

ABSTRACT
Objective: The live-attenuated oral polio vaccine (OPV) will be no longer used when wild poliovirus (WPV) eliminating in worldwide, according to GPEI (the Global Polio Eradication Initiative) Reports. It is planning to replace OPV by Sabin-based inactivated poliovirus vaccine (sIPV) in developing countries, with purpose of reducing of the economic burden and maintaining of the appropriate antibody levels in population. It studied serial fractional doses immunized by intradermal injection (ID) in rats, to reduce consume of antigen and financial burden, maintaining sufficient immunogenicity; Methods: Study groups were divided in 4 groups of dose gradient, which were one-tenth (1/10), one-fifth (1/5), one-third (1/3) and one-full dose (1/1), according to the volume of distribution taken from the same batch of vaccine (sIPV). Wistar rats were injected intradermally with the needle and syringe sing the mantoux technique taken once month for 3 times. It was used as positive control that intramuscular inoculation (IM) was injected with one-full dose (1/1) with same batch of sIPV. PBS was used as negative control. Blood samples were collected via tail vein. After 30 d with 3 round of immunization, it analyzed the changes of neutralization antibody titers in the each group by each immunization program end; Results: The results of seroconversion had positive correlation with different doses in ID groups. The higher concentration of D-antigen (D-Ag) could conduct higher seroconversion. Furthermore, different types of viruses had different seroconversion trend. It showed that the geometric mean titers (GMTs) of each fractional-dose ID groups increased by higher concentration of D-Ag, and it got significant lower than the full-dose IM group. At 90th days of immunization, the GMTs for each poliovirus subtypes of fractional doses were almost higher than 1:8, implied that it could be meaning positive seroprotection titer for polio vaccine types, according to WHO suggestion; Conclusions: The fractional dose with one-fifth (1/5) could be used by intradermal injection to prevent poliovirus infection, if there were more human clinical detail research consistent with this findings in rats.
KEYWORDS: fractional dose, intradermal delivery, Sabin IPV
Introduction
The global use of poliovirus vaccines is one of the most effective methods to prevent and control of polio epidemics, according to the World Health Organization (WHO) Global Polio Eradication Initiative launched in 1988.1,2 There were 2 main poliovirus vaccine used in the world, the live-attenuated oral polio vaccine (OPV) and the inactivated poliovirus vaccine (IPV). Most developing countries are still using OPV which has been used for 30 year, e.g. in China. IPV that are currently licensed and used in most developed countries are based on non-attenuated (Salk) vaccine virus strains, which are also referred to as wild-type IPV (wIPV). A lots of achievements have been got toward the elimination of polio, in which the Global Commission for the Certification of Poliomyelitis Eradication (GCC) concluded that wild poliovirus type 2 (WPV2) has been eliminated worldwide, and wild type 3 poliovirus has not been found anywhere in the world for nearly 3 y. wPV type 1 remains endemic only in 2 countries—Afghanistan and Pakistan.3,4 As for Nigeria, no wPV case has been seen since July 24, 2014.5 Although OPV is highly effective against all 3 serotypes of poliovirus and could interrupt chains of wild poliovirus transmission in the world, according to Global Polio Eradication Initiative Report,6 it also could be the source of occasional vaccine-associated paralytic poliomyelitis (VAPP) cases or outbreaks of circulating vaccine-derived polioviruses (VDPVs).7,8 If the current efforts to eradicate polioviruses are successful, and the scientist seeks to remain poliovirus-free situation, adverse reactions of OPV must to be solved, e.g., VAPP and VDPVs.
Therefore, inactivated poliovirus vaccine (IPV) might be a better choice to overcome restoration of virulence for long-term use.9,10 In addition, the eradication with WPV2 make worldwide health works consider that bivalent OPV (bOPV) should instead of trivalent OPV (tOPV) by removal of type 2 poliovirus.
According to the WHO Strategic Advisory Group of Experts on Immunization (SAGE), the plan of bivalent OPV using were implemented from April 2016.11 But it will take some time and some preparation before worldwide population immunized.
The important project was to establish the lasting immunity against the type 2 poliovirus among the whole population before immunized by bivalent OPV. The usage of sIPV, including type 1, 2 and 3 viruses, could stimulate human produce antibodies. So the routine immunization programs might be useful for whole population to maintain high level of antibodies with type 2 poliovirus.12
WHO Global Action Plan (GAP) III make plan to control minimize poliovirus facility-associated risk in the phase post-eradication/post-OPV in somewhere. This plan might be very helpful in low-income countries where the transmissibility of polioviruses is high.13,14 On the other side, Sabin polioviruses have less demanding of production conditions and production facility offers.15 Therefore, sIPV is very promising to developing countries. However, because of expensive production costs of sIPV, the low- and middle-income countries (LMICs) rarely use it. After review some reported methods, there are some useful suggestion, including: intradermal delivery (ID), ombined with adjuvant, lowered usage, optimization of production processes, use of Sabin strains,16-18 which is to reduce the cost.19
ID of fractional doses has been investigated for several vaccines, most notably influenza, and hepatitis B vaccines.20,21 ID firstly targeted to the resident Dendritic cells (DC) located in the deeper dermis, then the immature DC captured and processed the antigen. Dendritic cells that circulate in blood do not have all the typical features of their counterparts in tissue, i.e. they are less mature and have no dendrites. Still, they can perform complex functions including chemokine-production (in CD1c+ myeloid DCs), cross-presentation (in CD141+ myeloid DCs), and IFNalpha production (in CD303+ plasmacytoid DCs).22
Production license of Sabin-IPV was approved by CFDA (China Food and Drug Administration) in February, 2015, which affirmed the efficacy and safety of that vaccine using for human. However, according to our previous clinical studies, it demonstrated that sIPV conduct little immunity by IM method, compared with wild strain IPV (wIPV).23 Because of the high density of Dendritic cells (DC) in the skin, ID method could provide more sufficient initiative immune than intramuscular inoculation.
But the immunogenicity of sIPV administered by intradermally is unclear. To analyze that effect, it used the needle syringe in Wistar rats to evaluate the immune response by the fractional dose of sIPV. It was used as positive control that intramuscular inoculation (IM) was injected with one-full dose (1/1) with same batch of sIPV.
Results
Seroconversion analyzed
Definition: Blood samples were transported to Institute of Medical Biology where the separated serum was stored at −20°C till tested. Antibody determination was done by the standard micro-neutralization technique using Hep-2 cells. The sera were heated for half an hour at 56°C and tested in 12 steps of 2-fold dilutions from 1:4 to 1:8192. The paired samples were tested together and the titers were expressed as the reciprocal of those serum dilutions inhibiting viral growth by 50% or more. If no antibody was detected in 1:8 dilution in the vaccination sample, the serum was considered negative for polio antibodies. Detection of a 4-fold rise in antibody titer or a change in titer from less than 1:8 to 1:8 or more in paired serum was considered as seroconversion.
After first immunization 30 days, the seroconversion of ID group with different dose had different results. The higher concentration of D-Ag could conduct higher seroconversion. The effective antibody titers of rats immunized by 1/10- and 1/5-dose in ID group, was significantly lower than by one-full dose in IM group, for each subtype of poliovirus. But the 1/3-dose in ID group could stimulate the body to produce more antibodies than other fractional dose (Table 1).
Table 1.
Analyzed Seroconversion of trivalent sIPV with different fractional dose injection between ID and IM experiment group.
| Fractional-dose ID sIPV |
|||||||
|---|---|---|---|---|---|---|---|
| |
Full-dose IMsIPV (%) |
1/10-dose (%) |
P Value |
1/5-dose (%) |
P Value |
1/3-dose (%) |
P Value |
| The first immunization | |||||||
| Poliovirus type 1 | 90 | 15 | 0.000 | 30 | 0.000 | 55 | 0.013 |
| Poliovirus type 2 | 75 | 15 | 0.000 | 35 | 0.011 | 60 | 0.311 |
| Poliovirus type 3 | 95 | 50 | 0.001 | 70 | 0.091 | 80 | 0.342 |
| The second immunization | |||||||
| Poliovirus type 1 | 100 | 60 | 0.003 | 85 | 0.231 | 95 | 1.000 |
| Poliovirus type 2 | 100 | 55 | 0.001 | 90 | 0.487 | 95 | 1.000 |
| Poliovirus type 3 | 100 | 80 | 0.106 | 95 | 1.000 | 100 | NS |
| The third immunization | |||||||
| Poliovirus type 1 | 100 | 80 | 0.106 | 100 | NS | 100 | NS |
| Poliovirus type 2 | 100 | 70 | 0.020 | 100 | NS | 100 | NS |
| Poliovirus type 3 | 100 | 90 | 0.487 | 100 | NS | 100 | NS |
NOTE: Seroconversion refers to a reciprocal antibody titer of 8 or higher. Data are proportion (%) of subjects with seroconversion (n = 20), unless otherwise indicated. P values were calculated with the chi-square tests (with the Fisher's exact test). NS denotes not-significant. P values are compared with the full-dose IM group.
Abbreviations:
sIPV, Sabin strain inactivated polio vaccine;
ID, intradermal;
IM, intramuscular.
Furthermore, different types had different seroconversion trend. As for type 1, it had significant difference between ID group and IM group in each dose. However, the one-third dose could achieve enough high seroconversion for type 2 and type 3.
As the immunized continuously 3 times, the seroconversion could grow highly for each type with different dose in ID group. After the third time Immunization, there was no significant different in each type seroconversion between ID and IM group for every fractional doses, which showed in talbe1. But till the second immunization, the ID injection couldn't stimulate the rat body to produce enough antibodies. So the third ID immunization was necessary, compared with IM immunization.
The neutralizing antibody level
In order to analyze the level of special antibody growth and its relationship with dosage, it calculated the antibody geometric mean titers (GMTs). The reference sera used in the neutralizing test were from Chinese National Institutes for Food and Drug Control. The geometric mean titres (GMTs) against poliovirus types 1, 2, and 3 in each group were increased more slowly, in ID group than IM group after the first time immunization. The antibody titers in the ID groups were as low as 1:8.
However, there was rapid growth of special antibody in the ID group, after the second time immunization 30 days, with titer of ≥11.57. Up to the third time aggrandizement immunity, the antibody titer could increase to ≥55.02 in the frational-dose ID group. Table 2 showed that the antibody stimulated by ID with 1/3-dose were almost lower 5 times than IM with full-dose, for type 1 and 3. But, for type 2, the ID might be better a immunization routes than IM, because litter dose of virus stimulated more degree of antibody.
Table 2.
The geometric mean titres (GMTs) against poliovirus types 1, 2, and 3 in each group for different fractional dose by 3 time immunized.*
| Fractional-dose ID sIPV |
||||
|---|---|---|---|---|
| Poliovirus type, dose | Full-dose IM sIPV(n = 20) | 1/10-dose ID (n = 20) | 1/5-dose ID (n = 20) | 1/3-dose ID (n = 20) |
| Type 1 Antibody titer—GMT(95% CI) | ||||
| First dose | 45.60 (24.64–84.39) | 3.48 (2.55–4.76) | 4.29 (2.75–6.69) | 9.34 (5.12–17.05) |
| Second dose | 1168.14 (844.82–1615.20) | 11.57 (5.66–23.66) | 54.72 (25.87–115.74) | 133.53 (76.34–233.55) |
| Third dose | 1480.63 (1109.50–1975.91) | 73.67 (30.57–177.52) | 241.19 (127.90–454.80) | 453.20 (257.67–797.09) |
| Type 2 Antibody titer—GMT(95% CI) | ||||
| First dose | 11.80 (7.29–19.12) | 3.14 (2.17–4.54) | 4.67 (3.09–7.07) | 12.47 (6.14–25.33) |
| Second dose | 744.43 (438.31–1264.37) | 12.08 (5.34–27.34) | 28.90 (16.06–52.00) | 59.30 (29.73–118.27) |
| Third dose | 987.75 (715.94–1362.75) | 55.02 (18.37–164.85) | 183.04 (108.24–309.52) | 300.66 (164.21–550.50) |
| Type 3 Antibody titer—GMT(95% CI) | ||||
| First dose | 50.04 (31.75–78.86) | 7.62 (4.04–14.36) | 12.76 (6.67–24.44) | 15.63 (8.34–29.29) |
| Second dose | 971.45 (688.35–1370.99) | 54.72 (18.63–160.74) | 85.87 (49.03–150.38) | 148.16 (91.04–241.12) |
| Third dose | 1488.87 (1211.18–1830.22) | 111.04 (49.94–246.94) | 229.13 (125.03–419.90) | 409.30 (289.03–579.59) |
NOTE: Antibody titer was expressed as geometric mean titers.
Reverse Cumulative-Distribution Curves of antibody titers in serum samples obtained on days 30, 60 and 90, according to the number and timing of vaccine doses (Fig. 1). The percentages of subjects are based on the total number of subjects tested in each of the vaccine groups. All vaccine groups received different fractional doses according to the immunization schedule. Titers are expressed as reciprocal of the dilution and are given on a log2 scale.
Figure 1.
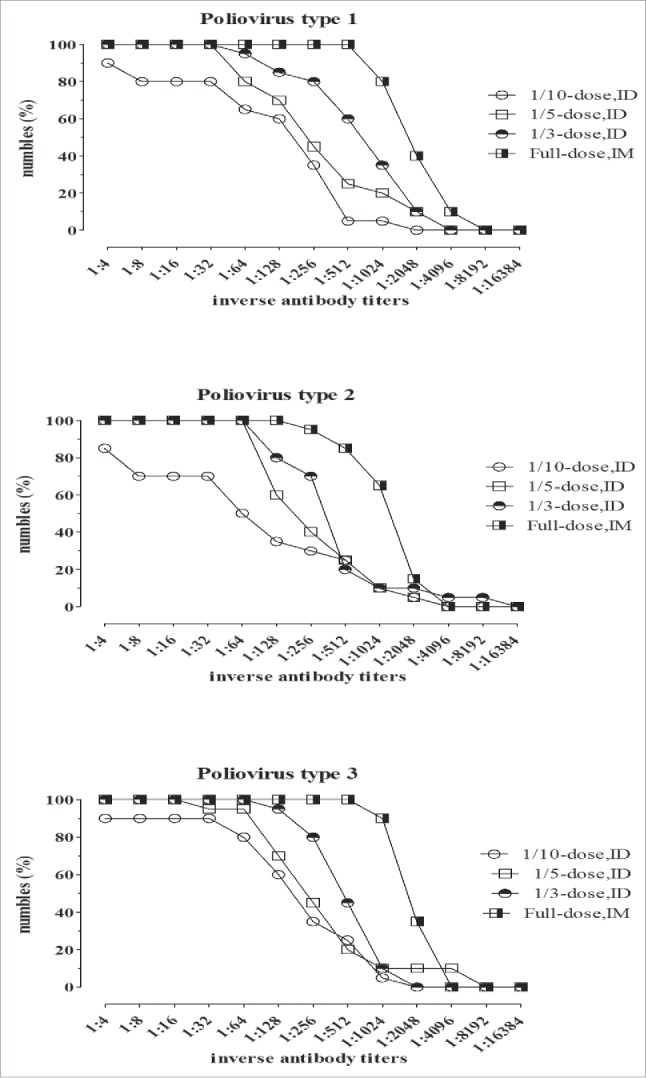
The Reverse cumulative distribution curves of antibody titers with different fractional dose of sIPV.
It showed that GMTs of the fractional-dose ID groups increased with higher concentration of D-Ag and were significant lower than the full-dose IM group. At 90th days of immunization, the GMTs for each poliovirus subtypes of fractional doses were almost higher than 1:8.
Vaccine delivery and safety
Animal conditions:The condition of the rats was monitored frequently, especially their actions, weights and reactions at the inoculation site. No convulsion, shock, death or other serious adverse effect was recorded in intradermal and intramuscular delivery group. Diameter of skin rash was measured after each immunization in the ID groups. Their weights increased and have no significant difference between the study groups and the control group (P > 0.5 (Fig. 2)).
Figure 2.
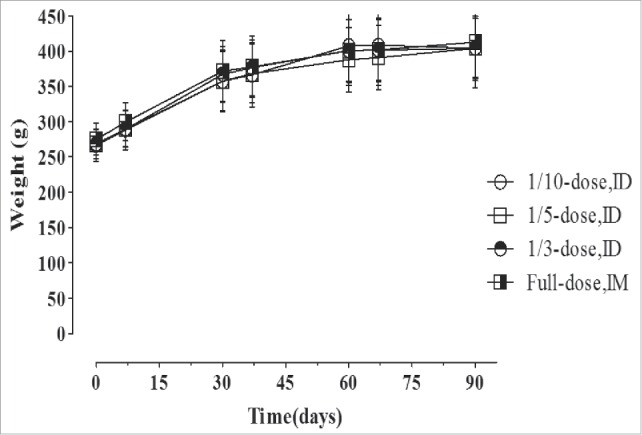
The Weights changes of rats on every 30 d after experiment immunized.
After experiment, the animals were in good conditions. Their weights were grown slowly and steady. It illustrated that the fractional doses of Sabin-inactivated poliovirus vaccine (sIPV) by intradermal injection would be safe to new direction for sIPV developing.
Discussion
Our study was to evaluate the immune effect with different fractional doses of sIPV by intradermally injection into Wistar rats. Our findings show that both 1/3-dose and 1/5-dose of sIPV could conduct high rates of seroconversion about all 3 poliovirus serotypes after third time aggrandizement immunity. According to vaccine schedule results, there was no significant different, compared with full-dose sIPV intramuscularly injection.
Furthermore, the rates of seroconversion seem to increase much more after the second dose in the intradermal groups than intramuscular group. After experiment, the animals were in good conditions. It illustrated that the fractional doses of Sabin-inactivated poliovirus vaccine (sIPV) by intradermal injection was in good efficacy and safety, which could be a new direction for sIPV developing.
At present, the license of prepared sIPV with IM injection by our institute has been already approved in China in June 30, 2015. The D-Ag Concentration contents were 30, 32, and 45 DU/0.5ml/per dose for types 1, 2, and 3, respectively. At this research, we have been performing fractional-dose ID study in order to reduce the consumption of sIPV antigen. However, this study also has a limitation, which is the small number of samples. This fractional-dose ID study in rats was meaningful for the further human clinical trials using of ID injection of sIPV, to reduce affordable IPV for developing countries.
There were several clinical and preclinical trials of ID franctional dose of wIPV reported.24,25 The studies of ID fractional doses of wIPV using Bioject needle-free devices in Oman and Cuba showed immunogenicities similar to those of IM injection, and to those in another recent trial in the Netherlands that involved ID of wIPV at a fractional dose with a PharmaJet Needle-free injector.26-28 However, in our study, it used Sabin strains not wild strain. The Sabin strain might be more safety, because of its clear genetic background and protein structure. On the other hand, our findings are of great significance for reducing antigen content of sIPV. The results confirm that ID administration of fractional 1/5 dose of sIPV could stimulate similar seroconversion as previous studies of wIPV.
By studying the difference of geometric mean titres (GMTs) between sIPV with fractional dose in ID group and one-full dose in IM group, it analyzed their reverse cumulative distributions. Although the GMTs of fractional-dose in ID groups were higher than protection level (1:8) after the third immunized, the antibody titers in the fractional-dose ID groups were significantly lower than in the full-dose IM group. However, a serum neutralizing antibody titer of 1:8 is considered to be a level of effective antibody protection againsted poliovirus.29
It should be point out that the first dose of fractional-dose of sIPV in the ID groups only stimulated lower seroconversion than IM group with one-full dose. But, the rates of seroconversion could increase faster after the second dose in the ID group. The reason might be that the low dose could induct temporary immune tolerance.
The fractional-dose of sIPV could be using with ID method (even in low seroconversion), which might produce the priming immune response for the body. The priming response might produce a rapid anamnestic immune response following the second time or even third enhance immunized with antigen like wIPV.30 It should make further detail following-up with sIPV, because immune memory is important to protect against poliomyelitis.31,32
In conclusion, our results showed that the more than 1/5-dose of sIPV by intradermal injection can produce the sufficient antibody protection in rats. Although there are some degree differences of the immune systems between rats and humans, this study might contribute the usage of fractional doses of Sabin-inactivated poliovirus vaccine (sIPV) with intradermal delivery for human. In fact, it need more research of vaccine clinical details before using for human. Regarding the cost-effectiveness of antigen consumed, the less consumption inducted fewer cost. So special fractional dose of sIPV by ID might be more suitable and applicable for developing country.33,34 Additionally, the safety and immunogenicity of ID of sIPV fractional doses need more evaluate in further human clinical trials.
Methods and materials
Animal sources
Wistar rats were purchased from Beijing Weitong Lihua Experimental Animal Technology Co. Ltd., with weight of 200–350 g. Female and male were half and half. All the animals were feed in the standard specific pathogen free (SPF) condition and under the care at the Institute of Medical Biology, Chinese Academy of Medicine Sciences, complying with the local laws and the protocols approved by the Institutional Animal Care & Welfare Committee and the Institutional Animal Experimental Ethical Inspection. All the animal experiments were under the supervision of the Animal Experimental Ethics Committee of Peking Union Medical College (Peking, China).
Vaccines
The used trivalent sIPV were prepared by the Institute of Medical Biology, Chinese Academy of Medical Sciences. The indirect Enzyme-linked immunosorbent assay (ELISA) method for detecting D-Ag using purified calf and rabbit anti-poliovirus IgG as the capture and detector Ab respectively was established in our laboratory. The international IPV reference reagent WHO 91/574 was used as a reference for calibration of Sabin IPV D-Ag content. The one-full dose (1/1) sIPV was composed with 30 DU of type 1, 32 DU of type 2, and 45 DU of type 3, in 0.5 ml volume.
Study schedule
80 rats were randomly divided into 4 groups (10 males and 10 females rats per group). It used 3 different fractional doses of the sIPV, which were 0.05, 0.1, and 0.17 ml of sIPV, representing 1/10, 1/5, and 1/3 of the full-dose respectively. After shearing rats' right back arm hair and stepwise iodine and alcohol disinfection, injected different doses into rats' right back arm for experiment groups using a needle syringe, replaced with PBS for blank control group. As for positive control group, it intramuscularly injected with the full-dose of sIPV. The Immunization procedure schedule of rats experiment was at 1st, 31st, and 61st. Taken Tail vein blood before each time of intradermal injection, and separated their serum. After first Immunization, it taken weight record every week, until 91st day. The Immunization schedule was illustrated in Figure 3.
Figure 3.
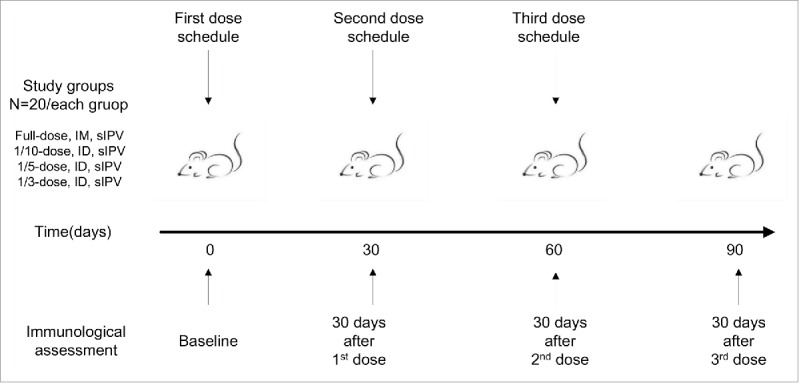
The Immunization schedule on wistar rats by serial fractional dose with ID injection.
Neutralization test
The titers of neutralizing antibodies against poliovirus types 1, 2 and 3 were determined using the micro-neutralization assay, according to the Manual for the virological investigation of polio.35 Serum samples pre-diluted fourfold with MEM (Gibco) were inactivated at 56°C for 30 mins. Samples were diluted by twofold step from 1:4 to 1:8192, and each sample had a duplicate well. Dilutions were neutralized for 3 hours at 35°C using 100 CCID50 (50% cell culture infectious dose) of Sabin strain poliovirus type 1, 2 and 3.
Hep-2 cells (1.0 × 104 cells per well) were added to the serum/virus mixture. After incubated for 7 d at 35°C (5% CO2), the results of the cytopathic effects (CPEs) were observed. The reciprocal of the highest serum dilution that inhibited 50% of the virus cytopathogenic effect was taken as the neutralization antibody titer against special type poliovirus. The seroconversion was defined as a titer ≥ 1:8 after vaccination.36
Statistical analysis
Statistical analyses were performed using IBM®SPSS® Statistics, version 21.0. The seroconversion rates were compared using the χ2 test (Fisher's exact test). Differences among the distribution of antibody titers were tested by one-way analysis of variance. Statistical significance was defined as P-value < 0.05. The 95% confidence intervals (CIs) of median values were derived by simulation.
Abbreviations
- sIPV
Sabin strain inactivated polio vaccine
- ID
intradermal
- IM
intramuscular
- CI
confidence interval
- OPV
oral polio vaccine
- WPV
wild poliovirus
- GMTs
geometric mean titers
- WHO
World Health Organization
- GCC
Global Commission for the Certification
- VAPP
vaccine-associated paralytic poliomyelitis
- SAGE
Strategic Advisory Group of Experts on Immunization
- GAP
Global Action Plan
- LMICs
low- and middle-income countries
- DC
endritic cells
- CFDA
China Food and Drug Administration
- GPEI
Global Polio Eradication Initiative
- SPF
specific pathogen free
- ELISA
Enzyme-linked immunosorbent assay
- CPEs
cytopathic effects
- CIs
confidence intervals
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Funding
This work was supported by Innovation team project in Yunnan Province #2015HC027; International Cooperation Project (2010DFB32890); The National 863 Program (2012AA02A404); Bill & Melinda Gates Foundation (OPP1049425).
References
- [1].Ward N, Milstien J, Hull H, Hull B. A global overview and hope for the eradication of poliomyelitis by the year 2000. Trop Geogr Med 1993; 45(5):198-202; PMID:8279055.15514582 [PubMed] [Google Scholar]
- [2].Centers for Disease Control and Prevention (CDC) . Laboratory surveillance for wild and vaccine-derived polioviruses, January 2003-June 2004. MMWR Morb Mortal Wkly Rep 2004; 53(42):990-3; PMID:15514582 [PubMed] [Google Scholar]
- [3].Norris A, Hachey K, Curtis A, Bourdeaux M. Crippling violence: Conflict and incident polio in Afghanistan. PLoS One 2016; 11:e0149074; PMID:26958854; http://dx.doi.org/ 10.1371/journal.pone.0149074 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Khan MU, Ahmad A, Aqeel T, Akbar N, Salman S, Idress J. A cross-sectional survey of healthcare workers on the knowledge and attitudes towards polio vaccination in Pakistan. PLoS One 2015; 10:e0142485; PMID:26559184; http://dx.doi.org/ 10.1371/journal.pone.0142485 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Manya S, Qazi J. From Pakistan a line of hope for ‘The polio eradication and endgame strategic plan 2013–2018’. Infect Dis (Lond) 2016; 48:167-8; PMID:26417889; http://dx.doi.org/ 10.3109/23744235.2015.1092050 [DOI] [PubMed] [Google Scholar]
- [6].Wang HB, Zhu SL, Zheng JS, Gou AL, Cui H, Zhang Y, Ning GJ, Fan CX, Chen YS, Li KL, et al.. Sero-survey of polio antibodies during wild poliovirus outbreak in southern Xinjiang Uygur Autonomous Region, China. PLoS One 2014; 9:e80069; PMID:24991811; http://dx.doi.org/ 10.1371/journal.pone.0080069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Kew OM, Sutter RW, de Gourville EM, Dowdle WR, Pallansch MA. Vaccine-derived polioviruses and the endgame strategy for global polio eradication. Annu Rev Microbiol 2005; 59:587-635; PMID:16153180; http://dx.doi.org/ 10.1146/annurev.micro.58.030603.123625 [DOI] [PubMed] [Google Scholar]
- [8].Jenkins HE, Aylward RB, Gasasira A, Donnelly CA, Mwanza M, Corander J, Garnier S, Chauvin C, Abanida E, Pate MA, Adu F, Baba M, Grassly NC. Implications of a circulating vaccine-derived poliovirus in Nigeria. N Engl J Med 2010; 362:2360-9; PMID:20573924; http://dx.doi.org/ 10.1056/NEJMoa0910074 [DOI] [PubMed] [Google Scholar]
- [9].Sutter RW, Caceres VM, Mas Lago P. The role of routine polio immunization in the post-certification era. Bull World Health Organ 2004; 82:31-9; PMID:15106298 [PMC free article] [PubMed] [Google Scholar]
- [10].Inactivated poliovirus vaccine following oral poliovirus vaccine cessation. Wkly Epidemiol Rec 2006; 81:137-44; PMID:16673508 [PubMed] [Google Scholar]
- [11].Okayasu H, Sutter RW, Jafari HS, Takane M, Aylward RB. Affordable inactivated poliovirus vaccine: strategies and progress. J Infect Dis 2014; 210(Suppl 1):S459-64; PMID:25316868; http://dx.doi.org/ 10.1093/infdis/jiu128 [DOI] [PubMed] [Google Scholar]
- [12].Muller DA, Pearson FE, Fernando GJ, Agyei-Yeboah C, Owens NS, Corrie SR, Crichton ML, Wei JC, Weldon WC, Oberste MS, et al.. Inactivated poliovirus type 2 vaccine delivered to rat skin via high density microprojection array elicits potent neutralising antibody responses. Sci Rep 2016; 6:22094; PMID:26911254; http://dx.doi.org/ 10.1038/srep22094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Conclusions and recommendations of the Advisory Committee on Poliomyelitis Eradication, Geneva, 27–28 November 2007. Wkly Epidemiol Rec 2008; 83:25-35; PMID:18203406 [PubMed] [Google Scholar]
- [14].Bruce Aylward R, Sutter RW, Cochi SL, Thompson KM, Jafari H, Heymann D. Risk management in a polio-free world. Risk Anal 2006; 26:1441-8; PMID:17184391; http://dx.doi.org/ 10.1111/j.1539-6924.2006.00840.x [DOI] [PubMed] [Google Scholar]
- [15].Polio Eradication Initiative Cessation of routine oral polio vaccine (OPV) use after global polio eradication: Framework for national policy makers in OPV-using countries. Geneva, Switzerland: World Health Organization; 2005. [Google Scholar]
- [16].Dietrich J, Andreasen LV, Andersen P, Agger EM. Inducing dose sparing with inactivated polio virus formulated in adjuvant CAF01. PLoS One 2014; 9:e100879; PMID:24956110; http://dx.doi.org/ 10.1371/journal.pone.0100879 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Thomassen YE, van 't Oever AG, van Oijen MG, Wijffels RH, van der Pol LA, Bakker WA. Next generation inactivated polio vaccine manufacturing to support post polio-eradication biosafety goals. PLoS One 2013; 8:e83374; PMID:24349497; http://dx.doi.org/ 10.1371/journal.pone.0083374 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Mahmood K, Pelkowski S, Atherly D, Sitrin RD, Donnelly JJ Hexavalent IPV-based combination vaccines for public-sector markets of low-resource countries. Hum Vaccin Immunother 2013; 9:1894-902; PMID: 23787559; http://dx.doi.org/24469907 10.4161/hv.25407 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].van der Maaden K, Trietsch SJ, Kraan H, Varypataki EM, Romeijn S, Zwier R, van der Linden HJ, Kersten G, Hankemeier T, Jiskoot W, et al.. Novel hollow microneedle technology for depth-controlled microinjection-mediated dermal vaccination: a study with polio vaccine in rats. Pharm Res 2014; 31:1846-54; PMID:24469907 [DOI] [PubMed] [Google Scholar]
- [20].McAllister L, Anderson J, Werth K, Cho I, Copeland K, Le Cam Bouveret N, Plant D, Mendelman PM, Cobb DK. Needle-free jet injection for administration of influenza vaccine: a randomised non-inferiority trial. Lancet 2014; 384:674-81; PMID:24881803; http://dx.doi.org/ 10.1016/S0140-6736(14)60524-9 [DOI] [PubMed] [Google Scholar]
- [21].Lebre F, Borchard G, de Lima MC, Borges O. Progress towards a needle-free hepatitis B vaccine. Pharm Res 2011; 28:986-1012; PMID:21088986; http://dx.doi.org/ 10.1007/s11095-010-0314-4 [DOI] [PubMed] [Google Scholar]
- [22].Le Borgne M, Etchart N, Goubier A, Lira SA, Sirard JC, van Rooijen N, Caux C, Aït-Yahia S, Vicari A, Kaiserlian D, et al.. Dendritic cells rapidly recruited into epithelial tissues via CCR6/CCL20 are responsible for CD8+ T cell crosspriming in vivo. Immunity 2006; 24:191-201; PMID:16473831; http://dx.doi.org/ 10.1016/j.immuni.2006.01.005 [DOI] [PubMed] [Google Scholar]
- [23].Liao G, Li R, Li C, Sun M, Li Y, Chu J, Jiang S, Li Q. Safety and immunogenicity of inactivated poliovirus vaccine made from Sabin strains: a phase II, randomized, positive-controlled trial. J Infect Dis 2012; 205:237-43; PMID:22158682; http://dx.doi.org/ 10.1093/infdis/jir723 [DOI] [PubMed] [Google Scholar]
- [24].Kouiavskaia D, Mirochnitchenko O, Dragunsky E, Kochba E, Levin Y, Troy S, Chumakov K. Intradermal inactivated poliovirus vaccine: a preclinical dose-finding study. J Infect Dis 2014; PMID:25391313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Resik S, Tejeda A, Mach O, Fonseca M, Diaz M, Alemany N, Garcia G, Hung LH, Martinez Y, Sutter R. Immune responses after fractional doses of inactivated poliovirus vaccine using newly developed intradermal jet injectors: a randomized controlled trial in Cuba. Vaccine 2015; 33:307-13; PMID:25448109; http://dx.doi.org/ 10.1016/j.vaccine.2014.11.025 [DOI] [PubMed] [Google Scholar]
- [26].Mohammed AJ, AlAwaidy S, Bawikar S, Kurup PJ, Elamir E, Shaban MM, Sharif SM, van der Avoort HG, Pallansch MA, Malankar P, et al.. Fractional doses of inactivated poliovirus vaccine in Oman. N Engl J Med 2010; 362:2351-9; PMID:20573923; http://dx.doi.org/ 10.1056/NEJMoa0909383 [DOI] [PubMed] [Google Scholar]
- [27].Resik S, Tejeda A, Lago PM, Diaz M, Carmenates A, Sarmiento L, Alemani N, Galindo B, Burton A, Friede M, et al.. Randomized controlled clinical trial of fractional doses of inactivated poliovirus vaccine administered intradermally by needle-free device in Cuba. J Infect Dis 2010; 201:1344-52; PMID:20350164; http://dx.doi.org/ 10.1086/651611 [DOI] [PubMed] [Google Scholar]
- [28].Soonawala D, Verdijk P, Wijmenga-Monsuur AJ, Boog CJ, Koedam P, Visser LG, Rots NY. Intradermal fractional booster dose of inactivated poliomyelitis vaccine with a jet injector in healthy adults. Vaccine 2013; 31:3688-94; PMID:23770332; http://dx.doi.org/ 10.1016/j.vaccine.2013.05.104 [DOI] [PubMed] [Google Scholar]
- [29].Plotkin SA, Vidor E. Poliovirus vaccine–inactivated In: Plotkin SA, Orenstein WA (eds) Vaccines, 4th edition. Philadelphia, PA: Saunders; 2004; 24:625-49. [Google Scholar]
- [30].Resik S, Tejeda A, Sutter RW, Diaz M, Sarmiento L, Alemani N, Garcia G, Fonseca M, Hung LH, Kahn AL, et al.. Priming after a fractional dose of inactivated poliovirus vaccine. N Engl J Med 2013; 368:416-24; PMID:23363495; http://dx.doi.org/ 10.1056/NEJMoa1202541 [DOI] [PubMed] [Google Scholar]
- [31].Avdicova M, Crasta PD, Hardt K, Kovac M. Lasting immune memory against hepatitis B following challenge 10–11 years after primary vaccination with either three doses of hexavalent DTPa-HBV-IPV/Hib or monovalent hepatitis B vaccine at 3, 5 and 11–12 months of age. Vaccine 2015; 33:2727-33; PMID:24962750; http://dx.doi.org/ 10.1016/j.vaccine.2014.06.070 [DOI] [PubMed] [Google Scholar]
- [32].Li R, Li CG, Li Y, Liu Y, Zhao H, Chen X, Kuriyakose S, Van Der Meeren O, Hardt K, Hezareh M, et al.. Primary and booster vaccination with an inactivated poliovirus vaccine (IPV) is immunogenic and well-tolerated in infants and toddlers in China. Vaccine 2016; 34:1436-43; PMID:26873055; http://dx.doi.org/ 10.1016/j.vaccine.2016.02.010 [DOI] [PubMed] [Google Scholar]
- [33].Wyman O Global post-eradication IPV supply and demand assessment: integrated findings. Commissioned by the Bill & Melinda Gates Foundation and prepared by Oliver Wyman, Inc. March 2009. Available at: www.oliverwyman.com. Accessed 20 April 2011. [Google Scholar]
- [34].Tano Y, Shimizu H, Martin J, Nishimura Y, Simizu B, Miyamura T. Antigenic characterization of a formalin-inactivated poliovirus vaccine derived from live-attenuated Sabin strains. Vaccine 2007; 25:7041-6; PMID:17825459; http://dx.doi.org/ 10.1016/j.vaccine.2007.07.060 [DOI] [PubMed] [Google Scholar]
- [35].World Health Organization Manual for the virological investigation of polio. WHO/EPI/GEN/97.01.44–51. 1997. Available at: http://www.who.int/mediacentre/factsheets/fs114/en/. Accessed 24 November 2011. [Google Scholar]
- [36].World Health Organization Expanded Programme on Immunization. Report of a WHO informal consultation on polio neutralizing antibody assays, Nashville, 5–6 December 1991. Geneva: (WHO/EPI/RD/913 Rev 1; ) 1991. [Google Scholar]