

Abstract
Background
The insertion of central venous catheters (CVCs) may be associated with peri‐ and post‐procedural bleeding. People who require a central line often have disorders of coagulation as a result of their underlying illness, co‐morbidities or the effects of treatment. Clinical practice in some institutions is to mitigate the risk of bleeding in these patients by prophylactically transfusing fresh frozen plasma (FFP) in order to correct clotting factor deficiencies prior to central line insertion. However, FFP transfusion is not without risk, and it remains unclear whether this intervention is associated with reduced rates of bleeding or other clinically‐meaningful outcomes.
Objectives
To assess the effect of different prophylactic plasma transfusion regimens prior to central line insertion in people with abnormal coagulation.
Search methods
We searched for randomised controlled trials (RCTs) in the Cochrane Central Register of Controlled Trials (CENTRAL) (the Cochrane Library 2016, Issue 3), PubMed (e‐publications only), Ovid MEDLINE (from 1946), Ovid Embase (from 1974), the Transfusion Evidence Library (from 1950) and ongoing trial databases to 1 March 2016.
Selection criteria
We included RCTs involving transfusions of plasma to prevent bleeding in people of any age with abnormal coagulation requiring insertion of a central venous catheter, published in English.
Data collection and analysis
We used standard methodological procedures expected by Cochrane.
Main results
We identified four trials eligible for inclusion, of which three are ongoing. We did not exclude any studies because they were not published in English.
The included study randomised 81 adults in intensive care whose INR (International Normalised Ratio) was greater than or equal to 1.5 to no FFP or to a single dose of 12 mL/kg FFP prior to undergoing central venous catheterisation (58 participants) or other invasive procedure (23 participants). It is the subgroup of 58 adults undergoing CVC insertion that were included in this review, the study authors provided unpublished data for this review's outcomes.
The quality of the evidence was low or very low across different outcomes according to the GRADE methodology. The included study was at high risk of bias due to lack of blinding of participants and personnel and imbalance in the number of participants who had liver disease between study arms.
There was insufficient evidence to determine a difference in major procedure‐related bleeding within 24 hours (one RCT; 58 participants; no events in either study arm, very low‐quality evidence). We are very uncertain whether FFP reduces minor procedure‐related bleeding within 24 hours of the study (one RCT; 58 participants, RR 0.67, 95% CI 0.12 to 3.70, very low‐quality evidence).
No studies were found that looked at: all‐cause mortality; the proportion of participants receiving plasma or red cell transfusions; serious adverse reactions (transfusion or line‐related complications); number of days in hospital; change in INR; or quality of life.
The three ongoing studies are still recruiting participants (expected recruitment: up to 355 participants in total). and are due to be completed by February 2018.
Authors' conclusions
There is only very limited evidence from one RCT to inform the decision whether or not to administer prophylactic plasma prior to central venous catheterisation for people with abnormal coagulation. It is not possible from the current RCT evidence to recommend whether or not prophylactic plasma transfusion is beneficial or harmful in this situation. The three ongoing RCTs will not be able to answer this review’s questions, because they are small studies and do not address all of the comparisons included in this review (355 participants in total). To detect an increase in the proportion of participants who had major bleeding from 1 in 100 to 2 in 100 would require a study containing at least 4634 participants (80% power, 5% significance).
Plain language summary
Plasma transfusions prior to insertion of central lines for people with abnormal coagulation
Review question We evaluated the evidence about whether people with abnormal coagulation (poor blood clotting) require a plasma transfusion prior to insertion of a central line (central venous catheter (CVC)), and if so, what is the degree of abnormal coagulation at which a plasma transfusion is required.
Background People with abnormal coagulation often require the insertion of central lines. Central lines are catheters whose tip usually lies in one of two main veins returning blood to the heart. They have a number of uses including: intensive monitoring and treatment of critically‐ill patients; giving nutrition into a vein (when the patient cannot eat); giving chemotherapy or other irritant drugs with fewer complications; and when patients require long‐term repeated treatments in to a vein. Current practice in many countries is to give plasma transfusions to prevent serious bleeding due to the procedure if blood tests to assess clotting are abnormal. The risk of bleeding after a central line insertion appears to be low if the clinician uses ultrasound to guide insertion of the line. Correction of clotting abnormalities with fresh frozen plasma (FFP) is not without risks of its own, and it is unclear whether this practice is beneficial or harmful. People may be exposed to the risks of a plasma transfusion without any obvious clinical benefit.
Study characteristics The evidence is current to March 2016. In this review we identified four randomised controlled trials, three trials are still recruiting participants and are due to complete recruitment by February 2018. The completed trial (58 participants) compared plasma transfusion to no plasma transfusion prior to central line insertion.
Key results There was not enough evidence to determine whether plasma transfusions affected minor or major procedure‐related bleeding. The included study did not report the number of people dying due to any cause, the number of people receiving red cell or plasma transfusions, the occurrence of transfusion or line‐related complications, length of time in hospital, correction of clotting abnormalities, or quality of life.
Quality of the evidence The quality of the evidence is very low because this review includes only one small study.
Authors' conclusions
The ongoing studies (expected to recruit 355 participants in total) will be unable to provide sufficient data for this review’s primary outcomes because major bleeding and mortality are uncommon. We would need to design a study with at least 4634 participants to be able to detect an increase in the number of people who had major bleeding from 1 in 100 to 2 in 100. It is not possible from the current randomised controlled trial evidence to recommend whether or not prophylactic plasma transfusion is beneficial or harmful in this situation.
Summary of findings
Summary of findings for the main comparison. Comparison of plasma transfusions versus no plasma transfusions when the INR is 1.5 prior to central venous catheter insertion.
| Comparison of plasma transfusions versus no plasma transfusions | ||||||
| Patient or population: people with abnormal coagulation requiring a central venous catheter Setting: In hospital Intervention: prophylactic plasma transfusion Comparison: no plasma transfusions | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with no plasma transfusions | Risk with prophylactic plasma transfusion | |||||
| Major procedure‐related bleeding follow‐up: 24 hours | There were no major procedure‐related bleeds in either of the study arms | Not estimable |
58 (1 RCT) |
⊕⊝⊝⊝ VERY LOW 1 2 | ||
| All‐cause mortality follow‐up: 30 days | ‐ | ‐ | ‐ | ‐ | Not reported |
|
| Respiratory deterioration attributable to transfusion‐associated circulatory overload (TACO), transfusion‐related acute lung injury (TRALI) or transfusion‐associated dyspnoea (TAD) | ‐ | ‐ | ‐ | ‐ | ‐ | Not reported |
| Minor procedure‐related bleeding follow‐up: 24 hours | Study population | RR 0.67 (0.12 to 3.70) | 58 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 2 3 | ||
| 103 per 1000 | 69 per 1000 (12 to 383) | |||||
| Proportion of participants receiving plasma transfusions | ‐ | ‐ | ‐ | ‐ | ‐ | Not reported |
| Line‐related complications | ‐ | ‐ | ‐ | ‐ | ‐ | Not reported |
| Quality of life | ‐ | ‐ | ‐ | ‐ | ‐ | Not reported |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded by 2 for very serious imprecision. The included study was a small study and this is a rare outcome with no events in either study arm
2 Downgraded by 1 for serious risk of bias. There was a high risk of performance bias and other bias
3 Downgraded by 2 for very serious imprecision. The included study was a small study and the 95% confidence interval of the risk ratio includes the possibility of significant harm or significant benefit.
Background
Description of the condition
Coagulopathy refers to the condition in which the blood's ability to clot is impaired (Hunt 2014). People requiring a central line (central venous catheter (CVC)) often become coagulopathic as a consequence of their underlying illness, co‐morbidities or the effects of treatment. Central venous catheters are catheters with tips that lie within the proximal third of the superior vena cava, the right atrium or the inferior vena cava (Bishop 2007; Smith 2013). They can be inserted through a superficial vein (e.g. the basilic or cephalic veins in the arm) or a central vein (most commonly the internal jugular, subclavian or femoral veins) (Bishop 2007; Smith 2013). There are four main types: 1) a non‐tunnelled line into a central vein (short‐term use); 2) a line inserted into a superficial vein (medium‐term use); 3) a tunnelled line (long‐term use); 4) a totally implanted device (long‐term use) (Bishop 2007; Smith 2013). They have a number of uses, these include: administration of chemotherapy and other irritant drugs with fewer complications; intensive monitoring and treatment of critically ill patients; administration of total parenteral nutrition; and long‐term intermittent intravenous access for patients requiring repeated treatments (Smith 2013). People requiring CVCs can have a variety of conditions and include people with liver failure, people who are critically ill and people requiring chemotherapy (Bishop 2007; Smith 2013).
A large national study of fresh frozen plasma (FFP) use in critical illness reported that 30% of people admitted to the intensive care unit (ICU) developed an abnormality of coagulation (Walsh 2010). The aetiology of coagulopathy in critical illness is complex and multi‐factorial; sepsis, haemodilution, haemorrhage, disseminated intra‐vascular coagulation, hepatic and renal disease and anti‐coagulant medication are all implicated (Hunt 2014). The causes of coagulopathy in non‐critically ill people undergoing CVC insertion are similarly broad. FFP is widely used in the management of coagulopathic patients with abnormal laboratory tests of blood coagulation (prolonged prothrombin time (PT) or elevated international normalised ratio (INR)), and may be administered as part of the resuscitation of actively bleeding patients, or as prophylaxis to prevent bleeding in coagulopathic patients undergoing invasive procedures such as CVC insertion.
Description of the intervention
Current practice in many centres is to correct disordered coagulation with FFP transfusion prior to internal jugular, femoral or subclavian venous catheterisation, in order to mitigate the risk of serious peri‐ or post‐procedural bleeding. Plasma is the non‐cellular component of blood and is prepared either from the centrifugation of whole blood or by plasmapheresis (Benjamin 2012). FFP refers to plasma that is frozen within eight hours to ‐30°C, whereas frozen plasma (F24) is that which is frozen within 24 hours. Both contain concentrations of clotting factors equivalent to those found in in vivo blood, although the levels of factor V and VIII fall rapidly on thawing (Stanworth 2007). Current recommendations regarding the correction of coagulopathy prior to CVC insertion reflect expert opinion rather than high‐quality evidence from randomised controlled trials. An INR greater than or equal to 1.5 is frequently advocated as the threshold above which patients should undergo correction of coagulopathy prior to CVC insertion (Bishop 2007; Hunt 2014). Whilst the use of standard laboratory tests of coagulation to assess bleeding has been criticised, an INR over 1.5 demarcates the level above which the activity of some coagulation factors falls to less than 50% (Juffermans 2014). An alternative approach to transfusing based on an INR threshold (which only detects low coagulation factor levels) is to use a test such as rotational thromboelastometry (ROTEM) or thromboelastography (TEG) that assesses how well a blood clot forms in whole blood (haemostasis). ROTEM and TEG not only assess coagulation factor function, but also platelet function, strength of the clot and whether the clot is rapidly broken down.
Recent studies report that 15% to 26% of non‐bleeding critically ill patients receive prophylactic FFP transfusions prior to an invasive procedure such as CVC insertion (Dara 2005; Stanworth 2010; Stanworth 2011). However, there remains substantial heterogeneity in clinicians' views about the effectiveness of this intervention, with doubts over its effectiveness and the balance of the risk‐benefit ratio (Watson 2011).
How the intervention might work
Plasma transfusion is administered to coagulopathic patients in order to correct multiple clotting factor deficiencies and therefore reduce the incidence of bleeding. However, although a dose of 10 mL to 15 mL/kg is required to significantly improve the INR (O'Shaughnessy 2004), patients are commonly under‐dosed and therefore exposed to the risks associated with FFP transfusion, but not the proposed benefits (Hall 2012). It remains unclear whether FFP transfusion in coagulopathic non‐bleeding patients, despite improving standard laboratory tests of coagulation, reduces the incidence of clinically important bleeding or improves other meaningful patient‐oriented outcomes such as mortality. Clinical studies also indicate that the INR is often minimally reduced following FFP administration, especially when only modestly increased pre‐transfusion (Stanworth 2011).
Risks associated with the intervention
The risks associated with FFP transfusion include transfusion‐associated lung injury (Khan 2007; Rana 2006), transfusion‐associated circulatory overload (Narick 2011), multi‐organ failure (Watson 2009), and sepsis (Sarani 2008). The requirement to administer FFP to correct coagulopathy prior to central line insertion may additionally delay the start of treatments such as vasoactive medication, which may be time‐critical in an emergency situation. Delays in initiating treatment may lead to poorer patient outcomes (increased morbidity and mortality).
Why it is important to do this review
The evidence to support the use of prophylactic FFP transfusion in coagulopathic patients requiring CVC insertion is weak (Hunt 2014; Stanworth 2007; Tinmouth 2011). There is no high‐quality evidence, outside the setting of major trauma and haemorrhagic shock, that FFP administration improves mortality (Murad 2010). Standard laboratory tests of coagulation poorly reflect in vivo haemostasis (Holland 2006), and abnormalities in INR and PT may not increase the risk of bleeding during CVC insertion (Segal 2005). Several case series have demonstrated the safety of performing invasive procedures without clinically significant bleeding in patients with an elevated INR who did not receive FFP cover (Doerfler 1996; Fisher 1999; Foster 1992; Haas 2010; Mumtaz 2000; Weigand 2009). The use of an INR threshold above which FFP transfusion is required prior to CVC insertion has therefore been called into question. It is uncertain whether plasma transfusions are effective at preventing bleeding in patients with deranged coagulation undergoing an invasive procedure. If effective, the INR threshold above which plasma transfusions are clinically effective is also uncertain. Wide variation in the use of FFP prior to central venous catheterisation exists, indicating significant clinician uncertainty and potentially exposing patients to varying risk (Watson 2011).
Objectives
To assess the effect of different prophylactic plasma transfusion regimens prior to central line insertion in people with abnormal coagulation.
Methods
Criteria for considering studies for this review
Types of studies
We included only randomised controlled trials (RCTs), irrespective of publication status published in English.
Types of participants
We included study participants of any age with abnormal coagulation (as defined by the studies) requiring insertion of a central venous catheter (CVC) (tunnelled or untunnelled), or porta‐cath. We excluded participants who were experiencing clinically significant bleeding at the time of the catheter insertion because such participants are routinely resuscitated with blood products including plasma.
Types of interventions
We included RCTs comparing two types of plasma transfusion policy.
-
No plasma transfusion prior to central line insertion versus:
plasma transfusion prior to central line insertion when the INR is 1.5 to 3 times control; OR
plasma transfusion when the INR is greater than 3 times control; OR
plasma transfusion when rotational thromboelastography (TEG) is above a certain threshold (as defined by the study).
-
Plasma transfusion prior to central line insertion when the INR is greater than 1.5 times control versus:
plasma transfusion prior to central line insertion when the INR is 2 to 3 times control; OR
plasma transfusion when the INR is greater than 3 times control; OR
plasma transfusion when rotational TEG is above a certain threshold (as defined by the study).
We planned to report each analysis separately, as subgroups within the two main comparisons.
Types of outcome measures
Primary outcomes
Major procedure‐related bleeding within 24 hours of the procedure.
Defining procedure‐related bleeds can be challenging as coagulopathic participants may bleed spontaneously in the absence of an intervention. We have sought to capture this group as accurately as possible by excluding participants who are already actively bleeding at the time of CVC insertion, and by defining 'procedure‐related bleeding' as that causing a significant fall in haemoglobin (Hb), e.g. 20 g/L or greater in the absence of another cause; a fall in systolic blood pressure (SBP) of at least 20 mmHg or an increase in heart rate (HR) of at least 20 beats per minute (BPM) or greater; haemothorax (blood in the space between the outside of the lungs and the inside of the chest wall); requiring an intervention such as a transfusion to treat bleeding; or major bleeding (not further defined) as reported by individual studies.
All‐cause mortality up to 30 days after the procedure.
Secondary outcomes
Minor procedure‐related bleeding within 24 hours of the procedure (defined as prolonged bleeding at the insertion site, which only requires treatment with a pressure bandage, or haematoma at the insertion site), or minor bleeding (not further defined) as reported by individual studies.
Serious adverse events:
Transfusion‐related complications within 24 hours of the procedure (including transfusion‐related acute lung injury (TRALI), transfusion‐transmitted infection, transfusion‐associated circulatory overload (TACO), transfusion‐associated dyspnoea (TAD), acute transfusion reactions);
Line‐related complications within seven days of the procedure (infection, thrombosis, other).
Total number of days in hospital.
Proportion of participants receiving plasma transfusions and red cell transfusions within 24 hours of the procedure.
Change in INR up to 24 hours following the procedure.
Quality of life, as defined by the individual studies.
Search methods for identification of studies
The Systematic Review Initiative's Information Specialist (CD) formulated the search strategies in collaboration with the Cochrane Haematological Malignancies Group.
Electronic searches
We limited our searches to five main electronic databases and two ongoing trial databases:
Cochrane Central Register of Controlled Trials (CENTRAL, 2016, issue 3, (1 March 2016)) (Appendix 1);
PubMed (e‐publications only up to 1 March 2016) (Appendix 2);
MEDLINE (1946 to 1 March 2016) (Appendix 3);
Embase (1974 to 1 March 2016) (Appendix 4);
Transfusion Evidence Library (www.transfusionevidencelibrary.com) (1950 to 1 March 2016) (Appendix 5)
We searched for ongoing RCTs to 1 March 2016 in the following databases:
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (Appendix 6);
ClinicalTrials.gov (Appendix 7).
We combined searches in MEDLINE with the Cochrane RCT highly sensitive search filter, as detailed in Chapter six of the Cochrane Handbook for Systematic Reviews of Interventions (Lefebvre 2011). We combined searches in Embase with the relevant SIGN (Scottish Intercollegiate Guidelines Network) RCT studies filter (www.sign.ac.uk/methodology/filters.html). We excluded studies published in languages other than English. We did not limit searches by year of publication or publication type.
Searching other resources
We handsearched the reference lists of included studies in order to identify further relevant studies, and made contact where appropriate with lead authors of included studies to identify any unpublished material, missing data or information regarding ongoing studies.
Data collection and analysis
Selection of studies
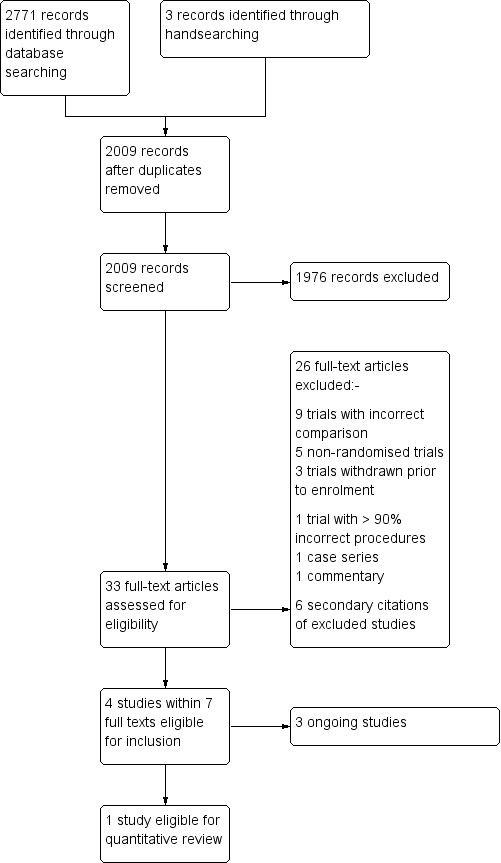
We selected studies for inclusion with reference to Chapter seven of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011a). The Systematic Review Initiative's Information Specialist (CD) initially screened all search hits for relevance against the eligibility criteria and discarded all those that were clearly irrelevant. Thereafter, two review authors (DH, LE) independently screened all the remaining references for relevance against the full eligibility criteria using DistillerSR. We retrieved full‐text articles for all references for which a decision on eligibility could not be made from the title and abstract alone. We requested additional information from study authors as necessary to assess the eligibility for inclusion of individual studies. The two review authors discussed the results of study selection in order to resolve any discrepancies between themselves. In the event that this was not possible, we referred the decision on eligibility to a third review author (TW). We reported the results of study selection using a PRISMA flow diagram (Moher 2009) (Figure 1).
1.
Study flow diagram.
Data extraction and management
As recommended in the Cochrane Handbook for Systematic Reviews of Interventions, two review authors (DH, LE) independently extracted data onto standardised forms and performed a cross‐check using DistillerSR software (Higgins 2011a). The two review authors reached a consensus without the need for a third review author (TW). The review authors were not blinded to names of authors, institutions, journals or the study outcomes. We planned to extract the following information for each study.
Source: study ID; report ID; review author ID; date of extraction; ID of author checking extracted data; citation of paper; contact authors details.
General study information: publication type; study objectives; funding source; conflict of interest declared; other relevant study publication reviewed.
Study details and methods: location; country; setting; number of centres; total study duration; recruitment dates; length of follow‐up; power calculation; primary analysis (and definition); stopping rules; method of sequence generation; allocation concealment; blinding (of clinicians, participants and outcome assessors); and any concerns regarding bias.
Characteristics of interventions: number of study arms; description of experimental arm; description of control arm; type of plasma product (e.g. fresh frozen plasma (FFP), frozen plasma (F24) (including solvent detergent and methylene blue treated plasma); type of thromboplastin used to measure INR.
Characteristics of participants: age; gender; primary diagnosis; type of catheter inserted; platelet count.
Participant flow: total number screened for inclusion; total number recruited; total number excluded; total number allocated to each study arm; total number analysed (for review outcomes); number of allocated participants who received planned treatment; number of dropouts with reasons (percentage in each arm); protocol violations; missing data.
Outcomes: major procedure‐related bleeding within 24 hours of the procedure; minor procedure‐related bleeding within 24 hours of the procedure; transfusion‐related complications within 24 hours of the procedure; line‐related complications within seven days of the procedure; total number of days in hospital; proportion of participants receiving plasma transfusions within 24 hours; change in INR up to 24 hours post‐procedure; all‐cause mortality up to 30 days from the procedure; quality of life.
Assessment of risk of bias in included studies
We assessed the included RCT using the Cochrane 'Risk of bias' tool as described in Chapter eight of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011b). Two review authors (DH, LE) worked independently to assess each element of potential bias listed below as 'high', 'low' or 'unclear' risk of bias. We reported a brief description of the judgement statements upon which the authors have assessed potential bias in the Characteristics of included studies table. We reach a consensus on the degree of risk of bias through comparison of the review authors statements without the need for a third review author (TW). We used Cochrane's tool for assessing risk of bias, including the following domains.
Selection bias: random sequence generation and allocation concealment.
Performance bias: blinding of participants and personnel.
Detection bias: blinding of outcome assessment.
Attrition bias: incomplete outcome data.
Reporting bias: selective reporting.
Other bias.
Measures of treatment effect
For continuous outcomes, we planned to record the mean, standard deviation and total number of participants in both the treatment and control groups, however no continuous outcomes were reported in the included study. In future updates of this review, we will perform analyses for continuous outcomes that use the same scale, using the mean difference (MD) with 95% confidence intervals (CIs). For continuous outcomes measured with different scales, we will present the standardised mean difference (SMD).
We planned to extract and report hazard ratios (HR), if available for mortality data, however there were no deaths in the included study. In future updates of this review, we will extract and report HRs, if available for mortality data. If HRs are not available, we will make every effort to estimate as accurately as possible the HR using the available data and a purpose‐built method based on the Parmar and Tierney tool (Parmar 1998; Tierney 2007).
For dichotomous outcomes we recorded the number of events and the total number of participants in both the treatment and control groups. We did not report the pooled risk ratio (RR) with a 95% CI because there was only one included trial. Where the number of observed events was small (less than 5% of sample per group), and where trials have balanced treatment groups, we planned to report the Peto odds ratio (OR) with 95% CIs (Deeks 2011). However in the only analysis performed (minor bleeding), the observed event rate was more than 5%, therefore a Peto odds ratio was not performed.
Where the data allowed, we undertook quantitative assessments using Review Manager 5.
Where appropriate, we planned to report the number needed to treat for an additional beneficial outcome (NNTB) and the number needed to treat or an additional harmful outcome (NNTH) with CIs, however the only analysis performed did not demonstrate a benefit or harm.
If we could not report the available data in any of the formats described above, we performed a narrative report and, where appropriate, we planned to present the data in tables.
Unit of analysis issues
There were no unit of analysis issues within the included study. In future updates of this review, we will treat any unit of analysis issues in accordance with the advice given in Chapter 16 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011c). If participants are randomised more than once, we will contact the authors of the study to provide us with data on the CVCs associated with the initial randomisation.
Dealing with missing data
Where data were identified as missing or unclear in the published literature, we contacted the study authors directly. In the one included trial participants were undergoing other invasive procedures besides central venous catheterisation (Müller 2015), the author provided additional unpublished data for the central venous catheter subgroup from the general trial dataset.
Assessment of heterogeneity
We did not perform an assessment of heterogeneity as the review included only one completed study. We had specified in the protocol that we planned to combine data to perform a meta‐analysis if the clinical and methodological characteristics of individual studies were sufficiently homogeneous. We had intended to assess statistical heterogeneity of treatment effects between studies using a Chi2 test with a significance level at P value < 0.1. We planned to use the I2 statistic to quantify the degree of potential heterogeneity and classify it as moderate if the I2 value is over 50% or considerable if the I2 is over 80%. We had intended to explore potential sources of statistical heterogeneity in each included study and perform sensitivity analyses as appropriate.
We had anticipated that at least moderate clinical and methodological heterogeneity would be identified within the studies selected for inclusion and intended to use the random‐effects model. If statistical heterogeneity had been considerable, we did not intend to pool the studies in a meta‐analysis. We planned to assess potential causes of heterogeneity by sensitivity and subgroup analyses (Deeks 2011).
Assessment of reporting biases
We did not perform a formal assessment of potential publication bias as the review included only one trial.
In future updates of this review, where at least 10 studies are identified for inclusion in a meta‐analysis, we will explore potential publication bias (small‐trial bias) by generating a funnel plot and using a linear regression test. We will consider a P value of less than 0.1 as significant for this test (Lau 2006; Sterne 2011).
Data synthesis
We planned to perform analyses according to the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions using aggregated data for analysis (Deeks 2011). For statistical analysis, we entered data into the Cochrane statistical package Review Manager 5. One review author (DH) entered the data into the software and a second review author (LE) checked this for accuracy.
Meta‐analysis was not feasible as the review included only one completed study.
In future updates of this review where meta‐analysis is feasible, we will use the random‐effects model for pooling the data. We will use the Mantel‐Haenszel method for dichotomous outcomes or Peto method as necessary, and we will use the inverse variance method (and SMDs as necessary) for continuous outcomes. We will use the generic inverse variance method for time‐to‐event outcomes.
If heterogeneity is found to be above 80%, we will not perform a meta‐analysis.We will comment narratively on results and we will comment on any trends in the data within the results section of the review.
Summary of findings
We planned to use GRADE to build separate 'Summary of findings' tables for both types of FFP transfusion regimen specified in the Types of interventions, as suggested in Chapters 11 and 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Schünemann 2011a; Schünemann 2011b). The included study compared no plasma transfusion prior to central line insertion versus plasma transfusion prior to central line insertion when the INR is 1.5 to 3 times control. The outcomes we included are listed below.
Major procedure‐related bleeding within 24 hours of the procedure.
All‐cause mortality up to 30 days after the procedure.
Respiratory deterioration attributable to transfusion‐associated circulatory overload (TACO), transfusion‐related acute lung injury (TRALI) or transfusion‐associated dyspnoea (TAD) within 24 hours of the procedure.
Minor procedure‐related bleeding within 24 hours of the procedure.
Proportion of participants receiving plasma transfusions within 24 hours of the procedure.
Line‐related complications within seven days of the procedure (infection, thrombosis, other).
Quality of life.
Subgroup analysis and investigation of heterogeneity
We were unable to perform any subgroup analyses because of insufficient data. In future updates of this review we plan to carry out subgroup analyses for each of the following outcomes in order to assess the effect on heterogeneity.
Type of central line inserted (venous tunnelled, venous untunnelled, porta‐cath, whether an emergency or elective procedure).
Type of participants (intensive care, liver disease, other).
Age of participants (neonate, child (one to 15 years), adult (16 years or older)).
Whether participants had associated platelet count abnormalities.
In future updates of this review investigation of heterogeneity between studies will also include the following, if appropriate.
Type of plasma component (fresh frozen plasma (FFP), frozen plasma (F24) (including solvent detergent and methylene blue treated plasma).
Type of thromboplastin used to measure INR.
Sensitivity analysis
Only one completed study was identified in this review and therefore we performed no sensitivity analyses. In future updates of this review if sufficient data are available we plan to assess the robustness of our findings by performing the following sensitivity analyses where appropriate.
Including only those studies with a 'low' risk of bias for detection and selection bias.
Including only those studies with less than a 20% dropout rate.
Results
Description of studies
See Characteristics of included studies; Characteristics of excluded studies; Characteristics of ongoing studies
Results of the search
The search (conducted on 1 March 2016) identified 2771 potentially relevant records (see the PRISMA Flow Diagram, Figure 1). There were 2009 records after we removed duplicates. Two review authors (LE and DH) excluded 1976 records on the basis of the abstract. We retrieved 33 full‐text articles for assessment by the same two review authors. Four studies met the inclusion criteria for review (Müller 2015; NCT02311985; NCT02561026; NCT02637427), but three of these are ongoing (NCT02311985; NCT02561026; NCT02637427).
Included studies
See Characteristics of included studies for full details of the included study.
The one completed study (Müller 2015) included within this review compared no plasma transfusion prior to central line insertion versus plasma transfusion prior to central line insertion when the INR was 1.5 to 3 times control.
No studies were identified that compared: no plasma transfusion prior to central line insertion versus plasma transfusion when the INR was greater than 3 times control; OR plasma transfusion when rotational thromboelastography (TEG) was above a certain threshold (as defined by the study).
No studies were identified that compared: plasma transfusion prior to central line insertion when the INR was greater than 1.5 times control; versus plasma transfusion prior to central line insertion when the INR was 2 to 3 times control; OR plasma transfusion when the INR was greater than 3 times control; plasma transfusion when rotational TEG was above a certain threshold (as defined by the study).
Study Design
The TOPIC Trial (Müller 2015) was a parallel‐group, multi‐centre, randomised, open‐label trial with blinded endpoint evaluation. Participants were enrolled from May 2010 to June 2013.
Setting
The study was conducted in the Netherlands with participants recruited at two university hospitals and two large teaching hospitals.
Participants
The study investigators planned to recruit 200 participants per treatment arm, but owing to slow recruitment, the trial was stopped before this target enrolment was reached. Inclusion criteria included people over 18 years old admitted to the Intensive Care Unit (ICU) with an INR of 1.5 to 3.0 and undergoing insertion of a central venous catheter, thoracocentesis, percutaneous tracheotomy, or drainage of abscess or fluid collection. The investigators provided supplementary unpublished data relating to only those patients who underwent CVC insertion.
Intervention and Comparator
The study compared no fresh frozen plasma (FFP) versus a single dose of FFP (12 mL/kg) prior to an invasive procedure. Eighty‐one participants were randomised (41 no FFP, 40 FFP), of which 58 received CVC insertion and were included in this review (29 no FFP, 29 FFP).
Co‐Interventions
There were no co‐interventions in this study.
Outcomes
The primary outcome was procedure‐related bleeding occurring within a 24‐hour period after the procedure. Secondary outcomes included the effects of FFP on correction of INR and additional transfusion requirements, development of lung injury within 24 hours after the intervention, the incidence of ventilator‐associated pneumonia, major bleeding and minor bleeding. Quality of life outcomes were not reported
Funding Sources
The study was funded by ZonMw Netherlands, Organization for Health, Research and Development, the Hague, the Netherlands (Project 171002206).
Ongoing studies
There are three ongoing clinical trials (NCT02311985; NCT02561026; NCT02637427). Please see Characteristics of ongoing studies for further details.
Two ongoing studies are comparing no plasma transfusion prior to central line insertion versus plasma transfusion prior to central line insertion when the INR is 1.5 to 3 times control (NCT02561026; NCT02637427). The third ongoing study is a three‐arm study comparing plasma transfusion prior to central line insertion when the INR is greater than 1.5 times control versus plasma transfusion when the INR is greater than 5 times control versus plasma transfusion when rotational TEG is above a certain threshold (NCT02311985).
NCT02311985
The POCKET Trial (Point‐of‐care versus standard coagulation tests versus restrictive strategy to guide transfusion in chronic liver failure patients requiring central venous line, (NCT02311985) is a single‐centre, double‐blind, randomised‐controlled trial that is currently enrolling participants and aims to complete recruitment by December 2016 (personal communication with Dr Rocha). The study is being conducted in Brazil and plans to enrol 165 participants with chronic liver disease, randomised to receive transfusion of fresh‐frozen plasma, platelets and/or cryoprecipitate guided by the use of standard tests of coagulation (INR > 1.5, activated partial thromboplastin time (APPT) > 50 seconds) versus thromboelastometry (ROTEM) versus standard tests of coagulation with a restrictive threshold (INR > 5, platelets < 25 x 109/L) prior to central venous catheterisation.
NCT02561026
The TOPPIT Trial (Transfusion of Plasma Prior to Invasive Procedures Pilot Trial, NCT02561026) is a three‐centre, randomised, parallel‐assignment, open‐label trial that began to enrol participants in January 2016. It plans to enrol 80 people in intensive care over the age of 18 with an INR 1.5 to 2.5 who are undergoing an invasive procedure (central venous catheterisation, thoracocentesis, bronchoscopy, endoscopy, biopsy or fluid drainage). Participants will be randomised to receive either transfusion of FFP or no transfusion prior to the procedure.
NCT02637427
Does Plasma Reduce Bleeding in Patients Undergoing Invasive Procedures (NCT02637427) is a multi‐centre, single‐blinded, parallel‐assignment randomised controlled trial that aims to recruit 110 participants with an INR 1.5 to 2.5 undergoing an invasive procedure at the bedside, in an endoscopy suite or in a radiology department between January 2016 and May 2017. Participants will be randomised to receive either 10 to 20 mL/kg FFP versus no FFP prior to the invasive procedure.
Excluded studies
See Characteristics of excluded studies for full details of excluded studies. A total of 23 full‐text articles were excluded, of which:
nine were trials with non‐eligible comparison groups (Alport 2012; Bartelmaos 2013; Corash 2006; Etemadrezaie 2007; Freeman 1998; Holcomb 2015; Mintz 2006; Tinmouth 2008; Williamson 1999)
five were non‐randomised trials (Amarapurkar 2014; Carino 2009; Friedman 1989; Napolitano 2012; Weigand 2009)
three were trials which were withdrawn prior to enrolment (NCT00233246; NCT00953901; NCT01754545)
one trial included fewer than 10% of participants receiving central venous catheterisation (De Pietri 2016)
one article was a case series (Gallieni 1995)
one article was a commentary (Harter 2004)
three articles were secondary citations of excluded studies
Risk of bias in included studies
See Figure 2 for a visual representation of the risk of bias in the included study. See the 'Risk of bias' table within the Characteristics of included studies for further information regarding the risk of bias identified within this trial.
2.
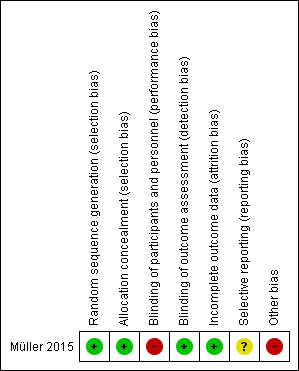
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Allocation
We assessed the risk of bias due to selection bias (sequence generation and allocation concealment) as low. The randomisation procedure was web‐based and password‐protected, using permuted blocks and stratified by study centre and invasive procedure.
Blinding
Performance bias
We assessed the risk of bias due to performance bias as high. Manufacture of a completely matched placebo was not considered possible and so investigators and clinicians were unblinded to the intervention. Due to this lack of blinding the compared groups may have received different amounts of attention, ancillary treatment, and diagnostic investigations by clinicians. It is unclear how many participants were sedated and therefore not aware of the intervention.
Detection bias
We assessed the risk of bias due to detection bias as low. Assessment of potential bleeding was by a physician blinded to the intervention who assigned a score of major, minor or no bleeding at one and 24 hours after the intervention.
Incomplete outcome data
We assessed the risk of bias due to attrition bias as low. All participants who were randomised and underwent an invasive procedure were included in the analysis
Selective reporting
We assessed the risk of bias due to reporting bias as unclear. The primary outcome was pre‐specified and reported ("procedure related relevant bleeding, occurring within 24 hours after the procedure") . However, changes were made to secondary outcomes between trial registration and reporting. Acute lung injury was reported at 24 hours, rather than 48 hours as specified in the trial registration. No evaluation of costs was reported, despite this being registered as a secondary outcome.
Other potential sources of bias
We assessed the risk of bias due to other bias as high. The major limitation of this trial was that it was stopped early due to slow inclusion. Despite the addition of extra recruitment sites, the study was only able to randomise 20% of the targeted participant number. There was also an imbalance in the number of participants with a history of liver disease between treatment arms. 45% (17/38) of participants had liver disease in the no FFP arm whereas only 16% (6/38) had liver disease in the FFP arm. People with liver disease are known to have re‐balanced haemostasis with a decrease in both pro‐coagulant and anticoagulant clotting factors (Habib 2014; Kujovich 2015), therefore people with liver disease may be less likely to bleed than other people with abnormal coagulation (measured using INR).
Effects of interventions
See: Table 1
Primary outcomes
Major procedure‐related bleeding within 24 hours of the procedure
There were no episodes of major procedure‐related bleeding reported in either of the two arms of the Müller 2015 study (58 participants, unpublished data provided by the study authors). There was therefore insufficient evidence to determine a difference in major procedure‐related bleeding between participants who received no FFP prior to CVC insertion compared to those transfused FFP (very low‐quality of evidence).
All‐cause mortality up to 30 days after the procedure
This was not reported for the 58 participants who underwent a CVC insertion.
For the 76 participants in the study who underwent any procedure there were 19 deaths in the FFP arm (38 participants) and 27 deaths in the no FFP arm (38 participants) (Müller 2015). Additional linear regression performed by the study authors demonstrated that liver disease was the sole predictor for mortality (P = 0.056).
Secondary outcomes
Minor procedure‐related bleeding within 24 hours of the procedure
This was defined as prolonged bleeding at the insertion site, which only required treatment with a pressure bandage/haematoma at the insertion site, or minor bleeding as reported by individual studies. In the only included study (58 participants, unpublished data provided by the study authors), there were two episodes of minor procedure‐related bleeding within 24 hours of central venous catheterisation in the FFP arm, compared to three episodes in the no FFP arm (risk ratio (RR) 0.67; 95% confidence interval (CI) 0.12 to 3.70, very low‐quality of evidence) (Analysis 1.1).
1.1. Analysis.
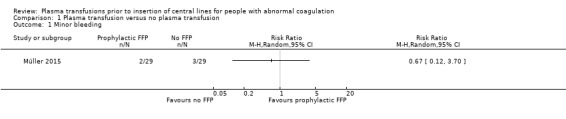
Comparison 1 Plasma transfusion versus no plasma transfusion, Outcome 1 Minor bleeding.
Serious adverse events
Transfusion‐related complications within 24 hours of the procedure
These complications included: transfusion‐related acute lung injury (TRALI); transfusion‐transmitted infection; transfusion‐associated circulatory overload (TACO); transfusion‐associated dyspnoea (TAD); and acute transfusion reactions.
These outcomes were not reported by the included study.
Line‐related complications within seven days of the procedure (infection, thrombosis, other)
These outcomes were not reported by the included study.
Total number of days in hospital
This outcome was not reported by the included study.
Proportion of participants receiving plasma transfusions and red cell transfusions within 24 hours of the procedure
This outcome was not reported by the included study.
Change in INR up to 24 hours following the procedure
This outcome was not reported for the subgroup of 58 participants who underwent a CVC insertion in the included study.
For the 76 participants who underwent any procedure, 38 were randomised to receive an FFP transfusion. An FFP transfusion resulted in a median reduction of INR from 1.8 (interquartile range (IQR) 1.5 to 2.5) to 1.4 (IQR, 1.3 to 1.63; P < 0.001) (study author's own results). Only 54% of participants had an INR less than 1.5 after an FFP transfusion (Müller 2015).
Quality of life
The included study did not report any quality of life outcome measures.
Discussion
Summary of main results
Four randomised controlled trials (RCTs) met the inclusion criteria, of which three are currently ongoing (NCT02311985, NCT02637427, NCT02561026) and one has been completed (Müller 2015). The completed study randomised a total of 81 adults in intensive care with coagulopathy (INR 1.5 or greater) who were due to undergo an invasive procedure to receive either prophylactic fresh frozen plasma (FFP) at 12 mL/kg or to receive no FFP; of these participants, 58 underwent central venous catheterisation (the remainder underwent other invasive procedures such as chest drain insertion). It is the subgroup of 58 patients undergoing central venous catheter (CVC) insertion that were included in this review.
In the Müller 2015 trial there were no reported episodes of major bleeding within 24 hours of the procedure, there was therefore insufficient evidence to determine a difference in this primary outcome.
There was insufficient evidence to determine the risk of minor procedure‐related bleeding (risk ratio (RR) 0.67; 95% confidence interval (CI) 0.12 to 3.70). No serious adverse events were reported by this study.
The proportion of participants who died due to any cause, as well as the change in INR in the 24 hours following the procedure, were not made available for the subgroup of 58 patients in the Müller 2015 trial who underwent central venous catheterisation.
Outcomes relating to the proportion of recipients receiving plasma or red cell transfusions within 24 hours of the procedure; serious adverse events (transfusion‐related within 24 hours of the procedure and line‐related within seven days of the procedure); total number of days in hospital and quality of life were not reported by the included study.
Overall completeness and applicability of evidence
The conclusions which can be drawn following this systematic review are very limited due to the inclusion of only one RCT (Müller 2015), from which only 58 patients were included in this review. There was insufficient evidence to determine the effect of plasma transfusion prior to central line insertion on the primary outcomes of all‐cause mortality or major procedure‐related bleeding. There were insufficient data to determine the effect on minor procedure‐related bleeding or any other secondary outcome. There are three ongoing RCTs (NCT02311985, NCT02561026, NCT02637427), which are scheduled to complete recruitment by February 2018.
These three ongoing studies (expected recruitment 355 participants in total) will be too small to provide sufficient data for this review’s primary outcomes. For example, if we assumed that major bleeding occurred in 1 out of 100 people who had a central line when their INR was 1.5 or less, and that the risk of major bleeding doubled to 2 out of 100 people when their INR was only 5 or less, we would need to design a study with at least 4634 participants to detect this difference with 80% power and 5% significance (6202 participants required to detect a difference with 90% power) (calculated using a power calculator at www.sealedenvelope.com/power/binary‐superiority/).
Quality of the evidence
The Müller 2015 study was stopped early as it failed to recruit sufficient participants, as such it was underpowered; investigators were only able to randomise 20% of the targeted number of participants, leading to a high risk of Type II error. There was low risk of selection or attrition bias. Clinicians and participants were unblinded to the intervention, leading to a high risk of performance bias. Although the primary outcome was pre‐specified and reported, minor changes were made to secondary outcomes between trial registration and reporting, increasing the risk of reporting bias. There was an imbalance in the number of participants who had liver disease between the two study arms, increasing the risk of other bias.
Overall, the quality of evidence was rated according to the GRADE methodology as very low across difference outcomes due to the high risk of bias in the included study and the imprecision of the estimates.
We assessed the GRADE quality of evidence as very low for:
major procedure‐related bleeding within 24 hours of the procedure.
minor procedure‐related bleeding within 24 hours of the procedure.
We could not assess the quality of the evidence for: all‐cause mortality; respiratory deterioration attributable to transfusion‐associated circulatory overload (TACO), transfusion‐related acute lung injury (TRALI) or transfusion‐associated dyspnoea (TAD); acute transfusion reactions) within 24 hours of the procedure; proportion of participants receiving plasma transfusions within 24 hours of the procedure; line‐related complications within seven days of the procedure (infection, thrombosis, other); or quality of life because these outcomes were not reported.
Potential biases in the review process
We conducted a comprehensive search of multiple databases and clinical trial registries to capture all relevant RCTs. We only included one study reported in English, however no relevant non‐English language studies were identified in the search. There are three ongoing studies. Two assessors carefully screened all papers identified by the search and performed data extraction. We pre‐specified all outcomes prior to undertaking the search. We were unable to undertake a meta‐analysis or assess publication bias as only one study was included in this review.
Agreements and disagreements with other studies or reviews
We are not aware of any other systematic reviews of RCTs which assess the effect of plasma transfusion prior to central line insertion for people with abnormal coagulation.
Authors' conclusions
Implications for practice.
The conclusion of this systematic review is that currently there exists only very limited evidence from one randomised controlled trial (RCT) to inform the decision whether or not to administer prophylactic plasma prior to central venous catheterisation for people with abnormal coagulation. It is not possible from the current RCT evidence to recommend whether or not prophylactic plasma transfusion is beneficial or harmful in this situation.
Implications for research.
It is common for people who are critically ill to become coagulopathic, and many of these will require insertion of a central venous catheter (CVC). The question of whether prophylactic plasma transfusion is indicated remains unanswered. An adequately‐powered trial which is able to recruit sufficient number of participants to address this is required. The ongoing trials that are due to be completed by February 2018 will be unable to answer the primary questions of this review because the studies are too small. To detect a doubling in the number of participants with major bleeding from 1% to 2% would require a two‐arm study with over 4600 participants; the three ongoing studies are only planning to recruit 355 participants in total.
Notes
This review is a rapid review (definition of a rapid review as previously agreed with the Cochrane Haematological Malignancies Group), and includes only English language publications.
Acknowledgements
We thank the editorial base of the Cochrane Haematological Malignancies Review Group.
We thank the National Institute of Health Research (NIHR). This review is part of a series of reviews that have been funded by NIHR Cochrane Programme Grant ‐ Safe and Appropriate Use of Blood Components. This research was also supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre Programme. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Appendices
Appendix 1. CENTRAL search strategy
#1 MeSH descriptor: [Catheterization, Central Venous] this term only #2 MeSH descriptor: [Catheters, Indwelling] this term only #3 MeSH descriptor: [Central Venous Catheters] this term only #4 MeSH descriptor: [Vascular Access Devices] this term only #5 hickman* or "port catheter*" or port‐a‐cath* or "invasive line*" or portacath* or TIVAD* #6 ((central* or venous* or vascular* or intravenous* or tunnel* or indwelling or "in‐dwelling" or implant* or placement* or subclavian or femoral or jugular) near/5 (catheter* or line* or cannul* or port*)) #7 ((vascular or venous) near/2 (access* or reservoir*)) #8 #1 or #2 or #3 or #4 or #5 or #6 or #7 #9 MeSH descriptor: [Plasma] explode all trees #10 MeSH descriptor: [Blood Component Transfusion] this term only #11 plasma #12 #10 and #11 #13 (plasma near/5 (transfus* or prophyla* or fresh* or frozen or freez* or prefrozen or prefreez* or thaw* or prethaw* or infus* or treatment* or therap* or administ* or donor* or donat* or autologous or allogen* or allo‐gen* or homolog*)) #14 (FFP or SDFFP or MBFFP or uniplas* or octaplas* or FP24 or frischplasma or "clinical plasma") #15 (plasma near/3 ("pathogen inactivated" or "pathogen reduced" or universal or donor*)) #16 ((pasteurized or pasteurised or methylene or solvent or detergent or cryoprecipitate or supernatant or cryosupernatant or thawed) near/5 plasma) #17 #9 or #12 or #13 or #14 or #15 or #16 #18 MeSH descriptor: [Blood Coagulation Disorders] explode all trees #19 ((coagulation* or clotting or bleeding) near/5 (disorder* or abnormal* or anomaly or disturb* or defect* or disseminated intravascular)) #20 ((abnormal* or elevated or prolonged) near/3 (international normalised ratio or international normalized ratio or INR)) #21 coagulopath* #22 #18 or #19 or #20 or #21 #23 #8 and #22 #24 (#8 or #22) and #17 #25 #23 or #24
Appendix 2. PubMed (for epublications) search strategy
#1 hickman* OR port catheter* OR port‐a‐cath* OR invasive line" OR portacath* OR TIVAD* #2 ((central* OR venous* OR vascular* OR intravenous* OR tunnel* OR indwelling OR "in‐dwelling" OR implant* OR placement* OR subclavian OR femoral OR jugular) AND (catheter* OR line* OR cannul* OR port*)) #3 ((vascular OR venous) AND (access* OR reservoir*)) #4 #1 OR #2 OR #3 #5 (plasma AND (transfus* OR prophyla* OR fresh* OR frozen OR freez* OR prefrozen OR prefreez* OR thaw* OR prethaw* OR infus* OR treatment* OR therapy OR administ* OR donor* OR donat* OR autologous OR allogen* OR allo‐gen* OR homolog*)) #6 (FFP OR SDFFP OR MBFFP OR uniplas* OR octaplas* OR FP24 OR frischplasma OR clinical plasma) #7 (plasma AND (pathogen inactivated OR pathogen reduced OR universal OR donor*)) #8 ((pasteurized OR pasteurised OR methylene OR solvent OR detergent OR cryoprecipitate OR supernatant OR cryosupernatant OR thawed) AND plasma) #9 #5 OR #6 OR #7 OR #8 #10 ((coagulation* OR clotting OR bleeding) AND (disorder* OR abnormal* OR anomaly OR disturb* OR defect* OR disseminated intravascular)) #11 ((abnormal* OR elevated OR prolonged) AND (international normalised ratio OR international normalized ratio OR INR)) #12 coagulopath* #13 #10 OR #11 OR #12 #14 #4 AND #13 #15 (#4 OR #13) AND #9 #16 #14 OR #15 #17 (random* OR blind* OR control group OR placebo OR controlled trial OR controlled study OR groups OR trials OR systematic review OR meta‐analysis OR metaanalysis OR literature search OR medline OR cochrane OR embase) AND (publisher[sb] OR inprocess[sb] OR pubmednotmedline[sb]) #18 #16 AND #17
Appendix 3. MEDLINE (OvidSP) search strategy
1. Catheterization, Central Venous/ 2. Catheters, Indwelling/ 3. Central Venous Catheters/ 4. Vascular Access Devices/ 5. (hickman* or port‐a‐cath* or port catheter* or port‐a‐cath* or invasive line* or portacath* or TIVAD*).tw. 6. ((central* or venous* or vascular* or intravenous* or tunnel* or indwelling or "in‐dwelling" or implant* or placement* or subclavian or femoral or jugular) adj5 (catheter* or line* or cannul* or port*)).tw. 7. ((vascular or venous) adj2 (access* or reservoir*)).tw. 8. or/1‐7 9. Plasma/ 10. Blood Component Transfusion/ and plasma.tw. 11. (plasma adj5 (transfus* or prophyla* or fresh* or frozen or freez* or prefrozen or prefreez* or thaw* or prethaw* or infus* or treatment* or therap* or administ* or donor* or donat* or allogen* or allo‐gen*)).tw. 12. (FFP or SDFFP or MBFFP or uniplas* or octaplas* or FP24 or frischplasma or clinical plasma).tw. 13. (plasma adj3 (pathogen inactivated or pathogen reduced or universal or donor*)).tw. 14. ((pasteurized or pasteurised or methylene or solvent or detergent or cryoprecipitate or supernatant or cryosupernatant or thawed) adj5 plasma).tw. 15. or/9‐14 16. exp Blood Coagulation Disorders/ 17. ((coagulation* or clotting or bleeding) adj5 (disorder* or abnormal* or anomaly or disturb* or defect* or disseminated intravascular)).tw. 18. ((abnormal* or elevated or prolonged) adj3 (international normali?ed ratio or INR)).tw. 19. coagulopath*.tw. 20. or/16‐19 21. 8 and 20 22. (8 or 20) and 15 23. 21 or 22 24. randomized controlled trial.pt. 25. controlled clinical trial.pt. 26. randomi*.tw. 27. placebo.ab. 28. clinical trials as topic.sh. 29. randomly.ab. 30. groups.ab. 31. trial.ti. 32. or/24‐31 33. 23 and 32
Appendix 4. Embase (OvidSP) search strategy
1. exp Central Venous Catheterization/ 2. exp Indwelling Catheter/ 3. exp Central Venous Catheter/ 4. (hickman* or port catheter* or port‐a‐cath* or invasive line* or portacath* or TIVAD*).tw. 5. ((central* or venous* or vascular* or intravenous* or tunnel* or indwelling or "in‐dwelling" or implant* or placement* or subclavian or femoral or jugular) adj5 (catheter* or line* or cannul* or port*)).tw. 6. ((vascular or venous) adj2 (access* or reservoir*)).tw. 7. or/1‐6 8. Fresh Frozen Plasma/ 9. Plasma Transfusion/ 10. (plasma adj5 (transfus* or prophyla* or fresh* or frozen or freez* or prefrozen or prefreez* or thaw* or prethaw* or infus* or treatment* or therap* or administ* or donor* or donat* or autologous or allogen or allo‐gen* or homolog*)).tw. 11. (FFP or SDFFP or MBFFP or uniplas* or octaplas* or FP24 or frischplasma or clinical plasma).tw. 12. (plasma adj3 (pathogen inactivated or pathogen reduced or universal)).tw. 13. ((pasteurized or pasteurised or methylene or solvent or detergent or cryoprecipitate or supernatant or cryosupernatant or thawed) adj5 plasma).tw. 14. or/8‐13 15. Blood Clotting Disorder/ or Bleeding Disorder/ or Bleeding Tendency/ or Disseminated Intravascular Clotting/ or Hypocoagulability/ 16. ((coagulation* or clotting or bleeding) adj5 (disorder* or abnormal* or anomaly or disturb* or defect* or disseminated intravascular)).tw. 17. ((abnormal* or elevated or prolonged) adj3 (international normali?ed ratio or INR)).tw. 18. coagulopath*.tw. 19. or/15‐18 20. 7 and 19 21. (7 or 19) and 14 22. 20 or 21 23. Randomized Controlled Trial/ 24. Randomization 25. Single Blind Procedure/ 26. Double Blind Procedure/ 27. Crossover Procedure/ 28. Placebo/ 29. exp Clinical Trial/ 30. Prospective Study/ 31. (randomi* or double‐blind* or single‐blind* or RCT*).tw. 32. (random* adj2 (allocat* or assign* or divid* or receiv*)).tw. 33. (crossover* or cross over* or cross‐over* or placebo*).tw. 34. ((treble or triple) adj blind*).tw. 35. or/23‐34 36. Case Study/ 37. case report*.tw. 38. (note or editorial).pt. 39. or/36‐38 40. 35 not 39 41. 22 and 40 42. limit 41 to embase
Appendix 5. Transfusion Evidence Library search strategy
Subject area: FFP OR (Title: hickman OR catheter OR line OR port‐a‐cath OR portacath OR cannula OR port OR ports) AND (Keywords: FFP OR plasma)
Appendix 6. WHO International Clinical Trials Registry Platform (ICTRP) search strategy
(Title: hickman OR catheter OR line OR port‐a‐cath OR portacath OR cannula OR port OR ports) AND (Intervention: FFP OR plasma) OR (Condition: coagulation OR clotting OR coagulopathy OR coagulopathies OR coagulopathic OR bleeding OR hemorrhagic) AND (Intervention: FFP OR plasma)
Appendix 7. ClinicalTrials.gov search strategy
(Search Terms: hickman OR catheter OR line OR port‐a‐cath OR portacath OR cannula OR port OR ports) AND (Intervention: FFP OR plasma transfusion OR fresh plasma OR frozen plasma OR uniplas OR octaplas OR universal plasma) OR (Search Terms: coagulation OR clotting OR coagulopathy OR coagulopathies OR coagulopathic OR bleeding OR hemorrhagic) AND (Intervention: FFP OR plasma transfusion OR fresh plasma OR frozen plasma OR uniplas OR octaplas OR universal plasma)
Data and analyses
Comparison 1. Plasma transfusion versus no plasma transfusion.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Minor bleeding | 1 | Risk Ratio (M‐H, Random, 95% CI) | Totals not selected |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Müller 2015.
| Methods | National, multi‐centre, randomised, open‐label trial with blinded endpoint evaluation. Enrolled May 2010 to June 2013. |
|
| Participants |
Inclusion criteria: Adults in intensive‐care (aged 18 years and older) with an INR greater than or equal to 1.5 undergoing insertion of a central venous catheter, thoracocentesis, percutaneous tracheotomy, or drainage of abscess or fluid collection (n = 81) Exclusion criteria: People with clinically overt bleeding (defined as either a decrease in haemoglobin [Hb] > 16 g/L or a need for transfusion or haemodynamic instability due to bleeding at the time of the procedure); thrombocytopenia of less than 30 × 109/L; patients treated with vitamin K antagonists, activated protein C, abciximab, tirofiban, ticlopidine, or prothrombin complex concentrates; patients with a history of congenital or acquired coagulation factor deficiency or bleeding diathesis; use of heparin < 1 hour before the procedure; use of therapeutic doses of low molecular weight heparin < 12 hours before the procedure Number screened: A total of 1478 patients had an INR of at least 1.5 and not more than 3.0. Of these, 615 patients did not fulfil inclusion criteria, leaving 263 patients with an INR of at least 1.5 and not more than 3.0 scheduled to undergo a pre‐defined intervention. Of these, 65 patients declined informed consent. An additional 83 patients were missed and 34 patients did not participate due to other reasons, including refusal from treating physicians to include a specific patient (3.8%). Number recruited: 81 participants. Five did not undergo an intervention and were therefore excluded from further analysis (2 FFP; 3 no FFP). Age: FFP: median 64 years (IQR 54 to 70): no FFP: median 66 years (IQR 62 to 72) Gender: Male 44 (FFP 26; no FFP 18); Female 32 (FFP 12; no FFP 20) Platelet count: FFP: median 92 x 109/L (IQR 52 to 180), no FFP: median 110 x 109/L (IQR 52 to 183) Number analysed for primary outcome: 76 participants (38 FFP and 38 no FFP) |
|
| Interventions | Participants assigned to receive or not to receive a single dose of 12 mL/kg FFP Arm 1: assigned to FFP (n = 40); underwent a CVC insertion (n = 29) Arm 2: assigned to no FFP (n = 41); underwent a CVC insertion (n = 29) |
|
| Outcomes |
Primary outcome: Procedure‐related bleeding, occurring within 24 hours after the procedure Secondary outcomes: Effects of FFP on correction of INR and additional transfusion requirements; development of lung injury 24 hours after intervention; incidence of ventilator‐associated pneumonia (VAP) |
|
| Assessment of bleeding |
Major bleeding: defined as bleeding accompanied by a decrease in Hb by more than 20 g/L in the absence of another cause of bleeding; transfusion of 2 or more units RBCs without an increase in Hb; a decrease in systolic blood pressure by more than 20 mmHg; an increase in heart rate by 20 beats per minute or more; wound‐related bleeding requiring an intervention. Minor bleeding: defined as prolonged bleeding at the site of insertion or increase in size of subcutaneous haematoma |
|
| Notes |
Trial registration: NCT01143909 and NTR 2262 (registered 26 March 2010) Sponsor: Academisch Medisch Centrum ‐ Universiteit van Amsterdam (AMC‐UvA) Location of trial: Netherlands Number of study centres: 4 Sample size calculation: was based on the assumption that the occurrence of major bleeding in patients with a coagulopathy undergoing invasive procedures was less than 1%. Group size calculation was focused on demonstrating noninferiority.With a sample size in each group of 198, a one‐sided Z test with continuity correction (pooled) achieved 80% power to reject the null hypothesis that the proportion of bleeding patients in the experimental group (no FFP transfusion) was higher, that is, inferior to the proportion in the control group (FFP transfusion) with a margin of 0.03. It was assumed that the expected difference in proportions is zero and the proportion in the control group is 0.01. The one‐sided significance level of the test was targeted at 0.05. Therefore, the authors intended to enrol 200 patients per treatment arm. Owing to slow inclusion, the trial was stopped before the pre‐defined target enrolment was reached. Conflict of interests: NPJ reported grants from the Netherlands Organisation for Scientific Research (NWO), during the conduct of the study. The other authors disclosed no conflicts of interest |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The randomization procedure is password protected, web‐based, using permuted blocks and stratified by study centre and invasive procedure" |
| Allocation concealment (selection bias) | Low risk | "The randomization procedure is password protected, web‐based, using permuted blocks and stratified by study centre and invasive procedure" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Investigators and clinicians were unblinded to the intervention. It is unclear how many participants were sedated and not aware of the intervention. "Since manufacturing a completely matched placebo in full compliance with the current good manufacturing practice standards was considered not possible, a prospective, randomized, open‐label, blinded endpoint evaluation (PROBE) design was chosen." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "The potential bleeding site was assessed by a physician blinded to the intervention who filled out a predefined bleeding score form consisting of blood pressure, heart rate, Hb level, and occurrence of procedure‐related bleeding with or without the need for intervention or transfusion. Subsequently this blinded physician assigned a score of major bleeding, minor bleeding, or no bleeding at 1 and 24 hours after the intervention." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants who were randomised and underwent an invasive procedure were included in the analysis |
| Selective reporting (reporting bias) | Unclear risk | The primary outcome was pre‐specified and reported ("procedure related relevant bleeding, occurring within 24 hours after the procedure") Minor changes were made to secondary outcomes between trial registration and reporting. Acute lung injury was reported at 24 hours, rather than 48 hours as specified in the trial registration. No evaluation of costs was reported, despite this being registered as a secondary outcome. |
| Other bias | High risk | The major limitation of this trial was that it was stopped early due to slow inclusion. Despite the addition of extra recruitment sites, the study was only able to randomise 20% of the targeted participant number. There was an imbalance in the number of participants with a history of liver disease between treatment arms. 45% (17/38) of participants had liver disease in the no FFP arm whereas only 16% (6/38) had liver disease in the FFP arm. |
CVC: central venous catheter; FFP: fresh frozen plasma; INR: International Normalised Ratio; IQR: interquartile range; RBC: red blood cell
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Alport 2012 | Comparison of different peripherally‐ inserted central venous catheters in non‐coagulopathic patients |
| Amarapurkar 2014 | Non‐randomised observational study |
| Bartelmaos 2013 | Comparison of quarantine, methylene blue and solvent/detergent plasmas in liver transplant recipients |
| Carino 2009 | Non‐randomised observational study |
| Corash 2006 | Comparison of standard FFP and photochemically‐treated FFP in coagulopathic patients prior to invasive procedures |
| De Pietri 2016 | Comparison of FFP transfusion guided by thromboelastography versus standard coagulation tests prior to invasive procedures. Fewer than 10% of included participants received central venous catheterisation. |
| Etemadrezaie 2007 | Comparison of FFP and saline in severe traumatic brain injury |
| Freeman 1998 | Comparison of solvent/detergent FFP and standard FFP in orthotopic liver transplantation |
| Friedman 1989 | Non‐randomised, observational study |
| Gallieni 1995 | Case‐series |
| Harter 2004 | Commentary |
| Holcomb 2015 | Comparison of plasma:platelet: red blood cell ratios in severe trauma with massive haemorrhage |
| Mintz 2006 | Comparison of photochemically‐treated and standard FFP in patients with coagulopathy of liver disease |
| Napolitano 2012 | Non‐randomised, observational study |
| NCT00233246 | Study withdrawn prior to enrolment |
| NCT00953901 | Study withdrawn prior to enrolment |
| NCT01754545 | Study withdrawn prior to enrolment; wrong subject group |
| Tinmouth 2008 | Comparison of high and standard dose FFP in coagulopathic patients undergoing invasive procedures |
| Weigand 2009 | Non‐randomised, observational study |
| Williamson 1999 | Comparison of solvent/detergent and standard FFP |
FFP: fresh frozen plasma
Characteristics of ongoing studies [ordered by study ID]
NCT02311985.
| Trial name or title | Point‐of‐care versus standard coagulation tests versus restrictive strategy to guide transfusion in chronic liver failure patients requiring central venous line: prospective randomised trial |
| Methods | Single centre. Double‐blind, randomised‐controlled trial. |
| Participants |
Inclusion Criteria: Adults (18 years or older) with chronic liver disease requiring central venous catheterisation Exclusion Criteria:
|
| Interventions | Transfusion of fresh‐frozen plasma, platelets and/or cryoprecipitate following the use of standard tests of coagulation (INR > 1.5, APPT > 50s) versus thromboelastometry (ROTEM) versus standard tests of coagulation with a restrictive threshold (INR > 5, platelets < 25 x 109/L) |
| Outcomes |
Primary outcome: proportion of participants receiving FFP, platelets and/or cryoprecipitate prior to central venous catheterisation Secondary outcomes: incidence of bleeding; adverse consequences of blood product transfusion; cost; duration of ICU stay; duration of hospital stay; 28‐day mortality |
| Starting date | September 2014 Estimated Study Completion Date: December 2016 |
| Contact information | Dr Leonardo Rocha ‐ lrocha23@gmail.com |
| Notes |
Trial registration: NCT02311985 on 3 December 2014 Planned recruitment: 165 adults Sponsor: Hospital Israelita Albert Einstein Location of trial: Brazil Number of study centres: 1 |
NCT02561026.
| Trial name or title | Transfusion of Plasma Prior to Invasive Procedures Pilot Trial (TOPPIT) |
| Methods | Three‐centre, randomised, parallel‐assignment open‐label trial |
| Participants |
Inclusion Criteria:
Exclusion Criteria:
Patients will not be excluded for thrombocytopenia or antiplatelet drugs. As a pilot trial for a pragmatic large randomised controlled trial, both thrombocytopenic patients and patients on antiplatelet agents will be enrolled as they are routinely encountered in clinical practice. |
| Interventions | Transfusion of fresh‐frozen plasma versus no transfusion prior to invasive procedure |
| Outcomes |
Primary outcome: recruitment feasibility Secondary outcomes: bleeding assessment; ventilator requirement; overall hospital length of stay; ICU length of stay |
| Starting date | January 2016 Estimated Study Completion Date: February 2018 |
| Contact information | Elizabeth Chatelain ‐ echatelain@ohri.ca |
| Notes |
Trial registration: NCT02561026 on 15 July 2015 Planned recruitment: 80 adults Sponsor: Ottawa Hospital Research Institute Location of trial: Canada Number of study centres: 3 |
NCT02637427.
| Trial name or title | Does Plasma Reduce Bleeding in Patients Undergoing Invasive Procedures? |
| Methods | Multi‐centre, single‐blind, parallel assignment randomised controlled trial |
| Participants |
Inclusion Criteria: Adults (aged 21 years or older) with an INR between 1.5 and 2.5 undergoing an invasive procedure at the bedside, in an endoscopy suite or in a radiology department Exclusion Criteria:
|
| Interventions | Transfusion of fresh frozen plasma (10 mL to 20mL/kg to a maximum of 5 units) versus no transfusion prior to an invasive procedure |
| Outcomes |
Primary outcomes: change in haemoglobin level; trial feasibility Secondary outcomes: rate of red cell transfusion; transfusion‐associated circulatory overload; transfusion‐associated acute lung injury; major bleeding; change in INR post‐procedure, at day one and day two; mortality; infection; ICU admission |
| Starting date | January 2016 Estimated Study Completion Date: May 2017 |
| Contact information | Dr Paul Ness ‐ pness@jhmi.edu |
| Notes |
Trial registration: NCT02637427 on 16 December 2015 Planned recruitment: 110 adults Sponsor: National Heart, Lung, and Blood Institute (NHLBI) Location of trial: United States Number of study centres: 4 |
APTT: activated partial thromboplastin time; ICU: intensive care unit; INR: International Normalised Ratio
Differences between protocol and review
Aspects of the protocol that were not implemented due to lack of data
There were several differences between the protocol (Hall 2015) and this review due to lack of data.
Interventions
We could not perform five of the six planned comparisons, because the one included study did not compare these interventions.
No studies were identified that compared: no plasma transfusion prior to central line insertion versus plasma transfusion when the INR is greater than 3 times control; OR plasma transfusion when rotational thromboelastography is above a certain threshold (as defined by the study).
No studies were identified that compared: plasma transfusion prior to central line insertion when the INR is greater than 1.5 times control; versus plasma transfusion prior to central line insertion when the INR is 2 to 3 times control; OR plasma transfusion when the INR is greater than 3 times control;plasma transfusion when rotational thromboelastography is above a certain threshold (as defined by the study).
Primary outcomes
The included study did not report the following review outcomes.
All‐cause mortality up to 30 days after the procedure.
Secondary outcomes
The included study did not report the following review outcomes.
Serious adverse events:
transfusion‐related complications within 24 hours of the procedure (including transfusion‐related acute lung injury (TRALI), transfusion‐transmitted infection, transfusion‐associated circulatory overload (TACO), transfusion‐associated dyspnoea (TAD), acute transfusion reactions);
line‐related complications within seven days of the procedure (infection, thrombosis, other).
Total number of days in hospital.
Proportion of participants receiving plasma transfusions and red cell transfusions within 24 hours of the procedure.
Change in INR up to 24 hours following the procedure.
Quality of life, as defined by the individual studies.
Measures of treatment effect
The included study did not report any continuous outcomes or hazard ratios.
We did not report the number needed to treat for an additional beneficial outcome (NNTB) and the number needed to treat for an additional harmful outcome (NNTH) with confidence interval (CIs), because the only analysis performed did not demonstrate a benefit or harm.
Data extraction and management
We could not pilot the data extraction form on two included RCTs because there was only one included RCT.
Assessment of heterogeneity
We did not perform an assessment of heterogeneity as the review included only one completed study.
Assessment of reporting biases
We did not perform a formal assessment of potential publication bias (Lau 2006; Sterne 2011) as the review included only one trial.
Data synthesis
Meta‐analysis was not feasible as the review included only one completed study.
Subgroup analyses
Inadequate data were available to perform subgroup analyses. We had planned to carry out these for each of the following outcomes in order to assess the effect on heterogeneity.
Type of central line inserted (venous tunnelled, venous untunnelled, porta‐cath, whether an emergency or elective procedure).
Type of participants (intensive care, liver disease, other).
Age of participants (neonate, child (one to 15 years), adult (16 years or older)).
Whether participants had associated platelet count abnormalities.
Sensitivity analyses
Only one completed study was identified in this review and therefore no sensitivity analyses could be performed.
Contributions of authors
David Hall: protocol and review development, searching, selection of studies, eligibility and quality assessment, data extraction and analysis and content expert. Lise Estcourt: protocol and review development, searching, selection of studies, eligibility and quality assessment, data extraction and analysis and content expert. Tim Walsh: protocol and review development and content expert. Carolyn Doree: protocol and review development, searching and selection of studies. Marialena Trivella: protocol and review development and statistical expert. Sally Hopewell: protocol and review development and methodological expert.
Sources of support
Internal sources
-
NHS Blood and Transplant, Research and Development, UK.
To fund the work of the Systematic Review Initiative (SRI)
External sources
-
The Cochrane Haematological Malignancies Group, Germany.
For editorial support
-
National Institute for Health Research (NIHR) Cochrane Programme Grant, UK.
To provide funding for systematic reviewers and methodological support from the Centre for Statistics in Medicine, Oxford
Declarations of interest
David Hall: none known. Lise Estcourt: is partly funded by NIHR Cochrane Programme Grant ‐ Safe and Appropriate Use of Blood Components. Timothy Walsh: none known. Carolyn Doree: none known. Marialena Trivella: is partly funded by NIHR Cochrane Programme Grant ‐ Safe and Appropriate Use of Blood Components. Sally Hopewell: is partly funded by NIHR Cochrane Programme Grant ‐ Safe and Appropriate Use of Blood Components.
New
References
References to studies included in this review
Müller 2015 {published and unpublished data}
- Müller M, Arbous M, Spoelstra‐de Man A, Vink R, Karakus A, Straat M, et al. Transfusion of fresh‐frozen plasma in critically ill patients with a coagulopathy before invasive procedures: a randomized clinical trial. Transfusion 2014;55(1):26‐35. [DOI: 10.1111/trf.12750] [DOI] [PubMed] [Google Scholar]
- Müller M, Jonge E, Arbous MS, Spoelstra‐de Man A, Karakus A, Vroom M, et al. Transfusion of fresh frozen plasma in non‐bleeding ICU patients‐TOPIC trial: study protocol for a randomized controlled trial. Trials 2011;12:266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT01143909. Transfusion of fresh frozen plasma in non‐bleeding intensive care unit (ICU) patients (TOPIC). ClinicalTrials.gov [accessed 26 May 2016].
- NTR2262. Transfusion of plasma to prevent bleeding in ICU patients. Nederlands Trial Register [accessed 13 February 2015].
References to studies excluded from this review
Alport 2012 {published data only}
- Alport B, Burbridge B, Lim H. Bard PowerPICC Solo2 vs Cook Turbo‐Ject: A Tale of Two PICCs. Canadian Association of Radiologists Journal 2012;63(4):323‐8. [DOI: 10.1016/j.carj.2011.05.002] [DOI] [PubMed] [Google Scholar]
Amarapurkar 2014 {published data only}
- Amarapurkar D, Shah A, Dharod M, Chandanani M, Baijal R, Kumar P, et al. Coagulopathy in cirrhosis a prospective study to correlate conventional tests of coagulation and bleeding following invasive procedures in cirrhotics. Gastroenterology 2014;146(5):S737. [DOI: 10.1016/S0016-5085(14)62671-8] [DOI] [PubMed] [Google Scholar]
Bartelmaos 2013 {published data only}
- Bartelmaos T, Chabanel A, Léger J, Villalon L, Gillon M, Rouget C, et al. Plasma transfusion in liver transplantation: a randomized, double‐blind, multicenter clinical comparison of three virally secured plasmas. Transfusion 2013;53(8):1335‐45. [DOI: 10.1111/j.1537-2995.2012.03895.x] [DOI] [PubMed] [Google Scholar]
- NCT00235183. Plasma transfusion in liver transplantation. ClinicalTrials.gov [accessed 8 March 2016].
Carino 2009 {published data only}
- Carino G, Tsapenko A, Sweeney J. Fresh frozen plasma use before line insertion in critically‐ill patients with coagulation abnormalities. Critical Care Medicine 2009;37(12):A468. [Google Scholar]
Corash 2006 {published data only}
- Corash L, Bass N, Petz LD, Steadman R, Streif M, McCullough J, et al. Fresh frozen plasma for management of hemostasis during minor and major surgical procedures associated with coagulopathy. Vox Sanguinis 2006;91:185. [Google Scholar]
De Pietri 2016 {published and unpublished data}
- Bianchini M, Pietri L, Maira T, Maria N, Begliomini B, Gerunda G, et al. Thrombelastography decreases hemoderivates requirement before invasive procedures in cirrhotic patients with coagulation disorders. A randomized controlled trial. Hepatology 2013;58(4):292A. [Google Scholar]
- Pietri L, Bianchini M, Montalti R, Maria N, Maira T, Begliomini B, et al. Thrombelastography‐guided blood product use before invasive procedures in cirrhosis with severe coagulopathy. A randomized controlled trial. Hepatology 2016;63(2):566‐73. [DOI: 10.1002/hep.28148] [DOI] [PubMed] [Google Scholar]
- Pietri L, Bianchini M, Montalti R, Maira T, Maria N, Begliomini B, et al. Thrombelastography before invasive procedures reduces hemoderivates requirement in cirrhotic patients with coagulation disorders. A randomized controlled trial. Journal of Hepatology 2013;58:S85‐S86. [Google Scholar]
- Pietri L, Bianchini M, Montalti R, Maria N, Maira T, Begliomini B, et al. Thrombelastography (TEG) decreases blood products requirement before invasive procedures in cirrhotic patients with coagulation tests derangement. A randomized controlled trial. Digestive and Liver Disease 2014;46:e5. [Google Scholar]
- NCT02362178. Thromboelastographic guide for blood products in cirrhotics. ClinicalTrials.gov [accessed 8 March 2016].
Etemadrezaie 2007 {published data only}
- Etemadrezaie H, Baharvahdat H, Shariati Z, Lari S, Shakeri M, Ganjeifar B. The effect of fresh frozen plasma in severe closed head injury. Clinical Neurology and Neurosurgery 2007;109:166‐71. [DOI: 10.1016/j.clineuro.2006.09.001] [DOI] [PubMed] [Google Scholar]
Freeman 1998 {published data only}
- Freeman J, Williamson L, Llewelyn C, Fisher N, Allain J, Bellamy M, et al. A randomized trial of solvent/detergent and standard fresh frozen plasma in the treatment of the coagulopathy seen during orthotopic liver transplantation. Vox Sanguinis 1998;74(S1):225‐9. [10.1111/j.1423‐0410.1998.tb05477.x] [DOI] [PubMed] [Google Scholar]
Friedman 1989 {published data only}
- Friedman E, Sussman I. Safety of invasive procedures in patients with the coagulopathy of liver disease. Clinical & Laboratory Haematology 1989;11:199‐204. [DOI] [PubMed] [Google Scholar]
Gallieni 1995 {published data only}
- Gallieni M, Cozzolino M. Uncomplicated central vein catheterization of high risk patients with real time ultrasound guidance. International Journal of Artificial Organs 1995;18:117‐21. [PubMed] [Google Scholar]
Harter 2004 {published data only}
- Harter C, Egerer G. Peripherally inserted central venous catheters for patients with hematological malignancies. Supportive Care in Cancer 2004;12:815‐6. [DOI: 10.1007/s00520-004-0619-0] [DOI] [PubMed] [Google Scholar]
Holcomb 2015 {published data only}
- Holcomb J, Tilley B, Baraniuk S, Fox E, Wade C, Podbielski J, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA 2015;313(5):471‐82. [DOI: 10.1001/jama.2015.12] [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT01545232. Pragmatic, Randomized Optimal Platelet and Plasma Ratios (PROPPR). ClinicalTrials.gov [accessed 8 March 2016].
Mintz 2006 {published data only}
- Mintz P, Bass N, Petz LD, Steadman R, Streiff M, McCullough J, et al. Photochemically treated fresh frozen plasma for transfusion of patients with acquired coagulopathy of liver disease. Blood 2006;107(9):3753‐60. [DOI] [PubMed] [Google Scholar]
Napolitano 2012 {published data only}
- Napolitano G, Valvano M, Caruso N, Merla A, Lauriola W, Ippolito A, et al. Hemorrhagic complications following invasive procedures in cirrhotic patients with normal or abnormal coagulopathy. A prospective study. Journal of Hepatology 2012;56(S2):S262. [DOI: 10.1016/S0168-8278(12)60675-8] [DOI] [Google Scholar]
NCT00233246 {published data only}
- NCT00233246. Study of hemostasis and invasive procedures. ClinicalTrials.gov 2015 [Accessed on 04 February 2015].
NCT00953901 {published data only}
- NCT00953901. Restrictive versus liberal fresh frozen plasma transfusion prior to low‐risk invasive procedures in hospitalized patients. ClinicalTrials.gov [Accessed 04 February 2015].
NCT01754545 {published data only}
- NCT01754545. Prophylactic plasma infusion therapy for congenital thrombotic thrombocytopenic purpura. ClinicalTrials.gov [Accessed 04 February 2015].
Tinmouth 2008 {published data only}
- Tinmouth A, Chatelain E, Fergusson D, McIntyre L, Giulivi A, Hubert P. A randomized controlled trial of high and standard dose frozen plasma transfusions in critically ill patients. Transfusion 2008;48:26A. [Google Scholar]
Weigand 2009 {published data only}
- Weigand K, Encke J, Meyer FJ, Hinkel U, Munder M, Stremmel W, et al. Low levels of prothrombin time (INR) and platelets do not increase the risk of significant bleeding when placing central venous catheters. Medizinische Klinik 2009;104:331‐5. [DOI] [PubMed] [Google Scholar]
Williamson 1999 {published data only}
- Williamson L, Llewelyn C, Fisher N, Allain J, Bellamy M, Baglin T, et al. A randomized trial of solvent/detergent‐treated and standard fresh‐frozen plasma in the coagulopathy of liver disease and liver transplantation. Transfusion 1999;39:1227‐34. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
NCT02311985 {published data only}
- NCT02311985. Point‐of‐care versus standard coagulation tests versus restrictive strategy to guide transfusion in chronic liver failure patients requiring central venous line: Prospective randomized trial. ClinicalTrials.gov [accessed 27 Oct 2015].
NCT02561026 {published data only}
- NCT02561026. Transfusion of Plasma Prior to Invasive Procedures Pilot Trial (TOPPIT). ClinicalTrials.gov [accessed 8 March 2016].
NCT02637427 {published data only}
- NCT02637427. Does Plasma Reduce Bleeding in Patients Undergoing Invasive Procedures. ClinicalTrials.gov [accessed 28 May 2016].
Additional references
Benjamin 2012
- Benjamin R, McLaughlin L. Plasma components: properties, differences, and uses. Transfusion 2012;52 Suppl 1:9S‐19S. [DOI] [PubMed] [Google Scholar]
Bishop 2007
- Bishop L, Dougherty L, Bodenham A, Mansi J, Crowe P, Kibbler C, et al. Guidelines on the insertion and management of central venous access devices in adults. International Journal of Laboratory Hematology 2007;29:261‐78. [DOI] [PubMed] [Google Scholar]
Dara 2005
- Dara S, Rana R, Afessa B, Moore S, Gajic O. Fresh frozen plasma transfusion in critically ill medical patients with coagulopathy. Critical Care Medicine 2005;33(11):2667‐71. [DOI] [PubMed] [Google Scholar]
Deeks 2011
- Deeks JJ, Higgins JPT, Altman DG (editors). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
DistillerSR [Computer program]
- DistillerSR. DistillerSR: Data Management Software. Ottawa, ON: Evidence Partners, 2015.
Doerfler 1996
- Doerfler M, Kaufman B, Goldenberg A. Central venous catheter placement in patients with disorders of hemostasis. Chest 1996;110(1):185‐8. [DOI] [PubMed] [Google Scholar]
Fisher 1999
- Fisher N, Mutimer D. Central venous cannulation in patients with liver disease and coagulopathy ‐ a prospective audit. Intensive Care Medicine 1999;25(5):481‐5. [DOI] [PubMed] [Google Scholar]
Foster 1992
- Foster P, Moore L, Sankary H, Hart M, Ashmann M, Williams J. Central venous catheterization in patients with coagulopathy. Archives of Surgery 1992;127(3):273‐5. [DOI] [PubMed] [Google Scholar]
Haas 2010
- Haas B, Chittams J, Trerotola S. Large‐bore tunneled central venous catheter insertion in patients with coagulopathy. Journal of Vascular and Interventional Radiology 2010;21(2):212‐7. [DOI] [PubMed] [Google Scholar]
Habib 2014
- Habib M, Roberts LN, Patel RK, Wendon J, Bernal W, Arya R. Evidence of rebalanced coagulation in acute liver injury and acute liver failure as measured by thrombin generation. Liver International 2014;34(5):672‐8. [DOI] [PubMed] [Google Scholar]
Hall 2012
- Hall D, Lone N, Watson D, Stanworth S, Walsh T, Intensive Care Study of Coagulopathy (ISOC) Investigators. Factors associated with prophylactic plasma transfusion before vascular catheterization in non‐bleeding critically ill adults with prolonged prothrombin time: a case‐control study. British Journal of Anaesthesia 2012;109(6):919‐27. [DOI] [PubMed] [Google Scholar]
Higgins 2011a
- Higgins JPT, Deeks JJ (editors). Chapter 7: Selecting studies and collecting data. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Higgins 2011b
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Higgins 2011c
- Higgins JPT, Deeks JJ, Altman DG (editors). Chapter 16: Special topics in statistics. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Holland 2006
- Holland L, Sarode R. Should plasma be transfused prophylactically before invasive procedures?. Current Opinion in Hematology 2006;13(6):447‐51. [DOI] [PubMed] [Google Scholar]
Hunt 2014
- Hunt B. Bleeding and coagulopathies in critical care. New England Journal of Medicine 2014;370(9):847‐59. [DOI] [PubMed] [Google Scholar]
Juffermans 2014
- Hall D, Walsh T. FFP transfusion in the intensive care unit. In: Juffermans N, Walsh T editor(s). Transfusion in the Intensive Care Unit. 1st Edition. Springer, 2014:151‐9. [Google Scholar]
Khan 2007
- Khan H, Belsher J, Yilmaz M, Afessa B, Winters J, Moore S, et al. Fresh‐frozen plasma and platelet transfusions are associated with development of acute lung injury in critically ill medical patients. Chest 2007;131(5):1308‐14. [DOI] [PubMed] [Google Scholar]
Kujovich 2015
- Kujovich, JL. Coagulopathy in liver disease: a balancing act. Hematology American Society Hematology Education Program 2015;2015:243‐9. [DOI] [PubMed] [Google Scholar]
Lau 2006
- Lau J, Ioannidis J, Terrin N, Schmid C, Olkin I. The case of the misleading funnel plot. BMJ 2006;333(7568):597‐600. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Moher 2009
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta‐Analyses: The PRISMA Statement. Annals of Internal Medicine 2009;151(4):264‐9. [DOI] [PubMed] [Google Scholar]
Mumtaz 2000
- Mumtaz H, Williams V, Hauer‐Jensen M, Rowe M, Henry‐Tillman RS, Heaton K, et al. Central venous catheter placement in patients with disorders of hemostasis. American Journal of Surgery 2000;180(6):503‐5. [DOI] [PubMed] [Google Scholar]
Murad 2010
- Murad M, Stubbs J, Gandhi M, Wang A, Paul A, Erwin P, et al. The effect of plasma transfusion on morbidity and mortality: a systematic review and meta‐analysis. Transfusion 2010;50(6):1370‐83. [DOI] [PubMed] [Google Scholar]
Narick 2011
- Narick C, Triulzi D, Yazer M. Transfusion‐associated circulatory overload after plasma transfusion. Transfusion 2011;52(1):160‐5. [DOI] [PubMed] [Google Scholar]
O'Shaughnessy 2004
- O'Shaughnessy D, Atterbury C, Bolton M, Murphy M, Thomas D, Yates S, et al. Guidelines for the use of fresh‐frozen plasma, cryoprecipitate and cryosupernatant. British Journal of Haematology 2004;126(1):11‐28. [DOI] [PubMed] [Google Scholar]
Parmar 1998
- Parmar M, Torri V, Stewart L. Extracting summary statistics to perform meta‐analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17(24):2815‐34. [DOI] [PubMed] [Google Scholar]
Rana 2006
- Rana R, Fernández‐Pérez E, Khan S, Rana S, Winters J, Lesnick T, et al. Transfusion‐related acute lung injury and pulmonary edema in critically ill patients: a retrospective study. Transfusion 2006;46(9):1478‐83. [DOI] [PubMed] [Google Scholar]
Review Manager 5 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sarani 2008
- Sarani B, Dunkman W, Dean L, Sonnad S, Rohrbach J, Gracias V. Transfusion of fresh frozen plasma in critically ill surgical patients is associated with an increased risk of infection. Critical Care Medicine 2008;36(4):1114‐8. [DOI] [PubMed] [Google Scholar]
Schünemann 2011a
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and 'Summary of findings' tables. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Schünemann 2011b
- Schünemann HJ, Oxman AD, Vist GE, Higgins JPT, Deeks JJ, Glasziou P, et al. on behalf of the Cochrane Applicability and Recommendations Methods Group. Chapter 12: Interpreting results and drawing conclusions. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Segal 2005
- Segal J, Dzik W, Transfusion Medicine/Hemostasis Clinical Trials Network. Paucity of studies to support that abnormal coagulation test results predict bleeding in the setting of invasive procedures: an evidence‐based review. Transfusion 2005;45(9):1413‐25. [DOI] [PubMed] [Google Scholar]
Smith 2013
- Smith RN, Nolan JP. Central venous catheters. BMJ 2013;347:f6570. [DOI: 10.1136/bmj.f6570] [DOI] [PubMed] [Google Scholar]
Stanworth 2007
- Stanworth S. The evidence‐based use of FFP and cryoprecipitate for abnormalities of coagulation tests and clinical coagulopathy. Hematology 2007;2007(1):179‐86. [DOI] [PubMed] [Google Scholar]
Stanworth 2010
- Stanworth S, Grant‐Casey J, Lowe D, Laffan M, New H, Murphy M, et al. The use of fresh‐frozen plasma in England: high levels of inappropriate use in adults and children. Transfusion 2010;51(1):62‐70. [DOI] [PubMed] [Google Scholar]
Stanworth 2011
- Stanworth S, Walsh T, Prescott R, Lee R, Watson D, Wyncoll D, et al. A national study of plasma use in critical care: clinical indications, dose and effect on prothrombin time. Critical Care 2011;15(2):R108. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sterne 2011
- Sterne JAC, Egger M, Moher D (editors). Chapter 10: Addressing reporting biases. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Tierney 2007
- Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time‐to‐event data into meta‐analysis. Trials 2007;8:16. [DOI: 10.1186/1745-6215-8-16] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tinmouth 2011
- Tinmouth A, McIntyre L. The conundrum of persistent inappropriate use of frozen plasma. Critical Care 2011;15(3):160. [DOI] [PMC free article] [PubMed] [Google Scholar]
Walsh 2010
- Walsh T, Stanworth S, Prescott R, Lee R, Watson D, Wyncoll D. Prevalence, management, and outcomes of critically ill patients with prothrombin time prolongation in United Kingdom intensive care units. Critical Care Medicine 2010;38(10):1939‐46. [DOI] [PubMed] [Google Scholar]
Watson 2009
- Watson G, Sperry J, Rosengart M, Minei J, Harbrecht B, Moore E, et al. Fresh frozen plasma is independently associated with a higher risk of multiple organ failure and acute respiratory distress syndrome. Journal of Trauma 2009;67(2):221‐8. [DOI] [PubMed] [Google Scholar]
Watson 2011
- Watson D, Stanworth S, Wyncoll D, McAuley D, Perkins G, Young D, et al. A national clinical scenario‐based survey of clinicians' attitudes towards fresh frozen plasma transfusion for critically ill patients. Transfusion Medicine 2011;21(2):124‐9. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Hall 2015
- Hall DP, Estcourt LJ, Doree C, Hopewell S, Trivella M, Walsh TS. Plasma transfusions prior to insertion of central lines for patients with abnormal coagulation. Cochrane Database of Systematic Reviews 2015, Issue 6. [DOI: 10.1002/14651858.CD011756] [DOI] [PMC free article] [PubMed] [Google Scholar]