

ABSTRACT
Background:
According to the World Health Organization viewpoint, social well-being is an important dimension of health along with physical and mental aspects. Evaluation of social well-being is necessary in students, especially in medical sciences students due to future responsibility as health care professionals. The present study attempted to investigate the level of social well-being, five domains of it (like actualization, integration, contribution), and some related factors in the school of nursing and midwifery students.
Methods:
This cross-sectional study was carried out between Julys to December 2015 and comprised 346 students in the school of nursing and midwifery in Shiraz University of Medical Sciences, Shiraz, Iran. Social well-being, socio-demographic status and physical activity were measured by valid questionnaires. Univariate linear regression analysis, multiple imputation method, ANOVA and independent sample t-test were used as different statistical methods. The P values less than 0.05 were considered as statistically significant.
Results:
The mean score of social well-being was 50. The minimum and maximum scores of social well-being were 20 to 100. Married students had higher social well-being than single students in univariate linear regression (Beta: 2.111, 95% CI: (0.387 to 3.738), P=0.017). Also, social integration had higher scores in married students (P=0.015). Social actualization was higher in male students (P=0.015); on the other hand, social contribution was higher in female students (P=0.026).
Conclusion:
The results of our study showed that social well-being status of students in this research was not satisfactory. Designing and conducting programs for promotion of social well-being, for example preparing facilities for marriage of students, can be helpful. Evaluation of social well-being in students of other schools with multicenter studies seems to be useful.
KEYWORDS: Social wellbeing, Nursing, Midwifery, Shiraz, Iran
INTRODUCTION
According to the World Health Organization viewpoint, social well-being is an important dimension of health along with physical and mental aspects. It plays an effective role in improving the quality of life, social efficacy, and social performance.1
Social well-being is an important factor which demonstrates the circumstance and functioning of the society. It contains five domains which include social integration “the evaluation of the quality of one’s relationship to society and community”, social acceptance “the construal of society through the character and qualities of other people as a generalized category”, social contribution “ the belief that one is a vital member of society, with something of value to give to the world”, social actualization “the evaluation of the potential and trajectory of society”, and social coherence “the perception of the quality, organization and operation of the social world, and it includes a concern for knowing about the world”.2
Students are considered as an impressive social class in sustainable development.3 Therefore, their social well-being status is a capital for society.4 Medical sciences students have the responsibility to provide health care services in future. Therefore, their appropriate social well-being status has an effective role in their efficacy.
There are a few studies about social well-being in students in Iran.5,6 The present study was an attempt to investigate the level of social well-being, five domains of it (like actualization, integration, contribution, and etc), and some related factors in the school of nursing and midwifery students.
MATERIALS AND METHODS
Participants
This cross-sectional study comprised the students studying in nursing and midwifery school in Shiraz University of Medical Sciences between July to December 2015. The fields of study included nursing, midwifery, anesthesiology, operation room technician, and emergency care. The Cochrane formula was used to determine the sample size with N=1200, d=0.05 p=0.5, q=0.5, and α=0.05.7 With stratified random sampling based on majors and program as stratum the numbers of classes in every category were identified. Eleven classes were chosen randomly. Different programs including PhD (Nursing students), Master and Bachelor degrees were considered.
Data Collection
Three independent interviewers were performed by research team. They briefed about the study before filling in the questionnaires. All of the students of the class were asked to fill out the questionnaires. In the first pages of the questionnaire, we ensured the students that participation is voluntary The inclusion criterion was belonging to the School of Nursing & Midwifery in Shiraz University of Medical sciences. On the other hand, if students came from another university or college, to be guest students, she or he was excluded. The Ethics Committee of Shiraz University of Medical Sciences approved this study. The ethics committee code is 94-01-64-9700. The verbal informed consent was obtained.
Social Well-Being Questionnaire
Keyes questionnaire was used for evaluating social well-being which was standardized by Iranian researchers. The Cronbach’s alpha was 0.81 and confirmatory factorial analysis showed the best fit for this questionnaire.8,9 The questionnaire was based on a Likert scale and Keyes’ social well-being theoretical mode provided a scale, including 33 and 20 items presented in long and short forms with constant domains. We used Keyes short form questionnaire which includes four, three, three, five and five items that were about social actualization, social coherence, social integration, social acceptance, and social contribution, respectively. Grading ranged from strongly disagrees to strongly agree represented by 1-2-3-4-5. The grading was inversed as 5-4-3-2-1 with respect to17 items. The score between 20 to 46, 47 to 74 and 75 to 100 obtained by the participants indicated low, middle and high social well-being statuses, respectively. In our study, the Cronach’s alpha was 0.63. Factor analysis was used for validating Keye’s questionnaire. Five dimensions were derived after omitting 2 items. A Kaiser-Meyer-Olkin (KMO) analysis supported factorability, R=0.79 and Bartlett’s test indicated a breach of sphericity, χ2= 1934.87, P=0.0001
Socio-Economic Status (SES)
In this study, we used SES questionnaire which was designed and standardized by Islami and their colleagues in GEMINI (Gastric and Esophageal Malignancy in Northern Iran) study group.10 This questionnaire contains various parts which include insurance support, family member, house ownership, and facilities in their house. We also use Amos software to evaluate composite reliability (CR), and discriminant validity for these subdomains. The CR for domains was higher than 0.7. The discriminant validity for various subdomains was appropriate unless the appliance was in their house.
Physical Activity Questionnaire
We used valid International Physical Activity Questionnaire (IPAQ), which was designed by World Health Organization (WHO).11 and used in several studies. 12-18 This questionnaire was validated in Iran. Vasheghani et al. showed that the IPAQ questionnaire was discriminated well between the subgroups of the study and showed the intra-class correlation coefficient (ICC) more than 0.7.19 In our study, the Cronbach’s alpha for this questionnaire was 0.84.
Statistical Analysis
We used Independent samples t-test and ANOVA to differentiate between the scores in 5 domains of social well-being in several variables. The univariate linear regression analyses were used to determine the association between different factors with social well-being. The data were missing completely at random (MCAR); therefore, multinomial logistic regression imputation method was employed for missing data in some parts of physical activity. Finally, multiple linear regression analysis was used to determine adjusted coefficient.
A factor analysis composed of principal components analysis followed by a Varimax rotation was performed to explore the scale for possible subscale constructs that recorded items for social well-being, socio-economic status, and physical activity.
Factorial Analysis for Validation
Although Keye’s questionnaire had already been validated, we performed factor analysis to explore the scale for possible subscale constructs that recorded items for social well-being. We used ANOVA and independent sample t-test to differentiate between scores in 5 domains of social well-being in demographic characteristics.
Statistical analyses were performed using SPSS software (SPSS for Windows 19.0, SPSS, Chicago, IL, USA and STATA version13) and the P-values less than 0.05 were considered as statistically significant.
RESULT
This study comprised 366 students, of whom 40 (10.9%) had low or weak, 303(82.8%) middle, and 3(0.8%) exhibited good or high social well-being score. Twenty participants (5.5%) were excluded due to incomplete questionnaires. (figure 1).
Figure1.
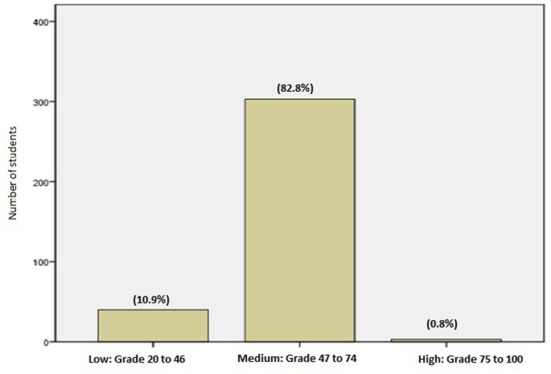
Social well-being statuses in students of school of midwifery and nursing in Shiraz University of Medical Sciences
The mean social well-being scores of students were about 50, of which the highest and lowest social well-being scores were those of emergency care and anesthesiology; also, PhD students had the highest social well-being scores. We did not find any significant difference between social well-being and its domains in different fields of study. (Table 1)
Table 1.
Social well-being scores of school of midwifery and nursing students in Shiraz University of Medical Sciences
| Characteristic | Sub Category | Number(%) | Social well-being score*(Mean±SD) | P value** |
|---|---|---|---|---|
| Sex | Male | 102(27.90) | 52.60±14.52 | 0.27 |
| Female | 259(70.80) | 52.39±14.10 | ||
| Missing | 5(1.40) | 43.20±24.6 | ||
| Place of residence | Native | 133(36.30) | 51.45±15.43 | 0.03 |
| Expatriates | 221(60.40) | 53.15±13.13 | ||
| Missing | 12 (3.30) | 46.83±22.24 | ||
| Marital Status | Single | 274(74.60) | 52.20±14.58 | 0.83 |
| Married | 92(24.80) | 52.07±11.50 | ||
| P value*** | ||||
| Major | Nursing | 143(39.10) | 54.30±12.28 | 0.87 |
| Midwifery | 86(23.50) | 53.15±13.10 | ||
| Anesthesiology | 50(13.70) | 47.44±17.77 | ||
| operation room technician | 38(10.40) | 50.71±16.91 | ||
| Emergency Care | 22(6) | 54.36±7.02 | ||
| Missing | 27(7.40) | 48.73±19.85 | ||
| Program | Bachelor | 330(90.20) | 52.46±14.24 | 0.46 |
| Master of Science and higher | 4(1.10) | 50.25±4.85 | ||
| Ph.D | 17(4.) | 54.52±15.89 | ||
| Missing | 15(4.10) | 48.38±17.26 | ||
| Educational Status of father | Under six grade | 155 (42.30) | 54.23±6.78 | 0.80 |
| High school diploma | 101(27.60) | 52.32±14.84 | ||
| Bachelor | 75(20.50) | 55.73±71.10 | ||
| Master of science and higher | 155(42.30) | 33.47±25.91 | ||
| Missing | 12(3) | 50.00±8.48 | ||
| Educational Status of mother | Under six grade | 205 (56) | 54.66±6.58 | 0.07 |
| Diploma | 92(25.10) | 53.40±13.08 | ||
| Bachelor | 47(12.80) | 52.02±18.56 | ||
| Master of science and higher | 4 (1.10) | 46.25±19.12 | ||
| PhD | 2(0.50) | 50.00±8.48 | ||
| Missing | 18(4) | 45.35±19.71 | ||
Due to 20 graded questions of instrument the expected minimum and maximum are 20 and 100, respectively.
Independent sample t-test
ANOVA
Social actualization mean scores in females (13.11) were higher than those of males students (11.34) significantly (P=0.015). On the other hand, social contribution mean scores in males (12.35) were higher than female students (11.15), (P=0.026). Also in regard to marital status, there was a significant difference in social integration mean scores between married (5.71) and single subjects (5.38), (P=0.015). The remaining variables did not show any significant difference in various domains.
The people who were under the supportive care of Imam Khomeini relief committee exhibited lower mean score of social well-being. The socio-economic status variables are demonstrated in Table 2.
Table 2.
Relationship between social well-being variable and socio-economic status of school of midwifery and nursing students in Shiraz University of Medical Sciences
| Variables | Subcategory | Number (percent) | social well-being score (Mean±SD)* | sP value** | |
|---|---|---|---|---|---|
| Under supportive organization coverage | Imam Khomeini committee | 8(2.20) | 34.25±28.87 | 0.71 | |
| Welfare | 5(1.40) | 48.00±27.00 | |||
| Martyr Foundation | 13 (3.60) | 53.92±5.33 | |||
| None | 254 (69.40) | 52.67±13.54 | |||
| House area (m2) | First tertile (<80) | 19(5.20) | 53.78±15.41 | 0.15 | |
| Second tertile (80-100) | 115(31.40) | 53.82±14.59 | |||
| Third tertile(>100) | 232(63.40) | 51.45±14.18 | |||
| Number of people in household | First tertile (1-4) | 203 (55.50) | 52.08±14.85 | 0.78 | |
| Second tertile (5-6) | 79(21.60) | 53.97±8.94 | |||
| Third tertile (7+) | 13(3.60) | 51.85±17.16 | |||
| Number of children | First tertile (0-6) | 195 (53.30) | 53.14±14.60 | 0.78 | |
| Second tertile (7-8) | 89 (24.30) | 52.21±12.72 | |||
| Third tertile (9+) | 80 (21.90) | 50.36±15.65 | |||
| P value*** | |||||
| Under insurance coverage | Yes | 295(80.60) | 52.59±14.11 | 0.57 | |
| No | 36 (9.80) | 52.44±11.39 | |||
| Supplementary insurance | Yes | 115 (31.40) | 51.85±12.72 | 0.67 | |
| No | 146 (39.90) | 52.95±14.93 | |||
| House ownership | Yes | 304(83.10) | 52.67±13.85 | 0.54 | |
| No | 53(14.40) | 51.62±14.85 | |||
| Appliance ownership | Car | Yes | 285(77.86) | 52.32±14.61 | 0.52 |
| No | 65(17.75) | 53.03±13.39 | |||
| Color TV | Yes | 351(95.01) | 52.56±14.08 | 0.31 | |
| No | 7(1.91) | 47.14±21.12 | |||
| Vacuum Cleaner | Yes | 330(90.16) | 52.27±14.68 | 0.66 | |
| No | 25(6.83) | 52.24±12.98 | |||
| Washing machine | Yes | 98(26.77) | 51.04±19.13 | 0.78 | |
| No | 242(66.12) | 53.09±12.15 | |||
| Refrigerator | Yes | 215(58.74) | 51.70±16.3 | 0.33 | |
| No | 133(36.33) | 53.38±11.39 | |||
| Computer | Yes | 308(84.15) | 52.19±14.75 | 0.67 | |
| No | 47(12.84) | 53.14±13.22 | |||
| Furniture | Yes | 231(63.11) | 51.58±15.68 | 0.96 | |
| No | 115(31.14) | 54.18±11.36 | |||
| Split | Yes | 154(42.07) | 51.20±16.97 | 0.27 | |
| No | 189(51.16) | 53.11±12.57 | |||
Because of missing information, the sum of percentages did not add up to 100%.
ANOVA
Independent sample t-test
Table 3 which displays the principal component method shows the relationship between 5 domains of social well-being. As expected, a high correlation was observed between most domains. This high correlation shows the consistence between various domains (Table 4).
Table 3.
The correlation between various domains of social well-being in School of midwifery and nursing students in Shiraz University of Medical Sciences
| Social actualization | Social coherence | Social integration | Social contribution | ||
|---|---|---|---|---|---|
| Social actualization | 1 | - | - | - | - |
| Social coherence | 0.96 | 1 | - | - | - |
| Social integration | 0.96 | 0.94 | 1 | - | - |
| Social acceptance | 0.97 | 0.96 | 0.94 | 1 | - |
| Social contribution | 0.96 | 0.96 | 0.94 | 0.97 | 1 |
For all domains every P value is less than 0.0001; Pearson correlation
Table 4.
Relationship between social well-being score and predictive variable in school of midwifery and nursing students in Shiraz University of Medical Sciences in 2015
| Variable | Coefficient | Standard. Error. | t | P>t | [95% Conf. Interval] | |
|---|---|---|---|---|---|---|
| Sex | 21.18 | 3.86 | 5.48 | 0.12 | -27.90 to 70.27 | |
| Age | 0.18 | 0.20 | 0.93 | 0.52 | -2.31 to 2.67 | |
| Program | Bachelor | -15.03 | 3.54 | -4.25 | 0.15 | -59.99 to 29.93 |
| Master of Science and higher | -17.96 | 6.02 | -2.98 | 0.21 | -94.48 58.57 | |
| Ph.D | 0.74 | 2.66 | 0.28 | 0.83 | -33.01 to 34.48 | |
| Educational status of Father | Under six grade | 2094.94 | 377.56 | 5.55 | 0.11 | -2702.61 to 6892.49 |
| High school diploma | 44.46 | 3.83 | 11.61 | 0.06 | -4.21 to 93.13 | |
| Bachelor | 38.73 | 3.86 | 10.04 | 0.06 | -10.30 to 87.76 | |
| Master of science and higher | 2075.99 | 373.78 | 5.55 | 0.11 | -2673.33 to 6825.31 | |
| Educational status of Mather | Under six grade | -21.64 | 2.76 | -7.85 | 0.08 | -56.66 to 13.38 |
| High school diploma | -30.67 | 3.63 | -8.46 | 0.08 | -76.74 to 15.39 | |
| Bachelor | 2040.76 | 375.62 | 5.43 | 0.12 | -2731.92 to 6813.43 | |
| Master of science and higher | -68.99 | 7.96 | -8.67 | 0.07 | -170.13 to 32.16 | |
| Marital status | -36.07 | 3.80 | -9.49 | 0.07 | -84.36 to 12.23 | |
| *SES | 1.10 | 0.47 | 2.35 | 0.26 | -4.85 to 7.05 | |
| Physical activity | -2066.07 | 375.54 | -5.50 | 0.11 | -6837.81 to 2705.67 | |
| Severity of Physical activity | 31.73 | 3.86 | 8.22 | 0.08 | -17.30 to 80.76 | |
| Home activity | 7.03 | 2.25 | 3.12 | 0.20 | -21.60 to 35.66 | |
| Intensity of home chore | -32.59 | 4.78 | -6.82 | 0.09 | -93.32 to 28.14 | |
The SES category was determine by Principal Component Method; Multiple linear regressions
Social well-being score was higher in married students than others in Univariate linear regression analysis significantly. (Beta: 2.111, 95% CI 0.387 to 3.738; P=0.017). There was no relationship between social well-being and other variables in multiple linear regressions.
The Result of Factorial Analysis
As we expected, the result of factorial analysis for Keye’s questionnaire was slightly different from previous result. It demonstrated that social contribution mean scores in females (9.74) were lower than male students (11.04) significantly (P=0.003). But other dimensions and total score of social well-being were not different significantly between gender groups. Native students had higher score (50.39) in social well-being than non-natives (48.23) significantly. (P=0.036) On the other hand, they had significantly higher social coherence score (9.98) than non-natives (9.42), (P=0.031). Also, factorial analysis did not show any significant impact on social well-being and its components.
DISCUSSION
To date few studies have been done about social well-being in university students. Evaluation of social well-being in medical sciences students is necessary due to their future responsibility. If medical sciences students have high social well-being status, they can be more effective in their jobs. Based on this study, the level of social well-being of these students is not high.
The mean of social well-being score in Iranian social sciences students in Tehran, the capital city of Iran, was high.20 In another study which was conducted in a college of Fars province, the mean score of social well-being was not high.8 In a study done on teachers in Iran, most participants had middle, good or high social well-being scores.21 Our study results are concordance with those of Fars study; on the other hand, teachers and Tehrani students had higher social well-being than our university students.
There was a relationship between social wellbeing score and marital status in this study. The Shapiro’ study in the United States showed an association between marital and social well-being statuses.22 In a study done in Netherlands, there were no differences between unmarried and married persons. They concluded that marriage no longer provides advantages over non-married persons in social life.23 The effect of marriage on social well-being status may relate to cultural properties in different countries.
Several studies demonstrated the important effect of physical activity and socio-economic status on health, but a few studies investigated the relationship between these factors with social well-being.24-27 Farzi et al. reported a high social well-being score in university students with high physical activity level.28 There was a direct association between social well-being score and SES in social sciences students in Tehran.20 We didn’t find a relationship between physical activity and SES on social well-being in our study.
In a multi-central study, social well-being of Iranian, Italian and American students was compared. There was no significant difference between sex and social well-being in this study.29 Our study showed no obvious difference in social well-being score between female and male students, but males had higher social contribution whereas females demonstrated higher social actualization. Social actualization implies the belief that society has the potential for positive changes. High female social actualization score indicates that female students’ attitude may enhance positive roles in future development of the society. This theory may explain higher social actualization in female students. Social contribution implies the belief that society has the potential responsibility for positive change and toward society as an important concept of social well-being. More social contribution score of male students demonstrated that male students’ attitude may enhance higher social responsibility than females; therefore, the high score for social contribution in male students seems reasonable.
Native students had more social well-being and social cohesion score than non-native students who lived in dormitories. Social coherence indicates personal belief about meaningful life. It seems that living with families may have positive effects on this concept; therefore, this relationship is reasonable.
A limitation of our study was missing data in some parts of physical activity questionnaire, which was not easy to complete, but the imputation method w used solved this problem. On the other hand, we used high sample size of students in school of nursing and midwifery in Shiraz University of Medical Sciences which may be the strength of this study.
CONCLUSION
The results of our study showed that social well-being status of Iranian nursing and midwifery students was not satisfactory. Because social well-being has an important impact on health status, it has important implications for the policy making of Shiraz University of, Medical Sciences. Designing and conducting programs for promotion of social well-being, for example preparing facilities for marriage of students, can be helpful. Evaluation of social well-being in students of other schools with sequential multi-center studies seems to be useful.
ACKNOWLEDGEMENT
The authors thank School of Nursing and Midwifery, and research center for traditional medicine and history of medicine faculty members for their valuable cooperation. They also thank those who helped us with this study, especially the students, and interviewer. This study was supported by Research Center for Traditional Medicine and History of Medicine of Shiraz University of Medical Sciences.
Conflict of Interest:None declared.
REFRENCES
- 1.Breslow L. A quantitative approach to the World Health Organization definition of health: physical, mental and social well-being. International Journal of Epidemiology. 1972;1:347–55. doi: 10.1093/ije/1.4.347. [DOI] [PubMed] [Google Scholar]
- 2.Keyes CLM. Social well-being. Social Psychology Quarterly. 1998;61:121–40. [Google Scholar]
- 3.Conroy MM, Berke PR. What makes a good sustainable development plan? An analysis of factors that influence principles of sustainable development. Environment and Planning A. 2004;36:1381–96. [Google Scholar]
- 4.Wang CCD, Castañeda-Sound C. The Role of Generational Status, Self-Esteem, Academic Self-Efficacy, and Perceived Social Support in College Students’ Psychological Well-Being. Journal of College Counseling. 2008;11:101–18. [Google Scholar]
- 5.Poorkhirodin J, Tousi F, Hekmati E. Study of Determinant Factors Role of Students’ Social Well-Being. Journal Management System. 2009;4:8–26. [In persian] [Google Scholar]
- 6.Kahan B, Goodstadt M. Continuous quality improvement and health promotion: can CQI lead to better outcomes? Health Promotion International. 1999;14:83–91. [Google Scholar]
- 7.Israel GD. Determining sample size[Internet]. US: University of Florida Cooperative Extension Service, Institute of Food and Agriculture Sciences, EDIS; 1992. [Cited 13 May 2016] Available from: [http://www.sut.ac.th/im/data/read6.pdf. ]
- 8.Baghsorkhi AR, Refahi Z, Jahedi S. The relationship between social health and self-efficacy mediated by personality characteristics of graduate students. Journal of Novel Applied Sciences. 2013;2:36–40. [Google Scholar]
- 9.Hashemi T, Hekmati I, Vahedi SH, Babapour J. Psychometric properties of short-form social well-being questionnaire. Journal of Behvaioral Sciences. 2014;8:11–9. [Google Scholar]
- 10.Islami F, Kamangar F, Nasrollahzadeh D, et al. Socio-economic status and oesophageal cancer: results from a population-based case–control study in a high-risk area. International Journal of Epidemiology. 2009;38:978–88. doi: 10.1093/ije/dyp195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Armstrong T, Bull F. Development of the world health organization global physical activity questionnaire (GPAQ) Journal of Public Health. 2006;14:66–70. [Google Scholar]
- 12.Voorrips LE, Ravelli AC, Dongelmans PC, et al. A physical activity questionnaire for the elderly. Med Sci Sports Exerc. 1991;23:974–9. [PubMed] [Google Scholar]
- 13.Jacobs DR Jr, Ainsworth BE, Hartman TJ, Leon AS. A simultaneous evaluation of 10 commonly used physical activity questionnaires. Medicine and Science in Sports and Exercise. 1993;25:81–91. doi: 10.1249/00005768-199301000-00012. [DOI] [PubMed] [Google Scholar]
- 14.Crocker PR, Bailey DA, Faulkner RA, et al. Measuring general levels of physical activity: preliminary evidence for the Physical Activity Questionnaire for Older Children. Medicine and Science in Sports and Exercise. 1997;29:1344–9. doi: 10.1097/00005768-199710000-00011. [DOI] [PubMed] [Google Scholar]
- 15.Stewart AL, Mills KM, King AC, et al. CHAMPS physical activity questionnaire for older adults: outcomes for interventions. Medicine and Science in Sports and Exercise. 2001;33:1126–41. doi: 10.1097/00005768-200107000-00010. [DOI] [PubMed] [Google Scholar]
- 16.Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB. [DOI] [PubMed] [Google Scholar]
- 17.Bahrami H, Sadatsafavi M, Pourshams A, et al. Obesity and hypertension in an Iranian cohort study; Iranian women experience higher rates of obesity and hypertension than American women. BMC Public Health. 2006;6:158. doi: 10.1186/1471-2458-6-158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bauman A, Ainsworth BE, Sallis JF, et al. The descriptive epidemiology of sitting: a 20-country comparison using the International Physical Activity Questionnaire (IPAQ) American Journal of Preventive Medicine. 2011;41:228–35. doi: 10.1016/j.amepre.2011.05.003. [DOI] [PubMed] [Google Scholar]
- 19.Vasheghani-Farahani A, Tahmasbi M, Asheri H, et al. The Persian, last 7-day, long form of the International Physical Activity Questionnaire: translation and validation study. Asian Journal of Sports Medicine. 2011;2:106–16. doi: 10.5812/asjsm.34781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hatami P. Studying The Effectual Factors In Social Health of Students Emphasizing of Social Networks [Thesis] Tehran (Iran): Allameh Tabataba’i University Faculty of social sciences; 2010. [Google Scholar]
- 21.Hatam N, Joulaei H, Kazemifar Y, Askarian M. Cost efficiency of the family physician plan in fars province, southern iran. Iranian Journal of Medical Sciences. 2012;37:253–9. [PMC free article] [PubMed] [Google Scholar]
- 22.Shapiro A, Keyes CLM. Marital status and social well-being: Are the married always better off? Social Indicators Research. 2008;88:329–46. [Google Scholar]
- 23.Müller ML. Social well-being: investigating the relation of social aspects to optical functioning in society [Thesis] Netherlands: Twente University; 2012. [Google Scholar]
- 24.Reiner M, Niermann C, Jekauc D, Woll A. Long-term health benefits of physical activity–a systematic review of longitudinal studies. BMC Public Health. 2013;13:813. doi: 10.1186/1471-2458-13-813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hallal PC, Andersen LB, Bull FC, et al. Global physical activity levels: surveillance progress, pitfalls, and prospects. The lancet. 2012;380:247–57. doi: 10.1016/S0140-6736(12)60646-1. [DOI] [PubMed] [Google Scholar]
- 26.Lampert T, Kroll LE, von der Lippe E, et al. results of the German Health Interview and Examination Survey for Adults (DEGS1) Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013;56:814–21. doi: 10.1007/s00103-013-1695-4. [DOI] [PubMed] [Google Scholar]
- 27.Chen E, Miller GE. Socioeconomic status and health: mediating and moderating factors. Annual Review of Clinical Psychology. 2013;9:723–49. doi: 10.1146/annurev-clinpsy-050212-185634. [DOI] [PubMed] [Google Scholar]
- 28.Farzi H, Zardoshti Sh, Eidipoor K. The effect of physical activity on social well-being in Kermanshah city. Sport Management. 2015;7:17–30. [In persian] [Google Scholar]
- 29.Cicognani E, Pirini C, Keyes C, et al. Social participation, sense of community and social well being: A study on American, Italian and Iranian university students. Social Indicators Research. 2008;89:97–112. [Google Scholar]