

Summary
Historically, American Indian/Alaska Native populations (AI/AN) have suffered excess morbidity and mortality from influenza. We investigated the risk factors for death from 2009 pandemic influenza A (H1N1) among persons residing in five states with substantial AI/AN populations. We conducted a case-control investigation using pandemic influenza fatalities from 2009 in Alaska, Arizona, New Mexico, Oklahoma and Wyoming. Controls were outpatients with influenza. We reviewed medical records and interviewed case proxies and controls. We used multiple imputation to predict missing data and multivariable conditional logistic regression to determine risk factors. We included 145 fatal cases and 236 controls; 22% of cases were AI/AN. Risk factors (p-value < 0.05) included: older age (adjusted matched odds ratio [OR] 3.2, for > 45 years. vs. < 18 years), pre-existing medical conditions (OR 7.1), smoking (OR 3.0), delayed receipt of antivirals (MOR 6.5), and barriers to healthcare access (OR 5.3). AI/AN race was not significantly associated with death. The increased influenza mortality among AI/ANs was due to factors other than racial status. Prevention of influenza deaths should focus on modifiable factors (smoking, early antiviral use, access to care) and identifying high risk persons for immunization and prompt medical attention.
Introduction
During the 2009 influenza A H1N1 pandemic (pH1N1), North American indigenous populations suffered disproportionately compared to the general population, as shown by higher rates of influenza-like illness1, hospitalization2,3,4, intensive care unit admissions4,5,6 and a four-fold increased rate of death7. We conducted a case-control investigation to determine risk factors for death due to 2009 H1N1 influenza A (pH1N1) in five U.S. states with large American Indian/Alaska Native (AI/AN) populations. Our objectives were to determine: 1) whether AI/AN racial status was an independent risk factor for death and, 2) the risk factors for death within the AI/AN population.
Methods
This investigation was conducted in Alaska, Arizona, New Mexico, Oklahoma and Wyoming. Case-patients (cases) were state residents who died related to infection with laboratory-confirmed influenza A from April 15, 2009 through January 31, 2010. Influenza infection was defined by a positive polymerase chain reaction (PCR) test, viral culture confirming pH1N1, a rapid influenza A test, or a direct fluorescent antibody test on a specimen collected from April 15 through December 31, 2009. We excluded cases who had no contact with a health care provider in the 14 days before death, or whose death and illness onset occurred when the person was located outside their state.
We attempted to match cases with two control-patients based on state of residence and influenza specimen date (within 14 days). Controls were state residents who had laboratory-confirmed pH1N1 infection (confirmed by PCR or culture) from April 15 through December 31, 2009 and who were not hospitalized for influenza within 30 days after their specimen collection date. Cases and controls were identified from death certificates and notifiable disease reports. Death certificates and medical records were abstracted using a standard form. Additionally, we interviewed a case proxy, defined as an adult who lived with or cared for the case prior to their illness, or a relative or close friend who lived nearby, or a relative knowledgeable of the case. If no case proxy was interviewed, we abstracted seven of the questions from the medical record. Interviews began October 2010 and ended March 2012. Data on fatalities from influenza for the U.S. population was obtained from national surveillance.
Four of the states required reporting of positive laboratory tests for pH1N1 (PCR and culture). Oklahoma obtained laboratory data from tests done by its Public Health Laboratory. Outpatients with pH1N1 were randomly-selected and contacted for an interview. Participant’s individual medical records were obtained and we abstracted demographic information, height, weight, health insurance status, medical and vaccination history, and influenza illness treatments. From interviews we obtained self-identified race, household characteristics, access to healthcare, past medical history, tobacco and alcohol habits, income and educational attainment.
Data were double entered into Paradox v 9.0 (Corel, Ottawa, Canada). Univariable tests were run in a conditional logistic regression model using the Wald chi-square statistic. Households with ≥ 1.5 persons per room were considered crowded and poverty was defined as having an annual household income < $25,0008. Obesity was defined as a BMI ≥30 (adults), a BMI ≥ 95th percentile for age (2–17 year olds), or ≥ 95th percentile of weight for age (<2 years old). Influenza-like illness (ILI) was defined by a reported fever, and either a cough or a sore throat. Age was modeled using three classes (< 18, 18–44 and ≥ 45 years). Receipt of antiviral medications was categorized into 3 levels: none, received ≤ 2 days after symptom onset, received ≥ 3 days after symptom onset.
Missing data ranged from 0% (age) to 25% (income). Missing data imputation procedures were employed, assuming data were missing at random. Data were imputed using Markov chain Monte Carlo iterations assuming a multivariate normal distribution9,10,11. The imputation model included variables for state of residence and specimen collection date, and all variables in the univariable analyses and case-control membership. Dichotomous variables derived from continuous variables were imputed in their continuous form; other dichotomous variables were imputed as dichotomous indicators9,10. We created 20 imputed datasets for the multivariable models12. A single chain was used with 200 burn-in iterations and 100 iterations between datasets. Each imputed dataset was analyzed using conditional logistic regression and then estimates were combined accounting for the parameter variability estimates and the variability associated with the imputation process. Analyses were conducted in SAS using logistic and imputation procedures13. Multivariable models used purposeful forward selection and included variables with a univariate p-value < 0.2514. After determining main effects, all two-way interactions with appropriate sample sizes were evaluated for statistical significance. Variable selection was repeated on the imputed datasets using the combined Wald χ2 statistic that incorporated the between- and within-imputation variation components15. Multivariable models included: the imputation model and a complete case analysis, where matched pairs or observations were entered or missing based on whether they had missing data for any given risk factor in the model.
A multivariable model restricted to AI/AN persons evaluated a subset of factors, due to sample size limitations, including demographics, healthcare access, one socio-economic variable, and all other variables that had adequate sample sizes. The variables that were used to match cases and controls were considered independent predictors in this model. Model diagnostics were run to identify influential observations or matched pairs in terms of model fit and parameter point and variance estimates. All p-values were two-sided and a value < 0.05 was considered statistically significant.
Results
A total of 257 fatalities associated with influenza A infection were reported in these states (annualized mortality: 6.6/100,000 persons/year). Of these, 145 met the case definition (Table 1). The epidemic peak occurred during calendar weeks 40 – 44, similar to the overall U.S. epidemic (Figure). Thirty-two fatalities were excluded, principally because they did not see a healthcare provider prior to death (90%); 69% of excluded cases were from Arizona. Eighty fatalities from Arizona were not included in analysis because of incomplete data or because Tribal approvals were not obtained. These persons were similar to the cases included from Arizona with regard to sex, age, diagnosis date, and underlying medical conditions; however, those not included were more likely to be of AI/AN racial status than the included fatal cases (26% vs. 11%, p = 0.01).
Table 1.
Characteristics of Participants, 5-State Influenza Mortality Investigation (Alaska, Arizona, New Mexico, Oklahoma, Wyoming), 2009
| Characteristic | Level | Cases (n = 145) |
Controls (n = 236) |
|
|---|---|---|---|---|
| Sex | Female | 73 (50%) | 120 (54%)a | |
| Male | 72 (50%) | 104 (46%) | ||
|
| ||||
| Age Group | < 5 years | 9 (6%) | 32 (14%) | |
| 5–10 years | 4 (3%) | 33 (14%) | ||
| 11–20 years | 14 (10%) | 52 (22%) | ||
| 21–30 years | 19 (13%) | 50 (21%) | ||
| 31–40 years | 9 (6%) | 23 (10%) | ||
| 41–50 years | 23 (16%) | 21 (9%) | ||
| 51–60 years | 35 (24%) | 17 (7%) | ||
| 61–70 years | 14 (10%) | 5 (2%) | ||
| 70+ years | 18 (12%) | 3 (1%) | ||
|
| ||||
| State | Alaska | 11 (8%) | 22 (9%) | |
| Arizona | 47 (32%) | 49 (21%) | ||
| Oklahoma | 37 (26%) | 74 (31%) | ||
| New Mexico | 47 (32%) | 85 (36%) | ||
| Wyoming | 3 (2%) | 6 (3%) | ||
|
| ||||
| Residence Typeb | Urban | 3 (4%) | 19 (9%) | |
| Large Rural | 17 (19%) | 81 (38%) | ||
| Small Rural | 8 (9%) | 16 (8%) | ||
| Isolated | 60 (68%) | 94 (45%) | ||
|
| ||||
| Race (when asked for a single race) | AI/AN | 25 (17%) | 27 (11%) | |
| White | 110 (76%) | 169 (72%) | ||
| Asian | 0 (0%) | 14 (6%) | ||
| Black | 5 (4%) | 3 (1%) | ||
| Other | 3 (2%) | 23 (10%)c | ||
| Unknown | 2 (1%) | 0 (0%) | ||
|
| ||||
| AI/AN race (alone or in combination) | 32 (22%) | 38 (16%) | ||
|
| ||||
| Specimen Collection Date | Summer (May – Aug) | 17 (12%) | 27 (11%) | |
| Fall (Sept – Oct) | 96 (66%) | 170 (72%) | ||
| Late Fall (Nov – Dec) | 32 (22%) | 39 (17%) | ||
|
| ||||
| Number of Controls per Case | 1 | 54 (37%) | ||
| 2 | 91 (63%) | |||
|
| ||||
| Time from specimen collection date of case and matched controls | ≤ 14 days | 193 (82%) | ||
| 15 – 30 days | 14 (6%) | |||
| 31 – 60 days | 13 (5%) | |||
| ≥ 60 days | 16 (7%) | |||
|
| ||||
| Number and % of cases without an interview of the case-proxy | 43 (29.7%) | |||
|
| ||||
| Diagnostic Test for Influenzad | Culture | 28 (19%) | 10 (4%) | |
| PCR | 98 (68%) | 209 (89%) | ||
| Rapid enzyme immunoassay | 16 (11%) | 15 (6%) | ||
| Fluorescent AB | 3 (2%) | 2 (1%) | ||
Twelve outpatient controls did not have a chart review completed and sex was not determined.
Residence type only available on 88 (61%) of the cases and 210 (89%) of the controls.
22 persons listed “Hispanic” as their race and one person listed “Filipino”
Results reflect medical chart review results. All controls were reported to the state health department as having a positive culture or PCR for pH1N1.
Figure.
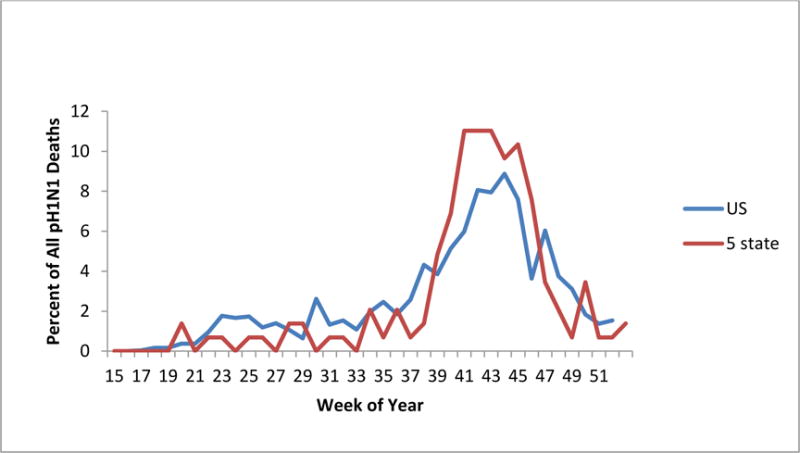
Fatal Influenza Cases by Week of Death, 2009., 5-States and Overall U.S.
We recruited 236 controls; 91 (63%) cases were matched to two controls and 54 were matched to one control. Proxy interviews with could not be obtained for 43 (30%) of fatal cases. Univariate risk factors for death are shown in Table 2. Multivariable analysis identified four independent risk factors for a fatal infection (Table 3): older age, having a pre-existing medical condition, being a smoker and receiving antivirals 3 or more days after illness onset. Using the imputed data set, a fifth independent variable was identified: a financial or transportation-related barrier to healthcare access. AI/AN race was not significantly associated with death after adding age and preexisting conditions to the models. There were no significant two-way interactions between the risk factors in the final models.
Table 2.
Univariate Risk Factors for Death Due to H1N1 in a Matched Case-control Investigation, 5 States (Alaska, Arizona, New Mexico, Oklahoma, Wyoming), 2009.
| Risk Factor | Level | Cases (n = 145) |
Controls (n = 236) |
Matched Odds Ratio (95% CI) | P-value |
|---|---|---|---|---|---|
| Mean Age | 43.4 | 23.0 | 1.62 (1.41, 1.84)a | <0.0001 | |
|
| |||||
| Age Class | <18 | 17% (25) | 47% (111) | ref | |
| 18–44 | 28% (40) | 38% (89) | 2.18 (1.17, 4.15) | 0.11 | |
| 45+ | 55% (80) | 15% (36) | 11.30 (5.55, 22.98) | <0.0001 | |
|
| |||||
| Sex | Male | 50%(73) | 46% (104) | ref | |
| Female | 50%(72) | 54% (120) | 0.87 (0.56, 1.36) | 0.55 | |
|
| |||||
| Regular Medical Provider | No | 18% (23) | 19% (44) | Ref | |
| Yes | 82% (105) | 81% (187) | 1.03 (0.58, 1.84) | 0.92 | |
|
| |||||
| Seek Healthcare in Previous 12 Months | No | 16% (15) | 24% (54) | Ref | |
| Yes | 84% (80) | 76% (169) | 1.67 (0.82, 3.38) | 0.16 | |
|
| |||||
| Barrier to Healthcare Access | No | 80% (81) | 93% (220) | Ref | |
| Yes | 20% (20) | 7% (16) | 3.22 (1.45, 7.17) | 0.004 | |
|
| |||||
| Healthcare Insurance | No | 7% (10) | 3% (8) | ||
| Yes | 93% (127) | 97% (227) | 0.39 (0.15, 1.03) | 0.06 | |
|
| |||||
| H1N1 | No | 83% (44) | 80% (70) | ref | |
| Vaccine | Yes | 17% (9) | 20% (17) | 0.78 (0.31, 1.96) | 0.24 |
|
| |||||
| Seasonal Influenza Vaccine | No | 52% (45) | 45% (82) | ref | |
| Yes | 48% (42) | 55% (102) | 0.70 (0.39, 1.27) | 0.24 | |
|
| |||||
| Living in an Institution | No | 91% (129) | 96% (226) | ref | |
| Yes | 9% (13) | 4% (10) | 2.32 (1.01, 5.33) | 0.047 | |
|
| |||||
| Household Density ≥ 1.5 Persons/room | No | 86% (75) | 90% (199) | ref | |
| Yes | 14% (12) | 10% (23) | 1.77 (0.73, 4.28) | 0.21 | |
|
| |||||
| Wood-Burning Stove | No | 87% (90) | 91%(213) | ref | |
| Yes | 13% (13) | 9% (21) | 2.78 (1.02, 7.64) | 0.047 | |
|
| |||||
| ≥ 4 Sinks in Household | No | 69% (62) | 61% (138) | ref | |
| Yes | 31% (28) | 40% (91) | 0.61 (0.33, 0.1) | 0.10 | |
|
| |||||
| Smoker | No | 72% (97)bd | 93% (173)b | 3.63 (1.61, 8.19)c | 0.002c |
| Yes | 28% (37)b | 7% (14)b | 4.67 (2.19, 9.92)b | <0.0001b | |
|
| |||||
| Alcohol Use | No | 75% (70)b | 78% (139)b | 0.57 (0.24, 1.34)c | 0.21c |
| Yes | 25% (23)b | 22% (39)b | 1.15 (0.56, 2.36)b | 0.71b | |
|
| |||||
| Heavy Alcohol Used | No | 84% (113)b | 94% (187)b | 1.77 (0.74, 4.19)c | 0.20c |
| Yes | 16% (21)b | 6% (12)b | 2.62 (1.16, 5.92)b | 0.02b | |
|
| |||||
| Secondhand Smoke-Home | No | 78% (82) | 87% (200) | ref | 0.11 |
| Yes | 22% (23) | 13% (31) | 1.75 (0.88, 3.50) | ||
|
| |||||
| Obesity BMI ≥ 30 | No | 51% (65) | 80% (176) | ||
| Yes | 49% (62) | 20% (44) | 3.72 (2.21, 6.28) | <0.0001 | |
|
| |||||
| AI/AN Race, alone or in combination with other races | No | 78% (111) | 84% (198) | ref | |
| Yes | 22% (32) | 16% (38) | 1.72 (1.00, 2.97) | 0.05 | |
|
| |||||
| AI/AN Race, alone | No | 83% (118) | 89% (209) | ref | |
| Yes | 17% (25) | 11% (27) | 1.95 (1.03, 3.68) | 0.04 | |
|
| |||||
| Graduated | No | 17% (18) | 10% (12) | ref | |
| High School | Yes | 83% (88) | 90% (109) | 0.71 (0.26, 1.93) | 0.50 |
|
| |||||
| Poverty (<$25,000/year) | No | 42% (33) | 68% (142) | ref | |
| Yes | 58% (45) | 32% (66) | 3.41 (1.57, 7.41) | 0.002 | |
|
| |||||
| ≥ 1 Pre-existing Conditione | No | 21% (31) | 80% (177) | 7.97 (3.59, 17.71)c | <0.0001c |
| Yes | 79% (114) | 20% (45) | 12.74 (6.60, 24.58) | <0.0001 | |
|
| |||||
| Asthma | No | 77% (112) | 90% (200) | 3.33 (1.40, 7.95)c | 0.007c |
| Yes | 23% (33) | 10% (21) | 2.82 (1.50, 5.31) | 0.001 | |
|
| |||||
| Chronic lung disease | No | 69% (100) | 99.5% (221) | 32.7 (4.4, 241.2)c | 0.0006c |
| Yes | 31% (45) | 0.5% (1) | 65.4 (9.0, 475.5) | <0.0001 | |
|
| |||||
| Diabetes | No | 72% (104) | 96% (213) | 5.27 (1.98, 14.02)c | 0.0009c |
| Yes | 28% (41) | 4% (9) | 9.27 (3.89, 22.07) | <0.0001 | |
|
| |||||
| Cardiovascular disease | No | 63% (91) | 98% (218) | 11.63 (4.13, 32.76)c | <0.0001c |
| Yes | 37% (54) | 2% (4) | 20.09 (7.25, 55.69) | <0.0001 | |
|
| |||||
| Influenza-like illness Symptoms | No | 40% (57) | 25% (50) | ref | |
| Yes | 60% (84) | 75% (154) | 0.55 (0.34, 0.91) | 0.02 | |
|
| |||||
| Antiviral Receipt | No | 42% (52) | 44% (94) | ||
| Yes (≤ 2 days) | 15% (18) | 46% (97) | 1.21 (0.77, 1.88) | 0.41 | |
| Yes (≥ 3 days) | 44% (54) | 10% (22) | 11.95 (3.65, 39.17) | <0.0001 | |
|
| |||||
| Antibiotics In Outpatient Setting | No | 82% (67) | 78% (171) | ||
| Yes | 18% (15) | 22% (48) | 0.92 (0.45, 1.87) | 0.81 | |
|
| |||||
| Corticosteroid Treatment | No | 50% (71) | 88% (191) | ||
| Yes | 50% (70) | 12% (26) | 8.83 (4.50, 17.35) | <0.0001 | |
|
| |||||
| Time from symptom onset to seeking care | ≤ 2 days | 54% (68) | 77% (154) | ||
| ≥ 3 days | 46% (58) | 23% (46) | 2.46 (1.50, 4.03) | 0.0002 | |
odds provided for a 10-year increase in age; odds for a single year increase was 1.04
odds, case numbers, percentages and p-values among those ≥ 7 years of age
odds and p-value among persons ≥ 18 years of age
alcohol abuse noted in chart or ≥ 15 drinks/month
includes asthma, chronic lung disease, cardiovascular disease, diabetes, other chronic metabolic disease, cancer (last 12 months), renal disease, liver disease, neuromuscular disease, blood disorder, <19 years old with aspirin therapy, immunosuppressive condition, and alcohol abuse
Table 3.
Risks Factors for Influenza Mortality, Multivariable Results for Matched Case-Control Investigation, for 5 States (Alaska, Arizona, New Mexico, Oklahoma, Wyoming), 2009.
| Multivariable Model | Risk Factor | Level | Complete Case Analysisa | Missing Data Imputationb | ||
|---|---|---|---|---|---|---|
|
| ||||||
| MOR (CI) | P-value | OR (CI) | P-value | |||
| All Races Model | Age Class | < 18 Years | Reference | Reference | ||
| 18–44 Years | 1.59 (0.37, 6.85) | 0.54 | 0.85 (0.31, 2.32) | 0.75 | ||
| 45+ Years | 4.77 (1.05, 21.76) | 0.04 | 3.22 (1.20, 8.62) | 0.02 | ||
|
| ||||||
| Pre-Existing Condition | No | Reference | <0.0001 | Reference | <0.0001 | |
| Yes | 6.74 (2.64, 17.20) | 7.10 (3.20, 15.78) | ||||
|
| ||||||
| Antiviral Receipt | Yes vs. No | 1.35 (0.71, 2.60) | 0.41 | 1.19 (0.60, 2.36) | 0.61 | |
| Receive ≥ 3 days from symptom onset vs. ≤ 2 days | 13.11 (3.37, 51.07) | 0.0006 | 6.46 (2.24, 18.62) | 0.0007 | ||
|
| ||||||
| Smoke at Time of Illness | No | Reference | 0.01 | reference | 0.04 | |
| Yes | 6.14 (1.56, 24.22) | 3.03 (1.01, 9.23) | ||||
|
| ||||||
| Barrier to Healthcare Access | No | not significant, removed from model | reference | 0.01 | ||
| Yes | 5.34 (1.45, 19.68) | |||||
|
| ||||||
| AI/AN Race Model | Pre-existing Condition | No | Reference | 0.02 | reference | 0.03 |
| Yes | 3.71 (1.26, 10.93) | 3.53 (1.14, 10.87) | ||||
|
| ||||||
| Obesity | No | Reference | 0.04 | reference | 0.03 | |
| Yes | 3.12 (1.04, 9.34) | 3.69 (1.18, 11.57) | ||||
|
| ||||||
| Smoke at Time of Illness | No | not significant, removed from model | reference | 0.03 | ||
| Yes | 5.39 (1.18, 24.68) | |||||
n = 258 observations in the final model for all races (from 106 case-control matches), and n = 63 observations in the final model for AI/AN race.
n = 381 observations the final model for all races (from 145 case-control matches), and n = 70 observations in the final model for AI/AN race.
Mortality risk factors for the 70 AI/AN participants are in Table 4. Multivariable analysis identified two independent risk factors for death: pre-existing medical conditions and obesity (Table 3). Using the imputed data, a third independent risk factor was identified: having been a smoker.
Table 4.
Univariate Risk Factors for Influenza Mortality among American Indian/Alaska Native Persons (alone or in combination with other races), for 5 states (Alaska, Arizona, New Mexico, Oklahoma, Wyoming), 2009.
| Risk Factor | Level | Cases (n = 32) |
Controls (n = 38) |
OR (CI) | P-value |
|---|---|---|---|---|---|
| Specimen Collection Date | April – September, October, November or Later | 31% (10) | 37% (14) | ||
| 50% (16) | 47% (18) | 0.87a | |||
| 19% (6) | 16% (6) | ||||
|
| |||||
| State | AK | 9% (3) | 13% (5) | ||
| AZ | 16% (5) | 5% (2) | |||
| NM | 41% (13) | 18% (7) | 0.11 | ||
| OK | 31% (10) | 58% (22) | |||
| WY | 3% (1) | 5% (2) | |||
|
| |||||
| Age Class | <18 | 22% (7) | 42% (16) | ref | 0.13 |
| 18–44 | 34% (11) | 34% (13) | 1.93 (0.58, 6.40) | ||
| 45+ | 44% (14) | 24% (9) | 3.56 (1.05, 12.05) | ||
|
| |||||
| Sex | Male | 50% (16) | 50% (18) | ref | |
| Female | 50% (16) | 50% (18) | 1.00 (0.39, 2.59) | 1.00 | |
|
| |||||
| Barrier to Healthcare | No | 65% (15) | 89% (34) | ref | |
| Yes | 35% (8) | 11% (4) | 4.53 (1.18, 17.40) | 0.03 | |
|
| |||||
| Household Density ≥ 1.5 Persons/room | No | 71% (15) | 89% (31) | ref | |
| Yes | 29% (6) | 11% (4) | 3.10 (0.76, 12.66) | 0.12 | |
|
| |||||
| Wood-Burning Stove | No | 78% (18) | 87% (33) | ref | |
| Yes | 22% (5) | 13% (5) | 1.83 (0.47, 7.19) | 0.38 | |
|
| |||||
| ≥ 4 Sinks in Household | No | 77% (17) | 61% (22) | ref | |
| Yes | 23% (5) | 39% (14) | 0.46 (0.14, 1.54) | 0.21 | |
|
| |||||
| Smoker at Illness Onset | No | 64% (18) | 91% (32) | 4.22b (0.99, 18.13) | 0.05 |
| Yes | 36% (10) | 9% (3) | 5.93 (1.44, 24.36) | 0.01 | |
|
| |||||
| Secondhand Smoke in Home | No | 75% (18) | 92% (35) | ref | |
| Yes | 25% (6) | 8% (3) | 3.89 (0.87, 17.39) | 0.08 | |
|
| |||||
| Heavy Alcohol User | No | 79% (22) | 91% (32) | 2.00b (0.44, 9.19) | 0.37 |
| Yes | 21% (6) | 9% (3) | 2.91 (0.66, 12.89) | 0.16 | |
|
| |||||
| Obesity | No | 41% (13) | 76% (29) | ref | |
| Yes | 59% (19) | 24% (9) | 4.71 (1.69, 13.17) | 0.003 | |
|
| |||||
| Poverty (<$25,000/year) | No | 35% (6) | 74% (23) | ref | |
| Yes | 65% (11) | 26% (8) | 5.27 (1.47, 18.94) | 0.01 | |
|
| |||||
| ≥ 1 Pre-existing Condition | No | 31% (10) | 69% (24) | 5.50b (1.44, 20.96) | 0.01 |
| Yes | 69% (22) | 31% (11) | 4.80 (1.71, 13.49) | 0.003 | |
|
| |||||
| Influenza-like illness | No | 28% (8) | 14% (5) | ref | |
| Yes | 72% (21) | 86% (30) | 0.44 (0.13, 1.53) | 0.19 | |
|
| |||||
| Antiviral Receipt | No | 40% (10) | 61% (20) | ref | |
| Yes (≤ 2 days) | 24% (6) | 30% (10) | 2.31c (0.80, 6.67) | 0.12 | |
| Yes (≥ 3 days) | 36% (9) | 9% (3) | 5.00d (0.96, 26.11) | 0.06 | |
|
| |||||
| Time from symptom onset to seeking care | ≤ 2 days | 60% (15) | 72% (23) | ref | |
| ≥ 3 days | 40% (10) | 28% (9) | 1.70 (0.56, 5.17) | 0.35 | |
test if overall mean specimen date differs between AI/AN cases and controls
among those 18 years of age and older
comparing those who received antivirals (≤ 2 days and ≥ 3 days combined) to those who did not
comparing those who received antivirals ≥ 3 days after symptom onset to those receiving antivirals ≤ 2 days after symptom onset
Discussion
In this case-control investigation from U.S. states with substantial AI/AN populations, we used medical records and interviews to assess potential risk factors for pH1N1 influenza A mortality. Three of the risk factors are modifiable (smoking, delayed receipt of antiviral medications, and a barrier to accessing health care). The association of death with smoking and a barrier to healthcare access have not been previously described for influenza16,17. Two other risk factors (older age and underlying medical conditions) are well recognized. AI/AN persons were overrepresented among the fatal cases (22% vs. 16% of controls, p = 0.05); however, AI/AN racial status was not an independent risk for death. The risk factors for death among the AI/AN population (pre-existing medical conditions, smoking, obesity) are similar to other North American populations17,18,19. This is the first population-based investigation to evaluate AI/AN race as a potential risk factor for influenza mortality and the first to evaluate influenza mortality risk factors among the AI/AN population.
Smoking has not been previously identified as a risk factor for influenza mortality16. Other studies of mortality risk during this pandemic either did not evaluate smoking17,18 or did not show an association when they compared fatal and hospitalized patients20,21. The prevalence of smoking among controls (11% for those 7 years or older) was much lower than the adult smoking prevalence in these states, which ranges from 19.2% to 26.1%22. This could have led to an overestimation of the magnitude of this risk factor. Despite this potential limitation, smoking is a biologically plausible risk factor and should be investigated further.
The financial or transportation-related barriers to healthcare access may have caused patients to delay seeking care after illness-onset, resulting in more severe illness that was less amenable to treatment. Although 93% of the fatal cases had health insurance, insurance coverage differs with regard to costs paid by the patient and healthcare seeking behavior is complicated. Further investigation is needed to identify ways to reduce barriers to healthcare among high-risk individuals, with and without health insurance.
Whether AI/AN race is, by itself, a risk factor for death or is a marker for other factors has substantial implications. Finding that AI/AN racial status was a risk factor might imply an undiscovered genetic susceptibility to severe influenza. A genetic explanation offers limited prevention options and could have a chilling effect on efforts to reduce influenza mortality among AI/AN23. Because AI/AN race is a marker for other risk factors, we can now focus on those modifiable risks among AI/AN persons. Three risk factors from the AI/AN-specific model were common among fatal cases (obesity 61%, smoking 35%, pre-existing conditions 69%). Similar to the overall population, we observed trends among AI/AN persons for higher mortality for older age, delay in antivirals (cases 36%, controls 9%), and healthcare access barriers (cases 35%, controls 11%). Accessing healthcare is a problem for AI/AN persons with influenza1. Among adults in 2009, AI/AN persons had the highest frequency of influenza-like illness of any racial group (16.2% vs. 8.2% overall), yet were the least likely to seek healthcare (37.4% vs. 42.1% overall). Further efforts are indicated to improve access and healthcare seeking behavior among AI/AN persons. Environmental determinants for lower respiratory tract infections common among AI/AN populations deserve further attention. These include household crowding24,25, limited access to in-home water and sanitation services26,27,28, and household air pollution from wood-burning stoves or second-hand tobacco smoke29.
The influenza mortality disparity between AI/AN persons and the general population is a challenge for influenza preparedness30. Prior to 2009, AI/ANs were not prioritized to receive vaccine or antiviral medications on the basis of racial status in the US. However, recommendations now include AI/AN persons as a high-risk group31,32. Some might consider that a risk factor-based strategy would be sufficient to identify AI/AN persons at risk for influenza complications. However, using the criteria for receipt of antiviral medications, 30% of fatal AI/AN cases would not have been considered high risk. In contrast, only 16% of influenza fatalities among whites would not have been considered high risk. AI/AN persons during 2009 also suffered disproportionately from influenza illness, hospitalizations and intensive care unit admissions. This is similar to the experience of AI/AN persons throughout the past 2 decades33. Thus, a risk factor-based strategy may not be comprehensive enough to address these long-standing influenza disparities. Designating AI/AN persons as high-risk can allow a more rapid delivery of vaccine, antiviral medications and education through U.S. Indian Health Service, tribal and urban Indian clinics. Thus, maintaining the high risk designation may be more likely to reduce the health disparity than a risk factor-based approach.
Influenza immunization uptake among AI/AN persons is similar to the general United States population, but should be improved34,35. Efforts to reduce smoking prevalence and obesity among AI/AN persons may be beneficial in reducing influenza mortality. Smoking prevalence among AI/AN adults (31.4%) far exceeds the overall U.S. population (19.0%)36. Likewise, obesity among AI/AN adults (39.6% prevalence) is more common that among non-Hispanic whites (26%)37.
These findings may not be generalizable to the entire U.S. or to all AI/AN persons. Because controls had access to health care and telephone service, comparisons for related socioeconomic factors may have been limited by design. By modelling only three age categories our ability to detect gradations in risk within age classes is limited. Missing data was addressed through multiple imputation which improved the power but would not solve potential bias related to representativeness of the population. We may have underestimated the AI/AN persons among the fatalities, since misclassification of AI/AN decedents has been documented38. Since approval was not obtained from all Arizona tribes, there was systematic under-recruitment of AI/AN persons and reduced representativeness of the included cases. Glucocorticoids used as a fever-reducing agent was identified as a risk factor for influenza death in China39. This is not a recommended practice in the United States40. However, because we did not obtain the timing or dosage of corticosteroid administration and nearly 50% of the fatal cases had received steroids, this remains a potential, uncontrolled confounder.
During the 2009 pandemic, AI/AN racial status was not independently associated with death, but was a marker for other modifiable factors. Keeping AI/AN race among the high-risk conditions for influenza complications should be considered as an appropriate response to the elevated risk of morbidity and mortality in this population. Increased efforts to reduce influenza mortality are needed to address this longstanding health disparity.
Acknowledgments
Jeremy Wood, Greg Raczniak, Michele Toomey
Arizona: Sara Imholte, John Meyer, Steve Baty, Anita Thorne, Zeenat Mahal, Sibeso Joyner, Eva Torres, Erica Weis, Justin Weddle, Tina Szopinski-Rubin, Reva Litt, Amritha Panachanathan
Oklahoma: Alfred Aiyanyor, Rachel Clinton, Margaret Selby
Wyoming: Tracy Murphy, Clayton Van Houten,
Council of State and Territorial Epidemiologists: Edward Chao, Jennifer Lemmings, Monica Huang
Other States: Melissa Powell (OR), Lon Kightlinger (SD), Rachelle Boulton (UT), Anthony Marfin (WA), Megan Hoopes (NPAIHB), Thomas Kim (CTEC), John Mosely Hayes (USETI), Thomas Weiser (NPAIHB), Lindsey VanderBusch (ND), Steven Helgersen (MT), Folorunso Akintan (RMTEC), Rachel Herlihy (UT), Ruta Sharangpani (MI), Jennie Finks (MI), Catherine Lexau (MN), Craig Morin (MN), Aaron DeVries (MN), Melissa Morrison (AL/CDC)
CDC: Alicia Fry, Scott Santibanez, Jay Wenger
Funding support was contributed by the Council of State and Territorial Epidemiologists (Cooperative Agreement Number 1U38HM000414 from CDC), plus in-kind contributions by CDC, state health departments and tribal epidemiology centers.
Footnotes
Human Participant Protection and Tribal Review
The investigation determined to be a non-research public health practice investigation by CDC and the Indian Health Service. Additional human subjects review and approval was obtained: Alaska Area IRB; Arizona: Navajo Nation Health Research Review Board, Arizona Department of Health Services-Human Subjects Review Board, Gila River Indian Community-Research Review Committee; New Mexico: New Mexico State University IRB, Southwest Tribal IRB, Navajo Nation Human Research Review Board; Oklahoma State Department of Health IRB; Wyoming Department of Health IRB. The protocol was approved by the following Tribal entities: Arizona: San Carlos Apache Tribe – Health Committee, San Carlos Apache Tribe Tribal Council, Tohono O’odham Nation – Health and Human Services Committee, Tohono O’odham Legislative Council, Alaska Native Tribal Health Consortium; Oklahoma City Area Intertribal Health Board; Wyoming: Eastern Shoshoni and Northern Arapahoe Tribes Montana/Wyoming Tribal Leaders Council/Rocky Mountain Tribal Epidemiology Center.
No financial disclosures were reported by the authors of this paper.
The findings and conclusions in this publication are those of the authors and do not necessarily represent the official views of the U.S. Centers for Disease Control and Prevention (CDC) or the Indian Health Service.
References
- 1.Dee DL, Bensyl DM, Gindler J, et al. Racial and ethnic disparities in hospitalizations and deaths associated with 2009 pandemic influenza (H1N1) virus infection in the United States. Ann Epidemiology. 2011;(8):623–30. doi: 10.1016/j.annepidem.2011.03.002. [DOI] [PubMed] [Google Scholar]
- 2.Wenger JD, Castrodale LJ, Bruden DL, et al. 2009 pandemic influenza A H1N1 in Alaska: temporal and geographic characteristics of spread and increased risk of hospitalization among Alaska Native and Asian/Pacific Islander people. Clinical Infectious Disease. 2011;52(S1):S189–S197. doi: 10.1093/cid/ciq037. [DOI] [PubMed] [Google Scholar]
- 3.Chowell G, Ayala A, Berisha V, Vibourd C, Schumacher M. Risk factors for mortality among 2009A/H1N1 influenza hospitalizations in Maricopa County, Arizona, April 2009 to March 2010. Comput Math Methods Med. 2012;2012:914196. doi: 10.1155/2012/914196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Thompson DL, Jungk J, Hancock E, et al. Risk factors for 2009 pandemic influenza A(H1N1)-related hospitalization and death among racial/ethnic groups in New Mexico. Am J Public Health. 2011;101:1776–1784. doi: 10.2105/AJPH.2011.300223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kumar A, Zarychanski R, Pinto R, et al. Critically ill patients with 2099 influenza A (H1N1) infection in Canada. JAMA. 2009;302:1872. doi: 10.1001/jama.2009.1496. [DOI] [PubMed] [Google Scholar]
- 6.Zarychanksi R, Stuart TL, Kumar A, et al. Correlates of severe disease in patients with 2009 pandemic influenza (H1N1) virus infection. CMAJ. 2010;10:257–64. doi: 10.1503/cmaj.091884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.CDC. Deaths related to 2009 pandemic influenza A (P-) among American Indian/Alaska Natives – 12 states, 2009. MMWR Morb Mortal Wkly Rep. 2009;58:1341–4. [PubMed] [Google Scholar]
- 8.Blake K, Kellerson R, Simic A. Measuring overcrowding in housing. Washington, DC: Department of Housing and Urban Development, Office of Policy Development and Research; 2007. [Google Scholar]
- 9.Allison PD. Missing Data. Sage Publications USA, Inc; Thousand Oaks, CA: 2001. (Series: Quantitative Application in the Social Sciences, Volume 136). [Google Scholar]
- 10.Bernaards CA, Belin TR, Schafer JL. Robustness of a multivariate normal approximation for imputation of incomplete binary data. Statistics in Medicine. 2007;26:1368–1382. doi: 10.1002/sim.2619. [DOI] [PubMed] [Google Scholar]
- 11.Lee KJ, Carlin JB. Multiple Imputation for Missing Data: Fully Conditional Specification Versus Multivariate Normal Imputation. Am J of Epi. 2010;171(5):624–32. doi: 10.1093/aje/kwp425. [DOI] [PubMed] [Google Scholar]
- 12.Graham JW, Alchowski AE, Gilreath TD. How Many Imputations are Really Needed? Some Practical Clarification of Multiple Imputation Theory. Prevention Science. 2007;(8):206–213. doi: 10.1007/s11121-007-0070-9. [DOI] [PubMed] [Google Scholar]
- 13.Yang Yuan. Multiple Imputation Using SAS Software. Journal of Statistical Software. 2011;45(6):1–25. doi: 10.18637/jss.v045.i01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hosmer DW, Lemeshow S. Applied Logistic Regression. Second. John Wiley & Sons, Inc.; New York, NY: 2000. [Google Scholar]
- 15.Wood AM, White IR, Royston P. How should variable selection be performed with multiply imputed data? Statistics in Medicine. 2008;27:3227–3246. doi: 10.1002/sim.3177. [DOI] [PubMed] [Google Scholar]
- 16.Epstein MA, Reynaldo S, Nelson El-Amin A. Is smoking a risk factor for influenza hospitalization and death? J Infect Dis. 2010;201(5):794–95. doi: 10.1086/650469. [DOI] [PubMed] [Google Scholar]
- 17.Regan J, Fowlkes A, Biggerstaff M, Jhung MA, Gindler J, Kennedy E, et al. Epidemiology of influenza A(H1N1)pdm09-associated deaths in the United States, September–October 2009. Influenza. 2012 Nov;6(6):169–77. doi: 10.1111/j.1750-2659.2012.00408.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Fowlkes AL, Arguin P, Biggerstaff MS, Gindler J, Blau D, Jain S, et al. Epidemiology of 2009 pandemic influenza A (H1N1) death in the United States, April–July 2009. Clin Infect Dis. 2011 Jan;1(S1):S60–68. doi: 10.1093/cid/ciq022. [DOI] [PubMed] [Google Scholar]
- 19.Morgan OW, Bramley A, Fowlkes, et al. Morbid obesity as a risk factor for hospitalization and death due to 2009 pandemic influenza A(H1N1) disease. PLosOne. 2010;5(3):e9694. doi: 10.1371/journal.pone.0009694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Zarychanski R, Stuart TL, Kumar A, Doucette S, Elliott L, Kettner J, Plummer F. Correlates of severe disease in patients with 2009 pandemic influenza (H1N1) virus infection. Can Med Assc J. 2010;182(3):257–64. doi: 10.1503/cmaj.091884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kumar A, Zarychanski R, Pinto R. Critically ill patients with 2009 influenza A(H1N1)infection in Canada. J Am Med Assc. 2009;302(17):1872–9. doi: 10.1001/jama.2009.1496. [DOI] [PubMed] [Google Scholar]
- 22.CDC. Selected Indicators for States. 2012 http://www.cdc.gov/tobacco/data_statistics/state_data/state_highlights/2012/pdfs/indicators.pdf Accessed on June 24, 2013.
- 23.Jones DS. The persistence of American Indian health disparities. Am J Pub Health. 2006;96(12):2122–2134. doi: 10.2105/AJPH.2004.054262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bulkow LR, Singleton RJ, DeByle C, Miernyk K, Redding G, Hummel KB, et al. Risk factors for hospitalization with lower respiratory tract infection in children in rural Alaska. Pediatrics. 2012;129(5):e1220–7. doi: 10.1542/peds.2011-1943. [DOI] [PubMed] [Google Scholar]
- 25.Singleton RJ, Bulkow L, Miernyk K, DeByle C, Pruitt L, Hummell KB, et al. Viral respiratory infection in hospitalized and community control children in Alaska. J Med Virol. 2010;82(7):1282–90. doi: 10.1002/jmv.21790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hennessy TW, Ritter T, Holman RC, Bruden DL, Yorita KL, Bulkow L, et al. The relationship between in –home water service and the risk of respiratory tract, skin, and gastrointestinal tract infections among rural Alaska Natives. Am J Pub Health. 2008;98(11):2072–2078. doi: 10.2105/AJPH.2007.115618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gessner BD. Lack of piped water and sewage services is associated with pediatric lower respiratory tract infection in Alaska. J Pediatr. 2008;152(5):666–700. doi: 10.1016/j.jpeds.2007.10.049. [DOI] [PubMed] [Google Scholar]
- 28.Wenger JD, Zulz T, Bruden D, Singleton R, Bruce MG, Bulkow L, et al. Invasive pneumococcal disease in Alaskan children: impact of the seven-valent pneumococcal conjugate vaccine and the role of water supply. Pediatr Infect Dis J. 2010;29(3):251–6. doi: 10.1097/INF.0b013e3181bdbed5. [DOI] [PubMed] [Google Scholar]
- 29.Robin LF, Less PS, Winget M, Steinhoff M, Moulton LH, Santosham M, Correa A. Wood-burning stoves and lower respiratory illnesses in Navajo children. Pediatric Infectious Disease Journal. 1996 Oct;15(10):859–65. doi: 10.1097/00006454-199610000-00006. [DOI] [PubMed] [Google Scholar]
- 30.Groom AV, Laroque M, Mason C, et al. Pandemic influenza preparedness and vulnerable populations in tribal communities. Am J Public Health. 2009;99:S271–8. doi: 10.2105/AJPH.2008.157453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Prevention and Control of Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices (ACIP) 2010 http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5908a1.htm?s_cid=rr5908a1_w. Accessed June 24, 2013. [PubMed]
- 32.Antiviral Agents for the Treatment and Chemoprophylaxis of Influenza: Recommendations of the Advisory Committee on Immunization Practices (ACIP) http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6001a1.htm Accessed June 24, 2013. [PubMed]
- 33.Groom AV, Hennessy TW, Singleton RJ, Butler JC, Holve S, Cheek JE. Pneumonia and influenza mortality among American Indian and Alaska Native people, 1990–2009. Am J Public Health. 2014 Jun;104(S3):S460–9. doi: 10.2105/AJPH.2013.301740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.CDC. Seasonal Influenza Vaccination Coverage – United States, 2009–10 and 2010–11, Morbidity and Mortality Weekly Reports. 2013 Nov 22;62(03):65–68. [PubMed] [Google Scholar]
- 35.Lindley MC, Groom AV, Wortley PM, Euler GL. Population status of influenza and pneumococcal vaccination among older American Indians and Alaska Natives. American Journal of Public Health. 2008;98(5):932–8. doi: 10.2105/AJPH.2007.119321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.CDC. Adult cigarette smoking in the United States. 2010 http://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/ Accessed June 24, 2013.
- 37.CDC. Summary Health Statistics for US Adults: National health Interview Survey, 2010. 2012 http://www.cdc.gov/nchs/data/series/sr_10/sr10_252.pdf Accessed June 24, 2013. [PubMed]
- 38.Arias E, Schauman WS, Eschbach K, Sorlie PD, Backlund E. The validity of race and Hispanic origin reporting on death certificates in the United States. Vital Health Stat. 2008;2(148) [PubMed] [Google Scholar]
- 39.Han K, Ma H, Xiangdong A, et al. Early use of glucocorticoids was a risk factor for crucial disease and death from pH1N1 infection. Clinical Infectious Diseases. 2011;53(4):326–333. doi: 10.1093/cid/cir398. [DOI] [PubMed] [Google Scholar]
- 40.CDC. Interim Information for Clinicians about Human Infections with H3N2v Virus. http://www.cdc.gov/flu/swineflu/h3n2v-clinician.htm Accessed April 10, 2015.