

Abstract
The reduction in blood pressure after the physical exercise practice is called postexercise hypotension (PEH). Previous studies have demonstrated that the ingestion of caffeine at levels corresponding to three doses of coffee eliminates this phenomenon. Thus, we evaluated the influence of different doses of coffee in the PEH in twelve hypertensives, who performed four experimental sessions of aerobic exercise on a cycle ergometer (lasting 40 minutes, with intensity between 60% and 80% of maximum heart rate), followed by the ingestion of one (CAF-1), two (CAF-2), or three (CAF-3) doses of caffeinated coffee, or three doses of decaffeinated coffee (DESC). The blood pressure was measured at rest and at 10-minute intervals during 120 minutes of recovery post exercise. DESC resulted in systolic PEH at all moments of measurement, with averages of -4.1±1.2 mmHg and -1.8±1.3 mmHg on the 1st and 2nd hours post exercise, respectively. In CAF-1, both systolic hypotensive and hypertensive responses to the exercise were identified, with averages of -1.2±1.7 and 0.5±0.4 mmHg after one and two hours of recovery. Conversely, hypertensive systolic response occurred in all measurements compared rest blood pressure. The 1st and 2nd hours post exercise was 4.5±1.1 and 6.5+1.1 mmHg in CAF-2 and 5.1+0.9 and 6.5+1.0 mmHg to CAF-3. Diastolic PEH was not found in any of the experimental sessions. Therefore, the ingestion of two and three doses of caffeinated coffee completely blunts the PEH, while one dose results in partial elimination of the PEH.
Keywords: Coffee, exercise, hypertension, post-exercise hypotension
Introduction
Coffee is a widely consumed beverage on a daily basis, second only to water in the United Sates [1]. Its consumption, however, has been correlated to the development of cardiovascular events, such as cerebrovascular accident, stroke, coronary diseases [2-4], and rise in blood pressure (BP) [5-7].
Caffeine, the main methylxanthine found in coffee, is the substance that accounts for the rise in blood pressure [6-10]. Studies have demonstrated that the administration of 250 mg of caffeine promoted mean elevations of 12.6 and 7.1 mmHg in systolic (SBP) and diastolic blood pressure (DBP), respectively, in volunteers who are not habituated to coffee consumption [2], and mean rises of 9 and 4 mmHg in SBP and DBP among those who are [10].
It has also been evidenced that one single bout of physical exercise is able to lower the blood pressure levels, when compared to the baseline or to volunteers submitted to a control session [11,12]. This phenomenon is called postexercise hypotension (PEH) and, under proper conditions, becomes beneficial to normotensive and hypertensive individuals. The latter, whether or not in use of antihypertensive medications, have been shown to benefit from the physical exercise practice and specifically from the PEH, which might enable drug dosage reduction or even elimination, thus reducing costs and side effects related to the treatment of hypertension [12].
However, this exercise-induced blood pressure response is also influenced by caffeine ingestion, as demonstrated by studies [13,14] in which the intravenous or oral administration of 4 mg of caffeine per kilogram of body weight (equivalent to three doses of coffee) blunted the PEH. More recent studies carried out in our laboratory, with the administration of three oral doses of coffee have produced similar effects, corroborating those author’s findings [15].
Nevertheless, it remained unclear whether volumes lower than 4 mg of caffeine per kilogram of body weight or three doses of coffee would also be able to bring about the elimination of the PEH, thus resulting in the loss of its protective effects in hypertensive subjects. Therefore, the aim of this study was to analyze the influence of different volumes of coffee, with their respective contents of caffeine, on the blood pressure response to exercise practice in hypertensives habituated to drinking this beverage.
Materials and methods
Volunteers
Twelve volunteers classified as hypertensive participated in the study, belonging to both genders (three men), from 40 to 55 years old, overweight, who had gone jogging regularly for at least three months. They were habituated to coffee consumption, under treatment with antihypertensive medication belonging to the class of beta-adrenergic receptor blockers, thiazide-type diuretics and angiotensin-converting enzyme inhibitors, and presented systolic and diastolic blood pressure values under control. Of the twelve volunteers, initially selected to take part in the study, four gave up along the experimental sessions because of insomnia, which was due to the ingestion of coffee during the experimental sessions, and migraine resulting from the period without the coffee ingestion. This study has been previously approved by the Human Research Ethics Committee at Lauro Wanderley Hospital, at Federal University of Paraíba, with protocol number 21/2011. All volunteers were previously notified about the experimental procedures and signed the written informed consent according to resolution 466/12 of National Health Council (Brazil).
Study design
The study was a clinical trial registered on ClinicalTrials.org and assigned the identifier number NCT02335840. The volunteers were asked to avoid consumption of any caffeinated food or drink for 48 hours prior to the experimental sessions. They performed four experimental sessions with the practice of physical exercise, as described below, followed by the ingestion of caffeinated or decaffeinated coffee, according to the following protocols: 1) one dose of 150 ml of coffee (144 mg of caffeine) ingested 10 minutes post exercise (CAF-1); 2) two doses of 150 ml of coffee (2×144 mg of caffeine) ingested 10 and 20 minutes post exercise (CAF-2); 3) three doses of 150 ml of coffee (3×144 mg of caffeine) ingested 10, 20, and 30 minutes post exercise (CAF-3); 4) three doses of 150 ml of decaffeinated coffee (108 mg of caffeine) ingested 10, 20, and 30 minutes post exercise (DESC). They remained seated during 120 minutes after the practice of physical exercise. Blood pressure was evaluated at rest, and during the 120 minutes of postexercise recovery, being measured every 10 minutes.
Coffee preparation and ingestion
The study utilized caffeinated and decaffeinated coffee from the same manufacturer (São Braz, Cabedelo, Brazil) with products of the same category acquired with the same serial number. Caffeinated and decaffeinated coffee had 1.2% and 0.3% of caffeine, respectively, in its composition. The method adopted in the preparation of caffeinated or decaffeinated coffee was previously utilized in another study [15]. Both types were prepared with the addition of 40 g coffee powder to each 500 ml of water heated for five minutes, limited by the beginning of boiling. This way, the volume of 500 ml of coffee contained 432 mg of caffeine. Each cup to be ingested had a volume of 150 ml, so that one, two, and three cups with caffeinated coffee had, respectively, 144 mg, 288 mg, and 432 mg of caffeine, whereas three cups of decaffeinated coffee contained 108 mg of caffeine. The doses of caffeinated or decaffeinated coffee were sweetened with sugar (Alegre, Mamanguape, Brazil). The coffee was strained with paper filters (Mellita®, Minden, Germany). A dosing glass, previously calibrated to have the volume of one cup (150 ml), was used to ensure the accuracy of the volume ingested by the volunteers.
The experimental sessions had their sequence randomly determined through the site www.randomizer.org. The ingestion of coffee occurred within the first 30 minutes of the period of recovery, at 10-minute intervals. During the ingestion, volunteers were seated and a deadline of five minutes was stipulated for the coffee consumption.
Physical exercise protocol
Volunteers performed four experimental sessions with aerobic exercise which lasted 40 minutes, on a stationary bicycle (Perform V3, Movement®, Pompeia, São Paulo), with an intensity between 60% and 80% of maximum heart rate (MHR). Previously established protocols [16,17] were adopted to perform the MHR estimate [16] and the prescription of the exercise target zone [17]. Heart rate was evaluated at rest and during the exercise with the use of a frequency meter (RS800CX, Polar Electro® Oy, Kempele, Finland).
Blood pressure measurement
After the volunteers arrived at the laboratory, they were oriented to remain at rest and seated for a 10-minute period prior to the measurement of the baseline blood pressure. Additional measurements of blood pressure were performed during the 120 minutes of post-exercise recovery, every 10 minutes. During the first 30 minutes of post-exercise recovery, blood pressure was measured one minute before the administration of each dose with caffeinated or decaffeinated coffee. The auscultatory method [18] was adopted to measure blood pressure, with use of a sphygmomanometer (Missouri, Embu, Brazil), which was previously calibrated against a mercury column, and also a stethoscope (Missouri, Embu, Brazil).
Statistical analysis
The data is presented as mean ± standard error of the mean. All variables were tested for normal distribution using Shapiro-Wilk and Levene’s tests. For the comparisons of heart rate, systolic and diastolic blood pressure at rest among the experimental sessions, a One-way ANOVA was conducted. For comparisons of systolic and diastolic responses among experimental sessions, repeated-measures ANOVA or the equivalent nonparametric tests were performed, when necessary. The p-value was set at 0.05. The analysis was carried out using GraphPad Prism software version 3.06 (GraphPad Software, San Diego, CA).
Results
The volunteers were middle-aged, overweight adults, who had been previously diagnosed as hypertensive, but had their blood pressure values kept under control (Table 1), in compliance with clinical blood pressure values previously established [18]. It is important to emphasize that, for all the analyzed variables, baseline values were not considerably different between the sessions.
Table 1.
Baseline characteristics of the hypertensives
| DESC | CAF-1 | CAF-2 | CAF-3 | |
|---|---|---|---|---|
| Age (years) | 54±1.1 | |||
| BMI (Kg/m2) | 28±1.2 | |||
| RHR (bpm) | 80.6±2.9 | 78.5±3.1 | 85.3±2.7 | 82.4±2.9 |
| RSBP (mmHg) | 122.7±3.9 | 126.6±3.3 | 125.7±4.2 | 118.6±4.4 |
| RDBP (mmHg) | 75.3±2.7 | 75.3±2.8 | 74.1±2.8 | 76.1±2.5 |
Data on mean ± standard error. DESC = decaffeinated (108 mg of caffeine); CAF-1: one dose of 150 ml of coffee (144 mg of caffeine); CAF-2: two doses of 150 ml of coffee (2×144 mg of caffeine); CAF-3: three doses of 150 ml of coffee (3×144 ml of caffeine); BMI = body mass index; RHR = resting heart rate; RSBP = resting systolic blood pressure; RDBP = resting diastolic blood pressure. There are no significant differences between the experimental sessions (One-way ANOVA).
The sessions DESC, CAF-1, CAF-2 and CAF-3 were effective in elevating the heart rate compared to rest (Figure 1), but no significant difference was observed between the procedures at the moments of heart rate measurement (p>0.05). Volunteers practiced the exercise with index of subjective perception of effort matching the standard established as a moderate intensity (from 11 to 14), and without significant differences between the experimental sessions (Figure 2).
Figure 1.
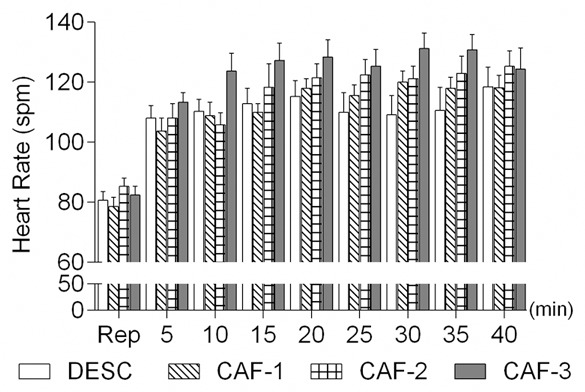
Heart rate at rest and during the exercise sessions. DESC = decaffeinated (108 mg of caffeine); CAF-1: one dose of 150 ml of coffee (144 mg of caffeine); CAF-2: two doses of 150 ml of coffee (2×144 mg of caffeine); CAF-3: three doses of 150 ml of coffee (3×144 ml of caffeine). Data are mean ± standard error. There are no significant differences between experimental sessions (Repeated measures ANOVA).
Figure 2.
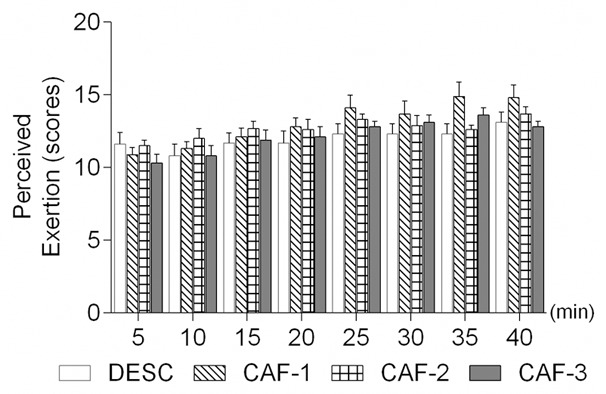
Perceived exertion during the exercise sessions. DESC = decaffeinated (108 mg of caffeine); CAF-1: one dose of 150 ml of coffee (144 mg of caffeine); CAF-2: two doses of 150 ml of coffee (2×144 mg of caffeine); CAF-3: three doses of 150 ml of coffee (3×144 ml of caffeine). Data are mean ± standard error. There are no significant differences between experimental sessions (Repeated measures ANOVA).
Exercise inducing systolic PEH was observed only in DESC session (all moments of post exercise measurement) at some moments in CAF-1 (Table 2). On the contrary, CAF-2 and CAF-3 promoted hypertensive behavior in all 12 measures obtained during the 120-minute recovery period after the exercise (except for one moment, at 20 minutes of recovery in CAF-2).
Table 2.
Absolute differences between the values of postexercise blood pressure and blood pressure at rest
| Delta systolic blood pressure | ||||
|
| ||||
| Moments of measurement | DESC | CAF-1 | CAF-2 | CAF-3 |
|
| ||||
| 10 | -6.6±2.0 | -7.0±2.3 | 2.0±2.5*,# | 4.7±4.6*,# |
| 20 | -1.3±2.0 | -6.0±3.3 | 1.0±2.2 | 3.1±3.7# |
| 30 | -6.3±2.0 | 0.0±3.8* | 7.0±2.5* | 2.0±3.5* |
| 40 | -7.5±4.0 | 1.0±2.5 | 8.0±2.3* | 6.5±3.4* |
| 50 | -2.0±5.0 | 2.0±4.7 | 5.0±2.9* | 6.4±4.4* |
| 60 | -1.1±3.0 | 3.0±3.8 | 4.0±3.0 | 7.7±5.2* |
| 70 | -6.0±3.0 | 0.0±3.7 | 2.0±3.9* | 2.9±5.1* |
| 80 | -1.4±3.0 | 0.0±3.3 | 8.0±1.4* | 7.0±3.4* |
| 90 | -4.9±2.0 | -1.0±3.8 | 5.0±3.5* | 5.8±4.3* |
| 100 | 1.1±5.0 | 1.0±3.7 | 9.0±2.6 | 9.6±4.8# |
| 110 | -1.3±4.0 | 2.0±4.2 | 8.0±3.4* | 5.4±4.5 |
| 120 | 2.0±5.0 | 1.0±4.2 | 7.0±3.2 | 8.4±3.4 |
| Mean in the 1st hour | -4.1±1.2 | -1.2±1.7 | 4.5±1.1*,# | 5.1±0.9*,# |
| Mean in the 2nd hour | -1.8±1.3 | 0.5±0.4 | 6.5±1.1*,# | 6.5±1.0*,# |
|
| ||||
| Delta diastolic blood pressure | ||||
|
| ||||
| 10 | -3.2±2.2 | 5.8±2.0* | 2.0±1.2 | 0.6±2.5 |
| 20 | 2.2±2.8 | 3.9±2.0 | 1.0±1.9 | 1.3±2.9 |
| 30 | 0.4±4.2 | 3.7±2.0 | 6.0±2.8 | 2.1±4.1 |
| 40 | 0.6±2.5 | 3.1±3.0 | 4.0±2.3 | 3.3±3.1 |
| 50 | 4.4±3.4 | 4.0±3.0 | 5.0±0.9 | 6.2±3.8 |
| 60 | 3.9±2.3 | 2.8±3.0 | 9.0±2.2 | 4.7±3.1 |
| 70 | 4.1±2.9 | 6.0±3.0 | 6.0±1.5 | 3.4±3.0 |
| 80 | 6.6±2.9 | 3.9±3.0 | 9.0±1.8 | 5.8±3.2 |
| 90 | 6.2±3.1 | 5.1±3.0 | 11.0±1.1 | 5.2±3.6 |
| 100 | 8.9±2.8 | 6.4±3.0 | 5.0±2.2 | 7.2±3.7 |
| 110 | 10.8±2.7 | 4.8±3.0 | 6.0±1.8 | 5.8±4.4 |
| 120 | 14±1.7 | 7.7±2.0 | 7.0±1.6 | 4.2±2.8 |
| Mean in the 1st hour | 1.4±1.1 | 3.9±0.4 | 4.5±1.2 | 3.0±0.9 |
| Mean in the 2nd hour | 8.4±1.5& | 5.7±0.5 | 7.3±0.9 | 5.3±0.5 |
Data on mean ± standard error. DESC = decaffeinated (108 mg of caffeine); CAF-1: one dose of 150 ml of coffee (144 mg of caffeine); CAF-2: two doses of 150 ml of coffee (2×144 mg of caffeine); CAF-3: three doses of 150 ml of coffee (3×144 ml of caffeine)
Significant difference with the session DESC (P<0,05);
Significant difference with the session CAF-1 (P<0.05);
Significant difference between 1st and 2nd hour (P<0.05).
Repeated measures ANOVA.
The presence of diastolic hypotensive response was only observed in measures obtained at 10, 20, and 40 minutes of recovery in session DESC. Conversely, a descriptive hypertensive diastolic response occurred at all the moments of blood pressure measurement in sessions CAF-1, CAF-2, and CAF-3. However, statistical significance was only verified during 10 minutes of recovery, when compared to CAF-1 and DESC (Table 2).
Discussion
The data of this study demonstrates that ingesting one dose of coffee of 150 ml (144 mg of caffeine) descriptively blunts the systolic PEH, whereas two and three doses promote significant hypertensive responses after one single bout of aerobic exercise, in relation to pre-exercise values. On the other hand, the diastolic component response was not significantly modified.
The influence of the ingestion of caffeine or coffee on the limitation of blood pressure reduction after the exercise has been previously evidenced [13-15]. However, in these previous studies, the caffeine was administered using intravenous [13] or oral routes [14]. Though these two procedures have considerable metodological value, its practical application is difficult, considering that few people use caffeine as an ergogenic aid, and its intake occurs mainly through coffee or caffeinated drinks or foods. This beverage has in its composition, besides the caffeine, antioxidants substances [19,20] that can promote some vasodilator effect, in opposition to the vasoconstrictor effect brought about by caffeine.
Despite this, researches conducted similarly to this study [15] have suggested a more prominent hypertensive effect observed post exercise. However, the authors adopted three doses of coffee, equivalent to 450 mg of caffeine, a concentration that is unusual to be ingestevd, considering that previous recommendations [21] indicate the intake of caffeine ranging from 150 to 200 mg per day, which is equivalent to the caffeine concentrations used in our study.
From the perspective that the present study corroborates the data supporting that the ingestion of coffee abolishes the post-exercise hypotension, all the previous studies were carried out with doses of 150 ml of coffee ingested within a short period of time before or after the exercise practice. Thus, until the present study, it was unclear whether smaller doses would be recommended to hypertensives who practice physical exercise.
The data in this study showed that volumes smaller than one dose of 150 ml of coffee, containing 144 mg caffeine, blunts the reduction in blood pressure after the aerobic exercise, while two or three doses not only abolish the PEH, but promote a post-exercise hypertensive response as well.
The practical recommendation of this study is to inform hypertensives who regularly practice physical exercise that they should avoid the ingestion of coffee within the first hours post exercise. However, we must consider in the protocol of the present study, there was a 48-hour washout period for caffeinated drinks and foods, and this may have promoted resensitization of adenosine receptors A2A, which participate in the mechanisms proposed to explain the hypertensive response to caffeine [22]. Thus, the habitual daily intake can reduce the sensibility of these receptors and the hypertensive response demonstrated in this study. It was demonstrated [23] that the ingestion of eight doses of coffee/day, for a month, by healthy young people who remained under resting conditions, was only able to elevate the blood pressure during the first five days of ingestion, without hypertensive response in the last three weeks of study.
Although the presence of diastolic PEH in our study corroborates the previous data [15], we must consider that the absence of this effect might have occurred due to the control session with decaffeinated coffee. The amount of caffeine present in the three doses of decaffeinated coffee (108 mg of caffeine) was similar to the observed in a caffeinated dose (144 mg caffeine), which might explain the absence of PEH in procedures with decaffeinated coffee. As a result, it was not possible to test the hypothesis that doses of coffee abolished the PEH that was inexistent. Previous studies [24,25] verifyed that the intake of 25 and 50 ml of decaffeinated coffee (with five and 10 mg of caffeine, respectively), by volunteers at rest, did not promote modification in the systolic and diastolic components of blood pressure.
Considering this was the main limitation of the present study, we suggest that further investigations adopt, as concentration of caffeine for the placebo with decaffeinated coffee, something similar to that used by these same studies [24,25]. Finally, we believe that other limiting factor of our results was the adoption of standardized doses of coffee, administrated without taking into account the body weight. However, our investigation aimed at maintaining a good external validity, with the understanding that people do not control the volume of coffee they drink according to their body weight. Considering that there was no significant variation of physical weight among the volunteers in the present study, we hypothetize that, even though this fact represents a limiting factor, it has not resulted in biased results.
Finally, it is known that caffeine has a plasma half-life ranging from two and a half to four and a half hours [26]. This way, whether the blunt of the PEH lasts for more than 120 minutes after the physical exercise is something that cannot be determined in this study and represents other recommendation for further studies.
In summary, considering previous data indicating that the ingestion of three doses of 150 ml of coffee, or 432 mg of caffeine, abolishes the post-exercise hypotension, this study demonstrated that doses smaller than 150 ml of coffee or 144 mg of caffeine, equivalent to the volume in a cup of coffee regularly used by the population, is sufficient to eliminate the systolic PEH, whereas two or three doses still promote a hypertensive response during the first two hours post exercise.
Disclosure of conflict of interest
None.
References
- 1.O’Keefe JH, Bhatti SK, Patil HR, DiNicolantonio JJ, Lucan SC, Lavie CJ. Effects of habitual coffee consumption on cardiometabolic disease, cardiovascular health, and all-cause mortality. J Am Coll Cardiol. 2013;62:1043–1051. doi: 10.1016/j.jacc.2013.06.035. [DOI] [PubMed] [Google Scholar]
- 2.Corti R, Binggeli C, Sudano I, Spieker L, Hanseler E, Ruschitzka F, Chaplin WF, Luscher TF, Noll G. Coffee acutely increases sympathetic nerve activity and blood pressure independently of caffeine content: role of habitual versus nonhabitual drinking. Circulation. 2002;106:2935–2940. doi: 10.1161/01.cir.0000046228.97025.3a. [DOI] [PubMed] [Google Scholar]
- 3.Hammar N, Andersson T, Alfredsson L, Reuterwall C, Nilsson T, Hallqvist J, Knutsson A, Ahlbom A SHEEP and the VHEEP study. Association of boiled and filtered coffee with incidence of first nonfatal myocardial infarction: the SHEEP and the VHEEP study. J Intern Med. 2003;253:653–659. doi: 10.1046/j.1365-2796.2003.01142.x. [DOI] [PubMed] [Google Scholar]
- 4.Mostofsky E, Schlaug G, Mukamal KJ, Rosamond WD, Mittleman MA. Coffee and acute ischemic stroke onset: the Stroke Onset Study. Neurology. 2010;75:1583–1588. doi: 10.1212/WNL.0b013e3181fb443d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lane JD, Pieper CF, Phillips-Bute BG, Bryant JE, Kuhn CM. Caffeine affects cardiovascular and neuroendocrine activation at work and home. Psychosom Med. 2002;64:595–603. doi: 10.1097/01.psy.0000021946.90613.db. [DOI] [PubMed] [Google Scholar]
- 6.McMullen MK, Whitehouse JM, Shine G, Towell A. Habitual coffee and tea drinkers experienced increases in blood pressure after consuming low to moderate doses of caffeine; these increases were larger upright than in the supine posture. Food Funct. 2011;2:197–203. doi: 10.1039/c0fo00166j. [DOI] [PubMed] [Google Scholar]
- 7.Papaioannou TG, Vlachopoulos C, Ioakeimidis N, Alexopoulos N, Stefanadis C. Nonlinear dynamics of blood pressure variability after caffeine consumption. Clin Med Res. 2006;4:114–118. doi: 10.3121/cmr.4.2.114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Funatsu K, Yamashita T, Nakamura H. Effect of coffee intake on blood pressure in male habitual alcohol drinkers. Hypertens Res. 2005;28:521–527. doi: 10.1291/hypres.28.521. [DOI] [PubMed] [Google Scholar]
- 9.Rakic V, Burke V, Beilin LJ. Effects of coffee on ambulatory blood pressure in older men and women: A randomized controlled trial. Hypertension. 1999;33:869–873. doi: 10.1161/01.hyp.33.3.869. [DOI] [PubMed] [Google Scholar]
- 10.Sudano I, Spieker L, Binggeli C, Ruschitzka F, Luscher TF, Noll G, Corti R. Coffee blunts mental stress-induced blood pressure increase in habitual but not in nonhabitual coffee drinkers. Hypertension. 2005;46:521–526. doi: 10.1161/01.HYP.0000177448.56745.c7. [DOI] [PubMed] [Google Scholar]
- 11.Rondon MUPB, Brum PC. Exercício físico como tratamento não-farmacológico da hipertensão arterial. Rev Bras Hipertens. 2003;10:134–139. [Google Scholar]
- 12.Laterza MC, Rondon MU, Negrão CE. Efeito anti-hipertensivo do exercício. Rev Bras Hipertens. 2007;14:104–111. [Google Scholar]
- 13.Notarius CF, Morris BL, Floras JS. Caffeine attenuates early post-exercise hypotension in middle-aged subjects. Am J Hypertens. 2006;19:184–188. doi: 10.1016/j.amjhyper.2005.07.022. [DOI] [PubMed] [Google Scholar]
- 14.Cazé RF, Franco GA, Porpino SK, Souza AA, Padilhas OP, Silva AS. Influência da cafeína na resposta pressórica ao exercício aeróbio em sujeitos hipertensos. Rev Bras Med Esporte. 2010;16:324–328. [Google Scholar]
- 15.Nobrega TKS, Moura Júnior JS, Alves NFB, Santos AC, Silva AS. A Ingestão de café abole a hipotensão induzida por exercício aeróbio: um estudo piloto. Rev Educ Fís/UEM. 2011;22:601–612. [Google Scholar]
- 16.Bruce RA, Fisher LD, Cooper MN, Gey GO. Separation of effects of cardiovascular disease and age on ventricular function with maximal exercise. Am J Cardiol. 1974;34:757–763. doi: 10.1016/0002-9149(74)90692-4. [DOI] [PubMed] [Google Scholar]
- 17.Karvonen MJ, Kentala E, Mustala O. The effects of training on heart rate; a longitudinal study. Ann Med Exp Biol Fenn. 1957;35:307–315. [PubMed] [Google Scholar]
- 18.Sociedade Brasileira de Cardiologia; Sociedade Brasileira de Hipertensão; Sociedade Brasileira de Nefrologia. [VI Brazilian Guidelines on Hypertension] . Arq Bras Cardiol. 2010;95:1–51. [PubMed] [Google Scholar]
- 19.Ochiai R, Chikama A, Kataoka K, Tokimitsu I, Maekawa Y, Ohishi M, Rakugi H, Mikami H. Effects of hydroxyhydroquinone-reduced coffee on vasoreactivity and blood pressure. Hypertens Res. 2009;32:969–974. doi: 10.1038/hr.2009.132. [DOI] [PubMed] [Google Scholar]
- 20.Watanabe T, Arai Y, Mitsui Y, Kusaura T, Okawa W, Kajihara Y, Saito I. The blood pressure-lowering effect and safety of chlorogenic acid from green coffee bean extract in essential hypertension. Clin Exp Hypertens. 2006;28:439–449. doi: 10.1080/10641960600798655. [DOI] [PubMed] [Google Scholar]
- 21.Ostchega Y, Hughes JP, Terry A, Fakhouri TH, Miller I. Abdominal obesity, body mass index, and hypertension in US adults: NHANES 2007-2010. Am J Hypertens. 2012;25:1271–1278. doi: 10.1038/ajh.2012.120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ralevic V, Burnstock G. Receptors forpurines and pyrimidines. Pharmacol Rev. 1998;50:413–492. [PubMed] [Google Scholar]
- 23.Ammon HP, Bieck PR, Mandalaz D, Verspohl EJ. Adaptation of blood pressure to continuous heavy coffee drinking in young volunteers. A double-blind crossover study. Br J Clin Pharmacol. 1983;15:701–706. doi: 10.1111/j.1365-2125.1983.tb01553.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Buscemi S, Verga S, Batsis JA, Donatelli M, Tranchina MR, Belmonte S, Mattina A, Re A, Cerasola G. Acute effects of coffee on endothelial function in healthy subjects. Eur J Clin Nutr. 2010;64:483–489. doi: 10.1038/ejcn.2010.9. [DOI] [PubMed] [Google Scholar]
- 25.Buscemi S, Verga S, Batsis JA, Tranchina MR, Belmonte S, Mattina A, Re A, Rizzo R, Cerasola G. Dose-dependent effects of decaffeinated coffee on endothelial function in healthy subjects. Eur J Clin Nutr. 2009;63:1200–1205. doi: 10.1038/ejcn.2009.51. [DOI] [PubMed] [Google Scholar]
- 26.Knutti R, Rothweiler H, Schlatter C. The effect of pregnancy on the pharmacokinects of caffeine. Arc Toxicol Suppl. 1982;5:187–192. doi: 10.1007/978-3-642-68511-8_33. [DOI] [PubMed] [Google Scholar]