

Abstract
The difference in clinical features and treatment outcomes between localized sinonasal diffuse large B cell lymphoma (SN-DLBCL) and sinonasal extranodal NK/T cell lymphoma (SN-ENKTL) is unclear. Therefore, we analyzed a total of 47 patients with localized SN-DLBCL and 211 patients with localized SN-ENKTL. The age distribution for these two subtypes is very distinct and the B symptoms were more common in SN-ENKTL. However, both SN-DLBCL and SN-ENKTL patients could achieve high overall response rate (ORR) and favorable prognoses. The 3-year overall survival (OS) rates for patients with SN-DLBCL and SN-ENKTL were 79.7 and 83.6% (p = 0.707), and the 3-year progression-free survival (PFS) rates were 61.4 and 70.1% (p = 0.294), respectively. For SN-DLBCL patients, chemotherapy followed by involved-field radiotherapy (IFRT) resulted in higher OS (83.7 vs 62.5%) and PFS (63.9 vs 50.0%) compared with chemotherapy alone, but the difference was not significant. No significant difference was found in the OS or PFS between radiotherapy alone and radiotherapy combined with chemotherapy for all patients with SN-ENKTL. But in extensive stage I and stage II SN-ENKTL patients, radiotherapy combined with chemotherapy could significantly improve the PFS (73.8 vs 50.0%) compared with radiotherapy alone. These results indicate that remarkable clinical disparities exist between localized SN-DLBCL and SN-ENKTL. However, different treatment strategies for them can result in similarly favorable prognoses.
Electronic supplementary material
The online version of this article (doi:10.1186/s13045-016-0368-9) contains supplementary material, which is available to authorized users.
Keywords: Diffuse large B cell lymphoma, Extranodal NK/T cell lymphoma, Sinonasal, Localized
Dear Editor
Remarkable differences exist in the distribution of lymphoma subtypes between China and western populations. The incidence of extranodal NK/T cell lymphoma (ENKTL) is much higher in China [1, 2]. Diffuse large B cell lymphoma (DLBCL) and ENKTL are most common subtypes of sinonasal lymphomas. What is more, both sinonasal DLBCL (SN-DLBCL) and sinonasal ENKTL (SN-ENKTL) are typically diagnosed in the localized stage which represents 70–90% of cases [3, 4]. Since the difference between localized SN-DLBCL and SN-ENKTL has seldom been demonstrated before and is not clear, this study provides a comprehensive evaluation that focuses on clinical features and prognoses of localized SN-DLBCL and SN-ENKTL in Chinese patients.
A total of 47 consecutive patients with localized SN-DLBCL and 211 patients with localized SN-ENKTL from 2000 to 2014 were compared at the Cancer Hospital of Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China. The methods used in this study are detailed in Additional file 1. This study showed that the incidence of SN-ENKTL was much higher than that of SN-DLBCL in China, which was opposite to the situation in the USA [4]. The ratio of males to females was 1.14:1 in SN-DLBCL and 2.40:1 in SN-ENKTL. Patients with SN-DLBCL had a higher median age (63 years old) than those with SN-ENKTL (40 years old). The B symptoms were more common in SN-ENKTL. The comparison of the main clinical characteristics between these two groups is presented in Table 1.
Table 1.
Clinical characteristics of patients with localized SN-DLBCL and SN-ENKTL
| Characteristic | All patients (n = 258), n (%) |
SN-DLBCL (n = 47), n (%) |
SN-ENKTL (n = 211), n (%) |
p(SN-DLBCL vs. SN-ENKTL) |
|---|---|---|---|---|
| Sex | ||||
| Male | 174 (67.4) | 25 (53.2) | 149 (70.6) | 0.021 |
| Female | 84 (32.6) | 22 (46.8) | 62 (29.4) | |
| Age (year) | ||||
| Median (range) | 43 (10–85) | 63 (11–82) | 40 (10–85) | <0.001 |
| ≤60 | 225 (87.2) | 25 (53.2) | 200 (94.8) | |
| >60 | 33 (12.8) | 22 (46.8) | 11 (5.2) | |
| Modified Ann Arbor stage | ||||
| Limited I | 73 (28.3) | 3 (6.4) | 70 (33.2) | 0.001 |
| Extensive I | 126 (48.8) | 32 (68.1) | 94 (44.5) | |
| II | 59 (22.9) | 12 (25.5) | 47 (22.3) | |
| Nodal involvement | ||||
| Present | 49 (19.0) | 10 (21.3) | 39 (18.5) | 0.659 |
| Absent | 209 (81.0) | 37 (78.7) | 172 (81.5) | |
| B symptoms | ||||
| Present | 104 (40.3) | 5 (10.6) | 99 (46.9) | <0.001 |
| Absent | 154 (59.7) | 42 (89.4) | 112 (53.1) | |
| LDH level | ||||
| Normal | 192 (74.4) | 37 (78.7) | 155 (73.5) | 0.514 |
| Elevated | 64 (24.8) | 10 (21.3) | 54 (25.6) | |
| Unknown | 2 (0.8) | 0 (0.0) | 2 (0.9) | |
| ECOG performance status | ||||
| 0 | 141 (54.7) | 25 (53.2) | 116 (55.0) | 0.018 |
| 1 | 94 (36.4) | 13 (27.7) | 81 (38.4) | |
| ≥2 | 23 (8.9) | 9 (19.1) | 14 (6.6) | |
| mIPI | ||||
| 0 | 126 (48.8) | 13 (27.7) | 113 (53.6) | 0.001 |
| 1 | 92 (35.7) | 20 (42.5) | 72 (34.1) | |
| 2–4 | 38 (14.7) | 14 (29.8) | 24 (11.4) | |
| Unknown | 2 (0.8) | 0 (0.0) | 2 (0.9) | |
| Treatment strategy | ||||
| CMT | 147 (57.0) | 37 (78.7) | 110 (52.1) | <0.001 |
| Chemotherapy alone | 17 (6.6) | 10 (21.3) | 7 (3.3) | |
| Radiotherapy alone | 94 (36.4) | 0 (0.0) | 94 (44.6) | |
| Response to treatment | ||||
| CR/CRu | 205 (79.5) | 36 (76.6) | 169 (80.1) | 0.686 |
| PR | 23 (8.9) | 6 (12.7) | 17 (8.1) | |
| SD | 1 (0.4) | 0 (0.0) | 1 (0.5) | |
| PD | 15 (5.8) | 2 (4.3) | 13 (6.2) | |
| Not evaluable | 14 (5.4) | 3 (6.4) | 11 (5.1) | |
SN-DLBCL sinonasal diffuse large B cell lymphoma, SN-ENKTL sinonasal extranodal NK/T cell lymphoma, LDH lactate dehydrogenase, ECOG Eastern Cooperative Oncology Group, mIPI modified International Prognostic Index, CMT combined modality therapy, CR complete response, CRu unconfirmed complete response, PR partial response, SD stable disease, PD progressive disease
The overall response rates (ORR) after completion of therapy were equally high for patients with SN-DLBCL and SN-ENKTL (89.3 vs 88.2%). For patients with SN-DLBCL, the ORR was 94.6% after chemotherapy followed by involved-field radiotherapy (IFRT) and 70% after chemotherapy alone. For patients with SN-ENKTL receiving radiotherapy combined with chemotherapy (combined modality therapy, CMT) and radiotherapy alone, the ORR were 91.8 and 87.2%. In CMT SN-ENKTL patients, the ORR and complete response (CR) rates were both 100% for chemotherapy containing pegaspargase or gemcitabine combined with radiotherapy group. In contrast, the ORR and CR rates were 87.1 and 79.0% for conventional chemotherapy regimens (cyclophosphamide, doxorubicin, vincristine, and prednisone, CHOP/CHOP-like) combined with radiotherapy group. In addition, the ORR was only 42.9% for patients with SN-ENKTL receiving chemotherapy alone which mainly consists of CHOP or CHOP-like regimens.
The treatment outcomes were similar between SN-DLBCL and SN-ENKTL. The 3-year overall survival (OS) and progression-free survival (PFS) rates were 79.7 and 61.4% for SN-DLBCL and 83.6 (p = 0.707) and 70.1% (p = 0.294) for SN-ENKTL, respectively (Fig. 1). Unfavorable Eastern Cooperative Oncology Group (ECOG) performance status (PS) and failure to achieve CR were significantly associated with worse OS and PFS for SN-DLBCL patients (Additional file 2). For patients with SN-ENKTL, factors related to worse OS and PFS included unfavorable modified Ann Arbor stage and failure to achieve CR (Additional file 2). In addition, higher modified International Prognostic Index (mIPI) [5] was significantly associated with worse OS but not significantly associated with worse PFS (Additional file 2).
Fig. 1.
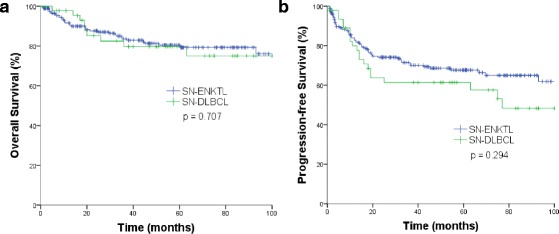
a Overall survival and b progression-free survival for patients with localized sinonasal diffuse large B cell lymphoma (SN-DLBCL, n = 47) and sinonasal extranodal NK/T cell lymphoma (SN-ENKTL, n = 211)
Although a short course of rituximab-CHOP (R-CHOP) chemotherapy followed by IFRT is the recommended treatment option for localized DLBCL, the treatment strategy for SN-DLBCL has seldom been explored because of limited cases. Lee et al. [6] found no significant differences in response rate and OS between patients with SN-DLBCL treated with R-CHOP chemotherapy alone and those treated with R-CHOP chemotherapy followed by IFRT. In our study, some patients were treated with CHOP or CHOP-like regimens without rituximab; the 3-year OS rates were 83.7% for patients receiving chemotherapy followed by IFRT and 62.5% for those receiving chemotherapy alone, but the difference was not significant (p = 0.113, Additional file 3).
Because of their different chemosensitivities, the treatment options for patients with ENKTL differ from those for patients with DLBCL. Currently, the optimal combination treatment modalities for localized SN-ENKTL have not been defined. Treatment options include radiotherapy alone, sequential chemotherapy and radiotherapy, or concurrent chemoradiotherapy [7, 8]. In this study, no significant difference was found in the OS or PFS between radiotherapy alone and CMT for all patients with localized SN-ENKTL (Additional file 4). But in extensive stage I and stage II SN-ENKTL group, CMT could significantly improve the PFS (73.8 vs 50.0%, p = 0.003) compared with radiotherapy alone, and CMT achieved higher 3-year OS rate though the difference was not significant (Additional file 4). In all SN-ENKTL patients receiving the CMT, chemotherapy containing pegaspargase or gemcitabine could achieve higher 3-year OS and PFS rates than conventional CHOP/CHOP-like chemotherapy regimens, but the difference was not significant.
In conclusion, the data from our study revealed that localized SN-DLBCL and SN-ENKTL had different clinical characteristics, but both of these two subtypes could achieve favorable prognoses. These results highlight that the heterogeneity of sinonasal lymphomas and therapeutic approaches should be selected according to the specific subtype and the stage at diagnosis.
Acknowledgements
Not applicable.
Funding
This work was supported in part by the National Key Technology Support Program (2014BAI09B12).
Availability of data and materials
The datasets supporting the conclusions of this article are included within the article and additional files.
Authors’ contributions
YH collected the data, analyzed the data, and wrote the paper. BJ and SYJ collected the data. SYZ, JLY, PL, LG, XHH, YQ, and YS interpreted the data and revised the manuscript. YKS conceived the concept, interpreted the data, and revised the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Cancer Hospital, Chinese Academy of Medical Sciences.
Abbreviations
- CHOP
Cyclophosphamide, doxorubicin, vincristine, and prednisone
- CMT
Combined modality therapy
- CR
Complete response
- CRu
Unconfirmed complete response
- ECOG
Eastern Cooperative Oncology Group
- IFRT
Involved-field radiotherapy
- LDH
Lactate dehydrogenase
- mIPI
Modified International Prognostic Index
- ORR
Overall response rate
- OS
Overall survival
- PD
Progressive disease
- PFS
Progression-free survival
- PR
Partial response
- SD
Stable disease
- SN-DLBCL
Sinonasal diffuse large B cell lymphoma
- SN-ENKTL
Sinonasal extranodal NK/T cell lymphoma
Additional files
Supplemental methods. (DOCX 12 kb)
Univariate analysis of prognostic factors for patients with localized SN-DLBCL and SN-ENKTL. (DOCX 19 kb)
Treatment outcomes for patients with localized SN-DLBCL. (A) Overall survival and (B) progression-free survival of chemotherapy followed by involved-field radiotherapy (IFRT, n = 37) and chemotherapy alone (n = 10). (DOCX 40 kb)
Treatment outcomes for patients with localized SN-ENKTL. (A) Overall survival and (B) progression-free survival for all SN-ENKTL patients (n = 211) treated with combined modality therapy (CMT) and radiotherapy alone. (C) Overall survival and (D) progression-free survival for extensive stage I and stage II SN-ENKTL patients (n = 141) treated with combined modality therapy (CMT) and radiotherapy alone. (DOCX 83 kb)
References
- 1.Sun J, Yang Q, Lu Z, He M, Gao L, Zhu M, et al. Distribution of lymphoid neoplasms in China: analysis of 4,638 cases according to the World Health Organization classification. Am J Clin Pathol. 2012;138(3):429–34. doi: 10.1309/AJCP7YLTQPUSDQ5C. [DOI] [PubMed] [Google Scholar]
- 2.Yang QP, Zhang WY, Yu JB, Zhao S, Xu H, Wang WY, et al. Subtype distribution of lymphomas in Southwest China: analysis of 6,382 cases using WHO classification in a single institution. Diagn Pathol. 2011;6:77. doi: 10.1186/1746-1596-6-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lu NN, Li YX, Wang WH, Jin J, Song YW, Zhou LQ, et al. Clinical behavior and treatment outcome of primary nasal diffuse large B-cell lymphoma. Cancer. 2012;118(6):1593–8. doi: 10.1002/cncr.26452. [DOI] [PubMed] [Google Scholar]
- 4.Dubal PM, Dutta R, Vazquez A, Patel TD, Baredes S, Eloy JA. A comparative population-based analysis of sinonasal diffuse large B-cell and extranodal NK/T-cell lymphomas. Laryngoscope. 2015;125(5):1077–83. doi: 10.1002/lary.25111. [DOI] [PubMed] [Google Scholar]
- 5.Miller TP, Dahlberg S, Cassady JR, Adelstein DJ, Spier CM, Grogan TM, et al. Chemotherapy alone compared with chemotherapy plus radiotherapy for localized intermediate- and high-grade non-Hodgkin’s lymphoma. New England J Med. 1998;339(1):21–6. doi: 10.1056/NEJM199807023390104. [DOI] [PubMed] [Google Scholar]
- 6.Lee GW, Go SI, Kim SH, Hong J, Kim YR, Oh S, et al. Clinical outcome and prognosis of patients with primary sinonasal tract diffuse large B-cell lymphoma treated with rituximab-cyclophosphamide, doxorubicin, vincristine and prednisone chemotherapy: a study by the Consortium for Improving Survival of Lymphoma. Leuk Lymphoma. 2015;56(4):1020–6. doi: 10.3109/10428194.2014.946027. [DOI] [PubMed] [Google Scholar]
- 7.Lin N, Song Y, Zheng W, Tu M, Xie Y, Wang X, et al. A prospective phase II study of L-asparaginase- CHOP plus radiation in newly diagnosed extranodal NK/T-cell lymphoma, nasal type. J Hematol Oncol. 2013;6:44. doi: 10.1186/1756-8722-6-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tse E, Kwong YL. How I treat NK/T-cell lymphomas. Blood. 2013;121(25):4997–5005. doi: 10.1182/blood-2013-01-453233. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets supporting the conclusions of this article are included within the article and additional files.