

Introduction
Lactococcus garvieae, originally a fish pathogen, has very rarely been isolated from human infections, mainly infective endocartditis.1, 2, 3 Most of the patients in the reported cases of human infections had a positive history of contact with raw fish. Another common factor, which was seen to be present in some patients of L. garvieae infection was valvular damage. This organism often misidentified as Enterococcus spp. because of its morphological and biochemical similarities.4
In this case report, we describe a rare case of meningitis caused by L. garvieae, in the absence of endocarditis, in an immunocompetent patient, who presented as a suspected case of posterior circulation stroke with no past history of contact with raw fish.
Case report
A 75 year old male, chronic alcoholic patient presented with history of progressive fatigue, weight loss and anorexia of 30 days duration. He also gave history of low grade, intermittent fever associated with disorientation in time and place for last 4 days. On examination, he was found to be drowsy, but arousable, had neck rigidity, weakness of the right side of body and a Glasgow Coma Scale (GCS) score of 12/15 (E4V3M5). Non-contrast computed tomography (NCCT) of brain was normal. Cerebrospinal fluid (CSF) examination revealed 50 WBCs/μl with predominant lymphocytes (75%), glucose level was 48 mg/dl and increased globulins which was suggestive of chronic meningitis.
CSF culture was done according to the standard protocol. After incubation at 37 °C for 24 h, blood agar showed small to medium-sized colonies with a smooth and shiny surface with no haemolysis (Fig. 1). Gram stain revealed Gram-positive cocci predominantly in pairs and occasionally in chains. With this morphology, negative catalase test, positive PYRase and bile esculin test, the organism was presumptively identified as Enterococcus spp. However, the isolate was identified as L. garvieae by Vitek-2 (Biomerieux, France) automated identification system with more than 99% probability. Later, more biochemical tests were carried out to confirm the finding of Vitek-2. Sorbitol fermentation test was performed on Andrade's carbohydrate broth and indicator, which was negative for the test organism but positive with Enterococcus faecalis ATCC 29212. The isolate was also tested on the Bruker (Bruker Daltonics) matrix assisted laser desorption ionization–time of flight mass spectrometer (MALDI-TOF MS). This new and highly specific instrument identified the organism as L. garvieae with a score of 2.096, representing a good identification.
Fig. 1.
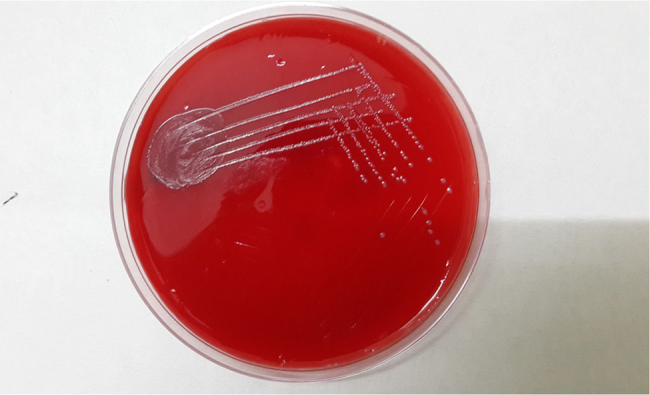
Growth of L. garvieae on blood agar plate.
As Clinical and Laboratory Standards Institute (CLSI) guidelines for performing antibiotic susceptibility testing for L. garvieae are not available, we performed the antibiotic susceptibility testing by Kirby–Bauer disc diffusion method and interpreted the results according to CLSI guidelines recommended for Enterococcus spp. It was found that the isolate was susceptible to erythromycin, gentamicin, tetracycline, doxycycline, vancomycin, teicoplanin and linezolid and resistant to amikacin, chloramphenicol, ciprofloxacin, levofloxacin and clindamycin.
Blood and urine cultures, CSF fungal culture and PCR for Mycobacterium tuberculosis were negative.
The patient was managed in ICU with Injection Vancomycin and Ceftriaxone, after which he showed clinical improvement within 3–4 days. He was finally discharged after 7 days of indoor management and observation.
Discussion
The genus Lactococcus was separated from the genus Streptococcus in 1985 on the basis of genetic analysis, and is still frequently misidentified as a variant of Enterococcus spp.5 The genus Lactococcus contains eight species and subspecies, of which the most common species involved in human infections are Lactococcus lactis and L. garvieae.6 Since an increasing number of human infections due to L. garvieae have been reported in recent times, this organism has gained recognition as an emerging zoonotic pathogen.2, 3, 4, 5, 6 One probable reason for its increasing reports might be availability of advanced bacterial identification techniques. A total of 21 cases of L. garvieae with clinical details have been reported in the literature7; most of which were suffering from endocarditis. The present case is probably the first of its kind, as the organism was isolated from CSF of a patient suffering from meningitis.
Initially the isolate was wrongly identified as Enterococcus spp., based on colony morphology, Gram stain, catalase and esculin hydrolysis test. The isolate was further tested by Vitek automated system, which identified the organism as L. garvieae with more than 99% probability. After this report we carried out more biochemical tests for L. garvieae to confirm the finding of Vitek system. The isolate was sent to a reference centre for final confirmation by Bruker (Bruker Daltonics) matrix assisted laser desorption ionization–time of flight mass spectrometer (MALDI-TOF MS). This new and highly specific instrument identified the organism as L. garvieae with a score of 2.096, showing a good identification.
Colonies on blood agar were nonhaemolytic, white and shiny. PYRase test was positive, and the isolate grew at 45 °C as well as at room temperature. It grew in the presence of 6.5% NaCl and was able to hydrolyze esculin. Sorbitol fermentation test was carried out using Andrade's carbohydrate broth, which showed that the test organism did not utilize sorbitol, whereas it was fermented by Enterococcus faecalis control strain (E. faecalis ATCC 29212).
As Clinical Laboratory Standards Institute (CLSI) guidelines for performing antibiotic sensitivity testing (ABST) for L. garvieae are not available, we performed the ABST by Kirby Bauer disc diffusion method and interpreted the results as per Enterococcus spp. guidelines. It was found to be resistant to amikacin, chloramphenicol, ciprofloxacin, levofloxacin and clindamycin and sensitive to remaining antibiotics tested.
To summarize, human infections caused by L. garvieae are extremely rare, the most common manifestation being infective endocarditis. Our case report is the first case of meningitis, which presented initially as a case resembling cerebral stroke.
Conflicts of interest
The authors have none to declare.
References
- 1.Texeira L., Maerquior V., Vianni M. Phenotypic and genotypic characterization of atypical Lactococcus garvieae strains isolated from water buffalos with subclinical mastitis and confirmation of L. garvieae as a senior subjective synonym of Enterococcus seriolicida. Int J Syst Bacteriol. 1996;46:664–668. doi: 10.1099/00207713-46-3-664. [DOI] [PubMed] [Google Scholar]
- 2.Yiu K.H., Siu C.W., To K.K. A rare cause of infective endocarditis; Lactococcus garvieae. Int J Cardiol. 2007;114:286–287. doi: 10.1016/j.ijcard.2005.11.092. [DOI] [PubMed] [Google Scholar]
- 3.Wang C.Y., Shie H.S., Chen S.C. Lactococcus garvieae infections in humans: possible association with aquaculture outbreaks. Int J Clin Pract. 2007;61:68–73. doi: 10.1111/j.1742-1241.2006.00855.x. [DOI] [PubMed] [Google Scholar]
- 4.Li W.K., Chen Y.S., Wann S.R., Liu Y.C., Tsai H.C. Lactococcus garvieae endocarditis with initial presentation of acute cerebral infarction in a healthy immunocompetent man. Intern Med. 2008;47:1143–1146. doi: 10.2169/internalmedicine.47.0795. [DOI] [PubMed] [Google Scholar]
- 5.Vinh D.C., Nichol K.A., Rand F., Embil J.M. Native-valve bacterial endocarditis caused by Lactococcus garvieae. Diagn Microbiol Infect Dis. 2006;56(1):91–94. doi: 10.1016/j.diagmicrobio.2006.02.010. [DOI] [PubMed] [Google Scholar]
- 6.Fihman V., Raskine L., Barrou Z. Lactococcus garvieae endocarditis: identification by 16S rRNA and sodA sequence analysis. J Infect. 2006;52(1):e3–e6. doi: 10.1016/j.jinf.2005.04.021. [DOI] [PubMed] [Google Scholar]
- 7.Gianluca R., Marco I., Alessandra D. Lactococcus garvieae endocarditis in a patient with colonic diverticulosis: first case report in Italy and review of the literature. New Microbiol. 2012;35:495–501. [PubMed] [Google Scholar]