

Abstract
Context:
Metabolic acidosis is frequently found in patients with severe sepsis. An understanding of types of acidosis in sepsis and their evolution over the course of treatment may give us insight into the behavior of acid–base balance in these patients.
Aims:
To describe at Intensive Care Unit (ICU) admission and over the first 5 days the composition of metabolic acidosis in patients with sepsis and to evaluate and compare acidosis patterns in survivors and nonsurvivors.
Settings and Design:
A prospective study conducted at Amrita Institute of Medical Sciences, Kochi, Kerala, in the Department of Internal Medicine.
Subjects and Methods:
Seventy-five consecutive patients admitted in the medical ICU with sepsis and metabolic acidosis were assessed. Arterial blood gas and serum electrolytes were measured during the first five days of admission or until death, renal replacement or discharge supervened.
Statistical Analysis:
To test the statistical significance of the difference in mean values of different study variables at day 1 and last day between survivors and non survivors, Mann–Whitney U-test was applied. To test the statistical significance of the difference in mean changes in different study parameters from day 1 to last day, paired t-test was done in the survivor group and Mann–Whitney U-test in the non survivor group.
Results:
Regardless of survival status, on day 1 of admission, 37 had High Anion Gap metabolic acidosis (HAGMA), 21 had predominant lactic acidosis (LA), 8 had Normal anion gap metabolic acidosis (NAGMA), and 9 had both HAGMA and LA [Figure 1]. When we compared this to the last day, 25 had HAGMA, 3 had LA, 3 had both HAGMA and LA, and 22 patients had resolution of acidosis. Sixty–four patients survived for up to 5 days of admission. Fifteen of these patients underwent hemodialysis on the day of admission itself in view of HAGMA. The remaining 49 comprised of HAGMA (31), Lactic acidosis (12), and a combination (6) on day 1. On the last day in this group, 25 had HAGMA, 2 had LA, and 22 patients had resolution of acidosis. In survivors, over the observation period, changes seen were: mean pH: 7.25–7.34 (P < 0.001), mean serum bicarbonate: 13.9 mEq to 17.2 mEq (P < 0.001), and mean serum lactate: 3.18–1.9 (P = 0.002). The changes in serum albumin and pCO2 were not significant. Eleven patients in the study population succumbed. Seven patients underwent hemodialysis on day 1 and the remaining four were followed up for more than 1 day. On day 1, 7 had lactic acidosis and 5 had HAGMA. Over the observation period, changes seen were mean pH: 7.15–7.14, mean serum lactate: 6.3–7.3 mEq.
Conclusions:
In patients with sepsis and septic shock, high anion gap metabolic acidosis is the dominant blood gas anomaly. Fall in lactate levels over the first 5 days of admission is a good prognostic marker of survival. Evolution of the blood gas profile over time suggests that a fall in lactate levels and a rise in bicarbonate levels correlate with a better outcome. The role of the anion gap as a prognostic marker holds promise and further studies are needed in this regard.
Key Words: Anion gap, lactic acidosis, metabolic acidosis, sepsis
INTRODUCTION
Metabolic acidosis is frequently found in patients with severe sepsis. Several studies have shown that the amount of metabolic acidosis and its evolution over hospital stay has an effect on the prognosis. However, the precise composition of metabolic acidosis in these patients is not well known. Metabolic acidosis in severe sepsis may be secondary to lactic acidosis, but studies have shown that there is an unidentified anion contributing to high anion gap metabolic acidosis in addition to lactate.[1] Alterations in acid–base balance occur both as part of the pathophysiology of the underlying disease and as part of therapeutic interventions.[2] Thus, an understanding of types of acidosis in sepsis and their evolution over the course of treatment may give us insight into the behavior of acid–base balance in these patients.
Aims and objectives
To describe at Intensive Care Unit (ICU) admission and over the first 5 days the composition of metabolic acidosis in patients with sepsis and to evaluate and compare acidosis patterns in survivors and non survivors.
SUBJECTS AND METHODS
It was a prospective study conducted at Amrita Institute of Medical Sciences, Kochi, Kerala, in the Department of Internal Medicine and done on patients with sepsis as defined by the standard criteria. ICU consecutive patients admitted in the medical ICU with sepsis and metabolic acidosis were assessed. This sample size had an allowable error of 28% on the estimate of mortality. Arterial blood gas and serum electrolytes were measured during the first 5 days of admission or until death, renal replacement, or discharge supervened. The arbitrary period of 5 days was decided based on previous studies conducted.[3] Hereafter, for the purpose of discussion, day 1 indicates the day of admission and last day indicates either day 5 after admission or until hemodialysis or death supervened. All patients above the age of 18 years were admitted with sepsis/septic shock according to internationally accepted guidelines, irrespective of comorbid diseases.
Statistical analysis
Percentage of mortality in ICU patients of metabolic acidosis and sepsis over the first 5 days of ICU admission was computed. To test the statistical significance of the difference in mean values of different study variables at day 1 and last day between survivors and non -survivors, Mann–Whitney U-test was applied. To test the statistical significance of the difference in mean changes in different study parameters from day 1 to last day, paired t-test was done in the survivor group and Mann–Whitney U-test in the nonsurvivor group.
RESULTS
Regardless of survival status, on day 1 of admission, 37 had HAGMA, 21 had predominant LA, 8 had NAGMA, and 9 had both HAGMA and LA [Figure 1]. When we compared this to the last day, 25 had HAGMA, 3 had LA, 3 had both HAGMA and LA, and 22 patients had resolution of acidosis.
Figure 1.
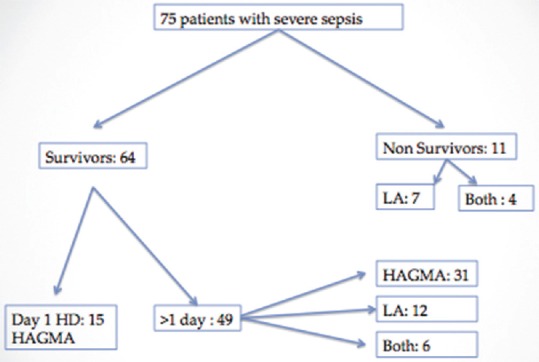
Study design
Sixty-four patients survived for up to 5 days of admission. Fifteen of these underwent hemodialysis on the day of admission itself in view of HAGMA. The remaining 49 comprised HAGMA (31), lactic acidosis (12), and a combination (6) on day 1. On the last day in this group, 25 had HAGMA, 2 had LA, and 22 patients had resolution of acidosis. In survivors, over the observation period, changes seen were mean pH: 7.25–7.34 (P < 0.001), mean serum bicarbonate: 13.9 mEq to 17.2 mEq (P < 0.001), and mean serum lactate: 3.18–1.9 (P = 0.002). The changes in serum albumin and pCO2 were not significant. Eleven patients in the study population succumbed. Seven patients underwent hemodialysis on day 1 and the remaining four were followed up for more than 1 day. On day 1, 7 had lactic acidosis and 5 had HAGMA. Over the observation period, changes seen were mean pH: 7.15–7.14, mean serum lactate: 6.3–7.3 mEq.
DISCUSSION
The 5-day survival rate among patients who were admitted in the ICU with sepsis and metabolic acidosis in our study was 85%. High anion gap metabolic acidosis was the most common pattern observed on admission. Among the 64 survivors of sepsis and metabolic acidosis, the predominant initial presentation was HAGMA. Among the 11 nonsurvivors, lactic acidosis was the dominant abnormality. Correlation of sepsis and the type of metabolic acidosis is complex, and various studies have yielded different results. The high incidence of a HAGMA in our study was significant. However, patients were chosen from within multiple specialties. We did not have any exclusion criteria as the attempt was to describe a baseline profile. Further investigation into the causes of the HAGMA is required. Forty–six percent of our patients were diabetic and 38% had chronic kidney disease, albeit not on maintenance hemodialysis. Almost 14.6% of these patients succumbed within a period of 5 days. In non survivors, lactic acidosis was the predominant initial presenting pattern. Mean albumin levels were lower in nonsurvivors and lactate levels higher showing a possible correlation with mortality. The high anion gap metabolic acidosis requires further investigation and study. An increased anion gap suggests the presence of unidentified anions that contribute to metabolic acidosis in patients with sepsis. In our study as well, HAGMA without lactic acidosis accounted for the majority of the patients. Hence, anion gap can also be used as a screening tool and a surrogate for lactic acid levels, thus helping in disease prognostication.[4]
Base excess and the fall in base excess over ICU stay may also be a prognostic marker of these patients.
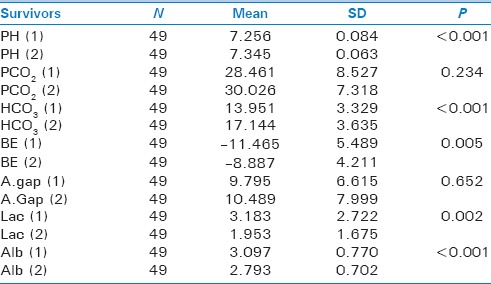
The evolution of acidosis over the 5-day period revealed that an increase in mean pH, mean bicarbonate, and a reduction in lactate, favored survival. Mean pH and mean bicarbonate levels were lower, and mean lactate levels were higher in non survivors [Table 1]. The change in pH (7.2–7.3), bicarbonate concentration (13.9–17.2 mEq), and lactate (3.1–1.9 mEq) in the survivor group was statistically significant [Table 2]. There was also a resolution of acidosis in 44.8% of patients. Although majority of patients on day 1 had HAGMA, there was no significant change in the anion gap over time, probably accounted for by other confounding factors such as use of intravenous fluids (mainly normal saline) and intravenous albumin. For the same reason, the observed change in albumin may not be an accurate description of the actual underlying process.
Table 1.
Comparison of different study variables between survivors and non survivors on Day 1 and last day
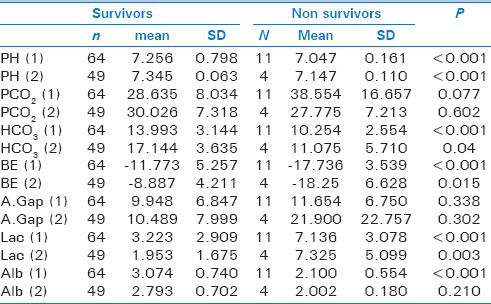
Table 2.
Change in different study variables from Day 1 to last day in Survivors
Lactic acidosis is most commonly associated with sepsis.[5] Non survivors had a lower mean pH and higher mean lactate levels than survivors.
Our study showed a higher incidence of lactic acidosis among nonsurvivors, thus indicating that lactate may be a factor useful in prognostification. Lactate levels are an important prognostic marker in patients with sepsis and septic shock.[6,7] Both point lactate-monitoring[8] and serial estimation are prognostic markers of sepsis. Our results seem to corroborate these data as early as 5 days into the condition. However, lactic acidosis does not entirely account for the metabolic acidosis during severe sepsis.
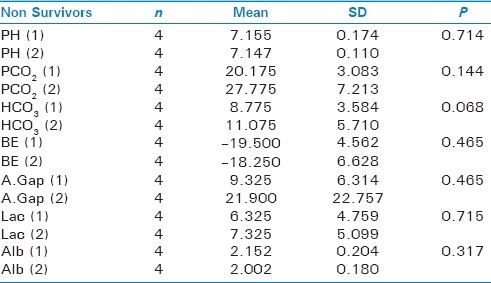
Nonsurvivors showed a lower mean pH, bicarbonate, and albumin and a higher mean lactate and base excess than survivors. There was a rise in anion gap in the nonsurvivors which was not statistically significant, probably for reasons stated earlier [Table 3].
Table 3.
Change in different study variables from Day 1 to last day in Non Survivors
Initial albumin values were lower in nonsurvivors. Over the course of ICU stay, both survivors and nonsurvivors exhibited a fall in albumin values. Statistical significance was achieved for the survivor group, and not for the nonsurvivors. In the survivors, a mean albumin of 3.09 ± 0.77 (standard deviation [SD]) at initial presentation fell to 2.79 ± 0.70 (SD). In nonsurvivors, due to small sample size, statistical significance is not possible, but nonsurvivors in our study showed both a lower level of albumin on day 1 of admission (mean 2.15) and a greater fall in albumin on the last day. Thus, albumin may have a role in ultimate prognosis, the derivation of which requires further studies.
CONCLUSIONS
In patients with sepsis and septic shock, high anion gap metabolic acidosis is the dominant blood gas anomaly. Fall in lactate levels over the first 5 days of admission is a good prognostic marker of survival. Evolution of the blood gas profile over time suggests that a fall in lactate levels and a rise in bicarbonate levels correlate with a better outcome. The role of the anion gap as a prognostic marker holds promise and further studies are needed in this regard.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Mecher C, Rackow EC, Astiz ME, Weil MH. Unaccounted for anion in metabolic acidosis during severe sepsis in humans. Crit Care Med. 1991;19:705–11. doi: 10.1097/00003246-199105000-00018. [DOI] [PubMed] [Google Scholar]
- 2.Kellum JA. Metabolic acidosis in patients with sepsis: Epiphenomenon or part of the pathophysiology? Crit Care Resusc. 2004;6:197–203. [PubMed] [Google Scholar]
- 3.Noritomi DT, Soriano FG, Kellum JA, Cappi SB, Biselli PJ, Libório AB, et al. Metabolic acidosis in patients with severe sepsis and septic shock: A longitudinal quantitative study. Crit Care Med. 2009;37:2733–9. doi: 10.1097/ccm.0b013e3181a59165. [DOI] [PubMed] [Google Scholar]
- 4.Berkman M, Ufberg J, Nathanson LA, Shapiro NI. Anion gap as a screening tool for elevated lactate in patients with an increased risk of developing sepsis in the Emergency Department. J Emerg Med. 2009;36:391–4. doi: 10.1016/j.jemermed.2007.12.020. [DOI] [PubMed] [Google Scholar]
- 5.Smith I, Kumar P, Molloy S, Rhodes A, Newman PJ, Grounds RM, et al. Base excess and lactate as prognostic indicators for patients admitted to intensive care. Intensive Care Med. 2001;27:74–83. doi: 10.1007/s001340051352. [DOI] [PubMed] [Google Scholar]
- 6.Rocha LL, Pessoa CM, Colombo G, Correa TD, de Assunção MS. Lactate as a prognostic marker in patients with severe sepsis or septic shock admitted to the ICU. Crit Care. 2013;17(Suppl 3):P51. [Google Scholar]
- 7.Blomkalns AL. Lactate: A marker for sepsis and trauma. Available from: http://www.emcreg.org .
- 8.Agrawal A, Agrawal N, Das J, Varma A. Point of care serum lactate levels as a prognostic marker of outcome in complex pediatric cardiac surgery patients: Can we utilize it? Indian J Crit Care Med. 2012;16:193–7. doi: 10.4103/0972-5229.106500. [DOI] [PMC free article] [PubMed] [Google Scholar]