 165 |
| Total number of THRs | 26 | 41 |
| THRs as a proportion of all arthroplasty surgery | 15.9% | 24.9% |
THR = total hip replacement
The mean time from presentation to theatre in 2012 was 35 hours and 55 minutes for THR, and 27 hours and 18 minutes for hemiarthroplasty. These times decreased in 2013 to 26 hours and 10 minutes, and 23 hours and 58 minutes respectively (Fig 2).
Figure 2.
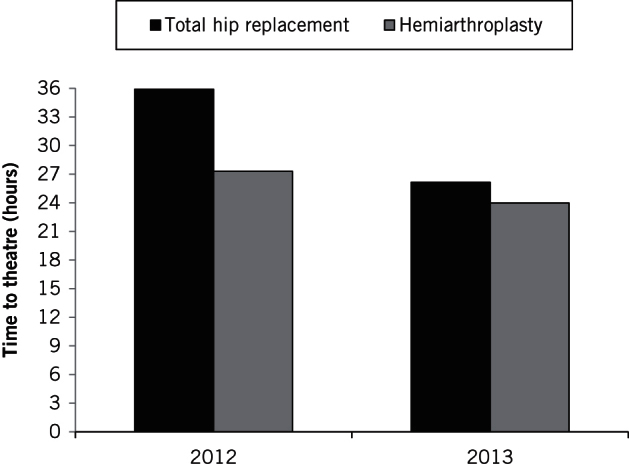
The mean time from presentation to theatre for total hip replacement and hemiarthroplasty patients
When assessing THR patients based on the NICE guidelines, only 65.4% of patients in 2012 and 46.3% in 2013 fulfilled all the criteria (Fig 3). The most common reason for not fulfilling these was having an ASA grade of >2. In fact, two patients in 2013 who had a THR were ASA grade 4.
Figure 3.
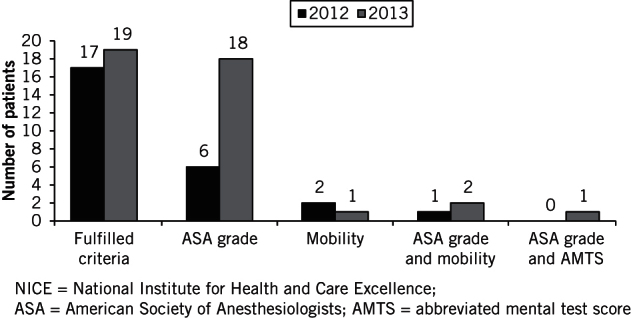
The numbers of patients who fulfilled NICE criteria for total hip replacement and those who did not, with reasons
Of the 138 patients who received a hip hemiarthroplasty in 2012, 18 (13.0%) actually fulfilled the NICE guidelines and would have been eligible for a THR. The situation was similar in 2013, with 15 (12.1%) of the 124 patients who received a hip hemiarthroplasty being eligible for a THR. Consequently, 48.6% and 55.9% of all patients eligible for THR actually received a THR in 2012 and 2013 respectively (Table 2).
Table 2.
Proportion of patients eligible for a THR who actually received a THR
| 2012 | 2013 | |
| Hemiarthroplasty patients who fulfilled NICE criteria for THR | 18 | 15 |
| THR patients who fulfilled NICE criteria for THR | 17 | 19 |
| Total patients who fulfilled NICE criteria for THR | 35 | 34 |
| Proportion of all patients eligible for THR actually receiving THR | 48.6% | 55.9% |
THR = total hip replacement; NICE = National Institute for Health and Care Excellence
Discussion
There was a significant increase in the number of patients receiving a THR for fractured NOF between 2012 and 2013. This is likely to have been due to the increasing knowledge in the orthopaedic community regarding the NICE guidelines and BPT. Although there was a statistically significant increase (p=0.04) in the number of patients receiving a THR, many (46.3%) did not actually fulfil the NICE criteria.
The most common reason for not fulfilling the criteria in both years was that the patient had an ASA grade of >2 (Fig 2). One possible explanation for this is that surgeons are not trained formally in assigning patients an ASA grade. There may therefore be a discrepancy between the surgeon’s and anaesthetist’s thoughts regarding the patient’s suitability for surgery. Furthermore, in many orthopaedic departments (including that at Scarborough Hospital), the anaesthetic team does not attend the formal trauma meeting and ‘post-take’ ward rounds, and so does not have the opportunity to assess the patient properly in the early preoperative period. As a result, it may be that orthopaedic staff are not assessing ASA grades accurately prior to the surgical decision being made regarding the operative device to be used. The anaesthetic team should therefore be involved early in the preoperative period to help prevent inappropriate surgical decisions.
During the study period, there was an increase in the proportion of eligible patients receiving a THR for fractured NOF. Indeed, the percentage of patients receiving a THR appropriately increased from 48.6% in 2012 to 55.9% in 2013 (Table 2). When compared with the national average of 20.7% in 2012 and 19.1% in 2013,4 it is clear that small hospitals such as Scarborough General Hospital can meet and even exceed the national average.
With regard to time from diagnosis/presentation to theatre and comparison with the 36-hour benchmark dictated by the BPT,3 there was a clear improvement for both THR and hemiarthroplasty surgery (Fig 2). In 2012 there was a considerably longer wait for THR than for hemiarthroplasty but this difference reduced dramatically in 2013, when the mean time to theatre was only 2 hours 12 minutes longer for THR patients.
Consequently, our data show that contrary to the concerns raised by the local orthopaedic staff, there was not a significantly increased waiting time for THR versus hemiarthroplasty. In fact, 84.6% of patients in 2012 and 87.7% of patients in 2013 had their THR within 36 hours of diagnosis/presentation. This compares with 80.4% of patients in 2012 and 90.3% in 2013 who had their hemiarthroplasty within 36 hours of diagnosis/presentation. On average, therefore, 81.1% of patients in 2012 and 90.2% of patients in 2013 had their surgery (THR or hemiarthroplasty) performed within 36 hours. This is considerably better than the national average of 70.6% in 2012 and 71.7% in 2013.4
Conclusions
This retrospective study suggests that small general hospitals can meet and even exceed the standards regarding treatment strategies for fractured NOF as published by NICE2 and as found in the BPT document.3 However, it is clear that some patients who do not match the NICE criteria are having THR surgery. This could have a detrimental effect on surgical outcomes. We suggest that the anaesthetic team should be involved at the earliest opportunity, to help optimise patients preoperatively and potentially prevent patients with an ASA grade of ≥3 from having more invasive surgery in the form of THR.
There does not appear to be a significant delay in getting patients to theatre if they are undergoing a THR compared with a hemiarthroplasty. This may be due to the fact that in this small department, four of the six full-time consultants were proficient in doing arthroplasty surgery in their elective practice. We appreciate that this may not be the case in all orthopaedic departments. Nevertheless, given the publication of the NICE guidelines, this should be taken into consideration when trauma networks and departments are auditing their practice.
References
- 1.White SM, Griffiths R. Projected incidence of proximal femoral fracture in England: a report from the NHS Hip Fracture Anaesthesia Network (HIPFAN). Injury 2011; : 1,230–1,233. [DOI] [PubMed] [Google Scholar]
- 2.National Institute for Health and Care Excellence Hip Fracture: Management. London: NICE; 2011. [PubMed] [Google Scholar]
- 3.Department of Health Best Practice Tariff (BPT) for Fragility Hip Fracture Care User Guide. London: DH; 2010. [Google Scholar]
- 4.Royal College of Physicians National Hip Fracture Database (NHFD) Annual Report 2014. London: RCP; 2014. [Google Scholar]
- 5.Scarborough and Ryedale Clinical Commissioning Group Sustainable Development Management Plan. Scarborough: Scarborough and Ryedale Clinical Commissioning Group; 2014. [Google Scholar]