

Abstract
Background:
Recalcitrant sacroiliac joint pain responds well to minimally-invasive surgical (MIS) techniques, although long-term radiographic and fusion data are limited.
Objective:
To evaluate the one-year clinical results from a cohort of patients with chronic sacroiliac (SI) joint pain unresponsive to conservative therapies who have undergone minimally invasive SI joint fusion.
Methods:
SI joint fusion was performed between May 2011 and January 2014. Outcomes included radiographic assessment of fusion status, leg and back pain severity via visual analog scale (VAS), disability via Oswestry Disability Index (ODI) and complication rate. Outcomes were measured at baseline and at follow-up appointments 6 months and 12 months post-procedure.
Results:
Twenty minimally invasive SI joint fusion procedures were performed on 18 patients (mean age: 47.2 (14.2), mean BMI: 29.4 (5.3), 56% female). At 12 months, the overall fusion rate was 88%. Back and leg pain improved from 81.7 to 44.1 points (p<0.001) and from 63.6 to 27.7 points (p=0.001), respectively. Disability scores improved from 61.0 to 40.5 (p=0.009). Despite a cohort containing patients with multiple comorbidities and work-related injuries, eight patients (50%) achieved the minimal clinically important difference (MCID) in back pain at 12 months, with 9 (69%) patients realizing this improvement in leg pain and 8 (57%) realizing the MCID in ODI scores at 12 months. No major complications were reported.
Conclusion:
Minimally invasive SI joint surgery is a safe and effective procedure, with a high fusion rate, a satisfactory safety profile and significant improvements in pain severity and disability reported through 12 months post-procedure.
Keywords: Low back pain, Minimally-invasive surgery, Sacroiliac joint, Sacroiliac joint fusion
INTRODUCTION
Low back pain is one of the most common conditions worldwide, with a lifetime prevalence of up to 40% [1, 2]. It is a common cause of disability and workplace absence [3-5]. despite the estimated $30-61 billion (USD) spent each year in the United States alone on treatments [6, 7]. Clinically, low back pain is challenging to diagnose, as the majority of low back pain presents as non-specific and a large proportion of low back pain cannot be attributed to one specific cause [8]. Patients suffering from low back pain are often subject to multiple diagnostic tests and diagnostic imaging, thus increasing the health care costs associated with this condition [9, 10].
Mechanical low back pain - and specifically sacroiliac (SI) joint dysfunction– comprises between 10-27% of chronic low back pain cases [11-16] and is often treated initially using conservative techniques such as physiotherapy, spinal manipulation, exercise, pharmacologic interventions, intra-articular injections or nerve ablation. While these treatments provide relief, in many cases it is modest and temporary [17]. In cases of chronic SI joint pain (>6 months duration) that do not respond to conservative care, patients may turn to SI joint fusion for relief [18]. Open surgical fusion of the SI joint is an invasive procedure associated with significant disruption of the skeletal structure, bone graft harvesting and instrumental fixation. It is associated with extended hospitalization, lengthy workplace absence, autograft harvest-related morbidity and potential complications such as blood loss and injury to surrounding structures such as neurovascular bundles and musculoligamentous structures [19-22]. Clinical effectiveness and patient safety have improved with the advent of minimally-invasive techniques for surgical SI joint fusion, which lowers patient morbidity and shorten recovery times, but little has been published on long-term clinical and fusion outcomes. One minimally invasive SI joint fusion procedure utilizes a novel decorticator to achieve proper joint preparation in order to promote bone growth and fusion (SImmetry® SI Joint Fusion System, Zyga Technology Inc. Minnetonka, MN, USA) [23]. This study reports one-year clinical results after use of the SImmetry system, with a focus on patient pain, functional ability and radiographic evidence of fusion.
METHODS
Patient Enrollment
Patients undergoing minimally invasive sacroiliac joint fusion at one institution between May 2011 and January 2014 were eligible for inclusion in this study. Patients were deemed eligible and suitable for surgery based on consultation with the treating surgeon. All patients underwent a physical examination of the sacroiliac joint, including orthopedic testing and imaging, and had two diagnostic injections with a minimum of 75% pain relief prior to being deemed a candidate for surgery. Prior to surgery, all patients signed an informed consent form that explained the procedure, its risks and benefits, and were informed that the results of their procedure may be collected for research purposes. Patients had the opportunity to withdraw their consent at any time. All procedures were performed as part of the standard of care and did not involve any investigational procedures or products.
Medical records of eligible patients were retrospectively reviewed by the treating surgeon to extract relevant outcomes and procedural details. Patient data was collected at baseline, 6 weeks post-surgery and then at 3 month intervals up to 12 months post-procedure. Outcome analysis was performed at 6 month and 12 month intervals.
Surgical Procedure
The surgical procedure using decortication and fixation was previously reported in detail by Miller et al. [23]. In brief, under general anaesthesia, patients were positioned prone on the operating table with the pelvis draped for a lateral incision on the buttocks. Anterior, lateral, pelvic inlet, pelvic inlet-oblique, pelvic outlet and pelvic outlet-oblique fluoroscopic views were obtained to localize the affected joint and appropriate landmarks. Access to the sacroiliac joint was gained via a 2 cm incision into which a 6 mm dilator was advanced to the planned entry point on the outer ilium (Fig. 1). A guide pin was inserted through the dilator, drilled into the outer ilium and advanced through the sacroiliac joint space, perpendicular to the plane of the joint, until contact was made with the sacral cortex. An osseous tunnel was created over the guide pin using a 9 mm cannulated drill, with cortical and cancellous shavings collected for later use in the grafting procedure. Debridement of the joint was completed with a novel device made of nitinol and a cutting shaver. The cutting device was advanced into the joint and undulates over the surface as it cuts. Decortication was completed in 3 steps, starting with the ilium and followed by the sacrum and a dual surface decorticating device that prepares the surface as illustrated in Fig. (2). Excess cartilage was cleared from the sacroiliac joint surfaces, followed by denuding of the cartilage and decortication of the joint surfaces utilizing a novel, proprietary decorticator instrument. Approximately 5 cc of bone graft was packed into the denuded cavity to promote bony fusion and fixation of the Fig. (3). A second, anti-rotational implant was placed to provide additional mechanical stability. Multiple views were obtained during and following implantation to confirm proper placement of the implant and the incision was closed using standard surgical techniques. Patients were discharged the same day as their procedure and were instructed to progress to full weight-bearing as tolerated.
Fig. (1).
Representative image of minimally-invasive surgical procedure. Access to the sacroiliac joint is gained through a 2 cm incision into which a 15mm working cannula is inserted to prepare the SI joint and insert implants.
Fig. (2).
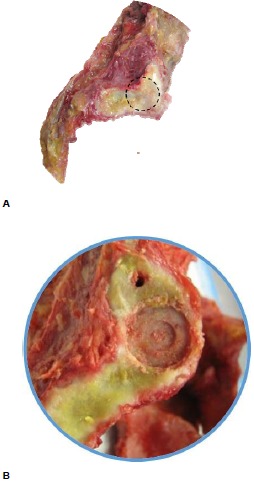
Representative images of decortication during SI joint fusion using the SImmetry joint fusion system. The location on the sacrum is illustrated in (A) (dotted circle). (B) illustrates the sacral margin following decortication.
Fig. (3).
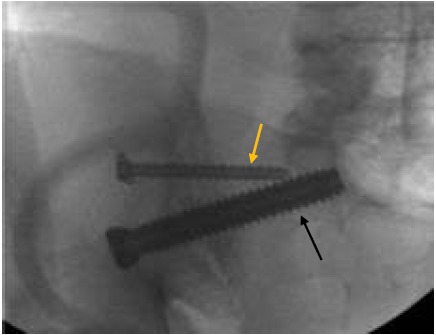
Fluoroscopic image showing SImmetry hardware in situ. Fixation of the joint is achieved with a 12.5 mm implant (black arrow). A second, anti-rotational implant may be placed to provide additional mechanical stability (yellow arrow). Patients are discharged the same day as their procedure with instructions to progress to full weight-bearing as tolerated.
Outcomes
Patient-reported Outcomes
Low back and leg pain severity was reported using the visual analog scale (VAS) ranging from 0 (no pain) to 100 (worst pain imaginable). Patient disability was evaluated using the Oswestry Disability Index (ODI), from 0 (no disability) to 100 (complete disability). Pain and disability scores were collected at baseline (pre-surgery) and at 6 weeks, 3 months, 6 months, 9 months and 12 months post-surgery. The minimal clinically important difference (MCID) in both VAS and ODI scores were determined a priori based on similar clinical studies. MCID for VAS was defined as a reduction of 20 points [24, 25], while the MCID for ODI was set at a reduction of 15 points [26, 27]. Patients were also stratified based on smoking status and body mass index (BMI) and the associated effects on pain and disability were analyzed.
Radiographic Outcomes
Sacroiliac joint fusion was assessed at the 12 month follow-up visit via thin slice (<2mm) CT, viewing four consecutive cuts on both coronal and sagittal reconstructions. Fusion status was defined as radiographic evidence of bony bridging across the sacroiliac joint and the absence of lucency in the joint space in both the coronal and sagittal planes.
Statistical Methods
Alpha was set a priori at 0.05 for all statistical comparisons. Continuous data are reported as mean and standard deviation (SD); categorical data are presented as frequencies and percentages. Means were compared using Student’s t-tests assuming unequal variances. Fusion rates were compared using Fisher’s exact test and/or chi-squared tests, where appropriate. All stated p-values are two-sided.
RESULTS
Twenty (20) procedures were performed on 18 patients, with two patients undergoing bilateral fusion in separate procedures. Patient demographics are summarized in Table 1. The mean age of patients was 47.2 years (SD: 14.2, range: 24-80 years), mean BMI was 29.4 (5.3) and 56% of patients were female. 56% of patients were smokers while 13 reported multiple comorbidities, 7 of whom reported concomitant back conditions including neck pain (n=1), low back pain (n=3), chronic back pain (n=2) or a history of lumbar disc herniation (n=1). One year follow-up data is available for 17 procedures (15 patients), the remaining 3 patients having been lost to follow-up. Data from the last appointment available for patients lost to follow-up was included in the analysis.
Table 1.
Patient demographics.
| All patients (n=18) | |
|---|---|
|
Age (years), mean (SD) BMI, mean (SD) Female, n (%) |
47.2 (14.2) 29.4 (5.3) 10 (56) |
|
Procedure side, % Left Right Length of hospital stay, mean (days) Patients discharged same day as surgery, n (%) Blood loss, mean cc |
55 45 0.3 15 (83) 14.5 |
|
Smoking status, % Current/past smoker Never smoked Work status, n/N (%) Not working at time of surgery Working, modified duties Working, full duties Other (no data, unemployed, etc.) |
56 44 9/18 (50) 3/18 (17) 0/18 (0) 6/18 (33) |
|
Medical history, n/N (%) Concomitant back disease Neck pain Previous lumbar surgery Lumbar fusion Lumbar discectomy/laminectomy |
6/18 (33) 1/18 (6) 4/18 (22) 4/18 (22) |
Procedure
All implant attempts were completed successfully. Mean blood loss was 14.5 cc for all patients, with a mean length of stay of 0.3 days (patients were discharged the same day of surgery in 16 of 20 procedures). No re-operations were required following SI joint implant procedures. Minor complications were reported in 4 procedures. During one procedure, a small portion of the metal cutting tool broke off and remained lodged in the joint cavity. Post-procedure imaging indicated that the piece was well-contained and clinically inconsequential. One patient with a previous, undisclosed history of narcotic dependence and a high opioid tolerance reported uncontrolled pain post-operatively and required an extended (4 days) hospital stay. Finally, in 2 patients, the surgical procedure was prolonged, one due to a dysplastic pelvis and the other as a consequence of the patient’s high BMI. No post-operative complications were reported in either of these patients.
Radiographic Evidence of Fusion
Successful SI joint fusion was observed in 15/17 (88%) procedures at 12 months (16 patients), as determined by CT evaluation of bone bridging the sacroiliac joint. Fusion status at 12-months was not affected by smoking status (smokers: 8/9; non-smokers: 6/7) or BMI (<30: 7/9; >30: 7/7) (Fig. 4).
Fig. (4).
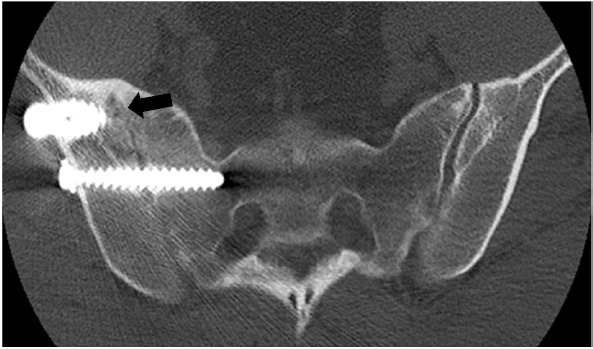
One-year follow-up CT image showing left SI joint fusion. Fusion is visible along the entire length of the SI joint (arrows).
Pain Severity
Both back and leg pain severity showed statistically significant improvement over baseline in all patients at 12 months post-procedure. VAS scores for back and leg pain improved from 81.7 (11.9) to 44.1 (24.2) (p<0.001) and from 63.6 (29.2) to 27.7 (26.8) (p=0.001), respectively (Table 2). The MCID in back pain severity (20 point reduction in VAS) was realized in 8/15 (53%) patients at 12 months. The MCID in leg pain was achieved in 9/13 (69%) patients at 12 months. Of those patients who achieved fusion, 80% (12/15) noted a minimum 20-point improvement in back pain severity, while 67% (10/15) noted this level of improvement in leg pain.
Table 2.
Summary of VAS scores for all participants.
| Baseline | 6 months | 12 months | p-value1 | |
|---|---|---|---|---|
| Back pain VAS, mean (SD) | ||||
| All | 81.7 (15.2) | 40.9 (26.3) | 44.1 (22.9) | <0.0001 |
|
Smokers Non-smokers p-value |
81.5 (17.5) 81.9 (13.0) 0.96 |
46.3 (27.6) 34.8 (25.0) 0.39 |
55.3 (16.7) 31.4 (23.3) 0.04 |
0.004 0.002 |
|
BMI <30 >30 p-value |
83.2 (16.9) 79.0 (12.3) 0.54 |
45.2 (30.8) 34.7 (18.4) 0.40 |
41.8 (26.0) 47.7 (18.9) 0.62 |
0.004 0.008 |
| Leg pain VAS, mean (SD) | ||||
| All | 63.6 (29.2) | 34.4 (33.3) | 27.7 (26.8) | 0.001 |
|
Smokers Non-smokers p-value |
71.3 (25.3) 54.1 (32.2) 0.21 |
40.8 (34.7) 27.1 (29.5) 0.39 |
35.1 (28.0) 19.3 (24.7) 0.26 |
0.01 0.02 |
|
BMI <30 >30 p-value |
65.7 (30.0) 59.6 (29.3) 0.67 |
44.1 (34.0) 20.4 (25.2) 0.11 |
34.4 (27.1) 17.7 (25.3) 0.25 |
0.03 0.02 |
1 Student’s t-test: baseline vs. 12 mos VAS: visual analog scale SD: standard deviation BMI: body mass index
Eleven (11) procedures were performed in 10 patients who identified themselves as smokers, versus 9 procedures (8 patients) in non-smokers. One patient in each group was lost to follow-up. In smokers (all of whom continued to smoke through their final follow-up), back pain severity improved over baseline by 28% (from 81.5 (17.5) to 55.3 (16.7), p=0.004) at 12 months, as compared with a 61% (from 81.9 (13.0) to 31.4 (23.3), p=0.002) improvement in non-smokers (Table 2). Among smokers, 4/8 (50%) realized the MCID in VAS at 12 months (non-smokers: 4/6, 67%, Fisher’s Exact: 0.627, p>0.05). Although back pain severity improved to a greater degree in non-smokers, the difference between smokers and non-smokers was not statistically significant (p=0.06).
Eleven (11) patients had a BMI <30 while 7 patients had a BMI >30 (2 were lost to follow-up). BMI had no impact on improvements in back or leg pain severity at 12 months, with both subsets of patients demonstrating statistically significant improvements over baseline (Table 2). All patients with a BMI >30 realized the MCID in leg pain severity at 12 months (5/5), while 4/8 of patients with a BMI <30 realized this level of improvement (Fisher’s exact: 0.104, p>0.05).
Disability
Patient disability improved significantly at 12 months post-procedure (Table 3). ODI scores improved from 61.0 (14.0) to 40.5 (22.0) (p=0.009) at 12 months, with 8/14 (57%) patients realizing the MCID in ODI scores (15 point reduction) at 12 months.
Table 3.
Summary of disability (ODI) scores for all participants.
| Baseline | 6 months | 12 months | p-value1 | |
|---|---|---|---|---|
| ODI score, mean (SD) | ||||
| All | 61.0 (14.0) | 39.1 (20.8) | 40.5 (22.0) | 0.009 |
|
Smokers Non-smokers p-value |
63.5 (15.0) 57.9 (12.9) 0.38 |
44.7 (18.5) 32.8 (22.7) 0.26 |
50.8 (18.6) 28.9 (20.7) 0.054 |
0.14 0.02 |
|
BMI <30 >30 p-value |
62.6 (16.5) 57.9 (7.9) 0.40 |
46.0 (19.9) 29.1 (19.2) 0.10 |
41.1 (25.2) 39.7 (18.6) 0.90 |
0.08 0.06 |
1 Student’s t-test: baseline vs. 12 mos ODI: Oswestry disability index SD: standard deviation BMI: body mass index
Improvements in disability scores were generally greater in non-smokers, although, as with pain severity, the difference between the two groups at 12 months post-procedure approached but did not reach statistical significance (p=0.08) (Table 3). Smokers demonstrated only a 19% improvement (from 63.5 (15.0) to 50.1 (18.6), p=0.14) over baseline in ODI scores at 12 months, while non-smokers demonstrated a 50% improvement (from 57.9 (12.9) to 28.9 (20.7), p=0.02). The proportion of patients realizing the MCID in ODI scores was similar in smokers and non-smokers at 12 months (smokers: 3/8, non-smokers: 3/6) (Fisher’s exact: 1.00, p>0.05). In patients who achieved fusion, 60% (9/15) realized a minimum 15-point improvement in ODI scores.
BMI did not affect improvements in disability at 12 months post-procedure (Table 3). The MCID was realized in similar proportions of patients across BMI measurements at 12 months (<30: 5/8; >30: 3/6; Fisher’s exact: 1.00, p>0.05).
DISCUSSION
Surgical fusion of the SI joint has been used for over a century, with open surgical procedures commonly performed beginning in the early 1900s [28, 29]. Open fusion requires large incisions, significant bone harvesting and lengthy hospital stays [21, 30], while providing lesser improvements in pain and dysfunction than minimally-invasive (MIS) procedures [31, 33]. In comparison, MIS procedures offer improvements over open procedures and conservative treatment from both the clinical and cost-effectiveness perspectives [34, 35].
MIS options for SI joint fusion have demonstrated comparable fusion rates with open fusion procedures, with fusion rates above 80% reported for both open [21, 36] and MIS [37, 38] procedures. Improvements in pain severity associated with MIS procedures have been noted to be equivalent to that of open procedures, with MIS fusion often demonstrating superiority over open fusion [31, 33]. In a recent comparison, MCID improvements in pain severity were reported in 86% of patients undergoing an MIS procedure, as compared with 61% undergoing open fusion [31]. Similar studies have demonstrated MCID improvements in disability ranging from 82% [32, 33] to 90% [28] in MIS procedures, far surpassing the results from open fusion (45%) [33]. We noted an 80% rate of MCID improvements in back pain in patients who achieved fusion at 12 months.
In this study, an 88% fusion rate at 12 months post-procedure and statistically significant improvements in back pain, leg pain and disability at both 6 months and 12 months post-procedure were observed, results which were comparable to other MIS procedures for SI joint fusion [28]. Our observed fusion rate was greater than that of similar studies and occurred within a shorter timeframe [39]. While the VAS improvements noted in our study were less than other studies, there were several confounding factors among the patients in our cohort. Eight patients in our study reported prior low back surgery and 10 were injured at work. While a history of lumbar surgery had no significant impact on pain or disability levels, a sensitivity analysis revealed that those patients who suffered their injury at work had significantly worse results, especially in leg pain severity. Patients who did not suffer their injury at work noted a mean improvement in leg pain of 85.2% at 12 months, compared to those who suffered their injury at work, who reported a mean improvement of only 49.3%. Injured workers are known to have generally poor results when compared with those who were not injured at work [40-42]. This was confirmed in our study. That this cohort was comprised of a majority of patients whose injury was work-related may explain the slightly lesser improvements in VAS scores as compared with other studies [43].
It is noteworthy that the rates of long-term fusion and pain relief observed in this study were achieved utilizing a fusion system that requires only two cannulated screws to stabilize and fuse the SI joint, in contrast to other MIS systems that require multiple implants, often impacted across the joint, to provide the necessary stabilization [28, 39, 44]. The use of only 2 cannulated screws further minimizes the invasiveness of the procedure, requiring a smaller incision than other MIS systems and eliminating the need for iliac crest bone grafting, as bone shavings collected during implantation process are collected and used as the bone graft material during the fusion procedure. Additionally, 15 of 18 patients were discharged on the same day as their procedure using the SImmetry system, resulting in a shorter mean length of stay than other MIS systems [45]. These data are in contrast with other MIS procedures or open fusion, which routinely require a hospital stay of 1 to 5 days [31, 45, 46].
The effect of smoking status, while not statistically significant, demonstrated a trend towards greater improvements in both pain and disability in non-smokers at 12 months. Previous studies have found that smokers realize lesser improvements in pain and disability in fusion procedures [47, 48]. We observed similar findings, with smokers realizing improvements in pain or disability at significantly lower rates than those of non-smokers. Interestingly, while smoking has been shown previously [47, 48] and in our study to adversely affect pain and healing, there is no evidence to indicate that smoking slows or decreases the likelihood of fusion [49, 50]. The data presented here support this observation, as there was no significant difference between the 12-month fusion rate in the smoking and non-smoking groups.
BMI played a role in pain relief, with patients with a BMI >30 demonstrating a significant improvement in leg pain, as compared with those with a BMI <30. All patients, regardless of BMI, demonstrated statistically significant improvements at 12 months in both back and leg pain severity, although the reductions in VAS scores for leg pain recorded at 12 months were significantly greater for those with a BMI >30. The proportion of patients achieving the MCID in leg pain was also higher in the BMI >30 group, with 100% of patients realizing this level of improvement at both 6 months and 12 months post-procedure. Having a BMI of >30 has been implicated as a risk factor for sacroiliac joint pain [51, 52], as there are increased forces exerted on the SI joints, resulting in increased pain and dysfunction. As leg pain is a common symptom of SI joint dysfunction, fusion of the joint in patients with a BMI >30 may serve to eliminate the pain-generating mechanism, resulting in substantial pain relief.
The rate of complication in our study was extremely low, with no re-operations required and only 4 patients experiencing procedural complications. Complications in open procedures have been reported as high as 21% and include post-operative infection, pulmonary embolism and surgical revision [53]. Our observed complication rate is comparable with other MIS fusion systems, which have reported minor complications in comparable percentages of patients as compared with open fusion. No additional complications were reported in our cohort at 12-month follow-up.
CONCLUSION
This study demonstrates the safety and clinical effectiveness of the SImmetry SI joint fusion system for chronic, recalcitrant SI joint pain and demonstrates that the SImmetry system is associated with significant improvements in back and leg pain and in patient disability. Outcomes were comparable with those of alternate MIS procedures, despite the presence of multiple comorbidities and a high proportion (56%) of workers’ compensation patients, who are known to have poor results regarding post-surgical pain relief. The wide variation of comorbidities made stratification impossible; however, the fact that a majority of patients suffered from concurrent conditions yet were still able to realize improvements reflects the overall effectiveness of the SImmetry system. Future studies will focus on larger cohorts which will enable stratification based on comorbidity and better characterization of the effectiveness of the system in patients with comorbid conditions.
ACKNOWLEDGEMENTS
Declared none.
CONFLICT OF INTEREST
The authors confirm that this article content has no conflict of interest.
REFERENCES
- 1.Hoy D., Bain C., Williams G., March L., Brooks P., Blyth F., Woolf A., Vos T., Buchbinder R. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–2037. doi: 10.1002/art.34347. [DOI] [PubMed] [Google Scholar]
- 2.Hoy D., Brooks P., Blyth F., Buchbinder R. The Epidemiology of low back pain. Best Pract. Res. Clin. Rheumatol. 2010;24(6):769–781. doi: 10.1016/j.berh.2010.10.002. [DOI] [PubMed] [Google Scholar]
- 3.Kuijer W., Groothoff J.W., Brouwer S., Geertzen J.H., Dijkstra P.U. Prediction of sickness absence in patients with chronic low back pain: a systematic review. J. Occup. Rehabil. 2006;16(3):439–467. doi: 10.1007/s10926-006-9021-8. [DOI] [PubMed] [Google Scholar]
- 4.Reiso H., Nygård J.F., Jørgensen G.S., Holanger R., Soldal D., Bruusgaard D. Back to work: predictors of return to work among patients with back disorders certified as sick: a two-year follow-up study. Spine. 2003;28(13):1468–1473. doi: 10.1097/01.BRS.0000067089.83472.1F. [DOI] [PubMed] [Google Scholar]
- 5.Wynne-Jones G., Cowen J., Jordan J.L., Uthman O., Main C.J., Glozier N., van der Windt D. Absence from work and return to work in people with back pain: a systematic review and meta-analysis. Occup. Environ. Med. 2014;71(6):448–456. doi: 10.1136/oemed-2013-101571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Soni A. Back problems: Use and expenditures for the U.S. adult population, 2007. 2010. [cited 2015 June 25]. Available from: http://www.meps.ahrq.gov/data_files/publications/st289/stat289.pdf .
- 7.Stewart W.F., Ricci J.A., Chee E., Morganstein D., Lipton R. Lost productive time and cost due to common pain conditions in the US workforce. JAMA. 2003;290(18):2443–2454. doi: 10.1001/jama.290.18.2443. [DOI] [PubMed] [Google Scholar]
- 8.van Tulder M.W., Assendelft W.J., Koes B.W., Bouter L.M. Spinal radiographic findings and nonspecific low back pain. A systematic review of observational studies. Spine. 1997;22(4):427–434. doi: 10.1097/00007632-199702150-00015. [DOI] [PubMed] [Google Scholar]
- 9.Braun J., Baraliakos X., Regel A., Kiltz U. Assessment of spinal pain. Best Pract. Res. Clin. Rheumatol. 2014;28(6):875–887. doi: 10.1016/j.berh.2015.04.031. [DOI] [PubMed] [Google Scholar]
- 10.Heidari P., Farahbakhsh F., Rostami M., Noormohammadpour P., Kordi R. The role of ultrasound in diagnosis of the causes of low back pain: a review of the literature. Asian J. Sports Med. 2015;6(1):e23803. doi: 10.5812/asjsm.23803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Katz V., Schofferman J., Reynolds J. The sacroiliac joint: a potential cause of pain after lumbar fusion to the sacrum. J. Spinal Disord. Tech. 2003;16(1):96–99. doi: 10.1097/00024720-200302000-00015. [DOI] [PubMed] [Google Scholar]
- 12.DePalma MJ, Ketchum JM, Saullo T. What is the source of chronic low back pain and does age play a role? Pain medicine (Malden, Mass). 2011;12(2):224–33. doi: 10.1111/j.1526-4637.2010.01045.x. [DOI] [PubMed] [Google Scholar]
- 13.Maigne J.Y., Aivaliklis A., Pfefer F. Results of sacroiliac joint double block and value of sacroiliac pain provocation tests in 54 patients with low back pain. Spine. 1996;21(16):1889–1892. doi: 10.1097/00007632-199608150-00012. [DOI] [PubMed] [Google Scholar]
- 14.Schwarzer A.C., Aprill C.N., Bogduk N. The sacroiliac joint in chronic low back pain. Spine. 1995;20(1):31–37. doi: 10.1097/00007632-199501000-00007. [DOI] [PubMed] [Google Scholar]
- 15.Bernard T.N., Jr, Kirkaldy-Willis W.H. Recognizing specific characteristics of nonspecific low back pain. Clin. Orthop. Relat. Res. 1987;(217):266–280. [PubMed] [Google Scholar]
- 16.Rupert M.P., Lee M., Manchikanti L., Datta S., Cohen S.P. Evaluation of sacroiliac joint interventions: a systematic appraisal of the literature. Pain Physician. 2009;12(2):399–418. [PubMed] [Google Scholar]
- 17.Hansen H., Manchikanti L., Simopoulos T.T., Christo P.J., Gupta S., Smith H.S., Hameed H., Cohen S.P. A systematic evaluation of the therapeutic effectiveness of sacroiliac joint interventions. Pain Physician. 2012;15(3):E247–E278. [PubMed] [Google Scholar]
- 18.Ashman B., Norvell D.C., Hermsmeyer J.T. Chronic sacroiliac joint pain: fusion versus denervation as treatment options. Evid. Based Spine Care J. 2010;1(3):35–44. doi: 10.1055/s-0030-1267066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dabezies E.J., Millet C.W., Murphy C.P., Acker J.H., Robicheaux R.E., DAmbrosia R.D. Stabilization of sacroiliac joint disruption with threaded compression rods. Clin. Orthop. Relat. Res. 1989;(246):165–171. [PubMed] [Google Scholar]
- 20.Simpson L.A., Waddell J.P., Leighton R.K., Kellam J.F., Tile M. Anterior approach and stabilization of the disrupted sacroiliac joint. J. Trauma. 1987;27(12):1332–1339. doi: 10.1097/00005373-198712000-00003. [DOI] [PubMed] [Google Scholar]
- 21.Buchowski J.M., Kebaish K.M., Sinkov V., Cohen D.B., Sieber A.N., Kostuik J.P. Functional and radiographic outcome of sacroiliac arthrodesis for the disorders of the sacroiliac joint. Spine J. 2005;5(5):520–528. doi: 10.1016/j.spinee.2005.02.022. [DOI] [PubMed] [Google Scholar]
- 22.Schütz U., Grob D. Poor outcome following bilateral sacroiliac joint fusion for degenerative sacroiliac joint syndrome. Acta Orthop. Belg. 2006;72(3):296–308. [PubMed] [Google Scholar]
- 23.Miller L.E., Block J.E. Minimally invasive arthrodesis for chronic sacroiliac joint dysfunction using the SImmetry SI Joint Fusion system. Med. Devices (Auckl.) 2014;7:125–130. doi: 10.2147/MDER.S63575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hagg O, Fritzell P, Nordwall A. The clinical importance of changes in outcome scores after treatment for chronic low back pain. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2003;12(1):12–20. doi: 10.1007/s00586-002-0464-0. [DOI] [PubMed] [Google Scholar]
- 25.Mannion A.F., Balagué F., Pellisé F., Cedraschi C. Pain measurement in patients with low back pain. Nat. Clin. Pract. Rheumatol. 2007;3(11):610–618. doi: 10.1038/ncprheum0646. [DOI] [PubMed] [Google Scholar]
- 26.Copay A.G., Glassman S.D., Subach B.R., Berven S., Schuler T.C., Carreon L.Y. Minimum clinically important difference in lumbar spine surgery patients: a choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and pain scales. Spine J. 2008;8(6):968–974. doi: 10.1016/j.spinee.2007.11.006. [DOI] [PubMed] [Google Scholar]
- 27.Ostelo R.W., Deyo R.A., Stratford P., Waddell G., Croft P., Von Korff M., Bouter L.M., de Vet H.C. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90–94. doi: 10.1097/BRS.0b013e31815e3a10. [DOI] [PubMed] [Google Scholar]
- 28.Cummings J., Jr, Capobianco R.A. Minimally invasive sacroiliac joint fusion: one-year outcomes in 18 patients. Ann. Surg. Innov. Res. 2013;7(1):12. doi: 10.1186/1750-1164-7-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Smith-Petersen M.N. Arthrodesis of the sacroiliac joint. A new method of approach. J. Bone Joint Surg. Am. 1921;3(8):400–405. [Google Scholar]
- 30.Giannikas KA, Khan AM, Karski MT, Maxwell HA. Sacroiliac joint fusion for chronic pain: a simple technique avoiding the use of metalwork. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2004;13(3):253–6. doi: 10.1007/s00586-003-0620-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Smith A.G., Capobianco R., Cher D., Rudolf L., Sachs D., Gundanna M., Kleiner J., Mody M.G., Shamie A.N. Open versus minimally invasive sacroiliac joint fusion: a multi-center comparison of perioperative measures and clinical outcomes. Ann. Surg. Innov. Res. 2013;7(1):14. doi: 10.1186/1750-1164-7-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ledonio C.G., Polly D.W., Jr, Swiontkowski M.F. Minimally invasive versus open sacroiliac joint fusion: are they similarly safe and effective? Clin. Orthop. Relat. Res. 2014;472(6):1831–1838. doi: 10.1007/s11999-014-3499-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ledonio C.G., Polly D.W., Jr, Swiontkowski M.F., Cummings J.T., Jr Comparative effectiveness of open versus minimally invasive sacroiliac joint fusion. Med. Devices (Auckl.) 2014;7:187–193. doi: 10.2147/MDER.S60370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ackerman S.J., Polly D.W., Jr, Knight T., Schneider K., Holt T., Cummings J. Comparison of the costs of nonoperative care to minimally invasive surgery for sacroiliac joint disruption and degenerative sacroiliitis in a United States Medicare population: potential economic implications of a new minimally-invasive technology. Clinicoecon. Outcomes Res. 2013;5:575–587. doi: 10.2147/CEOR.S52967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ackerman S.J., Polly D.W., Jr, Knight T., Schneider K., Holt T., Cummings J., Jr Comparison of the costs of nonoperative care to minimally invasive surgery for sacroiliac joint disruption and degenerative sacroiliitis in a United States commercial payer population: potential economic implications of a new minimally invasive technology. Clinicoecon. Outcomes Res. 2014;6:283–296. doi: 10.2147/CEOR.S63757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Moore M.R. Surgical treatment of chronic painful sacroiliac joint dysfunction. Movement, stability, and low back pain: the essential role of the pelvis. New York: Churchill Livingstone; 1997. pp. 563–572. [Google Scholar]
- 37.Khurana A., Guha A.R., Mohanty K., Ahuja S. Percutaneous fusion of the sacroiliac joint with hollow modular anchorage screws: clinical and radiological outcome. J. Bone Joint Surg. Br. 2009;91(5):627–631. doi: 10.1302/0301-620X.91B5.21519. [DOI] [PubMed] [Google Scholar]
- 38.Wise C.L., Dall B.E. Minimally invasive sacroiliac arthrodesis: outcomes of a new technique. J. Spinal Disord. Tech. 2008;21(8):579–584. doi: 10.1097/BSD.0b013e31815ecc4b. [DOI] [PubMed] [Google Scholar]
- 39.Rudolf L., Capobianco R. Five-year clinical and radiographic outcomes after minimally invasive sacroiliac joint fusion using triangular implants. Open Orthop. J. 2014;8:375–383. doi: 10.2174/1874325001408010375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Harris I.A., Dantanarayana N., Naylor J.M. Spine surgery outcomes in a workers compensation cohort. ANZ J. Surg. 2012;82(9):625–629. doi: 10.1111/j.1445-2197.2012.06152.x. [DOI] [PubMed] [Google Scholar]
- 41.Anderson J.T., Haas A.R., Percy R., Woods S.T., Ahn U.M., Ahn N.U. Single-level lumbar fusion for degenerative disc disease is associated with worse outcomes compared with fusion for spondylolisthesis in a workers compensation setting. Spine. 2015;40(5):323–331. doi: 10.1097/BRS.0000000000000734. [DOI] [PubMed] [Google Scholar]
- 42.Nguyen T.H., Randolph D.C., Talmage J., Succop P., Travis R. Long-term outcomes of lumbar fusion among workers compensation subjects: a historical cohort study. Spine. 2011;36(4):320–331. doi: 10.1097/BRS.0b013e3181ccc220. [DOI] [PubMed] [Google Scholar]
- 43.Polly D.W., Cher D.J., Wine K.D., Whang P.G., Frank C.J., Harvey C.F., Lockstadt H., Glaser J.A., Limoni R.P., Sembrano J.N., INSITE Study Group Randomized Controlled Trial of Minimally Invasive Sacroiliac Joint Fusion Using Triangular Titanium Implants vs Nonsurgical Management for Sacroiliac Joint Dysfunction: 12-Month Outcomes. Neurosurgery. 2015;77(5):674–690. doi: 10.1227/NEU.0000000000000988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Whang P., Cher D., Polly D., Frank C., Lockstadt H., Glaser J., Limoni R., Sembrano J. Sacroiliac Joint Fusion Using Triangular Titanium Implants vs. Non-Surgical Management: Six-Month Outcomes from a Prospective Randomized Controlled Trial. Int. J. Spine Surg. 2015;9:6. doi: 10.14444/2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Sachs D., Capobianco R., Cher D., Holt T., Gundanna M., Graven T., Shamie A.N., Cummings J., Jr One-year outcomes after minimally invasive sacroiliac joint fusion with a series of triangular implants: a multicenter, patient-level analysis. Med. Devices (Auckl.) 2014;7:299–304. doi: 10.2147/MDER.S56491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Duhon B.S., Cher D.J., Wine K.D., Lockstadt H., Kovalsky D., Soo C.L. Safety and 6-month effectiveness of minimally invasive sacroiliac joint fusion: a prospective study. Med. Devices (Auckl.) 2013;6:219–229. doi: 10.2147/MDER.S55197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Alkherayf F., Agbi C. Cigarette smoking and chronic low back pain in the adult population. Clin. Invest. Med. 2009;32(5):E360–E367. doi: 10.25011/cim.v32i5.6924. [DOI] [PubMed] [Google Scholar]
- 48.Behrend C., Prasarn M., Coyne E., Horodyski M., Wright J., Rechtine G.R. Smoking Cessation Related to Improved Patient-Reported Pain Scores Following Spinal Care. J. Bone Joint Surg. Am. 2012;94(23):2161–2166. doi: 10.2106/JBJS.K.01598. [DOI] [PubMed] [Google Scholar]
- 49.Luszczyk M., Smith J.S., Fischgrund J.S., Ludwig S.C., Sasso R.C., Shaffrey C.I., Vaccaro A.R. Does smoking have an impact on fusion rate in single-level anterior cervical discectomy and fusion with allograft and rigid plate fixation? Clinical article. J. Neurosurg. Spine. 2013;19(5):527–531. doi: 10.3171/2013.7.SPINE13208. [DOI] [PubMed] [Google Scholar]
- 50.Lee T.C., Ueng S.W., Chen H.H., Lu K., Huang H.Y., Liliang P.C., Su T.M., Yang L.C. The effect of acute smoking on spinal fusion: an experimental study among rabbits. J. Trauma. 2005;59(2):402–408. doi: 10.1097/01.ta.0000174918.38764.00. [DOI] [PubMed] [Google Scholar]
- 51.Irwin RW, Watson T, Minick RP, Ambrosius WT. Age, body mass index, and gender differences in sacroiliac joint pathology. Am. J. Phy. Med. & Rehab./Associat. Acad. Physiatr. 2007;86(1):37–44. doi: 10.1097/PHM.0b013e31802b8554. [DOI] [PubMed] [Google Scholar]
- 52.Essential J. What is Sacroiliac Joint Dysfunction (SI Joint Pain)? 2013. [cited 2015 July 07]. Available from: http://www.jointessential.com/ what-is-sacroiliac-joint-dysfunction-si-joint-pain/
- 53.Kibsgård T.J., Røise O., Stuge B. Pelvic joint fusion in patients with severe pelvic girdle pain - a prospective single-subject research design study. BMC Musculoskelet. Disord. 2014;15:85. doi: 10.1186/1471-2474-15-85. [DOI] [PMC free article] [PubMed] [Google Scholar]