

Abstract
Background:
Age estimation of living or deceased individuals is an important aspect of forensic sciences. Conventionally, pulp-to-tooth area ratio (PTR) measured from periapical radiographs have been utilized as a nondestructive method of age estimation. Cone-beam computed tomography (CBCT) is a new method to acquire three-dimensional images of the teeth in living individuals.
Aims:
The present study investigated age estimation based on PTR of the maxillary canines measured in three planes obtained from CBCT image data.
Settings and Design:
Sixty subjects aged 20–85 years were included in the study.
Materials and Methods:
For each tooth, mid-sagittal, mid-coronal, and three axial sections—cementoenamel junction (CEJ), one-fourth root level from CEJ, and mid-root—were assessed. PTR was calculated using AutoCAD software after outlining the pulp and tooth.
Statistical Analysis Used:
All statistical analyses were performed using an SPSS 17.0 software program.
Results and Conclusions:
Linear regression analysis showed that only PTR in axial plane at CEJ had significant age correlation (r = 0.32; P < 0.05). This is probably because of clearer demarcation of pulp and tooth outline at this level.
Key words: Age estimation, cone beam computed tomography, forensic odontology, forensic science, pulp-to-tooth area ratio
Introduction
Age estimation of living or deceased individuals is an important aspect of forensic investigation. Age is one of the triads of information that is vital to determine the identity in cases where visual recognition is not possible.[1] However, the role of aging in forensic investigations is not limited only to identification. In addition to the identification of extinct and extant populations, age changes can also be utilized in the context of crime investigation.[2] For example, age estimation can be vital to determining the quantum of punishment delivered to the accused, whose status of majority hinges on such evidence. Other uses of age estimation are in cases of immigrants (legal or otherwise) without concrete proof of age and birth records; age estimation is also useful to determine the status of majority (e.g. runaway brides). Therefore, age estimation covers both living and dead subjects, children, adolescents, and adult age groups.[3]
Teeth are one of the strongest structures in the human body, and the use and importance of teeth have long been recognized in age estimation. Dental age prediction in adults is based on quantification of morphological age-related changes of teeth such as secondary dentine deposition. It may be done precisely by histological and biochemical methods.[4] However, these techniques require extraction of teeth and usually, tooth sectioning/processing, which may not be feasible in living adults or for that matter in certain jurisdictions that prohibit tissue collection from human remains. Hence, methods that do not require tooth extraction or sectioning may be advocated for age evaluation.
The first recorded use of radiographic techniques in dental identification was by Schuller in 1921.[1] Its use in age estimation also spans more than a half-century. Kvaal et al.[5] were one of the early researchers to advocate dental age estimation in adults using radiographs. These authors proposed a number of length and width measurements of the tooth and pulp. Cameriere et al.[6] put forth a similar method for age estimation which, however, measured the tooth in two dimensions—specifically the tooth and pulp area. The method originally examined the maxillary canine but subsequently, included the second molar[7] and mandibular canine.[8] A similar study on mandibular canines has been done by Babshet et al.[9] on an Indian population. However, radiographs reproduce three-dimensional (3D) pulp as a 2D image. More recently, age estimation methods that use 3D volume ratio of the pulp cavity to the whole tooth in various types of single-rooted teeth using microfocus computed tomography have been reported.[10,11,12,13]
Cone beam CT (CBCT) has provided a new method to acquire 3D images of teeth in living individuals. It was introduced in 2000, allowing 3D imaging of the hard tissues in small volumes of the jaws.[14] CBCT is based on cone beam technology and uses a divergent source of ionizing radiation and a 2D area detector fixed on a rotating gantry to acquire multiple sequential projection images (basis images) in one complete scan around the area of interest.[15] Because cone beam reconstruction algorithms make it possible to reconstruct an entire volumetric region, this region can be reformatted to show anatomical detail in any imaginable plane.
The present study investigated age estimation based on the pulp-to-tooth area ratio (PTR) of maxillary canines measured in three planes (axial, sagittal, and coronal) obtained from CBCT image data.
Materials and Methods
Sixty adults of Indian origin (30 males, 30 females) visiting the Department of Oral Medicine and Radiology in our institution for consultation and diagnosis were included as study subjects. Subjects' age ranged between 20 and 85 years and was well-distributed across different age groups [Table 1]. The CBCT examinations were made using Kodak 9000 3D digital imaging system. Occlusal plane was positioned horizontally to the scan plane and the mid-sagittal plane was centered vertically to the scan plane. The scan volume was centered so that the maxillary canines were in the center. Images were obtained at 70–74 kV, 10 mA, and 10.8 s with a voxel size of 76.5 µm3. A limited volume (50 mm × 37 mm) 3D image was obtained from the area of interest, with a 200 µm image resolution. The acquired volumes were reformatted to a thickness of 200 µm images. For CBCT evaluation, 19-inch LCD monitor with 1280 pixel × 1024 pixel resolution, 800:1 contrast ratio was used. The KODAK Dental Imaging Software 6.8 Windows edition (Carestrean Health Inc., New York, USA) was used. The data of CBCT images were sliced in three dimensions [Figure 1]. In the axial plane, three sections representing cementoenamel junction (CEJ), one-fourth root length from CEJ, and mid-root level were assessed. For the sagittal plane, curved slices oriented along the curve of the maxillary arch were delineated. The cursor was oriented parallel to the long axis of the maxillary canine to obtain the mid-sagittal plane. With respect to the coronal plane, oblique slicing was done to obtain the mid-coronal section along the long axis of the tooth. These images were exported as 8-bit TIFF images, opened in Adobe Photoshop® CS2 image-editing software program (Adobe Systems Inc., Mountain View, CA, USA), and saved as high-resolution JPEG files on a desktop computer. The images were imported to AutoCAD 2004 computer-aided drafting program (Autodesk Inc., San Rafael, CA, USA). For each image, at least thirty points were marked on the outline of the tooth using the point tool on AutoCAD's Draw Toolbox; a minimum of 10 points was also marked on the pulp outline [Figure 2]. The points were connected using the line tool, also on the Draw Toolbox, and area was obtained for both tooth and pulp of that image [Figure 3]. This entire procedure was performed for all the five sections of each tooth. The data were entered in Microsoft Office 2007 Excel spreadsheet (Microsoft Corp., Redmond, WA, USA) and PTR calculated for all the five CBCT sections for each tooth. The PTR data obtained for each of the five sections (across the three planes) were subjected to regression analysis; their correlation to chronologic age (r) as well as the standard error of the estimate (SEE) was derived. A multiple regression analysis was also undertaken with all five independent variables entered together to determine if this improved the correlation and SEE. Repeat measurements were undertaken by the primary examiner (AR) on each of the five sections (across the three planes) for ten of the sixty subjects, and the values subjected to a paired t-test to assess potential intra-observer error. All statistical analyses were performed using an SPSS 17.0 software program (SPSS Inc., Chicago, USA; now IBM Corp., Armonk, USA).
Table 1.
Age- and sex-wise distribution of patients included in the study
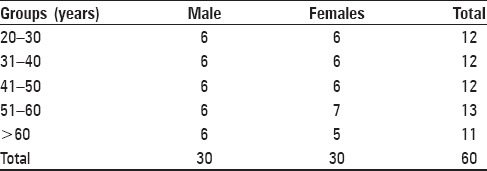
Figure 1.
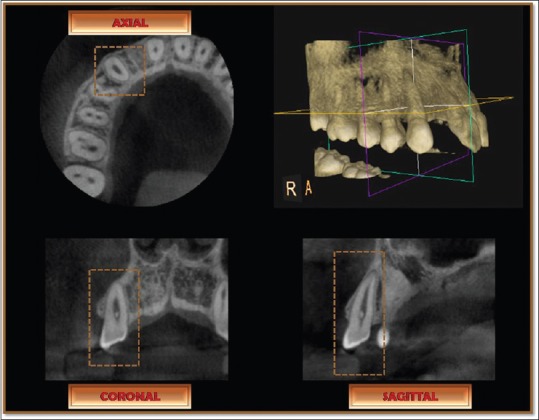
Cone beam computed tomography images of maxillary right arch obtained for the study subjects are shown in three-dimensional, axial, coronal, and sagittal views
Figure 2.
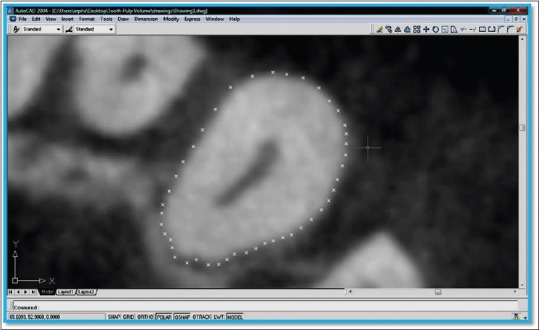
The axial section image at cementoenamel junction level seen in AutoCAD 2004 computer-aided drafting program with more than 30 points marked on the outline of the tooth using the point tool on AutoCAD's draw toolbox
Figure 3.
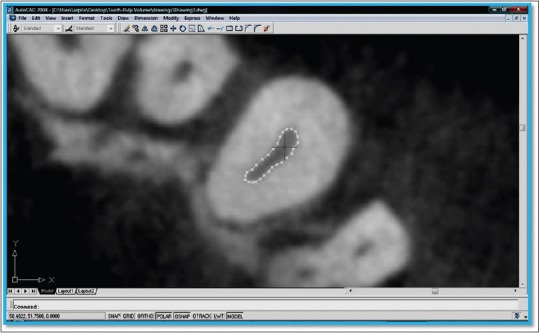
The axial section image at cementoenamel junction level seen in AutoCAD 2004 computer-aided drafting program with more than 10 points marked on the pulp outline which were connected using the line tool on the draw toolbox
Results
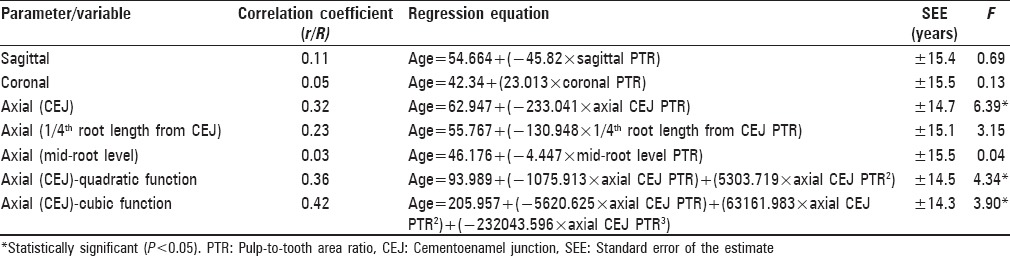
The regression analysis revealed that the PTR obtained in the sagittal, coronal, and two of the axial planes (one-fourth the distance from CEJ on the root and mid-root level) were low and statistically insignificant (P > 0.05) [Table 2]. The PTR obtained in the axial plane taken at the CEJ, alone, produced a statistically significant correlation (P < 0.05), albeit this too was low [Table 2]. Running a quadratic and cubic regression analysis for this variable produced marginally higher correlations which were also statistically significant (P < 0.05). The correlation for the cubic function alone was moderate in nature (R = 0.42). The quadratic and cubic regression analysis for the remaining four sections did not yield a statistically significant correlation, and hence, those results are not published here.
Table 2.
Pearson correlation coefficient (r), standard error of the estimate, F values, and the regression equations for the different ratios
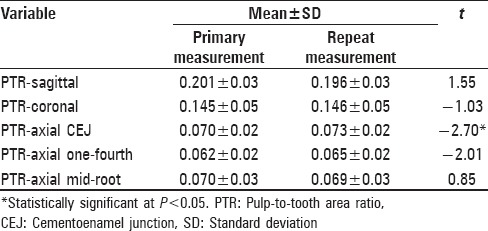
The paired t-test revealed statistically insignificant intra-observer differences (P > 0.05) for all but one of the sections, the exception being the PTR obtained for axial plane taken at the CEJ [Table 3]; however, the difference between the mean ratios of the primary and repeat evaluations is small.
Table 3.
The mean standard deviation and t values of the for the primary measurements and corresponding repeat evaluations of pulp-to-tooth area ratio on the five sections (across the three planes) for 10 of the 60 subjects
Discussion
Age estimation is an important aspect of forensic odontology, and in our experience, postmortem age estimation using radiography has been used extensively—particularly, using the dimensional changes of the pulp area in relation to the tooth area and the ratio therein. The assessment of PTR is an indirect quantification of secondary dentine deposition and generally correlates well with the chronological age of the subject.[6,8,16] Secondary dentine—which is encased by harder tissue such as enamel and cementum and in addition, by primary dentine—is preferred for age estimation.[8] Better correlation with chronologic age by the assessment of secondary dentine is thought to result since it may be more insulated from the effect of environmental factors on human remains.[17]
The introduction of CBCT creates new opportunities to get 3D tooth views, resulting in a reasonable image quality at a low-radiation dose (skin dose 1.19 mSv, total dose 20 mSv per examination).[18] There are several advantages of CBCT over conventional radiographic methods, including controlled magnification, lack of superimposition, absence of geometric distortion, and convenient multiplanar and 3D displays, which allow improved structure visualization and diagnostic efficacy.[19]
Although CBCT technology was originally introduced as state-of-the-art imaging, it has entered the mainstream dentistry and is becoming increasingly available to the dentists. The present study, therefore, explored the potential use of this, almost routine, technology in the field of forensics for age estimation using PTR of the maxillary canines.
The results of the present study did not show statistically significant correlation of PTR to age in the coronal plane. This could be attributed to the difficulty in deciding the representative section, which did not show the complete outline of the tooth and the pulp in one section. Even though oblique sections oriented to the long axis of the tooth were used to achieve the mid-coronal section, it was difficult to achieve a section that showed the complete outline of the tooth and the pulp in one single section. We tried to circumvent this problem by increasing the section thickness from 200 µm to up to 1000 µm (i.e., 1 mm), but the resultant poor resolution made it difficult to outline the tooth and more particularly, the pulp. The poor results for the coronal plane may be explained partly by the anatomical orientation of the pulp chamber of the maxillary canines, which is in a bucco-palatal plane.
We did not obtain a significant correlation between age and the sagittal plane also (P > 0.05). Considering the pattern of secondary dentine deposition and orientation of pulp chamber in the bucco-palatal plane, a significant correlation with age was anticipated in this plane. Perhaps, a more 3D quantification is necessary for this; we therefore suggest that in future, PTR in several sections in the sagittal plane have also be undertaken, which may give a higher correlation to age.
The present study found that the best, and the only statistically significant, correlation with age was observed for the axial plane at the CEJ (which was also higher compared to the axial plane at one-fourth the distance from the CEJ on the root and the mid-root level). This may be attributed to the clearer demarcation of the pulp and the tooth outline in the CEJ section as compared to those more apically. This highlights the limitations of CBCT related to cone beam projection geometry, detector sensitivity, and contrast resolution. The cone beam projection geometry results in a large volume being irradiated with every basis image projection. This results in increased Compton scattering interaction and high image noise which contributes to image degradation. At more apical root levels from CEJ, the soft tissue area (pulp) reduces in comparison to the dentine-cementum encasing around it, contributing more to the image noise in these sections.
Comparison of Pearson's correlation coefficient (r) in previous studies using PTR in age estimation reveals that its value is much higher than in the present study.[6,8] However, the present study has a comparable r value to previous studies undertaken on Indian populations,[9,20,21] which underscores the potential limitation of radiographic assessment of secondary dentinal formation in this country. It has been suggested that modest correlations may be inherent in Indians, precluding optimal age estimation,[22] and the findings of the present study reinforce the same. Coupled with the significant observer variation (P < 0.05) for the one variable which showed statistical correlation to age (PTR obtained in an axial plane taken at the CEJ), it appears that the use of PTR using CBCT must be undertaken guardedly.
However, the sample size for this study is small as the results reported here are preliminary analysis. Further investigations with higher sample size and comparing different CBCT scanners and different resolutions of the image sections are needed to make conclusions regarding the use of CBCT for age estimation.
Conclusions
CBCT technology offers 3D visualization and more complex and more accurate imaging compared to analog and digital radiographs. Increasing availability of this technology provides the forensic odontologist with an imaging modality capable of providing a 3D representation of the teeth and the jaws whose benefits may be extended in several ways to the science of forensic odontology. In the present study, age estimation using the PTR in several planes was undertaken using CBCT data. However, the results herein do not demonstrate any practical advantage of CBCT in terms of correlation with age and error rates, and its use may be limited also by issues related to repeatability. We recognize that the nature of this study is preliminary and the method may need to be further explored with larger sample size and multiple section analysis in every plane to ascertain the potential of this imaging modality in the field of forensic odontological age assessment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Wood RE. Forensic aspects of maxillofacial radiology. Forensic Sci Int. 2006;159(Suppl 1):S47–55. doi: 10.1016/j.forsciint.2006.02.015. [DOI] [PubMed] [Google Scholar]
- 2.Gustafson G. Age determination on teeth. J Am Dent Assoc. 1950;41:45–54. doi: 10.14219/jada.archive.1950.0132. [DOI] [PubMed] [Google Scholar]
- 3.Solheim T, Vonen A. Dental age estimation, quality assurance and age estimation of asylum seekers in Norway. Forensic Sci Int. 2006;159(Suppl 1):S56–60. doi: 10.1016/j.forsciint.2006.02.016. [DOI] [PubMed] [Google Scholar]
- 4.Ohtani S. Estimation of age from the teeth of unidentified corpses using the amino acid racemization method with reference to actual cases. Am J Forensic Med Pathol. 1995;16:238–42. doi: 10.1097/00000433-199509000-00010. [DOI] [PubMed] [Google Scholar]
- 5.Kvaal SI, Kolltveit KM, Thomsen IO, Solheim T. Age estimation of adults from dental radiographs. Forensic Sci Int. 1995;74:175–85. doi: 10.1016/0379-0738(95)01760-g. [DOI] [PubMed] [Google Scholar]
- 6.Cameriere R, Ferrante L, Cingolani M. Variations in pulp/tooth area ratio as an indicator of age: A preliminary study. J Forensic Sci. 2004;49:317–9. [PubMed] [Google Scholar]
- 7.Cameriere R, Ferrante L, Cingolani M. Precision and reliability of pulp/tooth area ratio (RA) of second molar as indicator of adult age. J Forensic Sci. 2004;49:1319–23. [PubMed] [Google Scholar]
- 8.Cameriere R, Ferrante L, Belcastro MG, Bonfiglioli B, Rastelli E, Cingolani M. Age estimation by pulp/tooth ratio in canines by peri-apical x-rays. J Forensic Sci. 2007;52:166–70. doi: 10.1111/j.1556-4029.2006.00336.x. [DOI] [PubMed] [Google Scholar]
- 9.Babshet M, Acharya AB, Naikmasur VG. Age estimation in Indians from pulp/tooth area ratio of mandibular canines. Forensic Sci Int. 2010;197:125.e1–4. doi: 10.1016/j.forsciint.2009.12.065. [DOI] [PubMed] [Google Scholar]
- 10.Vandevoort FM, Bergmans L, Van Cleynenbreugel J, Bielen DJ, Lambrechts P, Wevers M, et al. Age calculation using x-ray microfocus computed tomographical scanning of teeth: A pilot study. J Forensic Sci. 2004;49:787–90. [PubMed] [Google Scholar]
- 11.Aboshi H, Takahashi T, Komuro T, Fukase Y. A method of age estimation basedon the morphometric analysis of dental pulp in mandibular first premolars by means of three-dimensional measurements taken by micro CT. Nihon Univ Dent J. 2005;49:195–203. [Google Scholar]
- 12.Someda H, Saka H, Matsunaga S, Ide Y, Nakahara K, Hirata S, et al. Age estimation based on three-dimensional measurement of mandibular central incisors in Japanese. Forensic Sci Int. 2009;185:110–4. doi: 10.1016/j.forsciint.2009.01.001. [DOI] [PubMed] [Google Scholar]
- 13.Aboshi H, Takahashi T, Komuro T. Age estimation using microfocus x-ray computed tomography of lower premolars. Forensic Sci Int. 2010;200:35–40. doi: 10.1016/j.forsciint.2010.03.024. [DOI] [PubMed] [Google Scholar]
- 14.Arai Y, Tammisalo E, Iwai K, Hashimoto K, Shinoda K. Fundamental efficiency of limited cone-beam x-ray CT (3DX multi image micro CT) for practical use. Dent Radiol. 2000;40:145–54. [Google Scholar]
- 15.Scarfe WC, Farman AG. Cone beam computed tomography. In: White SC, Pharoah MJ, editors. Oral Radiology: Principles and Interpretation. 6th ed. St. Louis: Elsevier; 2008. pp. 225–43. Ch. 14. [Google Scholar]
- 16.Jeevan MB, Kale AD, Angadi PV, Hallikerimath S. Age estimation by pulp/tooth area ratio in canines: Cameriere's method assessed in an Indian sample using radiovisiography. Forensic Sci Int. 2011;204:209.e1–5. doi: 10.1016/j.forsciint.2010.08.017. [DOI] [PubMed] [Google Scholar]
- 17.Cameriere R, Brogi G, Ferrante L, Mirtella D, Vultaggio C, Cingolani M, et al. Reliability in age determination by pulp/tooth ratio in upper canines in skeletal remains. J Forensic Sci. 2006;51:861–4. doi: 10.1111/j.1556-4029.2006.00159.x. [DOI] [PubMed] [Google Scholar]
- 18.Yang F, Jacobs R, Willems G. Dental age estimation through volume matching of teeth imaged by cone-beam CT. Forensic Sci Int. 2006;159(Suppl 1):S78–83. doi: 10.1016/j.forsciint.2006.02.031. [DOI] [PubMed] [Google Scholar]
- 19.Kamburoglu K, Kiliç C, Ozen T, Horasan S. Accuracy of chemically created periapical lesion measurements using limited cone beam computed tomography. Dentomaxillofac Radiol. 2010;39:95–9. doi: 10.1259/dmfr/85088069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Babshet M, Acharya AB, Naikmasur VG. Age estimation from pulp/tooth area ratio (PTR) in an Indian sample: A preliminary comparison of three mandibular teeth used alone and in combination. J Forensic Leg Med. 2011;18:350–4. doi: 10.1016/j.jflm.2011.07.003. [DOI] [PubMed] [Google Scholar]
- 21.Kanchan-Talreja P, Acharya AB, Naikmasur VG. An assessment of the versatility of Kvaal's method of adult dental age estimation in Indians. Arch Oral Biol. 2012;57:277–84. doi: 10.1016/j.archoralbio.2011.08.020. [DOI] [PubMed] [Google Scholar]
- 22.Acharya AB, Vimi S. Effectiveness of Bang and Ramm's formulae in age assessment of Indians from dentin translucency length. Int J Legal Med. 2009;123:483–8. doi: 10.1007/s00414-009-0346-7. [DOI] [PubMed] [Google Scholar]