

Abstract
Background
Long non-coding RNAs (lncRNAs) have been confirmed to play an important role in the development and progression of diseases. Ankylosing spondylitis (AS) is a chronic inflammatory systemic disease and it is hard to be found in early time. The purpose of this study was to investigate the role of lncRNA-AK001085 in the diagnosis of AS.
Material/Methods
The expression of lncRNA-AK001085 was detected by quantitative real-time polymerase chain reaction (qRT-PCR) analysis. The relationship between its expression and clinicopathologic characteristics was also analyzed. Meanwhile the correlation between lncRNA-AK001085 expression and diseases activity indexes was estimated. In addition, the value of it in the diagnosis of AS was explored through establishing receiver operating characteristic (ROC) curve.
Results
Serum lncRNA-AK001085 expression was decreased in patients with AS compared with healthy individuals. And its expression was proved to be influenced by ever cigarette smoker, exercise level and occupational activity level. Besides, the correlation of the expression of lncRNA-AK001085 and disease activity indexes (BASDI, ASDAS, ESR, CRP) were all negative, which suggested that the lncRNA-AK001085 was significantly lower in patients with a high disease activity score. It might showed that the expression of lncRNA-AK001085 affected the activity of AS.
Conclusions
LncRNA-AK001085 was down-regulated in AS patients and it could be an independent diagnostic indicator.
MeSH Keywords: Diagnosis; Spondylitis; Spondylitis, Ankylosing
Background
Ankylosing spondylitis (AS) is a chronic inflammatory systemic disease that seriously influences human skeletal system [1]. It mainly affects the sacroiliac joints and the vertebral column, leading to syndesmophyte formation and impaired back mobility [2,3]. AS is usually seen in young adults and may causes significant disability [4]. Pain arising from an inflamed sacroiliac joint and HLA-B27 positive are typical in AS [5,6], but they can’t be independent markers for the diagnosis and prognosis of AS. Therefore, the finding of diagnostic and prognostic markers for AS is meaningful for the therapy.
LncRNAs are a kind of jumped-up non-coding RNA with a length of longer than 200 nucleotides without function of being translated into a protein which is significantly different from miRNAs and siRNAs [7]. Since the first lncRNAs (H19 and X-inactive specific transcript) were discovered with traditional gene mapping approaches, more and more lncRNAs had been found to take effect on diverse biological processes including brain development, embryonic development, histological differentiation and organogenesis, cell proliferation and metastasis cell growth, and differentiation etc [8–12]. Accumulated studies have confirmed that lncRNAs play an important role in the development of diseases and can serve as a potential carcinogenic or anti-carcinogenic RNA as its role in cell transformation [13]. However, the role of lncRNAs was rarely reported in AS.
In our study, we selected lncRNA-AK001085 as our object. To investigate the function of lncRNA-AK001085, we detected the expression of lncRNA-AK001085 in patients with AS and healthy people via qRT-PCR analysis. The value of lncRNA-AK001085 in the diagnosis of AS was evaluated by establishing ROC curve. In addition, the correlation between disease activity indexes and the expression of lncRNA-AK001085 was analyzed via Pearson test.
Material and Methods
Patients data
The study was approved by the council of ethics of The General Hospital of Chinese PLA. Written informed consent was signed by each participant in advance.
117 patients who were diagnosed as AS in The General Hospital of Chinese PLA during 2011–2014 were collected. In addition, 76 healthy people were taken as healthy controls. All patients hadn’t received any form of treatment and were accord with the modified New York criteria of 1984 [14]. Individuals with autoimmune, inflammatory, severe liver and kidney disease, cardiovascular disease, hematological diseases and malignancy were all needed to be excluded from our study. The patients with AS were ranked according to ankylosing spondylitis disease activity score (ASDAS) established by the International Association of Ankylosing Spondylitis (ASAS) [15].
Sampling
Serum of patients including 117 patients with AS as well as 76 healthy individuals were collected and put into blood collection tube of EDTA immediately, respectively. Then the serum samples were stored at −80°C for RNA extraction. The clinical factors such as age, gender, hip osteoarthritis, pain degree, hip joint function, kidney heart and pulmonary amyloidosis, immune globulin, erythrocyte sedimentation rate and fingers/toes inflammation were recorded in database.
RNA extraction and qRT-PCR
TRIzol®reagent (Invitrogen Life Technologies, Carlsbad, CA, USA) was used to isolated the total RNA from the serum of patients with AS and healthy controls. Reverse transcriphase synthesized the first chain of cDNA with SuperScript™ III (Invitrogen Life Technologies). Then RT-PCR reaction was performed in the Applied Biosystems 7900 Fast Real-Time PCR system (Applied Biosystems, Foster City, California, USA) with a internal control of β-actin. Comparative cycle threshold (CT) method was utilized for calculating the relative expression of lncRNA-AK001085.
Statistical analysis
SPSS version 13.0 for Windows (SPSS Inc, IL, USA) was utilized for data statistics. The difference between two groups was analyzed by students’ t test. The relationship between clinical factors and the expression of lncRNA-AK001085 was analyzed by chi-square test. The diagnostic value of lncRNA-AK001085 was estimated through ROC curve analysis. The correlation analysis between BASDI, ASDAS, inflammatory markers and the expression of lncRNA-AK001085 in the serum of patients with AS were conducted using Pearson correlation test. The difference was considered to be significant difference when P<0.05.
Results
The expression of lncRNA-AK001085 in AS patients and healthy controls
To investigate the expression level of lncRNA-AK001085 in patients with AS and healthy controls, qRT-PCR analysis was performed. The result demonstrated that lncRNA-AK001085 was obviously lower in patients with AS than that in healthy controls (Figure 1, P<0.05).
Figure 1.
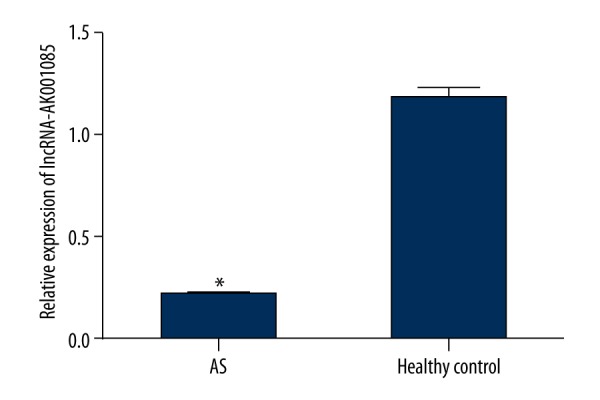
The expression of lncRNA-AK001085 in patients with AS and healthy controls. LncRNA-AK001085 expression was significantly decreased in AS patients compared to in healthy controls (P<0.05).
The relationship between lncRNA-AK001085 expression and clinicopathologic characteristics of patients with AS
To explore whether lncRNA-AK001085 was involved in the development of AS, we analyzed its relationship with clinicopathologic characteristics of patients. As shown in Table 1, ever cigarette smoker (P=0.000), exercise level (P=0.002) and occupational activity level (P=0.000) were proved to be related to the expression of lncRNA-AK001085 obviously. Meanwhile, there was no distinctively correlation between lncRNA- AK001085 expression and age, gender, hip osteoarthritis, iritis, and area first symptomatic.
Table 1.
The relationship between clinicopathological characteristics of patients with AS and lncRNA-AK001085 expression.
| Clinicopathological characteristics | n | lncRNA-AK001085 expression | P | |
|---|---|---|---|---|
| High | Low | |||
| Age | 0.357 | |||
| 10–20 | 25 | 16 | 9 | |
| 21–30 | 53 | 25 | 28 | |
| 31–40 | 39 | 18 | 21 | |
| Gender | 0.401 | |||
| Male | 91 | 47 | 44 | |
| Female | 26 | 12 | 14 | |
| Hip osteoarthritis | 0.408 | |||
| Absent | 65 | 31 | 34 | |
| Present | 52 | 28 | 24 | |
| Iritis | 0.164 | |||
| Absent | 68 | 31 | 37 | |
| Present | 49 | 28 | 21 | |
| Ever cigarette smoker | 0.000 | |||
| No | 77 | 50 | 27 | |
| Yes | 40 | 9 | 31 | |
| Area first symptomatic | 0.118 | |||
| Low back | 65 | 38 | 27 | |
| Hip/groin | 27 | 9 | 18 | |
| Knee/ankle | 25 | 12 | 13 | |
| Exercise level | 0.002 | |||
| None | 11 | 2 | 9 | |
| <2 h/week | 38 | 13 | 25 | |
| 2–4 h/week | 39 | 22 | 17 | |
| 5–9 h/week | 25 | 20 | 5 | |
| >10 h/week | 4 | 2 | 2 | |
| Occupational activity level | 0.000 | |||
| Active | 24 | 22 | 2 | |
| Sedentary | 44 | 17 | 27 | |
| Manua | 49 | 19 | 30 | |
The diagnostic value of lncRNA-AK001085 in AS
ROC curve was established to estimate the diagnostic value of lncRNA-AK001085 in AS. As shown in Figure 2, a curve with a AUC of 0.868 corresponding with a sensitivity of 62.9% and a specificity of 93.6% was obtained and the ideal cutoff value was 0.186.This indicated that lncRNA-AK001085 could be an independent diagnostic marker in AS.
Figure 2.
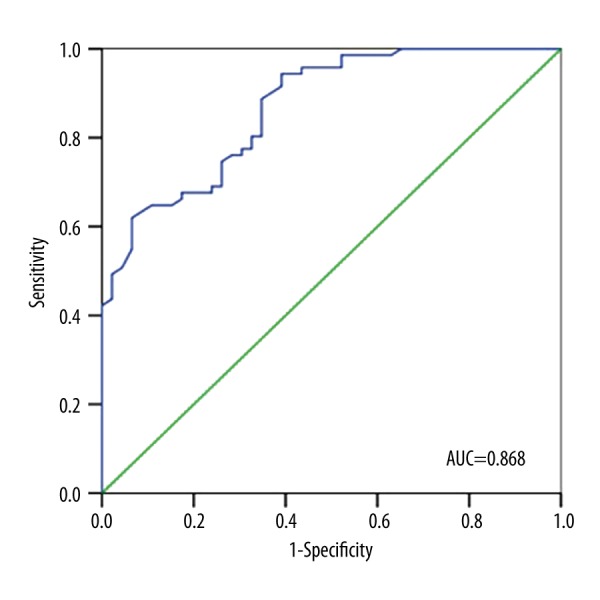
ROC curve for analyzing the diagnostic value of lncRNA-AK001085 in patients with AS.
Correlation between BASDI, ASDAS, inflammatory markers and the expression of lncRNA-AK001085 in the serum of patients with AS
The correlation between BASDI, ASDAS, inflammatory markers and the expression of lncRNA-AK001085 in the serum of patients with AS was analyzed. BASDI was accepted by most experts and used widely until ASDAS was provided at 2008 by ASAS. In our study, we used both two indexes. It indicated that the expression of lncRNA-AK001085 had a negative correlation with BASDI, ASDAS, ESR and CRP. However, the BASDI, ASDAS and ESR, CRP presented a positive correlation (Table 2).
Table 2.
The correlation between the expression of lncRNA-AK001085 and BASDI, ASDAS, ESR, CRP(r value).
| Cases | ESR | CRP | lncRNA-AK001085 | |
|---|---|---|---|---|
| BASDI | 117 | 0.872** | 0.825** | −0.470** |
| ASDAS1 | 117 | 0.907** | 0.874** | −0.467** |
| ASDAS2 | 117 | 0.917** | 0.850** | −0.460** |
| ASDAS3 | 117 | 0.886** | 0.877** | −0.452** |
| ASDAS4 | 117 | 0.903** | 0.872** | −0.490*** |
| ESR | 117 | – | 0.862** | −0.447** |
| CRP | 117 | 0.862** | – | −0.354** |
P<0.05;
P<0.01;
P<0.0001.
Discussion
In present study, lncRNA-AK001085 was considered to be down-regulated in AS. So we speculated that lncRNA-AK001085 might be a suppressor for AS. And the detailed roles it played and the mechanism still need further to be studied.
To investigate whether lncRNA-AK001085 was involved in the development of AS, we analyzed the relationship between its expression and clinicopathologic characteristics. According to chi-square test, ever cigarette smoker, exercise level and occupational activity level were considered to be vital influence factors for the expression of lncRNA-AK001085. This result might suggest that lncRNA-AK001085 participated in the progression of AS, but the detailed functions were still unclear.
The state of illness in advance time is irreversible and has no specificity treatments. The diagnose and treat in early time is the key for curing AS. Advanced magnetic resonance imaging (MRI) techniques, such as diffusion weighted imaging (DWI) and whole-body MRI (WB-MRI), have been utilized in the evaluation of patients with suspected early AS [16–18]. Other than these methods, there is no direct test to diagnose AS [19]. Nevertheless, the diagnosis time is often late that from symptom onset to diagnosis ranging from 5 to 8 years [20]. In patients with AS, the proper and accurate markers are still absent. HLA-B27-positive rate reached to 70% in patients with AS, but HLA-B27 was not considered to be a diagnostic marker of AS [21]. The rising of inflammatory markers including CRP and ESR are also helpful for the early diagnosis of AS. However, there was still no a gold standard of diagnostic. So diagnostic markers are important for this disease. In current study, we verified that lncRNA-AK001085 could be an independent marker in the diagnosis of AS via the establishment of ROC curve which has a high AUC of 0.868 combining with a sensitivity of 62.9% and a specificity of 93.6%. And lncRNA-AK001085 may be meaningful for the diagnosis of AS in future.
The disease activity reflects the inflammatory and its level. The evaluation of it is complicated and contain many aspects [22].The common indexes in clinical are relative systematic index (BASDI [23], ASDAS, etc.), single indicator (e.g., ESR, CRP [24] and so on) and radiological imaging indexes. AS disease activity index (BASDI) was the original standard for the evaluation of this disease. However, it can not reflect the disease activity on the whole as it is only the subjective evaluation from patients. Ankylosing spondylitis disease activity score (ASDAS) was provided and confirmed by the Assessment Of SpondyloArthritis international Society and Van der et al. [15,25]. In our study, we analyzed the correlation not only BASDI, ASDAS but also inflammatory markers ESR, CRP and the expression of lncRNA-AK001085. The results demonstrated that the expression of lncRNA-AK001085 had a negative correlation with BASDI, ASDAS, ESR and CRP. However, the BASDI, ASDAS and ESR, CRP presented a positive correlation. These data suggested that the lncRNA-AK001085 was significantly lower in patients with a high disease activity score.
Conclusions
In conclusion, lncRNA-AK001085 is decreased in patients with AS compared with healthy controls. The ROC curve revealed that lncRNA-AK001085 may be an independent marker in the diagnosis of AS. The disease activity is influenced by the expression of lncRNA-AK001085, too. However, as the number of the samples are limited and other unfavorable factors, some further studies are still need to be done in future.
Footnotes
Source of support: Miaopu foundation of PLAGH (15KMZ01)
References
- 1.Braun J, Sieper J. Ankylosing spondylitis. Lancet. 2007;369(9570):1379–90. doi: 10.1016/S0140-6736(07)60635-7. [DOI] [PubMed] [Google Scholar]
- 2.Atouf O, Benbouazza K, Brick C, et al. Distribution of HLA class I and II genes in ankylosing spondylitis patients from Morocco. Pathol Biol (Paris) 2012;60(6):e80–83. doi: 10.1016/j.patbio.2012.01.001. [DOI] [PubMed] [Google Scholar]
- 3.Gilgil E, Kaçar C, Tuncer T, Bütün B. The association of syndesmophytes with vertebral bone mineral density in patients with ankylosing spondylitis. J Rheumatol. 2005;32(2):292–94. [PubMed] [Google Scholar]
- 4.Robinson PC, Brown MA. Genetics of ankylosing spondylitis. Mol Immunol. 2014;57(1):2–11. doi: 10.1016/j.molimm.2013.06.013. [DOI] [PubMed] [Google Scholar]
- 5.Rudwaleit M, Metter A, Listing J, et al. Inflammatory back pain in ankylosing spondylitis: A reassessment of the clinical history for application as classification and diagnostic criteria. Arthritis Rheum. 2006;54(2):569–78. doi: 10.1002/art.21619. [DOI] [PubMed] [Google Scholar]
- 6.Liu F, Wang F, Wang CC, et al. Expression of IL-2 and IL-11 and its significance in patients with ankylosing spondylitis. Asian Pac J Trop Med. 2013;6(1):76–78. doi: 10.1016/S1995-7645(12)60205-3. [DOI] [PubMed] [Google Scholar]
- 7.Bu D, Yu K, Sun S, et al. NONCODE v3.0: integrative annotation of long noncoding RNAs. Nucleic Acids Res. 2012;40(Database issue):D210–15. doi: 10.1093/nar/gkr1175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pollard KS, Salama SR, Lambert N, et al. An RNA gene expressed during cortical development evolved rapidly in humans. Nature. 2006;443(7108):167–72. doi: 10.1038/nature05113. [DOI] [PubMed] [Google Scholar]
- 9.Beniaminov A, Westhof E, Krol A. Distinctive structures between chimpanzee and human in a brain noncoding RNA. RNA. 2008;14(7):1270–75. doi: 10.1261/rna.1054608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mercer TR, Dinger ME, Mattick JS. Long non-coding RNAs: insights into functions. Nat Rev Genet. 2009;10(3):155–59. doi: 10.1038/nrg2521. [DOI] [PubMed] [Google Scholar]
- 11.Prensner JR, Iyer MK, Sahu A, et al. The long noncoding RNA SChLAP1 promotes aggressive prostate cancer and antagonizes the SWI/SNF complex. Nat Genet. 2013;45(11):1392–98. doi: 10.1038/ng.2771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gupta RA, Shah N, Wang KC, et al. Long non-coding RNA HOTAIR reprograms chromatin state to promote cancer metastasis. Nature. 2010;464(7291):1071–76. doi: 10.1038/nature08975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Huarte M, Rinn JL. Large non-coding RNAs: Missing links in cancer? Hum Mol Genet. 2010;19(R2):R152–61. doi: 10.1093/hmg/ddq353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984;27(4):361–68. doi: 10.1002/art.1780270401. [DOI] [PubMed] [Google Scholar]
- 15.Lukas C, Landewé R, Sieper J, et al. Development of an ASAS-endorsed disease activity score (ASDAS) in patients with ankylosing spondylitis. Ann Rheum Dis. 2009;68(1):18–24. doi: 10.1136/ard.2008.094870. [DOI] [PubMed] [Google Scholar]
- 16.Goh L, Suresh P, Gafoor A, et al. Disease activity in longstanding ankylosing spondylitis: A correlation of clinical and magnetic resonance imaging findings. Clin Rheumatol. 2008;27(4):449–55. doi: 10.1007/s10067-007-0726-7. [DOI] [PubMed] [Google Scholar]
- 17.Gaspersic N, Sersa I, Jevtic V, et al. Monitoring ankylosing spondylitis therapy by dynamic contrast-enhanced and diffusion-weighted magnetic resonance imaging. Skeletal Radiol. 2008;37(2):123–31. doi: 10.1007/s00256-007-0407-2. [DOI] [PubMed] [Google Scholar]
- 18.Zochling J, Baraliakos X, Hermann KG, Braun J. Magnetic resonance imaging in ankylosing spondylitis. Curr Opin Rheumatol. 2007;19(4):346–52. doi: 10.1097/BOR.0b013e32816a938c. [DOI] [PubMed] [Google Scholar]
- 19.Reveille JD. Biomarkers for diagnosis, monitoring of progression, and treatment responses in ankylosing spondylitis and axial spondyloarthritis. Clin Rheumatol. 2015;34(6):1009–18. doi: 10.1007/s10067-015-2949-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Guillemin F, Briançon S, Pourel J, Gaucher A. Long-term disability and prolonged sick leaves as outcome measurements in ankylosing spondylitis. Possible predictive factors. Arthritis Rheum. 1990;33(7):1001–6. doi: 10.1002/art.1780330712. [DOI] [PubMed] [Google Scholar]
- 21.Rudwaleit M, Haibel H, Baraliakos X, et al. The early disease stage in axial spondylarthritis: Results from the German Spondyloarthritis Inception Cohort. Arthritis Rheum. 2009;60(3):717–27. doi: 10.1002/art.24483. [DOI] [PubMed] [Google Scholar]
- 22.Bakker C, Boers M, van der Linden S. Measures to assess ankylosing spondylitis: Taxonomy, review and recommendations. J Rheumatol. 1993;20(10):1724–30. [PubMed] [Google Scholar]
- 23.Garrett S, Jenkinson T, Kennedy LG, et al. A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol. 1994;21(12):2286–91. [PubMed] [Google Scholar]
- 24.Creemers MC, Franssen MJ, van de Putte LB, et al. Methotrexate in severe ankylosing spondylitis: An open study. J Rheumatol. 1995;22(6):1104–7. [PubMed] [Google Scholar]
- 25.van der Heijde D, Lie E, Kvien TK, Sieper J, et al. ASDAS, a highly discriminatory ASAS-endorsed disease activity score in patients with ankylosing spondylitis. Ann Rheum Dis. 2009;68(12):1811–18. doi: 10.1136/ard.2008.100826. [DOI] [PubMed] [Google Scholar]