

SUMMARY
This is a case of successful cochlear implantation in a 50-year-old man who experienced sudden hearing loss and developed ipsilateral severe tinnitus at three years following conservative stage 1 vestibular schwannoma retrosigmoid surgery. After cochlear implantation, tinnitus improved from THI grade 4 to 2. Localisation skills improved. Hearing in noise (S/N + 7 dB) with target signal from the operated side improved from 38 to 100% of correct answers. A significant improvement of spatial and speech items of the "speech, spatial and qualities of sounds" questionnaire was also measured. In conclusion, cochlear implantation is a feasible and effective solution after conservative vestibular schwannoma surgery should delayed hearing loss occur.
KEY WORDS: Cochlear implant, Vestibular schwannoma, Single-sided deafness
RIASSUNTO
Presentiamo un caso di posizionamento di impianto cocleare in un uomo di 50 anni che, dopo aver subito tre anni prima un intervento per via retrosigmoidea per un neurinoma dell'acustico in stadio 1, è stato colpito da ipoacusia improvvisa ipsilaterale sviluppando un intenso acufene. Dopo l'attivazione dell'impianto l'acufene è sceso da un grado 4 ad un grado 2 secondo il THI. Sono migliorate le capacità di localizzazione. L'ascolto nel rumore (S/R + 7 dB) con il segnale proveniente dal lato operato è migliorato da 38 a 100%. Abbiamo inoltre verificato un significativo incremento dei punteggi relativi a spazialità e linguaggio del questionario "Speech, spatial and qualities of sounds". In conclusione l'impianto cocleare è una soluzione praticabile ed efficace in caso di insorgenza di ipoacusia ritardata dopo chirurgia conservativa del neurinoma dell'acustico.
Introduction
Hearing preservation after surgical removal of vestibular schwannoma (VS) has become one of the greatest concerns in this field with many reports advocating very high rates of useful postoperative hearing with both middle cranial fossa (MCF) and retrosigmoid approaches. Recent reviews report that MCF is the best option for hearing conservation with tumours less than 1.5 cm in diameter, while the retrosigmoid corridor would be the best choice for larger tumours 1. The chance of hearing preservation decreases as tumour size increases and this is one of the reasons for offering early surgery according to several groups. Despite all efforts, hearing deterioration after VS surgery still remains an unsolved issue, which can lead to unserviceable hearing 2-4. Even if hearing is well preserved it is not clear if it can deteriorate more quickly in the years following surgery. From this point of view, there is a lack of studies investigating what happens to postoperative residual hearing and what solutions can be effectively used in case of delayed deterioration.
Case report
We present a 50-year-old male who had undergone surgery for right VS three years before, coming for consultation for sudden sensorineural hearing loss at the same side of the operation. VS removal was carried out by a retrosigmoid approach without any particular complication as stated in the operative report. The VS was intracanalicular (stage I according to Koos' classification) and 9 × 6 × 4 mm in size. There were no facial or cochlear nerve damage as shown by postoperative audiogram (Table I).
Table I.
Hearing threshold after vestibular schwannoma (VS) excision and at first consultation.
| Side | 125 Hz | 250 Hz | 0.5 kHz |
1 kHz |
2 kHz |
3 kHz |
4 kHz |
|
|---|---|---|---|---|---|---|---|---|
| After VS | L | 10 | 10 | 10 | 15 | 25 | 75 | 65 |
| surgery | R | 20 | 20 | 20 | 25 | 35 | 70 | 90 |
| At | L | 10 | 10 | 10 | 15 | 25 | 75 | 65 |
| consultation | R | / | 95 | 100 | 105 | 95 | 105 | / |
After three years of good hearing, he experienced sudden hearing loss, which we ascertained through pure tone audiometry (Table II).
Table II.
Speech perception in noise.
| Noise (63 dB) | S/N | Rate pre-op | Rate post-op CI on |
|---|---|---|---|
| Right | +7 dB | 38% | 100% |
| Left | +7 dB | 74% | 80% |
We immediately started intravenous therapy with steroids at a conventional suggested dose and hyperbaric oxygen therapy, without any hearing threshold improvement. The patient also developed severe tinnitus (THI: grade 4).
After thorough evaluation including HRCT scan and MRI showing the presence of the cochlear nerve on that side, without any recurrence of VS and a patent cochlea, we decided to offer cochlear implantation as a solution for his hearing loss and tinnitus.
A Cochlear Nucleus Freedom Contour Advance (Cochlear, Australia) was implanted and activated after 1 month.
The cochlear implant restored normal hearing threshold in the deaf ear. The patient improved his localisation skills as reported in Figure 1, which shows azimuth error in degrees in an identification task of the source of target signals randomly delivered through one out of 15 speakers panned from -60° to +60°. His hearing in noise, tested with disyllabic words at 70 dB with S/N + 7 dB, also improved from 38 to 100% of correct answers, when target signals were presented to the implanted ear, and from 74 to 80% when target signals were presented to the contralateral side.
Fig. 1.

Azimuth error (°) in localisation test before and after cochlear implantation. Positive values refer to sounds coming from the right and vice-versa. Triangles are median values.
The speech, spatial and qualities of hearing scale also confirmed this data with improvement of spatial and speech items (Fig. 2).
Fig. 2.
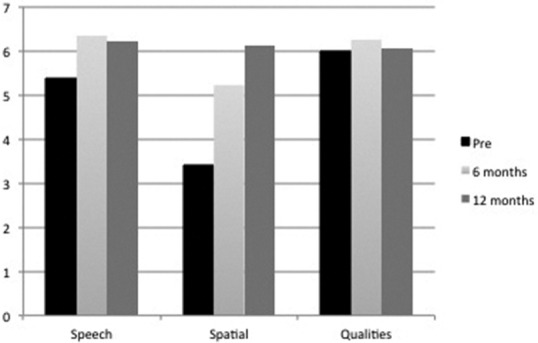
Results of the "Speech, Spatial and Qualities of hearing" questionnaire over time.
Also his tinnitus dropped from THI grade 4 to 2 with CI on. Tinnitus evolution over time is plotted in Figure 3.
Fig. 3.
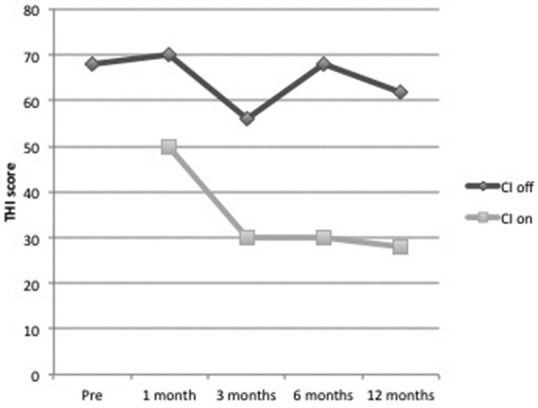
Tinnitus handicap inventory (THI) score over time.
Conclusions
This case shows several interesting aspects dealing with hotly debated topics: hearing preservation and restoration after VS surgery. This case is of particular interest because there are no reports in the literature about hearing restoration with cochlear implant in delayed sudden hearing loss after prior conservative VS surgery.
Hearing preservation in VS surgery is one of the key elements for subsequent hearing restoration 2. In fact, a cochlear implant can be a valid therapeutic option only if cochlear nerve function is preserved in the first place. There are several reports, which show how cochlear implantation can be an effective solution for hearing restoration in patients with VS either as hearing loss treatment without removing the tumour 3 or after VS resection, although they deal with severe bilateral hearing loss patients affected by neurofibromatosis 2 or by sporadic VS in the only hearing ear 4 5. The presented case was treated as a single-sided deafness in order to relieve the patient's severe tinnitus and to restore binaural hearing. VS surgery does not seem to affect the results of cochlear implantation, which are comparable to "normal" single-sided deafness implanted patients 6-8. We cannot understand the aetiology of the subsequent hearing loss, which might be a delayed consequence of the VS surgery itself or not. Whatever the aetiology, it did not affect the retrocochlear auditory pathway.
In conclusion, this case shows that in case of conservative VS removal, should a delayed hearing loss occur, it can be managed with cochlear implantation with good, stable and satisfactory results.
References
- 1.Ansari SF, Terry C, Cohen-Gadol AA. Surgery for vestibular schwannomas: a systematic review of complications by approach. Neurosurg Focus. 2012;33:E14–E14. doi: 10.3171/2012.6.FOCUS12163. [DOI] [PubMed] [Google Scholar]
- 2.Pai I, Dhar V, Kelleher C, et al. Cochlear implantation in patients with vestibular schwannoma: a single United Kingdom center experience. Laryngoscope. 2013;123:2019–2023. doi: 10.1002/lary.24056. [DOI] [PubMed] [Google Scholar]
- 3.Mukherjee P1, Ramsden JD, Donnelly N, et al. Cochlear implants to treat deafness caused by vestibular schwannomas. Otol Neurotol. 2013;34:1291–1298. doi: 10.1097/MAO.0b013e31829763a7. [DOI] [PubMed] [Google Scholar]
- 4.Amoodi HA, Makki FM, Cavanagh J, et al. Cochlear implant rehabilitation for patients with vestibular schwannoma: report of two cases. Cochlear Implants Int. 2012;13:124–127. doi: 10.1179/1754762810Y.0000000003. [DOI] [PubMed] [Google Scholar]
- 5.Ahsan S, Telischi F, Hodges A, et al. Cochlear implantation concurrent with translabyrinthine acoustic neuroma resection. Laryngoscope. 2003;113:472–474. doi: 10.1097/00005537-200303000-00015. [DOI] [PubMed] [Google Scholar]
- 6.Baguley DM, Atlas MD. Cochlear implants and tinnitus. Prog Brain Res. 2007;166:347–355. doi: 10.1016/S0079-6123(07)66033-6. [DOI] [PubMed] [Google Scholar]
- 7.Baguley. DM. Cochlear implants in single-sided deafness and tinnitus. Seminars in Hearing. 2010;31:410–413. [Google Scholar]
- 8.Punte AK, Vermeire K, Hofkens A, et al. Cochlear implantation as a durable tinnitus treatment in single-sided deafness. Cochlear Implants Int. 2011;12(Suppl 1):26–29. doi: 10.1179/146701011X13001035752336. [DOI] [PubMed] [Google Scholar]