

ABSTRACT
Background:
Anxiety among patients after surgery can affect their physiological and psychological well-being. The aim of this study was to investigate and compare the effects of Benson’s relaxation and rhythmic breathing techniques on postoperative anxiety in candidates for the mastectomy surgery.
Methods:
This randomized controlled clinical trial study was conducted with ninety patients in 2013. The patients were hospitalized for the mastectomy surgery in three surgical wards in a teaching hospital, Tehran, Iran. They were randomly assigned into three groups: Benson’s relaxation including the cognitive relaxation technique type, rhythmic breathing including the somatic relaxation technique type and control groups. According to the Davidson and Schwartz multi-process theory, the Benson’s relaxation and the rhythmic breathing techniques have cognitive and somatic effects, respectively. One day before the surgery, the patients in the intervention groups were trained regarding relaxation and breathing techniques and were asked to perform the techniques under the supervision of the researcher in the night before the surgery. The cognitive somatic anxiety questionnaire was used to measure anxiety before the intervention and half an hour after recovery of consciousness after the surgery. Descriptive and inferential statistics were used for data analysis via the SPSS v.21 software.
Results:
There were no statistically significant differences between the groups in terms of demographic characteristics. The application of both techniques reduced the level of patients’ anxiety after the surgery. The patients in the Benson’s relaxation technique group reported only the relief of somatic anxiety. However, the breathing technique patients reported a reduction in both cognitive and somatic anxiety.
Conclusion:
The Benson’s relaxation and rhythmic breathing techniques can reduce postoperative anxiety in patients after the mastectomy surgery.
Trial Registration Number: IRCT2014042017350N1
KEYWORDS: Anxiety, Breast cancer, Relaxation, Mastectomy
INTRODUCTION
Cancer is a major public health concern in the USA and other countries across the world. One in four deaths in the USA is caused due to cancer.1 Breast cancer is the most common invasive cancer among women and accounts for 22.9 percent of all diseases in the world.2 Of 1.40 million women diagnosed with cancer over the world,3 86.4 percent live in developed countries and 27.3 percent are the inhabitants of developing countries. It has been reported that breast cancer accounts for 23 percent of all cancers in Iranian women.4 Breast cancer is the most prevalent type of cancer in Iranian women (Acceleration Skid Regulation 28.25). Since 2010, 7822 cases of breast cancer is diagnosed in Iran. With regard to the provincial distribution of this disease in Iran, 2088 (26.6%) cases were in Tehran, 643 (8.2%) in Isfahan, 599 (7.6%) in Fars, 528 (6.7%) in Khorasan-e-Razavi and 529 (6.7%) in Khuzestan.5 Nowadays, patients have better prognoses and longer disease-free survival rates and can maintain their long-term physical and mental health due to advancements in the diagnosis and treatment of breast cancer.22 At the end of the 19th century, William Halsted described radical mastectomy as the standard method of treatment for women with all stages of breast cancer.6
It is well documented that hospitalization for surgery is associated with the increase of the patient’s anxiety.7 The negative consequences of the cancer diagnosis and cancer-related treatments, 20-30 percent of patients with breast cancer suffer from depression and anxiety. This is significantly higher than the corresponding prevalence of depression and anxiety 6-8 percent in a population of healthy women.8 The incidence of postoperative anxiety have been reported 11-80 percent in adult patients, which can be attributed to the course and outcomes of surgical treatments.9 The symptoms of depression and anxiety can persist for several years.10
The reduction of the patient’s anxiety is a postoperative nursing goal. The improvement of anxiety and depression in female patients with breast cancer needs interventions such as music therapy,11-13 relaxation training,14-16 exercise,17-19 cognitive-behavioural nursing intervention,9,20,21 laughter therapy,22 melatonin, acupressure and meditation.23-25 These interventions have been used as the one-pronged strategy, which were varied considerably in terms of the methodology, sample size and settings. Two or more interventions with similar effects have been rarely used simultaneously in the same sample of female patients with breast cancer.26 According to evidence, the strategies used in the postoperative setting to relieve the patient’s anxiety must be practical and evidenced-based.27 Relaxation techniques are commonly used by physical and mental therapist and in the various areas of psychological practice two particular methods that are widely used in clinical settings are the Benson’s relaxation and rhythmic breathing techniques.28
The Benson’s relaxation method is based on the Benson’s suggestion with four common elements including elicitations, a comfortable position, an object to dwell on such as the repetition of a word, which attracts one’s attention and helps clear the mind of distracting thoughts and a passive attitude. It not only includes empting all other thoughts from one’s mind, but also allow the person to pass on, while returning to one’s previous thoughts.
A wide variety of rhythmic breathing techniques have been proposed to induce relaxation such as slow breathing, deep breathing, breathing meditation and abdominal breathing,29. However, the general procedure used during rhythmic breathing is consisted of sitting in a comfortable position in a quiet room, closing the eyes, relaxing muscles from the bottom to the top, becoming aware of breathing and using a repeated word or phrase to notice the pattern and regulatory of breathing.30
The multi-process theory is an important model for explaining relaxation. Davidson and Schwartz described the effects of relaxation such as somatic, cognitive and intentional. The somatic response to a relaxation technique refers to the effect on physiological parameters including respiration and heart rates. The multi-process theory incorporates a ‘specific-effects’ hypothesis suggesting that relaxation techniques have different effects depending on the relative cognitive and somatic components involved in each technique.31
The multi-process theory predicts that the Benson’s relaxation procedure is a cognitive technique, as it primarily focuses on the attention on the control of cognitive activities through regulating breathing.8 According to Payne (2005), rhythmic breathing is one the methods of somatic techniques, primarily affecting somatic anxiety. The importance of this distinction lies in the desire by practitioners to provide treatment approaches that are evidence-based where possible and that best match the symptoms of their patients. For example, if a patient needs to reduce somatic anxiety, he/she can be taught a somatic based relaxation technique, while a patient prefers to reduce cognitive anxiety, he/she can be instructed to use a cognitive based technique.9
Davidson and Schwartz have suggested a psychobiological analysis of anxiety that emphasizes the pattern of multiple processes in the generation and self-regulation of state anxiety.11 Therefore, it is important to define state anxiety and its components. State anxiety is referred to “…subjective, consciously perceived feelings of apprehension and tension, accompanied by or associated with activation or arousal of the autonomic nervous system”.32 Anxiety has both cognitive and somatic components. Cognitive anxiety is described as” the mental component of anxiety and is caused by negative expectations about success or by negative self-evaluation ” Somatic anxiety refers to “the physiological and effective elements of the anxiety experience that is developed directly from autonomic arousal” .29
The aim of this study was to investigate and compare the effects of Benson’s relaxation and rhythmic breathing techniques on postoperative anxiety in candidates for the mastectomy surgery.
MATERIALS AND METHODS
This randomized controlled clinical trial study was approved by the ethics committee affiliated with Tehran University of Medical Sciences, Tehran, Iran and was registered in the Iranian registry of clinical trial (IRCT) at the www.irct.ir (registered number: IRCT2014042017350N1).
Before the interventions, all the participants were provided with information about the study’s aim and method. They were also reassured about the voluntary nature of the study and confidentiality of their information. Next, the written informed consent form was signed by those patients who willingly agreed to take part in this study.
For this study, 28 patients were required to be recruited in each group so that a medium effect size of 30 could be achieved. A three-sample t-test was performed at a 95% confidence interval and a significance level of 0.05. Given the probability of the samples’ dropout rate, 30 patients were recruited in each group. Since none of the patients withdrew from the study, 90 patients were selected using a convenient sampling method of those patients who were hospitalized one day prior to the elective mastectomy surgery.
Inclusion criteria were: aged 20-60 years, without any psychological and hearing, musculoskeletal and respiratory disorders and having no history of substance abuse.
The patients were assigned into a control group and two intervention groups of the Benson’s relaxation and rhythmic breathing techniques using the table of random numbers. The first two months of the study were spent to the allocation of the samples to the control group and the second two months to the allocation of the patients to the Benson’s relaxation and rhythmic breathing techniques groups. Two weeks after the discharge of the latest patients in the previous group, the recruitment of samples for the next group was started. The recruitment of the samples was performed from October 2013 to April 2014.
Exclusion criteria were unwillingness to continue participation in the study, no cooperation and failure to fill out questionnaires during the study and death during the surgery. Power analysis indicated that this sample size was sufficient to detect the effects of the interventions with a power of 90 percent with the standard error of 0.5.
The patients were randomly allocated into three groups (30 patients in each group): the Benson’s relaxation technique, rhythmic breathing technique and control groups.
One day before the mastectomy surgery, in the morning work shift, a quiet and private environment was provided. The researcher taught the patients individually regarding the techniques and asked them to follow them for 20 minutes twice in the evening and two hours later under the supervision of the researcher. The control group did not receive any type of intervention and only filled out cognitive and somatic anxiety questionnaire before the mastectomy surgery and soon after recovery after the surgery. Figure 1 shows the process of the study. The patients were asked to choose an option from the scale with 1=“not at all” and 5=“very much”
Figure1.
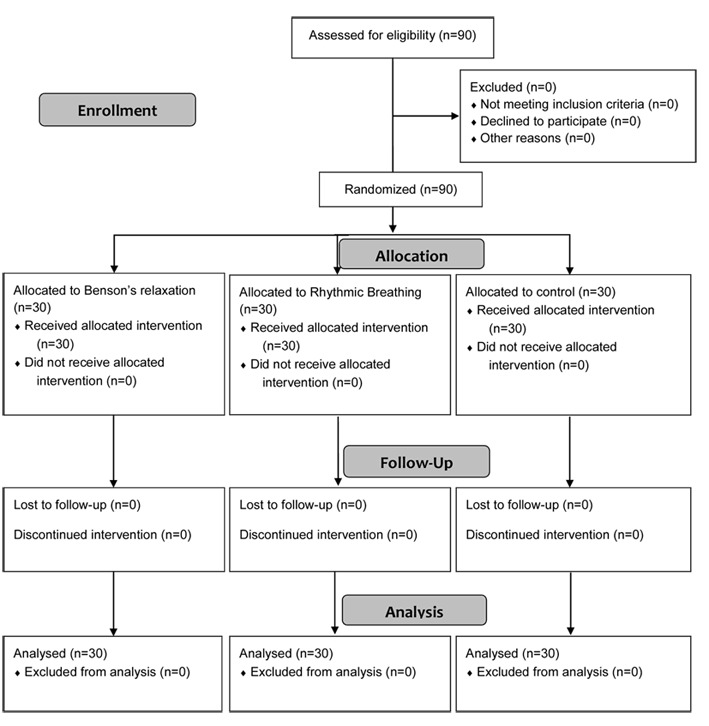
The process of the study
Instrument
The cognitive-somatic trait anxiety questionnaire (CSAQ) was developed using the items of other similar questionnaires along with the comments of experts in the field of cognitive and somatic anxiety. It was composed of 14 items from both cognitive and somatic anxiety with an equal number of items. The reliability and validity of the CSAQ was confirmed in a study by Reeder.33 The CSAQ was developed after a literature review and was translated using the forward and backward method. For content validity, 10 faculty members read the CSAQ and provided necessary feedbacks. With regard to its reliability, the CSAQ was assessed using the internal consistency and calculation of the Cronbach’s alpha coefficient, which was reported 85.3 percent for the whole scale.
The CSAQ was consisted of 14 questions and designed to measure cognitive and somatic components of anxiety with the equal number of items. Each question was scored using a five-point Likert scale with a range from “not at all” to “always”. The Cut-off point for the CSAQ was determined 14 and for each subscale was 7. Therefore, the patients who acquired a score below 14 scores had no anxiety, 14-27 scores had slight anxiety, 28-41 had moderate anxiety, 42-55 had severe anxiety and 56-70 had very much anxiety.
The sums of the scores were separately computed for the cognitive and somatic sections. The collected data were analysed using descriptive and inferential statistics via the SPSS V.21 software. Statistical tests used in this study were the repeated measures analysis of variance (ANOVA), Chi-square and Kruskal-Wallis tests. P<0.05 was considered statistically significant.
RESULTS
Most participants were satisfied with learning the Benson’s relaxation and rhythmic breathing techniques.
The age range of the participants was 30-50 years. In the Benson’s relaxation group, it was 30-40 years and in the rhythmic breathing and control groups was 40-50 years. There were no statistically significant differences between the groups in terms of demographic characteristics. (P˂0.05) (Table 1).
Table 1.
The demographic characteristics of the samples
| Variable | Control Group | Benson’s relaxation group | Rhythmic breathing | |
|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||
| Age | >50 y | 27 (90.0) | 19 (60.0) | 23 (63.3) |
| 50 y | 3 (10.0) | 11 (40.0) | 7 (36.7) | |
| Educational Status | School | 7 (56.7) | 10 (33.3) | 21 (70.0) |
| Secondary school | 8 (26.7) | 12 (40.0) | 8 (26.7) | |
| Academic | 5 (16.7) | 8 (26.7) | 1 (3.40) | |
| Fertility Status | Menstruation status | 24 (80.0) | 21 (70.0) | 22 (73.4) |
| Menopausal period | 6 (20.0) | 9 (30.0) | 8 (26.7) | |
| The history of OCP use | Yes | 24 (80.0) | 21 (70.0) | 22 (73.3) |
| No | 6 (20.0) | 9 (30.0) | 8 (26.7) | |
No statistically significant differences were observed between the groups regarding anxiety before the interventions (P=0.547), cognitive anxiety (P=0.186) and somatic anxiety (P=0.354). With regard to the postoperative anxiety, a statistically significant reduction was reported in the Benson’s relaxation technique group (P<0.001) and rhythmic breathing technique group (P˂0.001). However, in the control group, there was no statistically significant improvement in anxiety after the mastectomy surgery compared with before it was reported. Also, no statistically significance decrease in the postoperative anxiety (P=0.051) was found in the Benson’s relaxation technique group compared to the control group. However, after surgery the patients in the Benson’s relaxation technique group were significantly less anxious than the control group (P=0.049) (Table 2).
Table 2.
The comparisons of anxiety between the groups
| Variable | Before the intervention | After the surgery | ||||
|---|---|---|---|---|---|---|
| Group | Mean±SD | P value | Group | Mean±SD | P value | |
| Anxiety | Benson’s relaxation | 28.53±10.20 | 0.574 | Benson’s relaxation | 21.20±7.84 | 0.05 |
| Control | 24.73±7.87 | |||||
| Rhythmic breathing | 26.1±6.00 | Rhythmic breathing | 17.26±3.70 | ˂0.001 | ||
| Control | 24.73±7.87 | |||||
| Control | 26.6±7.40 | Benson’s relaxation | 21.20±7.84 | 0.04 | ||
| Rhythmic breathing | 17.26±3.70 | |||||
| Cognitive anxiety | Benson’s relaxation | 14.3±7.14 | 0.0186 | Benson’s relaxation | 15.46±6.8 | 0.20 |
| Control | 16.23±5.79 | |||||
| Rhythmic breathing | 14.2±4.87 | Rhythmic breathing | 10.73±3.70 | 0.001 | ||
| Control | 16.23±5.79 | |||||
| Control | 16.2±5.68 | Benson’s relaxation | 15.46±6.80 | 0.08 | ||
| Rhythmic breathing | 16.23±5.79 | |||||
| Somatic anxiety | Benson’s relaxation | 10.36±4.13 | 0.354 | Benson’s relaxation | 9.53±3.00 | 0.02 |
| Control | 11.93±4.17 | |||||
| Rhythmic breathing | 11.8±4.52 | Rhythmic breathing | 8.60±2.05 | 0.002 | ||
| Control | 11.93±4.17 | |||||
| Control | 10.36±4.12 | Benson’s relaxation | 9.53±3.00 | 0.32 | ||
| Rhythmic breathing | 11.93±4.70 | |||||
The means of postoperative cognitive anxiety in the Benson’s relaxation and rhythmic breathing techniques groups compared to the control group were statistically significant (P=0.006), and the participants in the rhythmic breathing technique group than the Benson’s relaxation technique group, experienced a lower postoperative cognitive anxiety (P=0.083).
A statistically significant difference between the interventions group and control group was seen regarding the mean score of postoperative anxiety (P=0.004). Moreover, no statistically significant differences were observed between the patients in the intervention groups (P=0.321)
DISCUSSION
Anxiety and other psychological distress lead to the stimulation of the sympathetic system. A regular use of relaxation techniques reduces stress response, and particularly reduces anxiety levels, allows for better coping with aggressive behaviours and negative emotions.
This study showed that rhythmic breathing can cause a reduction in the anxiety of patients after the mastectomy surgery. In a study by Kejellgren, patients found rhythmic breathing useful for reducing their anxiety.34 Another study on the yoga and progressive relaxation on anxiety and tension reduction reported that breathing yogic type of relaxation was an effective technique for increasing energy and reducing tension and anxiety.35 Yoga can be safely used as an instrument for improving patients’ psychological well-being. From the yogic perspective, well-being is more than psychological aspect and the results of this study supported the efficacy of two relaxation techniques in reducing tension and anxiety and enhancement of energy.
As hypothesized, the Benson’s relaxation and rhythmic breathing techniques reduced cognitive and somatic anxiety. Further, there appeared to be no statistically significant differences between the effects of either techniques on cognitive anxiety and somatic anxiety.
The Benson’s relaxation technique did not reduce cognitive anxiety greater than rhythmic breathing, but rhythmic breathing technique reduced somatic anxiety more than the Benson’s relaxation technique. Consistent with the findings of another study,8 the present study provided further evidence that the multi-process theory might not be adequate for predicting the specific effects of relaxation techniques on cognitive and somatic anxiety. From a practical viewpoint, our study’s findings supported the idea that the effect of both relaxation techniques on the reduction of cognitive and somatic anxiety. However, this study showed that the rhythmic breathing technique had a greater somatic effect than the Benson’s relaxation technique through its relaxing effect on the body.
The findings of this study should be viewed in light of the following limitations. For instance, Smith (1990) suggested that the education of relaxation techniques needs four to sixteen weeks.36 Consequently, the effects of a relaxation technique could change as patients become more experienced in performing the technique. However, in this study one day was spent for the education of the techniques. Also, the sample of this study was different from others. For instance, the Benson’s relaxation and the rhythmic breathing techniques could affect anxiety in mastectomy candidates differently from healthy people who might experience anxiety before an important sport event, before an elective surgery or a panic attack. Furthermore, the time interval between the intervention and postoperative period was too long and no interventions were performed before the surgery. Lastly, the implantation of rhythmic breathing was not possible after the surgery due to pain and the restriction of range of motions.
Given limitations discussed above, the findings of the present study provided evidence about the effectiveness of the Benson’s relaxation technique and rhythmic breathing in the reduction of cognitive and somatic anxiety. Further research is required to substantiate these findings by addressing the limitations already noted and exploring the effects of relaxation techniques in a clinical environment on a variety of population.
Since no similar study was found in the literature, we were unable to compare our findings with those of other studies.
CONCLUSION
The findings of this study suggested that the mastectomy surgery candidates could benefit from learning the Benson’s relaxation and rhythmic breathing techniques. Therefore, further studies are recommended for applying other types of cognitive and somatic relaxation techniques in healthy people or patients with other diseases.
ACKNOWLEDGEMENT
We express our appreciation to all participants and those who assisted with this study. The present article was the result of a master thesis supported financially by Tehran University of Medical Sciences, Tehran, Iran (Grant No: 657). Also, no conflict of interest is declared by the authors.
Conflict of Interest:None declared.
REFRENCES
- 1.Siegel R, Naishadham D, Jemal A. Cancer Statistics, 2012. CA: A Cancer Journal for Clinicians. 2012;62:10–29. doi: 10.3322/caac.20138. [DOI] [PubMed] [Google Scholar]
- 2.Ho SS, So WK, Leung DY, et al. Anxiety, depression and quality of life in Chinese women with breast cancer during and after treatment: A Comparative Evaluation. European Journal of Oncology Nursing. 2013;17:877–82. doi: 10.1016/j.ejon.2013.04.005. [DOI] [PubMed] [Google Scholar]
- 3.McDonald C, Bauer J, Capra S, Coll J. The muscle mass, omega-3, diet, exercise and lifestyle (MODEL) study - a randomized controlled trial for women who have completed breast cancer treatment. BMC Cancer. 2014;14:264. doi: 10.1186/1471-2407-14-264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. International Journal of Cancer. 2010;127:2893–917. doi: 10.1002/ijc.25516. [DOI] [PubMed] [Google Scholar]
- 5.Aghajani H, Eatemad K, Guya MM, et al. Iranian Annual of National Cancer Registration report 2008-2009. Tehran (Iran): Ministry of Health and Medical Education; 2011. [cited 1 January 2016] Available from: [http://eazphcp.tbzmed.ac.ir/uploads/26/CMS/user/file/90/%D8%A8%DB%8C%D9%85%D8%A7%D8%B1%DB%8C%D9%87%D8%A7%DB%8C%20%D8%BA%DB%8C%D8%B1%D9%88%D8%A7%DA%AF%DB%8C%D8%B1/%D8%A2%D9%85%D8%A7%D8%B1/%DA%AF%D8%B2%D8%A7%D8%B1%D8%B4%20%D9%83%D8%B4%D9%88%D8%B1%D9%8A%20%D8%AB%D8%A8%D8%AA%20%D8%B3%D8%B1%D8%B7%D8%A7%D9%86%201387.pdf. ] [In Persian]
- 6.Halsted WS. The results of operations for the cure of cancer of the pancreas performed at the Johns Hopkins Hospitals. Ann Surg. 1894;20:497–555. doi: 10.1097/00000658-189407000-00075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sakorafas GH, Safioleas M. Breast cancer surgery: an historical narrative. Part I. From prehistoric times to Renaissance Eur J Cancer Care (Engl) 2009;18:530–44. doi: 10.1111/j.1365-2354.2008.01059.x. [DOI] [PubMed] [Google Scholar]
- 8.Caumo W, Schmidt AP, Schneider CN, et al. Risk factors for postoperative anxiety in adults. Anaesthesia. 2001;56:720–8. doi: 10.1046/j.1365-2044.2001.01842.x. [DOI] [PubMed] [Google Scholar]
- 9.Bjorneklett HG, Lindemalm C, Rosenblad A, et al. A randomised controlled trial of support group intervention after breast cancer treatment: results on anxiety and depression. ActaOncologica. 2012;51:198–207. doi: 10.3109/0284186X.2011.610352. [DOI] [PubMed] [Google Scholar]
- 10.Den Oudsten BL, Van Heck GL, Van der Steeg AF, et al. Predictors of depressive symptoms 12 months after surgical treatment of early-stage breast cancer. Psycho-oncology. 2009;18:1230–7. doi: 10.1002/pon.1518. [DOI] [PubMed] [Google Scholar]
- 11.Li XM, Zhou KN, Yan H, et al. Effects of music therapy on anxiety of patients with breast cancer after radical mastectomy: a randomized clinical trial. Journal of Advanced Nursing. 2012;68:1145–55. doi: 10.1111/j.1365-2648.2011.05824.x. [DOI] [PubMed] [Google Scholar]
- 12.Lin MF, Hsieh YJ, Hsu YY, et al. A randomized controlled trial of the effect of music therapy and verbal relaxation on chemotherapy induced anxiety. Journal of Clinical Nursing. 2011;20:988–99. doi: 10.1111/j.1365-2702.2010.03525.x. [DOI] [PubMed] [Google Scholar]
- 13.Zhou KN, Li XM, Yan H, et al. Effects of music therapy on depression and duration of hospital stay of breast cancer patients after radical mastectomy. Chinese Medical Journal. 2011;124:2321–7. [PubMed] [Google Scholar]
- 14.Kovačič T, Zagoričnik M, Kovačič M. Impact of relaxation training according to the Yoga In Daily Life system on anxiety after breast cancer surgery. Journal of Complementary & Integrative Medicine. 2013;10:153–64. doi: 10.1515/jcim-2012-0009. [DOI] [PubMed] [Google Scholar]
- 15.Kovačič T, Kovačič M. Impact of relaxation training according to Yoga in Daily Life system on perceived stress after breast cancer surgery. Integrative Cancer Therapies. 2011;10:16–26. doi: 10.1177/1534735410387418. [DOI] [PubMed] [Google Scholar]
- 16.Kashani F, Babaee S, Bahrami M, Valiani M. The effects of relaxation on reducing depression, anxiety and stress in women who underwent mastectomy for breast cancer. Iranian Journal of Nursing and Midwifery Research. 2012;17:30–3. [PMC free article] [PubMed] [Google Scholar]
- 17.Ergun M, Eyigor S, Karaca B, et al. Effects of exercise on angiogenesis and apoptosis-related molecules, quality of life, fatigue and depression in breast cancer patients. European Journal of Cancer Care. 2013;22:626–37. doi: 10.1111/ecc.12068. [DOI] [PubMed] [Google Scholar]
- 18.Mehnert A, Veers S, Howaldt D, et al. Effects of a physical exercise rehabilitation group program on anxiety, depression, body image, and health-related quality of life among breast cancer patients. Onkologie. 2011;34:248–53. doi: 10.1159/000327813. [DOI] [PubMed] [Google Scholar]
- 19.Passik SD, Kirsh KL, Donaghy KB, et al. Effects of Pilates exercises on functional capacity, flexibility, fatigue, depression and quality of life in female breast cancer patients: a randomized controlled study. European Journal of Physical and Rehabilitation Medicine. 2010;46:481–7. [PubMed] [Google Scholar]
- 20.Yoo MS, Lee H, Yoon JA. Effects of a cognitive-behavioural nursing intervention on anxiety and depression in women with breast cancer undergoing radiotherapy. Journal of Korean Academy of Nursing. 2009;39:157–65. doi: 10.4040/jkan.2009.39.2.157. [DOI] [PubMed] [Google Scholar]
- 21.Liao MN, Chen PL, Chen MF, Chen SC. Effect of supportive care on the anxiety of women with suspected breast cancer. Journal of Korean Academy of Nursing. 2010;66:49–59. doi: 10.1111/j.1365-2648.2009.05139.x. [DOI] [PubMed] [Google Scholar]
- 22.Cho EA, Oh HE. Effects of laughter therapy on depression, quality of life, resilience and immune responses in breast cancer survivors. Journal of Korean academy of nursing. 2011;41:285–93. doi: 10.4040/jkan.2011.41.3.285. [DOI] [PubMed] [Google Scholar]
- 23.Hansen MV, Andersen LT, Madsen MT, et al. Effect of melatonin on depressive symptoms and anxiety in patients undergoing breast cancer surgery: a randomized, double-blind, placebo controlled trial. Breast Cancer Research and Treatment. 2014;145:683–95. doi: 10.1007/s10549-014-2962-2. [DOI] [PubMed] [Google Scholar]
- 24.Genc F, Tan M. The effect of acupressure application on chemotherapy in duced nausea, vomiting, and anxiety in patients with breast cancer. Palliative & Supportive Care. 2015;13:275–84. doi: 10.1017/S1478951514000248. [DOI] [PubMed] [Google Scholar]
- 25.Kim YH, Kim HJ, Ahn SD, et al. Effects of meditation on anxiety, depression, fatigue, and quality of life of women undergoing radiation therapy for breast cancer. Complementary Therapies in Medicine. 2013;21:379–87. doi: 10.1016/j.ctim.2013.06.005. [DOI] [PubMed] [Google Scholar]
- 26.de Niet G, Tiemens B, Lendemeijer B, Hutschemaekers G. Music-assisted relaxation to improve sleep quality: meta-analysis. Journal of Advanced Nursing. 2009;65:1356–64. doi: 10.1111/j.1365-2648.2009.04982.x. [DOI] [PubMed] [Google Scholar]
- 27.Brand LR, Munroe DJ, Gavin J. The Effect of Hand Massage on Preoperative Anxiety in Ambulatory Surgery Patients. AORN Journal. 2013; 97:708–17 . doi: 10.1016/j.aorn.2013.04.003. [DOI] [PubMed] [Google Scholar]
- 28.Gill S, Kolb GS, Keating J. Examining the multi-process theory: an investigation of the effects of two relaxation techniques on state anxiety. Journal of Bodywork and Movement Therapies. 2004;8:288–96. [Google Scholar]
- 29.Payne RA. Relaxation techniques: A practical handbook for the health care professional. 3rd ed. Netherlands: Elsevier; 2005. pp. 120–86. [Google Scholar]
- 30.Kwekkeboom KL, Gretarsdottir E. Systematic Review of Relaxation Intervention for Pain. Journal of Nursing Scholarship. 2006;38:269–77. doi: 10.1111/j.1547-5069.2006.00113.x. [DOI] [PubMed] [Google Scholar]
- 31.Schwartz GE, Davidson RJ, Goleman DJ. Patterning of cognitive and Somatic Processes in the self-regulation of Anxiety: Effects of meditation versus exercise. Psychosomatic Medicine. 1978;40:321–8. doi: 10.1097/00006842-197806000-00004. [DOI] [PubMed] [Google Scholar]
- 32.Spielberger CD. In: Weiner IB, Craighead WE, editors. The Corsini Encyclopedia of Psychology. 4th ed. US: John Wiley & Sons, Inc; 2010. [Google Scholar]
- 33.Reeder M. The emotional congruence of experience and bodily change [thesis] Australia: Australian Catholic University; 2001. [Google Scholar]
- 34.Kejellgren A, Bood SA, Axelsson K, et al. Wellness through a comprehensive Yogic breathing program - A controlled pilot trial. BMC Complementary and Alternative Medicine. 2007;7:43. doi: 10.1186/1472-6882-7-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kulmatycki L. Yoga and Progressive Relaxation for Anxiety and Tension Reduction. SENSE. 2012;2:93–102. [Google Scholar]
- 36.Smith JC. Cognitive-behavioural relaxation training: a new system of strategies for treatment and assessment. New York: Springer; 1990. [Google Scholar]