

Abstract
Background
We conducted a prospective cohort study to investigate prevalence of poststroke cognitive impairment at 3 and 12 months after stroke onset and identify clinical and demographic factors associated with improvement or decline in cognitive function between 3 months and 12 months.
Methods
We analyzed the cognitive assessments of total patients and patients older than 65 years separately. All patients with an ischemic stroke were divided into normal cognitive group (NCG) and impaired cognition group (ICG) by using a cutoff score on the Korean Mini-Mental State Examination (K-MMSE). Patients were additionally classified into 3 subgroups according to the changes in their K-MMSE scores between 3 and 12 months: Stable group with K-MMSE scores changes ranging from −2 to +2 points (−2 ≤ △MMSE ≤ +2); converter group with increase more than 3 points (3 ≤ △MMSE); and reverter group with decrease more than 3 points (−3 ≤ △MMSE). We also analyzed factors affecting cognitive change from 3 months to 12 months among the 3 groups including baseline medical record, stroke and treatment characteristics, and various functional assessments after 3 months.
Results
This study included 2,625 patients with the first time ischemic stroke. Among these patients, 1,735 (66.1%) were classified as NCG, while 890 patients (33.9%) were belonged to the ICG at 3 month. Within the NCG, 1,460 patients (82.4%) were stable group, 93 patients (5.4%) were converter group, and 212 patients (12.2%) were reverter group at 12 months onset. Within the ICG group, 472 patients (53.0%) were stable group, 321 patients (36.1%) were converter group, and 97 patients (10.9%) were reverter group. When different factors were investigated, the three subgroups in NCG and ICG showed significant different factors affecting cognitive function from 3 to 12 month.
Conclusions
The prevalence of cognitive impairment showed difference between 3,12 months. To analyze the cognitive change from 3 month to 12 month, the proportion stable group was dominant in NCG and converter group was higher in ICG. By investigating the influencing factors from each group, we were able to identify the predictors including the age factor.
Keywords: Ischemic stroke, Cognition, Inverter, Reverter, Risk factors
Background
Cerebrovascular stroke is considered one of the main causes of dementia [1–3]. It may decrease quality of life in addition to causing other neurological deficits [4]. Post-stroke dementia is defined as a presence of dementia identified at 3 months after an acute stroke [5]. Reasons for a stroke patient to develop dementia are still insufficiently understood. It is not always a direct consequence of cerebrovascular lesions, and, in some cases, post-stroke dementia has a progressive course, suggesting a degenerative rather than a vascular origin [6, 7]. In previous autopsy series, 10 to 15% of dementias occurring after a stroke were found to be due to a combination of vascular and Alzheimer’s disease [8, 9].
Despite consensus that strokes are associated with an increased risk of post-stroke dementia, the data regarding prevalence at 3 months post-stroke are still conflicting, with reports ranging from 6% to more than 50% [10–14]. In addition, cognitive function may vary (either improve or decline) years after a stroke. Snaphaan et al. reported that post-stroke memory dysfunction varied from 23 to 55% at 3 months after a stroke, and this declined from 11 to 31% at 1 year after a stroke. Declined cognitive function may change. A previous cohort study showed 33% of patients with mild cognitive impairments diagnosed in the first 6 months after a stroke showed improvement at 1 year. Several prospective studies have identified delayed improvement in cognitive function after strokes using various diagnostic assessment tools for dementia [15-17].
The pathophysiology of delayed cognitive change after a stroke is multifactorial, and the prevalence rate of post-stroke dementia is higher among older patients [18, 19]. Previous studies have tracked cognitive changes to identify the factors associated with delayed improvement or a decline in cognitive function after stroke. However, no large-scale study has been conducted to investigate the pattern of post-stroke cognitive changes, identify the risk factors, or compare age-related differences using repeated administration of the most commonly used screening tool.
Therefore, we conducted a prospective cohort study in conjunction with the Korean Stroke Cohort for Functioning and Rehabilitation (KOSCO) to identify 1) the prevalence of delayed cognitive impairment; patients progress to either converter, stable, or reverter group after ischemic stroke and 2) clinical and demographic factors associated with improvement or decline in cognitive function between 3 months and 12 months after ischemic stroke. The present study is the first to involve a large and well-characterized Korean cohort, a battery of short cognitive and functional assessments, and a 1-year follow-up.
Methods
Study design
KOSCO is a large, multi-centered, prospective cohort study of all acute, first-time stroke patients admitted to participating hospitals in nine distinct areas of Korea. A written informed consent is obtained from all patients prior to inclusion in the study, and the study protocols were approved by the ethics committee of each hospital. The detailed rationale and protocols of KOSCO were described in a previous article [20].
Study subjects
All consecutive patients with an acute, first-time IS admitted to the representative hospitals were asked to participate in the study. The inclusion criteria were: 1) first-time ischemic stroke with corresponding lesion on a MRI/A scan, 2) age ≥19 years at stroke onset, and 3) onset of symptoms within 7 days prior to inclusion. Exclusion criteria were: 1) recurrent stroke; 2) hemorrhagic stroke; 3) traumatic intracerebral hemorrhage; 4) previously diagnosed dementia or cognitive impairment; 5) persistent aphasia; and 6) history of systemic diseases known to involve the central nervous system.
Procedure
All eligible patients were recruited from August 2012 to April 2015 at the time of stroke evaluation. After providing a written informed consent, patients were formally enrolled in the study. If a patient was unable to provide informed consent, the consent was obtained from the patient’s legally authorized representative.
Demographic and clinical characteristics
Baseline demographic and clinical characteristics of enrolled patients were evaluated at 3 months. A complete enumeration survey of all patients was performed using a review of medical records upon the first admission. Survey items included demographic data and presence of cerebrovascular risk factors using standardized, structured questionnaires. The items were classified according to the current guidelines of the American Heart Association [21]. Comorbidities were assessed using the Charlson comorbidity index [22]. Initial stroke severity was recorded at the time of hospital arrival using the Korean National Institute of Health Stroke Scale (K-NIHSS) for ischemic strokes [23]. Physical examination findings and laboratory measures were also recorded. The course of the disease during admission was documented including information on medication use, treatments such as intravenous or arterial thrombolysis, and complications. Patients that received rehabilitation at 3 months were transferred to the rehabilitation center to initiate active rehabilitation after acute management at the neuroscience center. The remaining patients that did not receive any rehabilitation treatments were discharged or transferred to other hospitals instead of being transferred to the Rehabilitation Medicine Department.
Classification of ischemic stroke; etiology, and neuroimaging
The etiologies of ischemic strokes were classified according to the TOAST criteria [24]. Etiology was determined based on neuro-imaging, medical history, and use of medication. MRI scans were reviewed by neuroimaging specialists in each institute. Ischemic strokes were classified according to arterial territory and as either lacunar or territorial.
Cognitive assessment
To identify influencing factors by age, we analyzed the Korean Mini-Mental State Examination (K-MMSE) at 3 months separately between total patients and patients older than 65 years. To analyze changes in cognitive function, all patients were divided into normal cognitive group (NCG) and impaired cognition group (ICG) by using standard deviation score after correcting raw scores by age, sex and education level of the patients [25]. Patients were again classified according to the changes in their K-MMSE scores between 3 and 12 months after stroke onset into stable groups (NCG-SG, ICG-SG) with K-MMSE changes ranging from −2 to +2 points (−2 ≤ △MMSE ≤ +2), converter groups (NCG-CG, ICG-CG) with increases of K-MMSE more than 3 points (3 ≤ △MMSE), and reverter groups (NCG-RG, ICG-RG) with score decreases of K-MMSE more than 3 points (−3 ≤ △MMSE). Factors affecting cognitive change from 3 months to 12 months including baseline medical record, stroke and treatment characteristics, and various functional assessments after 3 months were analyzed among the groups (Fig. 1).
Fig. 1.
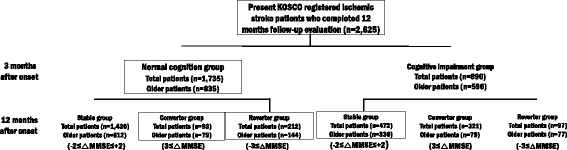
Flow diagram of this study
Functional assessment battery
At 3 months after stroke onset, a face-to-face functional assessment was performed. Assessments included the K-NIHSS for stroke severity, Functional Independence Measure (FIM) [26], Korean modified Barthel Index (K-MBI) [27] for activities of daily living, Fugl-Meyer Assessment (FMA) [28] for motor function, Functional Ambulatory Category (FAC) [29] for mobility and gait, mRS (modified rankin scale) [30] for general functional level, Geriatric depression scale-short form (GDS-SF) [31] for mood, and Euro Quality of Life (EQ)-5D [32] for quality of life (Table 1).
Table 1.
Functional assessments at 3 months
| Domain | Assessment |
|---|---|
| Stroke severity | National Institute of Health Stroke Scale (NIHSS) |
| Activities of daily living | Korean modified Barthel Index (K-MBI) |
| Functional Independence Measure (FIM) | |
| Cognition function | Korean Mini-Mental State Examination (K-MMSE) |
| Motor function | Fugl-Meyer Assessment (FMA) |
| Modified Ashworth scale (mRS) | |
| Mobility function | Functional Ambulatory Category (FAC) |
| Mood | Geriatric depression scale-short form (GDS) |
| Quality of life | Euro Quality of Life-5D |
Statistical analysis
For statistical analysis, we used descriptive statistics for the demographic and clinical characteristics, initial stroke features and treatment methods. Nominal and ordinal data obtained from a baseline review of medical records and initial stroke features were compared using frequency analysis. Scale factors were analyzed using average analysis. Chi-square test and one-way ANOVA were used to compare the influencing factors among groups. Bonferroni correction was done for post-hoc analysis of ANOVA. Statistical analysis was completed using SPSS for Windows version 21.0 (SPSS Inc., Chicago, IL). P < 0.05 is considered statistically significant.
Results
A total of 2,625 patients (older patients = 1,431) with first time ischemic stroke were included in this study. Among these patients, 1,735 (66.1%) (older patients = 835 (58.4%)) were classified as NCG, while 890 patients (33.9%) (older patients = 596 (41.6%)) were the ICG at 3 month K-MMSE assessment. Although, percentage of normal and declined cognitive function was similar for older patients at 3 months and 12 months, percentage of normal cognition group was slightly increased and percentage of declined cognition groups was decreased in total patients (Fig. 2). Among NCG, 1,460 (82.4%) (older patients = 612 (73.3%)) were stable group, 93 patients (5.4%) (older patients = 79 (9.5%)) were converter group, and 212 patients (12.2%) (older patients = 144(17.2%)) were reverter group at 12 months onset. Among ICG, 472 patients (53.0%) (older patients = 336 (56.4%)) were stable group, 321 patients (36.1%) (older patients = 183(30.7%)) were converter group, and 97 patients (10.9%) (older patients = 77 (12.9%)) were reverter group (Table 2) (Figs. 3, 4). To analyze the cognitive change from 3 month to 12 month, the proportion stable group was dominant in NCG and converter group was higher in ICG.
Fig. 2.
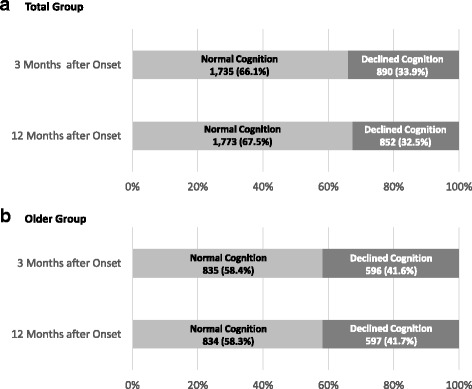
Cognitive function of patients at 3 months and 12 months after stroke onset
Table 2.
Cognitive change divided by age from 3 months to 12 months
| Age | Group | n (%) | Cognitive Change | 3 months after onset | 12 months after onset | |
|---|---|---|---|---|---|---|
| n (%) | K-MMSE (mean ± SD) | K-MMSE (mean ± SD) | ||||
| Total Subjects (n = 2,625) |
Normal Cognition | 1,735 (66.1) |
Stable | 1,430 (82.4) | 28.09 ± 2.66 | 28.14 ± 2.75 |
| Converter | 93 (5.4) | 23.67 ± 3.60 | 27.41 ± 3.19 | |||
| Reverter | 212 (12.2) | 26.81 ± 3.53 | 22.00 ± 4.80 | |||
| Declined Cognition | 890 (33.9) |
Stable | 472 (53.0) | 16.14 ± 9.81 | 16.42 ± 10.09 | |
| Converter | 321 (36.1) | 17.87 ± 9.81 | 24.11 ± 5.69 | |||
| Reverter | 97 (10.9) | 16.34 ± 7.27 | 11.03 ± 7.46 | |||
| Older age (n = 1,431) |
Normal Cognition | 835 (58.4) |
Stable | 612 (73.3) | 26.86 ± 3.41 | 26.88 ± 3.50 |
| Converter | 79 (9.5) | 23.18 ± 3.69 | 27.01 ± 3.30 | |||
| Reverter | 144 (17.2) | 25.85 ± 3.82 | 20.66 ± 4.90 | |||
| Declined Cognition | 596 (41.6) |
Stable | 336 (56.4) | 14.46 ± 9.71 | 14.68 ± 9.95 | |
| Converter | 183 (30.7) | 15.95 ± 7.64 | 22.46 ± 5.78 | |||
| Reverter | 77 (12.9) | 16.08 ± 7.09 | 10.52 ± 7.21 | |||
n, Number; SD, Standard Deviation; K-MMSE, Korean Mini Mental State Examination
Fig. 3.

Cognitive change of total patients from 3 months to 12 months
Fig. 4.

Cognitive change of the older patient group from 3 months to 12 months
Among NCG of total patients, hypertension, and cortical or multiple level involvement was dominant in reverter group, male sex, lower onset age, higher education level were dominant in stable group. In addition, functional assessments in stable group including NIHSS, mRS, FIM, K-MBI, FAC, GDS, and EQ-5D at 3 months were significantly better in scores compared to other groups. For the tendency of ICG of total patients, onset age, hypertension history was higher, education level was lower in reverter group. All functional assessments at 3 months showed better scores in converter groups and worse scores in reverter group (Table 3). Among separated older patients, male sex, lower onset age were dominant in stable group, educational level was lower in reverter group. Functional assessments including NIHSS, mRS, FIM, K-MBI, FAC, GDS, and EQ-5D, at 3 months showed better scores in stable group compared to others. In addition, proportion of receiving rehabilitation therapy at 3 months was lower and all functional l assessments showed better scores in converter group compared to others (Table 4).
Table 3.
Factors affecting cognitive change from 3 months to 12 months in total patients
| Parameters | Normal Cognition (n = 1,735) | Declined Cognition (n = 890) | ||||||
|---|---|---|---|---|---|---|---|---|
| Stable (n = 1,430) | Converter (n = 93) | Reverter (n = 212) | P value | Stable (n = 472) | Converter (n = 321) | Reverter (n = 97) | P value | |
| 1) Baseline medical record assessments | ||||||||
| Male, n (%) | 991 (69.3) | 46 (49.5) | 107 (50.5) | .000** | 248 (52.5) | 185 (57.6) | 52 (53.6) | .362 |
| Age, (mean ± SD) | 61.52 ± 12.53a | 69.44 ± 11.16b | 73.75 ± 8.85c | .000** | 70.32 ± 11.07a | 66.34 ± 11.54b | 72.32 ± 9.45ab | .000** |
| Education, n (%) | ||||||||
| Uneducated | 114 (8.0) | 25 (26.9) | 44 (20.8) | .000** | 35 (7.4) | 11 (3.4) | 13 (13.4) | .000** |
| 0–3 years | 46 (3.2) | 10 (10.8) | 12 (5.7) | 40 (8.5) | 26 (8.1) | 11 (11.3) | ||
| 4–6 years | 189 (13.2) | 25 (26.9) | 52 (24.5) | 117 (24.8) | 73 (22.7) | 27 (27.8) | ||
| 7–9 years | 222 (15.5) | 17 (18.3) | 45 (21.2) | 113 (23.9) | 70 (21.8) | 21 (21.6) | ||
| 10–12 years | 468 (32.7) | 8 (8.6) | 36 (17.0) | 135 (28.6) | 93 (29.0) | 19 (19.6) | ||
| 13 years– | 391 (27.3) | 8 (8.6) | 23 (10.8) | 32 (6.8) | 48 (15.0) | 6 (6.2) | ||
| BMI (kg/m2), (mean ± SD) | 24.10 ± 3.28a | 23.59 ± 3.61ab | 23.49 ± 3.33b | .023* | 23.35 ± 3.08 | 23.47 ± 3.30 | 22.62 ± 3.27 | .071 |
| Risk factors of stroke, n (%) | ||||||||
| Hypertension | 779 (54.5) | 63 (67.7) | 118 (88.7) | .030* | 275 (58.3) | 178 (55.5) | 68 (70.1) | .037* |
| Diabetes Mellitus | 206 (14.4) | 15 (16.1) | 24 (11.3) | .412 | 70 (14.8) | 44 (13.7) | 22 (22.7) | .091 |
| Coronary heart disease | 98 (6.9) | 9 (9.7) | 15 (7.1) | .587 | 40 (8.5) | 20 (6.2) | 5 (5.2) | .339 |
| Atrial fibrillation | 118 (8.3) | 14 (15.1) | 27 (12.7) | .014* | 68 (14.4) | 37 (11.5) | 11 (11.3) | .433 |
| Hyperlipidemia | 246 (17.2) | 12 (12.9) | 39 (18.4) | .493 | 54 (11.4) | 42 (13.1) | 15 (15.5) | .505 |
| Obesity | 190 (13.3) | 14 (15.1) | 23 (10.8) | .522 | 49 (10.4) | 40 (12.5) | 4 (4.1) | .063 |
| Family history | 135 (9.4) | 5 (5.4) | 20 (9.4) | .420 | 48 (10.2) | 26 (8.1) | 7 (7.2) | .483 |
| Smoking, n (%) | ||||||||
| Current smokers | 462 (32.3) | 17 (18.3) | 44 (20.8) | .000** | 127 (26.9) | 87 (27.1) | 29 (29.9) | .859 |
| Former smokers | 202 (14.1) | 10 (10.8) | 19 (9.0) | 55 (11.7) | 39 (12.1) | 8 (8.2) | ||
| Never smokers | 766 (53.6) | 66 (71.0) | 149 (70.3) | 290 (61.4) | 195 (60.7) | 60 (61.9) | ||
| Alcohol consumption, n (%) | ||||||||
| None | 793 (55.5) | 62 (66.7) | 144 (67.9) | .002** | 327 (69.3) | 202 (63.0) | 67 (69.1) | .253 |
| Moderate | 452 (31.6) | 23 (24.7) | 42 (19.8) | 97 (20.6) | 72 (22.4) | 21 (21.6) | ||
| Heavy | 185 (12.9) | 8 (8.6) | 26 (12.3) | 48 (10.2) | 47 (14.6) | 9 (9.3) | ||
| 2) Stroke characteristics | ||||||||
| Ischemic type (TOAST) | ||||||||
| Large–artery atherosclerosis | 641 (44.8) | 58 (62.4) | 101 (47.6) | .062 | 229 (48.5) | 173 (53.9) | 56 (57.7) | .572 |
| Small-artery occlusion | 373 (26.1) | 14 (15.1) | 53 (25.0) | 85 (18.0) | 57 (17.8) | 15 (15.5) | ||
| Cardioembolism | 156 (10.9) | 6 (6.5) | 24 (11.3) | 74 (15.7) | 39 (12.1) | 9 (9.3) | ||
| Other determined | 115 (8.0) | 4 (4.3) | 12 (5.7) | 29 (6.1) | 14 (4.4) | 5 (5.2) | ||
| Undetermined ischemic stroke | 145 (10.1) | 11 (11.8) | 22 (10.4) | 55 (11.7) | 38 (11.8) | 12 (12.4) | ||
| Ischemic location | ||||||||
| Rt. hemisphere | 680 (47.6) | 46 (49.5) | 99 (46.7) | .580 | 178 (37.7) | 117 (36.4) | 41 (42.3) | .698 |
| Lt. hemisphere | 648 (45.3) | 37 (39.8) | 94 (44.3) | 262 (55.5) | 185 (57.6) | 48 (49.5) | ||
| Both hemisphere | 102 (7.1) | 10 (10.8) | 19 (9.0) | 178 (37.7) | 19 (5.9) | 8 (8.2) | ||
| Affected level | ||||||||
| Cortical level | 440 (30.8) | 37 (39.8) | 70 (33.0) | .007** | 191 (40.5) | 139 (43.3) | 41 (42.3) | .878 |
| Subcortical level | 454 (31.7) | 22 (23.7) | 49 (23.1) | 115 (24.4) | 83 (25.9) | 25 (25.8) | ||
| Brainstem level | 330 (23.1) | 13 (14.0) | 58 (27.4) | 63 (13.3) | 41 (12.8) | 14 (14.4) | ||
| Multiple level | 206 (14.4) | 21 (22.6) | 35 (16.5) | 103 (21.8) | 58 (18.1) | 17 (17.5) | ||
| 3) Treatment characteristics | ||||||||
| IV thrombolysis | 104 (7.3) | 7 (7.5) | 13 (6.1) | .826 | 43 (9.1) | 29 (9.0) | 15 (15.5) | .136 |
| IA thrombolysis | 21 (1.5) | 3 (3.2) | 4 (1.9) | .404 | 23 (4.9) | 9 (2.8) | 2 (2.1) | .208 |
| IV heparin | 121 (8.5) | 5 (5.4) | 17 (8.0) | .573 | 33 (7.0) | 18 (5.6) | 10 (10.3) | .271 |
| Antiplatelet agent | 1,140 (79.7) | 77 (82.8) | 166 (78.3) | .668 | 333 (70.6) | 240 (74.8) | 65 (67.0) | .241 |
| Rehabilitation Therapy | 386 (27.0) | 29 (31.2) | 59 (27.8) | .669 | 187 (60.4) | 116 (36.1) | 43 (44.3) | .311 |
| Cognitive Therapy | 56 (3.9) | 4 (4.3) | 9 (4.2) | .961 | 28 (5.9) | 33 (10.3) | 11 (11.3) | .041* |
| 4) Functional assessments | ||||||||
| Cognitive function (K-MMSE) | ||||||||
| 3 months from onset | 28.09 ± 2.66a | 23.67 ± 3.60b | 26.81 ± 3.53c | .000** | 16.14 ± 9.81a | 17.87 ± 7.81b | 16.34 ± 7.27ab | .024* |
| 12 months from onset | 28.14 ± 2.75a | 27.41 ± 3.19a | 22.00 ± 4.80b | .000** | 16.42 ± 10.09a | 24.11 ± 5.69b | 11.03 ± 7.46c | .000** |
| Variation (from 3 months to 12 months) | 0.05 ± 1.07a | 3.41 ± 1.23b | −4.81 ± 2.91c | .000** | 0.29 ± 1.09a | 6.25 ± 4.19b | −5.31 ± 2.81c | .000** |
| Stroke Severity, ADL, Motor, Gait, Depression, QoL (3 months from onset) | ||||||||
| NIHSS | 0.77 ± 1.85a | 1.11 ± 2.03ab | 1.12 ± 2.02b | .015* | 5.09 ± 6.86a | 3.12 ± 4.62b | 5.25 ± 4.63a | .000** |
| mRS | 0.99 ± 1.02a | 1.44 ± 1.28b | 1.43 ± 1.20b | .000** | 2.57 ± 1.68a | 2.17 ± 1.52b | 3.15 ± 1.29c | .000** |
| FIM | 120.00 ± 12.73a | 114.16 ± 17.39b | 113.93 ± 18.05b | .000** | 88.70 ± 38.13a | 100.18 ± 30.85b | 82.80 ± 30.61a | .000** |
| K-MBI | 95.44 ± 11.90a | 90.03 ± 16.88b | 89.88 ± 17.34b | .000** | 69.11 ± 36.99a | 79.71 ± 28.65b | 63.41 ± 30.94a | .000** |
| FMA | 94.11 ± 15.80 | 91.19 ± 18.70 | 89.88 ± 17.34 | .119 | 72.75 ± 35.71a | 81.68 ± 30.77b | 63.65 ± 35.07c | .000** |
| FAC | 4.66 ± 0.87a | 6.59 ± 4.07b | 6.74 ± 4.40b | .000** | 3.10 ± 2.03a | 3.65 ± 1.77b | 2.66 ± 1.83a | .000** |
| GDS | 4.95 ± 3.79a | 6.59 ± 4.07b | 6.74 ± 4.40b | .000** | 7.25 ± 4.11a | 7.30 ± 4.32a | 9.31 ± 3.92b | .006** |
| EQ-5D | 0.78 ± 0.28a | 0.69 ± 0.33b | 0.65 ± 0.36b | .000** | 0.44 ± 0.41a | 0.53 ± 0.40b | 0.31 ± 0.37c | .000** |
n, Number; SD, Standard Deviation; BMI, Body Mass Index; TOAST, Trial of Org 10172 in Acute Stroke Treatment; Rt, Right; Lt, Left; IV, Intra-Venous; IA, Intra-Artrial; K-MMSE, Korean Mini Mental State Examination; NIHSS, National Institutes of Health Stroke Scale; mRS, modified Rankin Scale; ADL, Activity of Daily Living; FIM, Functional Independence Measure; K-MBI, Korean version of Modified Barthel Index; FMA, Fugl-Meyer Assessment; FAC, Functional Ambulation Categories; GDS, Geriatric Depression Scale; QoL, Quality of Life; EQ-5D, EuroQol-5D
* p < 0.05; ** p < 0.01
abc Post HOC group
Table 4.
Factors affecting cognitive change from 3 months to 12 months in older patients
| Parameters | Normal Cognition (n = 835) | Declined Cognition (n = 596) | ||||||
|---|---|---|---|---|---|---|---|---|
| Stable (n = 612) | Converter (n = 79) | Reverter (n = 144) | P value | Stable (n = 336) | Converter (n = 183) | Reverter (n = 77) | P value | |
| 1) Baseline medical record assessments | ||||||||
| Male, n (%) | 375 (61.3) | 37 (46.8) | 66 (45.8) | .000** | 163 (48.5) | 91 (49.7) | 38 (49.4) | .963 |
| Age, (mean ± SD) | 73.15 ± 5.86a | 75.24 ± 6.84b | 76.53 ± 6.21b | .000** | 76.06 ± 6.15 | 74.78 ± 5.55 | 75.95 ± 6.09 | .059 |
| Education, n (%) | ||||||||
| Uneducated | 98 (16.0) | 24 (30.4) | 41 (28.5) | .000** | 33 (9.8) | 10 (5.5) | 12 (15.6) | .307 |
| 0–3 years | 34 (5.6) | 9 (11.4) | 10 (6.9) | 36 (10.7) | 20 (10.9) | 9 (11.7) | ||
| 4–6 years | 132 (21.6) | 22 (27.8) | 43 (29.9) | 106 (31.5) | 61 (33.3) | 23 (29.9) | ||
| 7 - 9 years | 103 (16.8) | 12 (15.2) | 25 (17.4) | 74 (22.0) | 35 (19.1) | 17 (22.1) | ||
| 10 - 12 years | 142 (23.2) | 4 (5.1) | 15 (10.4) | 71 (21.1) | 41 (22.4) | 13 (16.9) | ||
| 13 years - | 103 (16.8) | 8 (10.1) | 10 (6.9) | 16 (4.8) | 16 (8.7) | 3 (3.9) | ||
| BMI (kg/m2), (mean ± SD) | 23.72 ± 3.20 | 23.59 ± 3.61 | 23.11 ± 3.43 | .115 | 23.00 ± 2.96 | 23.24 ± 3.15 | 22.26 ± 3.23 | .066 |
| Risk factors of stroke, n (%) | ||||||||
| Hypertension | 414 (67.6) | 54 (68.4) | 91 (63.2) | .570 | 212 (63.1) | 116 (63.4) | 55 (71.4) | .371 |
| Diabetes Mellitus | 102 (16.7) | 12 (15.2) | 15 (10.4) | .175 | 55 (16.4) | 28 (15.3) | 17 (22.1) | .392 |
| Coronary heart disease | 60 (9.8) | 8 (10.1) | 11 (7.6) | .711 | 27 (8.0) | 16 (8.7) | 5 (6.5) | .831 |
| Atrial fibrillation | 78 (12.7) | 11 (13.9) | 22 (15.3) | .712 | 59 (17.6) | 27 (14.8) | 10 (13.0) | .515 |
| Hyperlipidemia | 110 (18.0) | 11 (13.9) | 31 (21.5) | .357 | 39 (11.6) | 19 (10.4) | 12 (15.6) | .489 |
| Obesity | 79 (12.9) | 12 (15.2) | 11 (7.6) | .154 | 29 (8.6) | 20 (10.9) | 3 (3.9) | .185 |
| Family history | 52 (8.5) | 4 (5.1) | 11 (7.6) | .562 | 30 (8.9) | 12 (6.6) | 6 (7.8) | .635 |
| Smoking, n (%) | ||||||||
| Current smokers | 105 (17.2) | 11 (13.9) | 23 (16.0) | .050 | 67 (19.9) | 27 (14.8) | 19 (24.7) | .285 |
| Former smokers | 107 (17.4) | 10 (12.7) | 12 (8.3) | 39 (11.6) | 28 (15.3) | 8 (10.4) | ||
| Never smokers | 400 (65.4) | 58 (73.4) | 109 (75.7) | 230 (68.5) | 128 (69.9) | 50 (64.9) | ||
| Alcohol consumption, n (%) | ||||||||
| None | 414 (67.6) | 54 (68.4) | 108 (75.0) | .322 | 249 (74.1) | 133 (72.7) | 56 (72.7) | .367 |
| Moderate | 141 (23.0) | 20 (25.3) | 23 (16.0) | 63 (18.8) | 28 (15.3) | 15 (19.5) | ||
| Heavy | 57 (9.3) | 5 (6.3) | 13 (9.0) | 24 (7.1) | 22 (12.0) | 6 (7.8) | ||
| 2) Stroke characteristics | ||||||||
| Ischemic type (TOAST) | ||||||||
| Large-artery atherosclerosis | 278 (45.4) | 51 (64.6) | 67 (46.5) | .052 | 167 (49.7) | 94 (51.4) | 46 (59.7) | .662 |
| Small-artery occlusion | 155 (25.3) | 11 (13.9) | 39 (27.1) | 60 (17.9) | 34 (18.6) | 12 (15.6) | ||
| Cardioembolism | 89 (14.5) | 5 (6.3) | 17 (11.8) | 59 (17.6) | 28 (15.3) | 7 (9.1) | ||
| Other determined | 36 (5.9) | 4 (5.1) | 5 (3.5) | 15 (4.5) | 5 (2.7) | 4 (5.2) | ||
| Undetermined ischemic stroke | 54 (8.8) | 8 (10.1) | 16 (11.1) | 35 (10.4) | 22 (12.0) | 8 (10.4) | ||
| Ischemic location | ||||||||
| Rt. hemisphere | 309 (50.5) | 39 (49.4) | 64 (44.4) | .394 | 135 (40.2) | 68 (37.2) | 33 (42.9) | .667 |
| Lt. hemisphere | 247 (40.4) | 31 (39.2) | 70 (48.6) | 178 (53.0) | 106 (57.9) | 38 (49.4) | ||
| Both hemisphere | 56 (9.2) | 9 (11.4) | 10 (6.9) | 23 (6.8) | 9 (4.9) | 6 (7.8) | ||
| Affected level | ||||||||
| Cortical level | 203 (33.2) | 32 (40.5) | 49 (34.0) | .047* | 143 (42.6) | 75 (41.0) | 32 (41.6) | .729 |
| Subcortical level | 193 (31.5) | 20 (25.3) | 30 (20.8) | 83 (24.7) | 53 (29.0) | 21 (27.3) | ||
| Brainstem level | 125 (20.4) | 11 (13.9) | 40 (27.8) | 42 (12.5) | 20 (10.9) | 13 (16.9) | ||
| Multiple level | 91 (14.9) | 16 (20.3) | 25 (17.4) | 68 (20.2) | 35 (19.1) | 11 (14.3) | ||
| 3) Treatment characteristics | ||||||||
| IV thrombolysis | 40 (6.5) | 5 (6.3) | 9 (6.3) | .991 | 27 (8.0) | 16 (8.7) | 7 (9.1) | .935 |
| IA thrombolysis | 9 (1.5) | 2 (2.5) | 3 (2.1) | .722 | 20 (6.0) | 4 (2.2) | 1 (1.3) | .049* |
| IV heparin | 52 (8.5) | 5 (6.3) | 9 (6.3) | .575 | 29 (8.6) | 10 (5.5) | 8 (10.4) | .301 |
| Antiplatelet agent | 485 (79.2) | 65 (82.3) | 115 (79.9) | .818 | 239 (71.1) | 131 (71.6) | 53 (68.8) | .901 |
| Rehabilitation Therapy | 157 (25.7) | 25 (31.6) | 43 (29.9) | .363 | 133 (39.6) | 54 (29.5) | 36 (46.8) | .015* |
| Cognitive Therapy | 26 (4.2) | 4 (5.1) | 5 (3.5) | .844 | 19 (5.7) | 11 (6.0) | 10 (13.0) | .061 |
| 4) Neuropsychological assessments | ||||||||
| Cognitive function (K-MMSE) | ||||||||
| 3 months from onset | 26.86 ± 3.41a | 23.18 ± 3.69b | 25.85 ± 3.82c | .000** | 14.46 ± 9.71 | 15.95 ± 7.64 | 16.08 ± 7.09 | .112 |
| 12 months from onset | 26.88 ± 3.50a | 27.01 ± 3.30a | 20.66 ± 4.90b | .000** | 14.68 ± 9.95a | 22.46 ± 5.78b | 10.52 ± 7.21c | .000** |
| Variation (from 3 months to 12 months) | 0.03 ± 1.17a | 3.84 ± 1.31b | −5.19 ± 3.05c | .000** | 0.21 ± 1.10a | 6.51 ± 4.03b | −5.56 ± 2.99c | .000** |
| Stroke Severity, ADL, Motor, Gait, Depression, QoL (3 months from onset) | ||||||||
| NIHSS | 0.78 ± 1.98a | 1.15 ± 2.06a | 1.32 ± 2.15b | .009** | 5.75 ± 7.43a | 3.17 ± 4.69b | 5.08 ± 4.68b | .000** |
| mRS | 1.12 ± 1.12a | 1.51 ± 1.32b | 1.63 ± 1.25b | .000** | 2.79 ± 1.68a | 2.37 ± 1.54b | 3.26 ± 1.29a | .000** |
| FIM | 117.40 ± 15.58a | 113.08 ± 18.30ab | 111.16 ± 19.83b | .000** | 83.68 ± 39.78a | 95.74 ± 32.33b | 81.34 ± 31.60a | .001** |
| K-MBI | 93.31 ± 16.11a | 89.09 ± 17.82ab | 87.34 ± 19.10b | .000** | 64.13 ± 38.83a | 75.71 ± 30.51b | 61.61 ± 32.50a | .001** |
| FMA (affected side) | 93.92 ± 16.11 | 90.53 ± 19.31 | 91.44 ± 17.83 | .094 | 70.49 ± 36.80a | 81.45 ± 30.54b | 65.90 ± 35.97a | .000** |
| FAC | 4.51 ± 1.05a | 4.15 ± 1.40b | 4.00 ± 1.35b | .000** | 2.83 ± 2.10a | 3.45 ± 1.79b | 2.70 ± 1.87a | .001** |
| GDS | 5.40 ± 3.79a | 6.83 ± 4.19b | 7.41 ± 4.35b | .000** | 7.63 ± 4.09a | 8.03 ± 4.27ab | 9.65 ± 4.04b | .022* |
| EQ-5D | 0.76 ± 0.29a | 0.67 ± 0.34b | 0.63 ± 0.36b | .000** | 0.39 ± 0.41a | 0.49 ± 0.40b | 0.31 ± 0.37a | .003** |
n, Number; SD, Standard Deviation; BMI, Body Mass Index; TOAST, Trial of Org 10172 in Acute Stroke Treatment; Rt, Right; Lt, Left; IV, Intra-Venous; IA, Intra-Artrial; K-MMSE, Korean Mini Mental State Examination; NIHSS, National Institutes of Health Stroke Scale; mRS, modified Rankin Scale; ADL, Activity of Daily Living; FIM, Functional Independence Measure; K-MBI, Korean version of Modified Barthel Index; FMA, Fugl-Meyer Assessment; FAC, Functional Ambulation Categories; GDS, Geriatric Depression Scale; QoL, Quality of Life; EQ-5D, EuroQol-5D
* p < 0.05; ** p < 0.01
abc Post HOC group
Discussion
In our study, total the percentage of cognitive impairment group did not change at 12 months compared to 3 months assessment. Otherwise, the percentage of cognitive impairment at 3 months, the percentage of patients in the reverter group, and the percentage of patients transferring from the NCG to the ICG at 12 months were higher in older patients compared to total group analysis (Table 2) (Fig. 2). Influencing factors for delayed cognitive change were discretely determined in the NCG and ICG of total and older patients. Hypertension history and onset age, sex, education level were somewhat repeated influencing factors. Although presence of atrial fibrillation, smoking, alcohol history showed statistical significance, large difference of number of patients between groups made it difficult to define it as meaningful result. Another unique aspect of our study is that we included functional assessment since it could influence on patients’ delayed cognitive function. Patients with better functional assessment scores not only in cognitive field but in all other domains including activities of daily living, motor function, mobility and gait, general functional level, quality of life at 3 month tend to have less cognitive decline and more cognitive improvement from 3 month to 12 month. Otherwise, stroke characteristics including ischemic type, location, treatment characteristics showed no significant difference between the groups. Patients in the ICG-RG that were aged >65 years received more rehabilitation therapy. Moreover, compared to the other patient groups, the patients in the ICG-SG received less cognitive therapy, which was a component of the rehabilitation therapy. We believe that unlike the other factors, the administration of rehabilitation treatment depended on the cognitive status of the patient; however, rehabilitation was not a factor that improved cognitive function.
Stroke severity, onset age, pre-stroke cognitive function, level of education, and bilateral lesions are well-known factors associated with development of post-stroke dementia [33–36]. In contrast, a cohort study of younger stoke patients (mean age, 60 years) showed that more than 30% of the patients with mild cognitive impairments between 0 and 6 months were classified as cognitively intact by 12 to 18 months [16]. For older patients (mean age, 80.4 ± 3.8), about 50% of the patients experienced an improvement in MMSE at 15 months [17]. As the prognosis of stroke varies according to the patient’s age at onset, identifying the factors affecting cognitive changes by age might aid in both preventing secondary cognitive decline, and enhancing post-stroke cognitive function. In our study, separating patients by age, cognitive function at 3 month, and aspect of cognitive change to find the propensity of each prevalence and influencing factors was meaningful. Also, compared to other cross sectional studies, our study analyzed delayed post stroke cognitive function and focused on amount and aspect of cognitive change from 3 month to 12 month and its influencing factors.
To carry this analysis further, we examined the differences in the MMSE scores among the groups by using the cutoff score of <24 points, conventionally accepted for the diagnosis of significant cognitive impairment, i.e., dementia [37]. Previous studies have established more than 3 points of MMSE variability as a significant change for improvement or decline in cognitive function.
MMSE is the most frequently applied test for dementia screening. A systematic review and meta-analysis examining cognitive tests to detect dementia found 10,263 cases of dementia identified from 36,080 participants in 108 cohort studies. The result reported a sensitivity of 0.81 and a specificity of 0.89 for the MMSE [38]. The MMSE requires only 5–10 min to evaluate various cognitive domains (orientation, memory, language, attention, visuospatial) and is practical to use serially and routinely [39].
The overall prevalence of dementia in subjects aged greater than 65 in Korea is estimated to be 9.2%. In addition, the pooled age-specific prevalence of dementia is estimated to increase with each 5-year age band (65–69 years) [40]. This result is much higher than the estimated overall prevalence of dementia in Asian people [41]. We analyzed our data by separating patients older than 65 y/o to compare the age factors. The percentages of normal cognitive group and cognitive impaired patients and mean MMSE scores showed significant differences between total and older patient groups. In particular, the percentage of patients in the reverter group was higher and the converter group was lower at 12 months in older patient group, and their average MMSE showed differences by age. Otherwise, in older ICG, less factors were significant compared to other groups. This finding may be due to the lower percentage of patients when compared to the entire study population and NCG.
Limitations
First, we only used a MMSE to test cognitive function. Although there are 40 other more detailed tests for dementia diagnosis in healthcare settings, we required multi-domain, serial functional assessments for screening and detecting post stroke cognitive decline. Also, MMSE was optimal for our insurance benefits and medical policy which can be done consecutively for our large-scale cohort study [40].
Second, we excluded patients with pre-stroke cognitive decline, but we had no objective assessment data on which to base our exclusions. Instead, patients’ pre-stroke cognitive function was determined by administered questionnaires and face-to-face interviews. Additional studies, such as volumetric analysis by MRI/MRA scans, may be valuable to investigate and compare the severity of stroke among the groups.
Third, we excluded patients who are not capable of 1 year follow up examination including functional assessments which could make selection bias. However, it could be a strength of this cohort study which differs from others and it may suggest more objective data for stroke survivors.
Conclusions
The prevalence of cognitive impairment at 3 month showed difference between total and older patient groups. To analyze the cognitive change from 3 month to 12 month, the proportion stable group was dominant in NCG and converter group was higher in ICG. By investigating the influencing factors from each group, we were able to identify the early predictors including the age factor.
Acknowledgments
Funding
This study was supported by the research program funded by the Korea Centers for Disease Control and Prevention (2013-2013E3301702).
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
JAY, YIS, KPP, MSP: contribution to conception and design; acquisition of data; involvement in drafting the manuscript; final approval of the version to be published. MKS, JL, DYK, SGL, YIS, GJO, KHN, WHC: contribution to conception and design; acquisition of data; final approval of the version to be published. YSL, MCJ, EYH, JHH: acquisition of data; final approval of the version to be published. YHK: contribution to conception and design; acquisition of data; revising the manuscript critically; final approval of the version to be published. All authors read and approved the final manuscript.
Competing interest
The authors declare that they have no competing interest.
Consent for publication
Not applicable.
Ethics approval and consent to participate
The study was approved by the Research Ethics Committee of the Pusan National University Yangsan Hospital and all patients provided written informed consent.
Abbreviations
- CG
Converter group
- EQ-5D
Euro quality of Life
- FAC
Functional ambulatory category
- FIM
Functional independence measure
- FMA
Fugl-meyer assessment
- GDS-SF
Geriatric depression scale-short form
- ICG
Impaired cognitive group
- K-MBI
Korean modified Barthel index
- K-MMSE
Korean mini-mental State examination
- K-NIHSS
Korean national institute of health stroke scale
- KOSCO
Korean stroke cohort for functioning and rehabilitation
- mRS
Modified rankin scale
- NCG
Normal cognitive group
- RG
Reverter group
- SG
Stable group
Contributor Information
Jin A. Yoon, Email: yjk5289@naver.com
Deog Young Kim, Email: kimdy@yuhs.ac.
Min Kyun Sohn, Email: mksohn@cnu.ac.kr.
Jongmin Lee, Email: leej@kuh.ac.kr.
Sam-Gyu Lee, Email: lee9299@daum.net.
Yang-Soo Lee, Email: leeyangsoo@knu.ac.kr.
Eun Young Han, Email: clearblue10@naver.com.
Min Cheol Joo, Email: mcjoo68@wonkwang.ac.kr.
Gyung-Jae Oh, Email: pmokj@wonkwang.ac.kr.
Junhee Han, Email: punyh.rass@gmail.com.
Minsu Park, Email: minus.park.otr@gmail.com.
Kyung Pil Park, Email: kppark@pusan.ac.kr.
Kyung-Ha Noh, Email: coolnoh@gmail.com.
Won Hyuk Chang, Email: wh.chang@samsung.com.
Yong-Il Shin, Phone: +82-55-360-4250, Email: rmshin@pusan.ac.kr.
Yun-Hee Kim, Phone: +82-2-3410-2824, Email: yunkim@skku.edu.
References
- 1.Hebert R, Brayne C. Epidemiology of vascular dementia. Neuroepidemiology. 1995;14:240–257. doi: 10.1159/000109800. [DOI] [PubMed] [Google Scholar]
- 2.Leys D, Pasquier F, Parnetti L. Epidemiology of vascular dementia. Haemostasis. 1998;28:134–150. doi: 10.1159/000022425. [DOI] [PubMed] [Google Scholar]
- 3.Skoog I, Nilsson L, Palmertz B, Andreasson LA, Svanborg A. A population-based study of dementia in 85-year-olds. N Engl J Med. 1993;328:153–158. doi: 10.1056/NEJM199301213280301. [DOI] [PubMed] [Google Scholar]
- 4.de Haan R, Limburg M, Van der Meulen J, Jacobs H, et al. Quality of life after stroke impact of stroke type and lesion location. Stroke. 1995;26:402–408. doi: 10.1161/01.STR.26.3.402. [DOI] [PubMed] [Google Scholar]
- 5.Pohjasvaara T, Erkinjuntti T, Ylikoski R, Hietanen M, et al. Clinical determinants of poststroke dementia. Stroke. 1998;29:75–81. doi: 10.1161/01.STR.29.1.75. [DOI] [PubMed] [Google Scholar]
- 6.Tatemichi TK, Foulkes MA, Mohr JP, Hewitt JR, Hier DB, Price TR, Wolf PA. Dementia in stroke survivors in the stroke data bank cohort: prevalence, incidence, risk factors, and computed tomographic findings. Stroke. 1990;21:858–866. doi: 10.1161/01.STR.21.6.858. [DOI] [PubMed] [Google Scholar]
- 7.He’non H, Pasquier F, Durieu I, Godefroy O, Lucas C, Lebert F, Leys D. Preexisting dementia in stroke patients: baseline frequency, associated factors, and outcome. Stroke. 1997;28:2429–2436. doi: 10.1161/01.STR.28.12.2429. [DOI] [PubMed] [Google Scholar]
- 8.Tomlinson BE, Blessed G, Roth M. Observations on the brains of demented old people. J Neurol Sci. 1970;11:205–242. doi: 10.1016/0022-510X(70)90063-8. [DOI] [PubMed] [Google Scholar]
- 9.Katzman R. Vascular disease and dementia. In: Yahr MD, editor. H. Houston Merritt memorial volume. New York: Raven; 1983. pp. 153–176. [Google Scholar]
- 10.Madureira S, Guerreiro M, Ferro JM. Dementia and cognitive impairment three months after stroke. Eur J Neurol. 2001;8:621–27. doi: 10.1046/j.1468-1331.2001.00332.x. [DOI] [PubMed] [Google Scholar]
- 11.Henon H, Durieu I, Guerouaou D, Lebert F, Pasquier F, Leys D. Poststroke dementia: incidence and relationship to prestrike cognitive decline. Neurology. 2001;57:1216–22. doi: 10.1212/WNL.57.7.1216. [DOI] [PubMed] [Google Scholar]
- 12.Inzitari D, Di Carlo A, Pracucci G, Lamassa M, Vanni P, Romanelli M, et al. Incidence and determinants of poststroke dementia as defined by an informant interview method in a hospital-based stroke registry. Stroke. 1998;29:2087-93. [DOI] [PubMed]
- 13.Henon H, Pasquier F, Leys D. Poststroke dementia. Cerebrovasc Dis. 2006;22:61–70. doi: 10.1159/000092923. [DOI] [PubMed] [Google Scholar]
- 14.Snaphaan L, de Leeuw FE. Poststroke memory function in nondemented patients: a systematic review on frequency and neuroimaging correlates. Stroke. 2007;38:198–203. doi: 10.1161/01.STR.0000251842.34322.8f. [DOI] [PubMed] [Google Scholar]
- 15.Desmond DW, Moroney JT, Sano M, Stern Y. Recovery of cognitive function after stroke. Stroke. 1996;27:1798–1803. doi: 10.1161/01.STR.27.10.1798. [DOI] [PubMed] [Google Scholar]
- 16.Tham W, Auchus AP, Thong M, Goh M-L, Chang H-M, Wong M-C, Chen C. Progression of cognitive impairment after stroke: one year results from a longitudinal study of Singaporean stroke patients. J Neurol Sci. 2002;203–204:49–52. doi: 10.1016/S0022-510X(02)00260-5. [DOI] [PubMed] [Google Scholar]
- 17.Ballard C, Rowan E, Stephens S, Kalaria R, Kenny RA. Prospective follow-up study between 3 and 15 months after stroke improvements and decline in cognitive function among dementia-free stroke survivors >75 years of Age. Stroke. 2003;34:2440–2445. doi: 10.1161/01.STR.0000089923.29724.CE. [DOI] [PubMed] [Google Scholar]
- 18.Lowery K, Ballard C, Rodgers H, McLaren A, O’Brien J, Rowan E, Stephens S. Cognitive decline in a prospectively studied group of stroke survivors, with a particular emphasis on the 75’s. Age Ageing. 2002;31(suppl 3):24–27. doi: 10.1093/ageing/31.suppl_3.24. [DOI] [PubMed] [Google Scholar]
- 19.Pohjasvaara T, Erkinjuntti T, Vataja R, Kaste M. Clinical determinants of post-stroke dementia in the Helsinki stroke aging memory study (SAM) cohort. Stroke. 1997;28:785–792. doi: 10.1161/01.STR.28.4.785. [DOI] [PubMed] [Google Scholar]
- 20.Chang WH, Sohn MK, Lee J, et al. Korean stroke cohort for functioning and rehabilitation (KOSCO): study rationale and protocol of a multi-centre prospective cohort study. BMC Neurol. 2015;15:42. doi: 10.1186/s12883-015-0293-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass LM, Bushnell CD, et al. Primary prevention of ischemic stroke. Stroke. 2006;37:1583–1633. doi: 10.1161/01.STR.0000223048.70103.F1. [DOI] [PubMed] [Google Scholar]
- 22.Bernardini J, Callen S, Fried L, Piraino B. Inter-rater reliability and annual rescoring of the Charlson comorbidity index. Adv Perit Dial. 2004;20:125–127. [PubMed] [Google Scholar]
- 23.Oh MS, Yu KH, Lee JH, Jung S, Ko IS, Shin JH, et al. Validity and reliability of a Korean version of the national institutes of health stroke scale. J Clin Neurol. 2012;8:177–83. doi: 10.3988/jcn.2012.8.3.177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Amarenco P, Bogousslavsky J, Caplan LR, Donnan GA, Hennerici MG. Classification of stroke subtypes. Cerebrovasc Dis. 2009;27:493–501. doi: 10.1159/000210432. [DOI] [PubMed] [Google Scholar]
- 25.Kang Y, Na DL, Hahn S. A validity study on the Korean mini-mental state examination (K-MMSE) in dementia patients. J Korean Neurol Assoc. 1997;15:300–8. [Google Scholar]
- 26.Dodds TA, Martin DP, Stolov WC, Deyo RA. A validation of the functional independence measurement and its performance among rehabilitation inpatients. Arch Phys Med Rehabil. 1993;74:531–6. doi: 10.1016/0003-9993(93)90119-U. [DOI] [PubMed] [Google Scholar]
- 27.Jung HY, Park BK, Shin HS, Kang YK, Pyun SB, Paik NJ, et al. Development of the Korean version of modified barthel index (K-MBI): multi-center study for subjects with stroke. J Korean Acad Rehabil Med. 2007;31:283–97. [Google Scholar]
- 28.Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1. A method for evaluation of physical performance. Scand J Rehabil Med. 1975;7:13–31. [PubMed] [Google Scholar]
- 29.Holden MK, Gill KM, Magliozzi MR, Nathan J, Piehl-Baker L. Clinical gait assessment in the neurologically impaired. Reliability and meaningfulness Phys Ther. 1984;64:35–40. doi: 10.1093/ptj/64.1.35. [DOI] [PubMed] [Google Scholar]
- 30.Burn JP. Reliability of the modified Rankin scale. Stroke. 1992;23:438. [PubMed] [Google Scholar]
- 31.Lesher EL, Berryhill JS. Validation of the geriatric depression scale–short form among inpatients. J Clin Psychol. 1994;50:256–60. doi: 10.1002/1097-4679(199403)50:2<256::AID-JCLP2270500218>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 32.Greiner W, Claes C, Busschbach JJ, von der Schulenburg JM. Validating the EQ-5D with time trade off for the German population. Eur J Health Econ. 2005;6:124–30. doi: 10.1007/s10198-004-0264-z. [DOI] [PubMed] [Google Scholar]
- 33.Pendlebury ST, Rothwell PM. Prevalence, incidence, and factors associatted with pre-stroke and poststroke dementia: a systematic review and meta-analysis. Lancet Neurol 2009;8(11):1006–18. [DOI] [PubMed]
- 34.Inzitari D, Di Carlo A, Pracucci G, Lamassa M, Vanni P, Romanelli M, Spolveri S, Adriani P, Meucci I, Landini G, Ghetti A. Incidence and determinants of poststroke dementia as defined by an informant interview method in a hospital-based stroke registry. Stroke. 1998;29:2087–2093. doi: 10.1161/01.STR.29.10.2087. [DOI] [PubMed] [Google Scholar]
- 35.Desmond DW, Moroney JT, Paik MC. Frequency and clinical determinants of dementia after ischemic stroke. Neurology. 2000;54:1124–1131. doi: 10.1212/WNL.54.5.1124. [DOI] [PubMed] [Google Scholar]
- 36.Barba R, Martinez ES, Rodriguez GE, Pondal M, Vivancos J, Del Ser T. Poststroke dementia: clinical features and risk factors. Stroke. 2000;31:1494–1501. doi: 10.1161/01.STR.31.7.1494. [DOI] [PubMed] [Google Scholar]
- 37.Tatemichi TK, Desmond DW, Paik M, et al. The mini-mental state examination as a screen for dementia following stroke [abstract] J Clin Exp Neuropsychol. 1991;13:419. [Google Scholar]
- 38.Tsoi K, Chan J, Hirai H, Wong S, Kwok T. Cognitive tests to detect dementia a systematic review and meta-analysis. JAMA Intern Med. 2015;175:1450–1458. doi: 10.1001/jamainternmed.2015.2152. [DOI] [PubMed] [Google Scholar]
- 39.Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–198. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- 40.Kim YJ, Han JW, So YS, Seo JY, Kim KY, Kim KW. Prevalence and trends of dementia in Korea: a systematic review and meta-analysis. J Korean Med Sci. 2014;29:903–912. doi: 10.3346/jkms.2014.29.7.903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Alzheimer’s Disease International. World Alzheimer’s report 2009. London: Alzheimer’s Disease International, 2009. p. 26.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.