

A 42-year-old woman presented with recurrent acid regurgitation and heartburn. On initial upper endoscopy, multiple mucosal breaks were seen in the lower esophagus, but no abnormalities were observed in the stomach (Fig. 1). The patient took proton pump inhibitors for consistent reflux symptoms and reflux esophagitis. On follow-up endoscopy 4 years later, confluence of mucosal breaks and stenosis were seen at the lower esophagus and multiple polyps were found throughout the body of the stomach, which were diagnosed as fundic gland polyps by endoscopic biopsies. She continued maintenance therapy of proton pump inhibitors twice daily. Follow-up endoscopy at 2 years later showed more numerous and enlarged fundic gland polyps compared to the previous endoscopy (Fig. 2).
Figure 1.
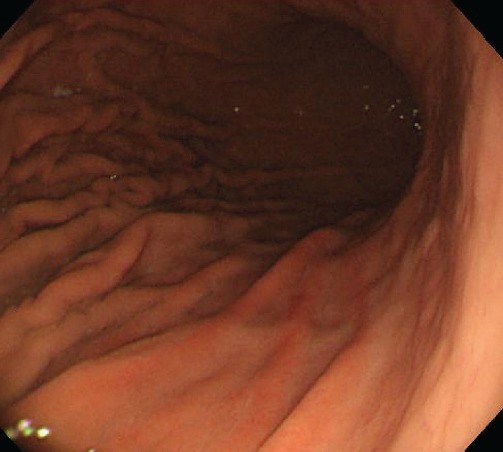
Initial esophagogastroduodenoscopy shows no abnormal findings in the stomach.
Figure 2.
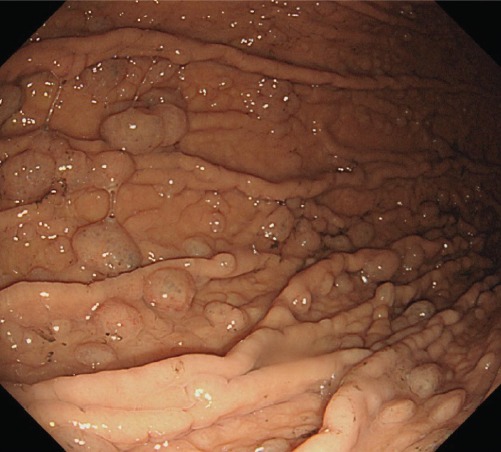
Multiple polyps are noted throughout the body of the stomach 6 years later after continuous proton pump inhibitor therapy.
Fundic gland polyps are benign, multiple, sessile, localized lumps, usually detected in the gastric body and fundus. Cystic dilatation of pits which is located in the deep mucous neck cell is one of characteristics of fundic gland polyps and they are usually observed with chief cells and parietal cells lining those microcysts. In the past, it is reported that fundic gland polyps are mainly associated with hereditary diseases. Recently, fundic gland polyps have become increasingly detected in patients who are treated with long-term proton pump inhibitor therapy. Generally, the risk for occurrence of fundic gland polyps increases after 12 months of proton pump inhibitor use. When chronic acid suppression therapy is applied, substantial physiological changes such as increased circulating gastrin and chromogranin A occur and these hormonal changes stimulate fundic gland proliferation.
Footnotes
No potential conflict of interest relevant to this article was reported.