

Abstract
Background
Pain is a major limiting factor in patient’s recovery from major thoracic surgical procedures. Thoracic epidural analgesia (TEA), the current gold standard of perioperative management, has contraindications, can technically fail, and carries a risk of complications such as epidural abscess and spinal hematoma. The ultrasound-guided serratus anterior plane (SAP) block is a promising regional analgesia technique.
Objectives
Since the anatomic space involved in the SAP block corresponds to the area exposed by the surgeon during right posterolateral thoracotomy, we investigated the feasibility of a “surgically guided” continuous SAP block as an alternative to TEA in selected esophagectomy patients.
Study design
This was a pilot case-series study.
Setting
This study was carried out in a tertiary-care university hospital.
Methods
The demographic and clinical data of patients in whom the continuous SAP block was performed were retrieved from a prospectively maintained database of hybrid (laparoscopy plus right thoracotomy) Ivor Lewis esophagectomy. The SAP block was performed upon closure of the thoracotomy incision using a 19-gauge catheter tunnelized subcutaneously and positioned in the deep plane between the serratus anterior muscle and the ribs. A bolus dose of 30 mL of levobupivacaine 0.25% was injected, followed by a continuous infusion of the 0.125% solution at 7 mL/h until postoperative day 4.
Results
Between January 2016 and July 2016, seven (20%) out of 37 esophagectomy patients underwent a SAP block rather than TEA for the following reasons: inability to insert the epidural catheter, antiaggregation or anticoagulant therapy, or unplanned thoracotomy. The procedure was uneventful in all patients. Only two patients required rescue analgesia on day 1.
Conclusion
Continuous SAP block under direct vision is feasible and safe. This novel “surgically guided” application of the SAP block may be useful in case of failure or contraindications to TEA.
Keywords: serratus anterior block, thoracic epidural anesthesia, post-thoracotomy pain, esophageal carcinoma, transthoracic esophagectomy
Introduction
Esophagectomy is one of the most complex surgical procedures and carries a high risk of perioperative morbidity. Suboptimal pain management is a recognized risk factor for respiratory complications after transthoracic esophagectomy.1 Thoracic epidural analgesia (TEA) is the current gold-standard analgesia in these patients and is an important component of the fast-track programs.2–4 However, TEA cannot always be performed and other strategies of pain relief need to be considered in select patients. The serratus anterior plane (SAP) block provides a prolonged anesthesia of the hemithorax with numbness over the thoracic area supplied by the lateral cutaneous branches of the T2–T9 spinal nerves. An ultrasound-guided SAP block has been recently described and employed mainly in breast surgery.5 Ultrasound-guided SAP block has also been reported for post-thoracotomy pain.6,7
The aim of this pilot study was to describe a novel technique of “surgically guided” application of the SAP block in patients undergoing hybrid minimally invasive transthoracic esophagectomy.
Methods
The demographic and clinical data of patients in whom the continuous SAP block was performed were retrieved from the prospectively maintained database of esophagectomy for carcinoma at our institution. All patients gave full written informed consent for the anesthesiological and surgical procedures and for using data and images. The study was approved by the internal review board at IRCCS Policlinico San Donato, University of Milano.
The esophagectomy is conducted under a balanced anesthesia technique using remifentanil and desflurane. Protective mechanical ventilation combined with lung recruitment strategy and a perioperative goal-directed therapy is applied. The surgical procedure consists of two steps. First, through a five-port laparoscopic approach, supramesocolic lymphadenectomy and stapled gastric tubulization are performed. Second, a right posterolateral thoracotomy is performed; the latissimus dorsi muscle is transected, and the serratus anterior muscle with its vascular pedicle is carefully preserved. The pleural cavity is entered through the fifth intercostal space. En bloc esophagectomy is performed, and the esophagogastric anastomosis is created using a circular stapler. The pleural cavity is routinely drained using a Blake tube exiting the upper abdominal port.
Upon closure of the rib cage, a peripheral nerve block catheter set (Contiplex Tuohy or Arrow StimuCath) is used to perform the continuous SAP block. A 19-gauge catheter, 60–100 cm long, is tunnelized subcutaneously through a Tuohy needle and positioned in the deep plane between the serratus anterior muscle and the ribs (Figures 1A and B and 2). After repair of the latissimus dorsi muscle, a bolus dose of 30 mL of levobupivacaine 0.25% is injected, followed by a continuous infusion of the 0.125% solution at 7 mL/h. The dose is then reduced to 5 mL/h on postoperative day (POD) 3 and to 3 mL/h on POD 4. For abdominal pain control, intravenous acetaminophen 1 g and morphine 0.1 mg/kg are administered before emergence from anesthesia. The same pain management protocol used for TEA is applied: intravenous acetaminophen 1 g every 8 hours and remifentanil 0.03–0.05 mcg/kg/min, with ketorolac 30 mg as rescue if visual analog scale (VAS) >40, are given on POD 1. Titration of remifentanil doses is used for breakthrough pain. On PODs 2 and 3, only acetaminophen 1 g every 8 hours and ketorolac 30 mg every 12 hours are given, and morphine 2 mg is used as rescue. Ondansetron 4 mg daily is used for prophylaxis of nausea and vomiting, and metoclopramide 10 mg is given as needed.
Figure 1.
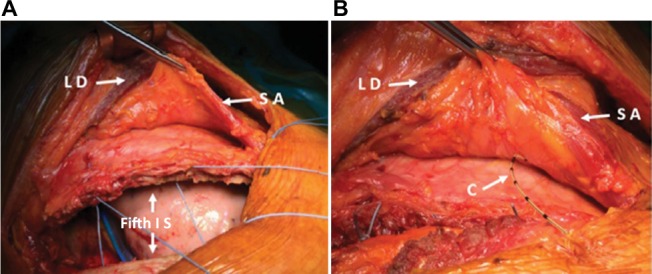
Right posterolateral thoracotomy (A) and SAP block (B): a 19-gauge catheter is tunnelized subcutaneously and its tip positioned in the plane below the serratus muscle and the rib cage.
Abbreviations: C, catheter; IS, intercostal space; LD, latissimus dorsi; SA, serratus anterior.
Static VAS and dynamic VAS are used to monitor postoperative pain. The VAS score, measured in millimeters from the left-hand end of the line to the point marked by the patient (0 – no pain to 100 – worst possible pain), is obtained three times daily. Vital signs (heart rate, non-invasive blood pressure, and peripheral oxygen saturation) are recorded every 8 hours. Dermatome distribution is tested at 2, 8, and 24 hours from surgery.
Results
Between January 1, 2016, and July 31, 2016, 37 patients underwent hybrid transthoracic esophagectomy and esophageal replacement by gastric pull-up through laparoscopy and right posterolateral thoracotomy at our institution. Seven of these patients (20%) underwent a continuous SAP block rather than TEA for different reasons (Table 1). In three cases, the epidural catheter could not be inserted due to severe kyphoscoliosis or obesity. Three patients were under antiaggregation or anticoagulant therapy; one of them had an inferior vena cava filter via jugular vein placed due to deep venous thrombosis. Finally, in patient 3, only a laparoscopic exploration, and not a thoracotomy, was initially planned due to the strong suspicion of metastatic disease. Since the tumor appeared resectable and liver metastases were not found, the esophagectomy was then performed.
Table 1.
Patients’ demographic and clinical characteristics
| Variables | Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Median (IQR) |
|---|---|---|---|---|---|---|---|---|
| Age (years) | 75 | 45 | 44 | 73 | 62 | 68 | 77 | 68.0 (20.5) |
| Sex | M | M | M | M | M | M | F | |
| BMI (kg/m2) | 26.3 | 29.4 | 29 | 29.1 | 21.3 | 24.7 | 44 | 29.0 (3.8) |
| Comorbidity | COPD, DM2, hypertension | DVT | OSAS | Hypertension, hypothyroidism | Hypertension | CAD (stented) | CAD (stented) | |
| Tumor histology | SCC | ADC | SCC | ADC | ADC | ADC | ADC | |
| Neoadjuvant therapy | CRT | CRT | CRT | None | CRT | CRT | CRT | |
| pTNM | T2N0M0 | T2N1M0 | T2N3M0 | T3N2M0 | T2N1M0 | T3N1M0 | T2N0M0 | |
| ASA score | 3 | 2 | 2 | 3 | 2 | 2 | 3 | 2.0 (1.0) |
| Indication to SAP | TEA technical failure | Anticoagulation therapy | Unplanned thoracotomy | TEA technical failure | Antiaggregation therapy | Antiaggregation therapy | TEA technical failure | |
| Operative time (minutes) | 235 | 300 | 385 | 295 | 300 | 325 | 270 | 300.0 (30.0) |
| Static VAS | ||||||||
| POD 1 | 40 | 0 | 15 | 15 | 20 | 35 | 30 | 20 (17.5) |
| POD 2 | 20 | 0 | 10 | 15 | 10 | 30 | 20 | 15 (10) |
| POD 3 | 10 | 0 | 0 | 0 | 0 | 10 | 0 | 0 (5) |
| POD 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 (0) |
| Dynamic VAS | ||||||||
| POD 1 | 50 | 15 | 20 | 25 | 15 | 50 | 30 | 25 (22.5) |
| POD 2 | 40 | 0 | 15 | 10 | 10 | 25 | 30 | 15 (17.5) |
| POD 3 | 20 | 0 | 0 | 0 | 0 | 0 | 10 | 0 (5) |
| POD 4 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0(0) |
| Rescue analgesia | ||||||||
| POD 1 | Remifentanil | Remifentanil | Remifentanil | |||||
| PODs 2–3 | Naropin | Ketorolac | ||||||
| ICU stay (days) | 1 | 1 | 1 | 2 | 1 | 2 | 2 | 1 (1) |
| Hospital stay (days) | 10 | 10 | 10 | 10 | 20 | 7 | 8 | 10.0 (1.5) |
| Follow up (months) | 6 | 5 | 5 | 4 | 3 | 2 | 2 | 5 (2) |
Abbreviations: ADC, adenocarcinoma; ASA, American Society of Anesthesiologists; BMI, body mass index; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; CRT, chemoradiation therapy; CT, chemotherapy; DM2, diabetes mellitus type 2; DVT, deep vein thrombosis; F, female; ICU, intensive care unit; IQR, interquartile range; M, male; OSAS, obstructive sleep apnea syndrome; POD, postoperative day; pTNM, pathological tumor–node–metastasis; SAP, serratus anterior plane; SCC, squamous cell carcinoma; TEA, thoracic epidural analgesia; VAS, visual analog scale.
In patient 1, a posterior rib fracture occurred at thoracotomy, and an additional 24 French chest drain was placed through the eighth intercostal space. Time to perform the SAP block procedure, including tunnelization, positioning, and fixation of the catheter to the skin, varied between 3 and 5 minutes. At the end of the weaning process, all patients had normal tidal breathing with sufficient ventilation and oxygenation and were successfully extubated in the operating room. Pain control was adequate, and no rescue doses were required. Subsequent stay in ICU for postoperative monitoring was uneventful. No episodes of nausea, vomiting, or hypotension occurred. All patients maintained a good level of consciousness and cough strength and followed a fast-track protocol upon return to the surgical ward. The postoperative chest film on days 1 and 5 confirmed re-expansion of the lung without evidence of atelectasis.
The infusion of levobupivacaine through the SAP catheter was continued until POD 4. The SAP catheter was uneventfully removed on POD 5. No complications related to local or systemic anesthetic toxicity were detected. The area of numbness in the right hemithorax, tested by cold application and pinprick at 2, 8, and 24 hours after anesthesia recovery, corresponded to the full extent of the thoracotomy incision, except for patient 6 who complained of persistent pain along the paravertebral area. Patient 1 suffered from persistent localized pain at the point of exit of the intercostal chest tube; a local infiltration of 7 mL of Naropin 0.75% was effective in reducing static and dynamic VAS. Patients were discharged from hospital within POD 10, except patient 5 whose postoperative course was complicated by chylothorax, requiring thoracoscopic stapling of the thoracic duct. No hospital readmissions occurred. At the follow-up visits 2–6 months later, the VAS score was 0 in all patients (Figure 3A and B).
Figure 3.

Static (A) and dynamic (B) VAS values.
Abbreviations: VAS, visual analog scale; POD, postoperative day.
Discussion
This pilot study shows that a “surgically guided” SAP block after hybrid transthoracic esophagectomy is feasible, easy and fast to perform, and safe. The continuous SAP block provided a good level of analgesia and no need of rescue doses in five of the seven patients.
Optimized postoperative pain relief allows early patient’s mobilization and respiratory physiotherapy and is a prerequisite for enhanced recovery after major thoracic surgery. However, optimal analgesia management after transthoracic esophagectomy may be difficult because both the abdominal and thoracic components of this procedure cause wound and visceral pain. The laparoscopic approach has reduced the intensity of pain compared to laparotomy in patients undergoing hybrid transthoracic esophagectomy.8,9 The thoracotomy incision involves a significant amount of trauma and distraction forces on multiple muscle layers, fascia, neurovascular bundles, rib cage, and parietal pleura. Postoperative pain can impair respiratory mechanics and contribute to the occurrence of pulmonary complications; in the long-term, it may also lead to the post-thoracotomy chronic pain syndrome. Unfortunately, no trials have assessed pain management protocols after hybrid or minimally invasive esophagectomy.
Epidural anesthesia remains the gold-standard technique in these patients and has been associated with reduction in respiratory complications,1 improvement in microcirculation in the gastric conduit and reduction in anastomotic leak rate,10 decrease in stress-induced immunosuppression and systemic anti-inflammatory response,11 and decrease in the incidence of post-thoracotomy chronic pain.12 However, TEA demands normal coagulation patterns and can fail in up to 30% of patients in clinical practice because of technical difficulties in epidural catheter placement or catheter dislodgement. High epidural catheterization for thoracic surgery is also associated with a risk of spinal hematoma and epidural abscess.13 Moreover, TEA may induce hypotension, requiring fluids load and/or vasopressors that may impair microcirculation of the esophageal substitute. Other reported side effects such as nausea, vomiting, and pruritus are related to the use of epidural opioids.14
The continuous paravertebral block may be a valid alternative to TEA. A recent meta-analysis has shown that the paravertebral block has equivalent analgesic effects to epidural analgesia and is associated with a lower incidence of nausea, vomiting, hypotension, and urinary retention.15 However, the reported failure rate is 6–12%, and the risk of neurological damage should not be underestimated.16 A few publications following the report by Blanco et al5 have confirmed the short-term efficacy of the SAP block to achieve numbness over the thoracic area supplied by the lateral cutaneous branches of the spinal nerves T2–T9.17,18 The possibility to perform a continuous SAP block by siting a catheter under ultrasound guidance has already been reported.19,20 Unique to our study is the “surgically guided” application of the continuous SAP block in a series of patients undergoing hybrid transthoracic esophagectomy. However, limitations of the present study are the prospective, not randomized design and the lack of a control group treated with TEA.
Conclusion
TEA still remains the gold standard for pain control after transthoracic esophagectomy. The SAP block may prove as effective as TEA in reducing postoperative pain, but clinical evidence is still lacking. The “surgically guided” SAP block has proven feasible and was easy and fast to perform and safe in our experience. Larger case series and randomized clinical trials are necessary to validate the effectiveness of SAP block in open transthoracic esophagectomy and its potential role in the context of enhanced recovery programs.
Figure 2.
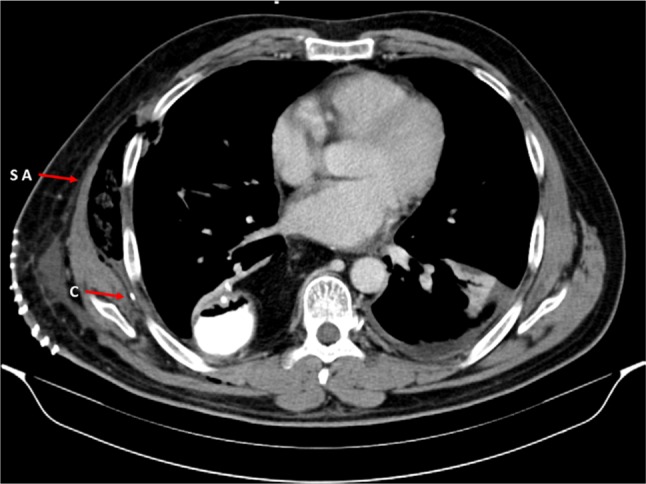
Computed tomography scan on POD 3.
Note: Arrows indicate the tip of the C and the SA muscle.
Abbreviations: C, catheter; POD, postoperative day; SA, serratus anterior.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Weijs TJ, Ruurda JP, Nieuwenhuijzen GA, van Hillegersberg R, Luyer MD. Strategies to reduce pulmonary complications after esophagectomy. World J Gastroenterol. 2016;19(39):6509–6514. doi: 10.3748/wjg.v19.i39.6509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Block BM, Liu SS, Rowlingson AJ, Cowan AR, Cowan JA, Wu CL. Efficacy of postoperative epidural analgesia: a meta-analysis. JAMA. 2003;290(18):2455–2463. doi: 10.1001/jama.290.18.2455. [DOI] [PubMed] [Google Scholar]
- 3.Rudin A, Flisberg P, Johansson J, Walther B, Lundberg CJ. Thoracic epidural analgesia or intravenous morphine analgesia after thoracoabdominal esophagectomy: a prospective follow-up of 201 patients. J Cardiothorac Vasc Anesth. 2005;19:350–357. doi: 10.1053/j.jvca.2005.03.013. [DOI] [PubMed] [Google Scholar]
- 4.Findlay JM, Gillies RS, Millo J, Sgromo B, Marshall RE, Maynard ND. Enhanced recovery for esophagectomy. A systematic review and evidence-based guidelines. Ann Surg. 2014;259(3):413–431. doi: 10.1097/SLA.0000000000000349. [DOI] [PubMed] [Google Scholar]
- 5.Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68(11):1107–1113. doi: 10.1111/anae.12344. [DOI] [PubMed] [Google Scholar]
- 6.Madabushi R, Tewari S, Gautam SK, Agarwal A, Agarwal A. Serratus anterior plane block: a new analgesic technique for post-thoracotomy pain. Pain Physician. 2015;18(3):E421–E424. [PubMed] [Google Scholar]
- 7.Okmen K, Okmen BM, Uysal S. Serratus anterior plane (SAP) block used for thoracotomy analgesia: a case report. Korean J Pain. 2016;29(3):189–192. doi: 10.3344/kjp.2016.29.3.189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bonavina L, Bona D, Binyom PR, Peracchia A. A laparoscopy-assisted surgical approach to esophageal carcinoma. J Surg Res. 2004;117(1):52–57. doi: 10.1016/j.jss.2003.11.007. [DOI] [PubMed] [Google Scholar]
- 9.Bonavina L, Scolari F, Aiolfi A, et al. Early outcome of thoracoscopic and hybrid esophagectomy: propensity matched comparative analysis. Surgery. 2016;159(4):1073–1081. doi: 10.1016/j.surg.2015.08.019. [DOI] [PubMed] [Google Scholar]
- 10.Michelet P, D’Journo XB, Roch A, et al. Perioperative risk factors for anastomotic leakage after esophagectomy: influence of thoracic epidural analgesia. Chest. 2005;128(5):3461–3466. doi: 10.1378/chest.128.5.3461. [DOI] [PubMed] [Google Scholar]
- 11.Ahlers O, Nachtigall I, Lenze J, et al. Intraoperative thoracic epidural anaesthesia attenuates stress-induced immunosuppression in patients undergoing major abdominal surgery. Br J Anaesth. 2008;101(6):781–787. doi: 10.1093/bja/aen287. [DOI] [PubMed] [Google Scholar]
- 12.Bong CL, Samuel M, Ng JM, Ip-Yam C. Effects of preemptive epidural analgesia on post-thoracotomy pain. J Cardiothorac Vasc Anesth. 2005;19(6):786–793. doi: 10.1053/j.jvca.2005.08.012. [DOI] [PubMed] [Google Scholar]
- 13.Rosero EB, Joshi GP. Nationwide incidence of serious complications of epidural analgesia in the United States. Acta Anaesthesiol Scand. 2016;60(6):810–820. doi: 10.1111/aas.12702. [DOI] [PubMed] [Google Scholar]
- 14.Hermanides J, Hollmann MW, Stevens MF, Lirk P. Failed epidural: causes and management. Br J Anaesth. 2012;109(2):144–154. doi: 10.1093/bja/aes214. [DOI] [PubMed] [Google Scholar]
- 15.Scarfe AJ, Schumann-Hingel S, Duncan JK, Ma N, Atukorale YN, Cameron AL. Continuous paravertebral block for cardio-thoracic surgery analgesia: a systematic review and meta-analysis. Eur J Cardio Thorac Surg. 2016 May 30; doi: 10.1093/ejcts/ezw168. Epub. [DOI] [PubMed] [Google Scholar]
- 16.Niemi G, Breivik H. Pain relief with paravertebral blocks or epidural analgesia? Those who do not know the history of paravertebral blocks are condemned to rediscover the complications. Scand J Pain. 2010;1:3–4. doi: 10.1016/j.sjpain.2009.11.002. [DOI] [PubMed] [Google Scholar]
- 17.Eid M. Other potential uses of serratus anterior plane block. Anaesthesia. 2014;69(8):933–934. doi: 10.1111/anae.12778. [DOI] [PubMed] [Google Scholar]
- 18.Barr K. Serratus plane block - is a high volume of local anaesthetic needed? Anaesthesia. 2014;69(2):192–193. doi: 10.1111/anae.12570. [DOI] [PubMed] [Google Scholar]
- 19.Broseta AM, Errando C, De Andrés J, Díaz-Cambronero O, Ortega-Monzó J. Serratus plane block: the regional analgesia technique for thoracoscopy? Anaesthesia. 2015;70(11):1329–1330. doi: 10.1111/anae.13263. [DOI] [PubMed] [Google Scholar]
- 20.Fujiwara S, Komasawa N, Minami T. Pectoral nerve blocks and serratus-intercostal plane block for intractable postthoracotomy syndrome. J Clin Anesth. 2015;27(3):275–276. doi: 10.1016/j.jclinane.2015.01.007. [DOI] [PubMed] [Google Scholar]