

Abstract
Traumatic abdominal wall hernia (TAWH) is a rare clinical entity in terms of aetiology. It occurs following a blunt abdominal injury with energy high enough to cause disruption of the musculoaponeurotic layer but not the elastic skin layer. It is often associated with underlying intra-abdominal injuries, which can be diagnosed either clinically or radiologically. We report a case of TAWH in a young man with associated large bowel transection, which remained undiagnosed in the preoperative period owing to its masked features. He was managed surgically, with no recurrence to date. Considering the high volume of blunt abdominal trauma cases that present to the accident and emergency department, only few cases of TAWH have been reported in the literature. Confusion still exists regarding the timing and mode of management of this condition.
Keywords: Abdominal wall, Traffic accidents, Abdominal hernia, Aetiology, Motorcycles
Traumatic abdominal wall hernia (TAWH) is an unusual type of hernia that occurs following a non-penetrating abdominal trauma resulting in breach of the musculoaponeurotic layers of the abdomen with an intact overlying skin. Although blunt abdominal trauma is very common, the incidence of TAWH is low. The diagnosis of TAWH is rarely straightforward owing to the various clinical presentations and management therefore varies substantially.1 We report a unique case of TAWH following a road traffic accident with associated hollow viscous injury.
Case history
A 30-year-old man presented to the accident and emergency department having sustained a high velocity blunt trauma injury over his left flank from a hollow metal pipe two hours earlier while driving a motorcycle. The patient was haemodynamically unstable. He had a tender, irreducible swelling of approximately 15cm x 10cm over the left flank with evidence of an overlying bruise and abrasions (Fig 1). There was no expansile cough impulse over the swelling and the swelling was soft in consistency. General abdominal examination was insignificant and there was no peritonitis.
Figure 1.

Swelling (arrow) and abrasions (arrowhead) at site of traumatic abdominal wall hernia
Focused assessment with sonography for trauma showed no intra-abdominal fluid collection. However, ultrasonography indicated a possible parietal breach at the site of the lump. Multidetector computed tomography (CT) of the abdomen revealed a full-thickness defect over the left lumbar region with small bowel herniation (Fig 2).
Figure 2.
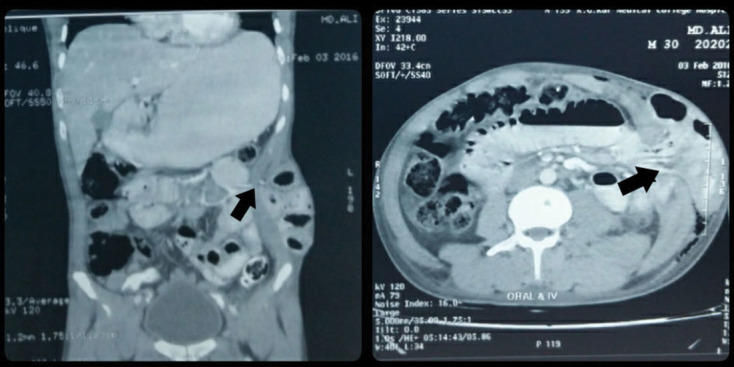
Computed tomography showing small bowel herniation through hernia site (arrow)
The patient was posted for an exploratory laparotomy by a midline approach. A 20cm loop of jejunum was found to be herniating through a gap of 7cm over the left lumbar region. A complete transection of the descending colon was also noted (Fig 3). Both the proximal and distal ends of the transected colon were also seen to be herniating through the defect. There was collection of stool and blood clots in the intraparietal cavity. The cavity was explored from the superficial surface and cleaned thoroughly (Fig 4). The defect was primarily closed with interrupted polypropylene sutures (Fig 5). The cavity was packed with antiseptic solution soaked mops and the wound was left open. The proximal end of the transected colon was converted to an end colostomy after mobilising the splenic flexure and the distal end was closed. The abdomen was closed after thorough peritoneal lavage.
Figure 3.

Intraoperative photograph showing hernial defect (white arrowhead), proximal (black arrowhead) and distal (black arrow) colonic transection
Figure 4.

Hernial site from superficial surface
Figure 5.

Hernial defect closure
During the immediate postoperative period, the wound became infected and there was localised abscess formation in the hernia cavity, which was drained.
Discussion
TAWH is encountered infrequently despite the high incidence of blunt abdominal trauma. Not surprisingly, more cases of TAWH have been reported in children owing to the thin parietal wall and more elastic skin.2 The first case of TAWH was reported by Selby in 1906.3 Strict criteria for diagnosis were first laid down by McWhorter, later modified by Clain and Damschen et al; these included immediate appearance of the swelling following blunt trauma and failure of the injury to penetrate the skin.1
The most common cause appears to be bicycle handlebar injury, especially in children.2 High velocity injuries are sustained during road traffic accidents. The pathophysiology leading to hernia development is believed to be the result of a tangential shearing force on the musculoaponeurotic layers associated with a sudden increase in intra-abdominal pressure, as occurs when performing the Valsalva manoeuvre.4
Wood et al attempted to classify the injuries into three types: small lower quadrant defects such as those resulting from handlebar injuries, larger abdominal wall defects such as those resulting from motor accidents and intra-abdominal herniations such as those resulting from a deceleration injury.4 The most common site of occurrence is the left lower quadrant of the abdomen but any quadrant can be affected.1
A tender subcutaneous swelling over the abdominal wall with an overlying bruise and ecchymosis is the usual mode of presentation. A high index of suspicion is necessary for diagnosis. There may be features of associated intra-abdominal injuries.1 In our case, the associated colonic injury was masked as the transected ends opened outside the peritoneal cavity.
Although ultrasonography can be used for screening, CT has been established as the gold standard investigation for diagnosis. It allows proper visualisation of the abdominal wall, and helps to differentiate between a rectus sheath haematoma and a hernia.5
The timing of repair of TAWH depends on the associated injuries and haemodynamic stability of the patient. Stable patients with a small defect require early repair. In unstable patients, the timing of repair is dependent on the size of the defect, risk of incarceration, associated hollow viscous injury and availability of biological mesh. Surgical repair can be via a midline approach or local exploration with primary closure of the defect, or by using mesh. In cases of associated hollow viscous injury with contamination, consideration should be given to use of biological mesh.6 TAWH has also been repaired successfully using a laparoscopic approach.5
Conclusions
Despite the high incidence of blunt abdominal injury, TAWH is rather rare and its diagnosis is often missed. It can be associated with other intra-abdominal injuries. Ultrasonography and multidetector CT are useful modalities for diagnosis but the findings should always be correlated clinically. A low threshold for early exploration is desirable to exclude any associated concealed, undiagnosed injury.
References
- 1.Singal R, Gupta R, Mittal A et al. Delayed presentation of the traumatic abdominal wall hernia; dilemma in the management – review of literature. Indian J Surg 2012; : 149–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chen HY, Sheu MH, Tseng LM. Bicycle-handlebar hernia: a rare traumatic abdominal wall hernia. J Chin Med Assoc 2005; : 283–285. [DOI] [PubMed] [Google Scholar]
- 3.Selby CD. Direct abdominal hernia of traumatic origin. JAMA 1906; : 1,485–1,486. [Google Scholar]
- 4.Wood RJ, Ney AL, Bubrick MP. Traumatic abdominal hernia: a case report and review of the literature. Am Surg 1988; : 648–651. [PubMed] [Google Scholar]
- 5.Munshi IA, Ravi SP, Earle DB. Laparoscopic repair of blunt traumatic anterior abdominal wall hernia. JSLS 2002; : 385–388. [PMC free article] [PubMed] [Google Scholar]
- 6.Hamidian Jahromi A, Skweres J, Sangster G et al. What we know about management of traumatic abdominal wall hernia: review of the literature and case report. Int Surg 2015; : 233–239. [DOI] [PMC free article] [PubMed] [Google Scholar]