

Abstract
Introduction:
Noise is one of the most extensive environmental factors affecting the general population. The present study is focused on the association between discomfort caused by noise and the incidence of certain diseases (ischaemic heart disease, stroke and hypertension).
Materials and Methods:
This cross-sectional questionnaire study, conducted in 10 cities in the Czech Republic, comprises two stages with 3592 obtained questionnaires in the first phase and 762 in the second phase. Twelve variables describe subjective responses to noise from different sources at different times of day. The intensity of the associations between variables was measured by correlation coefficient. Logistic regression was used for fitting models of morbidity, and confounders such as age and socio-economic status were included. The hypotheses from the first phase were independently validated using data from the second phase.
Results:
The general rates of noise annoyance/sleep disturbance had greater correlation with traffic noise variables than with neighbourhood noise variables. Factors significantly associated with diseases are: for hypertension − annoyance by traffic noise (the elderly, odds ratio (OR) 1.4) and sleep disturbance by traffic and neighbourhood noise (the elderly, OR 1.6); for ischaemic heart disease − the general rate of noise annoyance (all respondents, OR 1.5 and the adults 30–60 years, OR 1.8) and the general rate of annoyance and sleep disturbance (all respondents, OR 1.3); for stroke − annoyance and sleep disturbance by traffic and neighbourhood noise (all respondents, OR 1.8).
Conclusion:
Factors that include multiple sources of noise or non-specific noise are associated with the studied diseases more frequently than the source-specific factors.
Keywords: Annoyance, community noise, morbidity, sleep disturbance, subjective responses
Introduction
Environmental noise together with its impact on public health has been an important issue for many years. Substantial evidence has been accumulated on the negative physiological and psychological effects of environmental noise. Sufficiently evidenced effects on health and well-being are annoyance, sleep disturbance (polysomnographic or self-reported), learning and memory hindrance, changes in levels of stress hormones, deterioration of reported health, hypertension and ischaemic heart disease.[1] It is estimated that in the European Union member states and other western European countries, at least one million healthy life years are lost annually as a result of traffic-related noise. Sleep disturbance and annoyance, mostly related to road traffic noise, comprise the main burden of environmental noise.[2] The biological plausibility of the association between noise and cardiovascular diseases is supported by Babisch.[3]
The impact of noise on human health has been studied in a number of ways. The first is direct association between environmental noise levels and morbidity of various, mainly cardiovascular, diseases.[4,5,6,7] The impact of environmental noise is considered to be sufficiently demonstrated for ischaemic heart disease and hypertension.[1] The relationship between environmental noise and annoyance and sleep disturbance is the subject of a number of studies[8,9,10,11] and is likewise considered to be sufficiently demonstrated.[1,12] Other types of studies deal with the relationships between subjective responses to noise and morbidity of various diseases. Self-reported noise annoyance and sleep disturbance are commonly used markers of subjective response to noise. Although annoyance is not considered a direct health effect,[1] it may play a mediating role in the causal chain between noise and health. This indirect pathway of activation of the organism represents cognitive perception of sound, its cortical activation and related emotional responses. This can, like noise itself, initiate physiological stress reactions affecting the hypothalamus, limbic system, autonomous nervous system and pituitary and adrenal glands. The ensuing physiological dysfunction may result in manifest physiological changes and health effects over long-term periods of chronic noise exposure.[3] Noise annoyance acts as an effective modifier of the relationship between noise levels and hypertension.[13] In some cases, noise annoyance can also act as independent exposure variable.[12]
Babisch[4] summarized the results of the studies focused on the relationships between traffic noise annoyance or sleep disturbance and hypertension or ischaemic heart disease. These results are regarded as consistent when subjective responses of disturbance and annoyance are considered, showing relative risks ranging from 0.8 to 2.7 in highly annoyed/disturbed subjects. However, the author surmises that these findings may be of lower validity due to methodological issues. The Large Analysis and Review of European housing and health Status (LARES) study[14,15,16] coordinated by World Health Organization (WHO) has revealed significantly elevated relative risks in the cardiovascular, respiratory and musculoskeletal systems as well as increased risk of depressive disorder in adults reporting strong annoyance. Analogous problems are evident in the case of sleep disturbance. LARES also studied the effects of neighbourhood noise which had been considerably underestimated up to that point. It was found that the health effects of neighbourhood noise annoyance are approximately in the similar range as the health effects of traffic noise annoyance.[14]
Whereas the majority of the quoted studies dealt with the health effects of noise separately, Ohrström and Barregård[17] focused on the impact of exposure to single and combined noise sources. They found that combined exposure to noise from two sources, road and railway traffic, induced more extensive annoyance reactions than noise from particular sources at the same sound levels.
Most studies typically deal separately with different sources of noise. They are usually split into two parts devoted to the effects of noise during 24 h or in night. Our approach to the studied problem is more complex. We focused on subjective responses to noise from various sources (traffic and neighbourhood noise and non-specific noise with no given source) at various times (at day, at night and over 24-h periods) and their combination. We ascertained the mutual relationships between these subjective responses to noise. Furthermore, our aim was to study in detail the relationships between particular and combined subjective responses to noise on one hand, and the occurrence of diseases whose risk is known to be increasing with increasing noise levels on the other. We were trying to answer the following questions:
-
(1)
“What are the relationships between individual variables expressing subjective responses to noise, and which of the particular subjective responses most contribute to an overall feeling of discontent?”
-
(2)
“Which indicator better explains probability of disease: (subjectively perceived) traffic noise, neighbourhood noise, combined exposure or the total rate of noise (irrespective of the source)?”
Materials and Methods
Study areas and subjects
The study was conducted as a part of the Environmental Health Monitoring system in the Czech Republic[18] at the National Institute of Public Health in Prague. Part of this system includes noise monitoring in selected cities in the Czech Republic. The cities involved are of varying sizes with populations ranging from 14,000 to 1.3 million inhabitants. In each of the cities, two localities with different noise levels were chosen. The localities have an area of approximately 0.5 km2 and comprise various types of building, mostly street houses and apartment blocks. All localities are situated in built-up urban areas; none of them are urban satellites. Noise levels in these localities were subject to long-term monitoring. An overall evaluation of noise levels in all monitored localities did not reveal significantly increasing or decreasing trends.[19] Questionnaire surveys were repeatedly done in all monitored localities.
Data for this study were collected during two phases of a questionnaire survey which was undertaken in 2007 and 2013. The involved cities are shown in Figure 1. During the first phase (2007) 14 localities and in the second phase (2013) another six localities were investigated, taking two localities from the same city.
Figure 1.
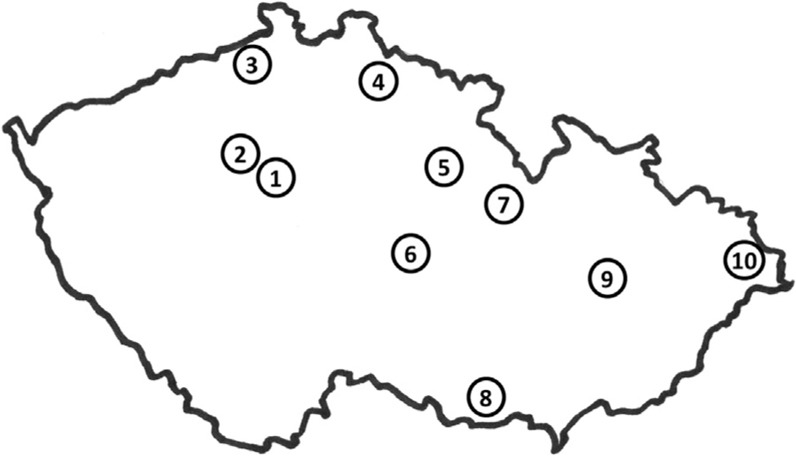
Map of cities included in the study. (1) Praha (Prague), (2) Kladno, (3) Ústí nad Labem, (4) Jablonec nad Nisou, (5) Hradec Králové, (6) Havlíčkův Brod, (7) Ústí nad Orlicí, (8) Znojmo, (9) Olomouc, (10) Ostrava
Localities and its characterisation are shown in Table 1. The main source of noise in localities is road traffic. In some localities, there are trams or railways too, and in quiet localities, the effect of neighbourhood noise is apparent. The day noise level range between 47 and 72 dB and the night noise level range between 39 and 66 dB. All persons aged 30–80 living in the included localities were requested to complete the questionnaire. A total of 6777 inhabitants in the first phase and 2116 inhabitants in the second phase were addressed.
Table 1.
Characterisation of localities included in questionnaire surveys
| Name of locality | Main types of building | Main sources of noise | Sound pressure levels | Year of survey | Response rate [%] | Number of respondents | ||
|---|---|---|---|---|---|---|---|---|
| Lday [dB] | Lnight [dB] | Adults ≤ 60 | Elderly | |||||
| Havlí kův Brod 1 | Blocks | road t., neighb. | 54 | 47 | 2007 | 38 | 136 | 40 |
| Havlí kův Brod 2 | Blocks | road t. | 69 | 63 | 2007 | 63 | 142 | 167 |
| Hradec Králové 1 | Street | road t., neighb. | 56 | 45 | 2007 | 32 | 83 | 64 |
| Hradec Králové 2 | Blocks | road t. | 72 | 65 | 2007 | 40 | 129 | 64 |
| Jablonec n.N. 1 | Blocks | neighb., road t. | 47 | 39 | 2013 | 39 | 54 | 45 |
| Jablonec n.N. 2 | Blocks | road t. | 58 | 50 | 2013 | 28 | 43 | 63 |
| Kladno 1 | Blocks | road t., neighb. | 54 | 48 | 2007 | 50 | 241 | 40 |
| Kladno 2 | Blocks | road t. | 63 | 53 | 2007 | 48 | 194 | 97 |
| Olomouc 1 | Blocks | road t. | 60 | 51 | 2013 | 34 | 30 | 83 |
| Olomouc 2 | Blocks, street | road t. | 66 | 60 | 2013 | 45 | 35 | 78 |
| Ostrava 1 | Street | road t., neighb. | 54 | 43 | 2007 | 62 | 191 | 76 |
| Ostrava 2 | Street | road t., tram | 69 | 62 | 2007 | 77 | 282 | 119 |
| Praha (Prague) 1 | Blocks | road t., neighb. | 52 | 43 | 2013 | 37 | 35 | 107 |
| Praha (Prague) 2 | Street | road t., tram | 71 | 66 | 2007 | 35 | 118 | 45 |
| Ústí n.L. 1 | Blocks | road t., neighb. | 53 | 44 | 2007 | 43 | 164 | 107 |
| Ústí n.L. 2 | Blocks | road t. | 66 | 57 | 2007 | 60 | 81 | 80 |
| Ústí n.O. 1 | Blocks | road t., neighb. | 52 | 45 | 2007 | 60 | 205 | 104 |
| Ústí n.O. 2 | Blocks | road t., rail t. | 61 | 58 | 2013 | 37 | 82 | 28 |
| Znojmo 1 | Street | road t. | 53 | 45 | 2007 | 72 | 197 | 63 |
| Znojmo 2 | Street | road t. | 68 | 58 | 2007 | 69 | 230 | 85 |
Blocks=apartment blocks, mostly built after year 1945, street=street houses mostly built before year 1938, road t.=road traffic, rail t.=railway traffic, neighb.=neighbourhood, adults≤ 60=age 30–60 years, elderly=age 60.1–80 years.
Data from the first phase of the questionnaire survey were used to test as many hypotheses about the relationships as possible. Data from the second phase were used to validate the hypotheses from the first phase. In this way, we obtained independent validation (or falsification) of the significant relationships from the first phase, since the data from 2013 were gathered in different localities than the data from 2007.
The questionnaire
The questionnaire consisted of sections devoted to demographic and socio-economical characteristics of respondents (age, sex, marital status, education and economic status), their health (hypertension, ischaemic heart diseases including heart attack and stroke) and rates of noise annoyance and sleep disturbance. Although the respondents completed the questionnaire independently, they were asked to report only those diagnoses confirmed by a doctor. The section of the questionnaire dealing with subjective response to noise was divided into two parts − one dealing with annoyance during the day and the other dealing with sleep disturbance at night. Respondents rated their total noise annoyance without identification of source of the noise. In a separate question, respondents rated their annoyance caused by six different sources of traffic noise (cars, trucks, motorcycles, buses, air transport, rail transport) and four different sources of neighbourhood noise (noise created by neighbours, technical equipment in the house, noise from restaurants and cultural facilities and commercial supplying). Every item was rated on 6-point scale with responses ranging from strongly to not at all. The same scheme was followed for noise-related sleep disturbance.
Data processing and statistical analysis
Rates of noise annoyance as well as sleep disturbance were summed up separately to differentiate the effects of noise from various sources at various times of day. For each of the following three categories − noise annoyance during day, noise sleep disturbance during night and feelings of discomfort (noise annoyance and sleep disturbance) during both day and night − four variables were defined according to the source of disturbing noise: traffic noise only, neighbourhood noise only, simultaneous traffic and neighbourhood noise and all sources of noise. Newly created variables are presented in Table 2. The first three groups of variables (traffic noise, neighbourhood noise, simultaneous traffic and neighbourhood noise) were based on source-specific items in the questionnaire. The last group of variables (all sources of noise) was based on separate questions pertaining to total rate of noise annoyance and sleep disturbance, respectively.
Table 2.
Scheme of variables describing subjective responses to noise according to day/night period and noise sources
| Traffic only | Neighbourhood only | Traffic and neighbourhood | All sources | |
|---|---|---|---|---|
| Day only | A t. | A n. | A (t. + n.) | A g. |
| Night only | SD t. | SD n. | SD (t. + n.) | SD g. |
| Day and night | (A + SD) t. | (A + SD) n. | (A + SD) (t. + n.) | (A + SD) g. |
A t.=annoyance by traffic noise, A n.=annoyance by neighbourhood noise, A (t. + n.)=annoyance by traffic and neighbourhood noise, A g.=the general rate of noise annoyance, SD t.=sleep disturbance by traffic noise, SD n. =sleep disturbance by neighbourhood noise, SD (t. + n.)=sleep disturbance by traffic and neighbourhood noise, SD g.=the general rate of sleep disturbance by noise, (A + SD) t.=annoyance and sleep disturbance by traffic noise, (A + SD) n.= annoyance and sleep disturbance by neighbourhood noise, (A + SD) (t. + n.)=annoyance and sleep disturbance by traffic and neighbourhood noise, (A + SD) g.=the general rate of annoyance and sleep disturbance by noise.
For each of the above 12 new variables, three categories were distinguished: 1–not at all, 2–moderately and 3–strongly annoyed/sleep disturbed. For the variables dealing with source-specific noise, the classification into one of the categories was based on the sum of scores from corresponding items in the questionnaire. For traffic noise, there are cars, trucks, motorcycles, buses, air transport and rail transport, and the sum ranges from 6 to 36. For neighbourhood noise, there are sounds created by neighbours, technical equipment in the house, noise from restaurants and cultural facilities and commercial deliveries, and the sum ranges from 4 to 24. Discretization into categories was performed in such a way that approximately 50% of respondents were included in the first category (not at all annoyed/disturbed), 35% were included in the second category (moderately annoyed/disturbed) and 15% of respondents were in the third category (strongly annoyed/disturbed). This distribution was chosen because we considered it to be characteristic for the European urban population on the basis of the results obtained by the WHO LARES study.[14] The same three categories were distinguished also for total noise annoyance/sleep disturbance (here, the original 6-point scale was used for categorization). In all following analyses, we used the 12 variables in the above-described 3-point scale form. All responses were included except missing answers.
Initially, we focused on the relationships between variables describing subjective responses to noise. Combined data from both phases of the study were used for the purposes of this analysis. The strength of the association between any two variables was measured by the correlation coefficient, which form the correlation matrix.
Furthermore, we studied the association between subjective responses to noise and occurrence of disease. Data on the occurrence of diseases were based on questionnaire responses. The significance of the association was tested by means of logistic regression. Occurrence of a particular disease (hypertension, ischaemic heart disease and stroke) was considered to be a dependent variable while one of the 12 variables described in Table 2 was considered as independent variable. As the prevalence of considered diseases was highly correlated with age, all analyses were performed first separately for adults (age ≤60) and elderly people (age > 60.1). When the studied effects were similar for both age groups, the analysis was subsequently performed on a joint data. In this way, the statistical power was increased. Demographic and socio-economic characteristics (age, sex, marital status, education and economic status) were first tested for their significance and eventually excluded (if non-significant) to make the model as simple as possible.
All possible models were in the first instance fitted on the data from 2007. Models with significant association between subjective responses to noise and disease occurrence were considered to be plausible, and the usual 5% significance level was used in this phase. All plausible models were fitted on the data from 2013. The same association was tested again, but now on new (independent) data. In this way, the models from the first phase in which an effect was significant just by chance were falsified, solving the problem of multiple testing. Only the models where significance remained can be considered to be plausible. Since the dataset from 2013 was smaller, the significance level was increased to 15% in the second stage. At the end, all plausible models were re-estimated on joint datasets by 5% significance level, and these models are reported in the “Results” section.
Results
In the first phase, 3592 questionnaires were obtained (53% response rate) whereas in the second stage, 762 questionnaires were obtained (36% response rate). Response rates in individual localities and numbers of respondents are given in Table 1. The basic socio-demographic characteristics of respondents are summarized in Table 3. The settlement of the sites is relatively stable. The average length of living in the locality was 22 years in the first stage and 29 years in the second study stage; less than 5 years, it was in 10% of the whole respondent group.
Table 3.
Basic socio-demographic characteristics of respondents − number of cases (percentages)
| 2007 | 2013 | |||
|---|---|---|---|---|
| Number | Percentage | Number | Percentage | |
| Age | ||||
| Adults ≤ 60 | 2393 | 66.6 | 279 | 36.6 |
| Elderly | 1151 | 32.0 | 404 | 53.0 |
| N. a. | 48 | 1.3 | 79 | 10.4 |
| Sex | ||||
| Women | 2042 | 56.8 | 457 | 60.0 |
| Men | 1547 | 43.1 | 295 | 38.7 |
| N. a. | 3 | 0.1 | 10 | 1.3 |
| Marital status | ||||
| Single | 285 | 7.9 | 51 | 6.7 |
| Married | 2345 | 65.3 | 492 | 64.6 |
| Divorced | 517 | 14.4 | 101 | 13.2 |
| Widow(-er) | 279 | 7.8 | 91 | 11.9 |
| Other or N. a. | 166 | 4.6 | 27 | 3.5 |
| Education | ||||
| Basic | 321 | 8.9 | 47 | 6.2 |
| Lower secondary | 1263 | 35.2 | 209 | 27.4 |
| Upper secondary | 1448 | 40.3 | 331 | 43.4 |
| University | 540 | 15.0 | 169 | 22.2 |
| N. a. | 20 | 0.6 | 6 | 0.8 |
| Economical status | ||||
| Employed | 1724 | 48.0 | 249 | 32.7 |
| Retired | 1076 | 30.0 | 391 | 51.3 |
| Business trader | 290 | 8.1 | 31 | 4.1 |
| Other or N. a. | 502 | 14.0 | 91 | 11.9 |
Adults ≤ 60=age 30–60 years, elderly=age 60.1–80 years, N. a.= not available.
The individual variables expressing subjective responses to noise were correlative. The correlative intensity was defined by correlation coefficients, which form the correlation matrix [Table 4]. Only six variables were included in correlation matrix − annoyance by traffic noise, annoyance by neighbourhood noise, sleep disturbance by traffic noise, sleep disturbance by neighbourhood noise, the general rate of noise annoyance and the general rate of sleep disturbance. The correlation between variables that were partly based on the same questions (e.g. annoyance by transportation noise versus annoyance and sleep disturbance by transportation noise) was high (about 0.8) in all cases and was not included in correlation matrix.
Table 4.
Correlations between variables describing subjective responses to noise-correlation coefficients
| A n. | SD t. | SD n. | A g. | SD g. | |
|---|---|---|---|---|---|
| A t. | 0.282 | 0.739 | 0.250 | 0.689 | 0.547 |
| A n. | 0.295 | 0.718 | 0.200 | 0.207 | |
| SD t. | 0.354 | 0.605 | 0.630 | ||
| SD n. | 0.182 | 0.277 | |||
| A g. | 0.643 |
A t.=annoyance by traffic noise, A n.=annoyance by neighbourhood noise, SD t.=sleep disturbance by traffic noise, SD n. =sleep disturbance by neighbourhood noise, A g.= the general rate of noise annoyance, SD g.=the general rate of sleep disturbance, All correlation coefficients are statistically significant, and P-values are less than 0.001.
High correlation could be found between the two variables dealing with traffic noise (correlation coefficient 0.7) and also between the two variables dealing with neighbourhood noise (correlation coefficient 0.7). The other pairs of source-specific variables showed only moderate association (correlation coefficient 0.2 and 0.3). The general rate of annoyance was correlated with annoyance by traffic noise (correlation coefficient 0.7) and the general rate of sleep disturbance was correlated with sleep disturbance by traffic noise (correlation coefficient 0.6), whereas the variables dealing with neighbourhood noise were not as strongly correlated with the general rates (correlation coefficients under 0.3). Besides correlations given in Table 4, high correlation was also found between annoyance by traffic and neighbourhood noise and the general rate of noise annoyance, as well as between sleep disturbance by traffic and neighbourhood noise and the general rate of sleep disturbance (correlation coefficient 0.6 in both cases).
In the next part of the analysis, we studied the relationship between indicators for subjective responses to noise and diseases. From the three considered diseases, hypertension was the most prevalent (32% of all respondents). Ischaemic heart disease (including heart attack) was reported by 11% of respondents and stroke by 2% of respondents. The number of cases as well as corresponding percentages for adults and elderly people are summarized in Table 5.
Table 5.
Prevalence of diseases − number of cases (percentages)
| Disease | Adults | Elderly | Total |
|---|---|---|---|
| Hypertension | 498 (19.5%) | 794 (54.9%) | 1292 (32.2%) |
| Ischaemic heart disease | 179 (7.2%) | 235 (17.6%) | 414 (10.8%) |
| Stroke | 27 (1.1%) | 67 (5.2%) | 94 (2.5%) |
Data collected in 2007 revealed a significant relationship between a number of subjective responses to noise and occurrence of diseases, and the outcomes are presented in Table 6. For significant associations, the odds ratio (OR) ranged from 1.2 to 1.8 for hypertension, from 1.3 to 1.8 for ischaemic heart disease (including heart attack) and from 1.8 to 3.3 for stroke.
Table 6.
Odds ratios (OR) for significant association (P < 0.05) in the first stage of the questionnaire survey
| Hypertension | Ischaemic heart disease | Stroke | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All | Adults ≤ 60 | Elderly | All | Adults ≤ 60 | Elderly | All | Adults ≤ 60 | Elderly | |
| A t. | 1.61 | 1.51 | 1.81 | X | X | X | 2.31 | X | 2.71 |
| 1.32 | 1.32 | 1.32 | 1.92 | 2.23 | |||||
| 1.53 | 1.43 | 1.73 | |||||||
| A n. | X | X | 1.52 | X | X | X | 2.31 | X | 2.61 |
| 2.13 | |||||||||
| A (t. + n.) | 1.22 | X | 1.32 | 1.43 | X | X | 2.91 | X | 3.21 |
| 1.92 | 2.12 | ||||||||
| 2.33 | 2.43 | ||||||||
| A g. | 1.31 | 1.41,3 | X | 1.31 1.53 | 1.61 | X | X | X | X |
| 1.83 | |||||||||
| 1.22 | |||||||||
| 1.33 | |||||||||
| SD t. | 1.41 | 1.51 | X | 1.51 | 1.71 | X | 2.71 | 2.72 | 2.81 |
| 1.32 | 1.32 | 1.43 | 1.52 | 1.82 | 2.63 | ||||
| 1.33 | 2.23 | ||||||||
| SD n. | X | X | X | X | X | 1.81 | X | X | X |
| 1.73 | |||||||||
| SD (t. + n.) | 1.31,3 | X | 1.61 | X | X | X | X | X | X |
| 1.22 | 1.32 | ||||||||
| SD g. | 1.31 | X | X | 1.51 | X | 1.51 | X | X | X |
| 1.43 | |||||||||
| (A + SD) t. | 1.41 | 1.32 | 1.42 | X | X | X | 2.61 | X | 2.91 |
| 1.32 | 1.82 | 2.43 | |||||||
| 2.23 | |||||||||
| (A + SD) n. | X | X | 1.32 | X | X | X | X | X | X |
| (A + SD) (t + n) | 1.31 | X | 1.42 | X | X | X | 2.81 | 3.31 | 2.71 |
| 1.32 | 1.82 | 2.53 | |||||||
| 2.43 | |||||||||
| (A + SD) g. | 1.31 | 1.31,2 | X | 1.33 | 1.53 | X | X | X | 2.31 |
| 1.32 | 2.02 | ||||||||
| 1.93 | |||||||||
A t.=annoyance by traffic noise, A n.=annoyance by neighbourhood noise, A (t. + n.)=annoyance by traffic and neighbourhood noise, A g.=the general rate of noise annoyance, SD t.=sleep disturbance by traffic noise, SD n. =sleep disturbance by neighbourhood noise, SD (t. + n.)=sleep disturbance by traffic and neighbourhood noise, SD g.=the general rate of sleep disturbance by noise, (A + SD) t.=annoyance and sleep disturbance by traffic noise, (A + SD) n.= annoyance and sleep disturbance by neighbourhood noise, (A + SD) (t. + n.)=annoyance and sleep disturbance by traffic and neighbourhood noise, (A + SD) g.=the general rate of annoyance and sleep disturbance by noise, adults≤60=age 30–60 years, elderly= age 60.1–80 years, N. a.=not available, 1strongly/not at all,2strongly or moderately/not at all, 3strongly/moderately or not at all, X=no significant correlation, Adjusted for age, sex, marital status, education and economic status, OR significant by level of significance P < 0.005 is printed in bold, by level of significance 0.005 < P < 0.01 is printed in normal font and by level of significance 0.01 < P < 0.05 is printed in italics.
Hypotheses were subsequently validated using data collected in the second stage (2013). Only some of the hypotheses were confirmed. Significant associations in both phases of the questionnaire survey were: for hypertension, none of the subjective responses to noise represented a significant indicator for the whole dataset (both age groups). However, for elderly people, annoyance by traffic noise was one significant indicator and sleep disturbance by traffic and neighbourhood noise was another significant indicator. For ischaemic heart disease, the general rate of noise annoyance and the general rate of annoyance and sleep disturbance were identified as significant indicators. None of the source-specific variables were significant. For stroke, annoyance and sleep disturbance by traffic and neighbourhood noise were the only significant indicators. ORs, which describe the strength of these associations, are summarized in Table 7, where the results are based on the united data file from 2007 and 2013.
Table 7.
Plausible models (significant in both phases of the questionnaire survey) and estimated odds ratios measuring the association between subjective responses to noise and disease occurrence
| Hypertension | Ischaemic heart disease | Stroke | ||
|---|---|---|---|---|
| Elderly | All | Adults ≤ 60 | All | |
| A t. | ||||
| OR | 1.382 | X | X | X |
| P | 0.00532 | X | X | X |
| 95% CI | (1.10, 1.73)2 | X | X | X |
| A g. | ||||
| OR | X | 1.431 | 1.813 | X |
| 1.543 | ||||
| P | X | 0.00421 | 0.00043 | X |
| 0.00033 | ||||
| 95% CI | X | (1.12, 1.83)1 | (1.30, 2.53)3 | X |
| (1.22, 1.95)3 | ||||
| SD (t. + n.) | ||||
| OR | 1.641 | X | X | X |
| P | 0.00841 | X | X | X |
| 95% CI | (1.13, 2.36)1 | X | X | X |
| (A + SD) (t. + n.) | X | X | X | |
| OR | X | X | X | 1.853 |
| P | X | X | X | 0.01083 |
| 95% CI | (1.15, 2.98)3 | |||
| (A + SD) g. | X | X | X | |
| OR | 1.343 | |||
| P | X | 0.01993 | X | X |
| 95% CI | X | (1.05, 1.70)3 | X | X |
A t.=annoyance by traffic noise, A n.=annoyance by neighbourhood noise, A (t. + n.)=annoyance by traffic and neighbourhood noise, A g.=the general rate of noise annoyance, SD t.=sleep disturbance by traffic noise, SD n.=sleep disturbance by neighbourhood noise, SD (t. + n.)=sleep disturbance by traffic and neighbourhood noise, SD g.=the general rate of sleep disturbance by noise, (A + SD) t.=annoyance and sleep disturbance by traffic noise, (A + SD) n. =annoyance and sleep disturbance by neighbourhood noise, (A + SD) (t. + n.)=annoyance and sleep disturbance by traffic and neighbourhood noise, (A + SD) g. =the general rate of annoyance and sleep disturbance by noise, adults≤ 60=age 30–60 years, elderly= age 60.1–80 years, 1strongly/not at all, 2strongly or moderately/not at all, 3strongly/moderately or not at all, X= no significant correlation, Adjusted for age, sex, marital status, education and economic status, OR significant by level of significance P < 0.005 is printed in bold, by level of significance 0.005 < P < 0.01 is printed in normal font and by level of significance 0.01<P<0.05 is printed in italics.
Discussion
The high correlation between the general rates of annoyance/sleep disturbance and variables dealing with traffic noise shows that traffic noise is a key factor affecting overall noise annoyance. The high correlation between annoyance and sleep disturbance from traffic noise is perhaps linked with the fact that localities close to the busy roads/railways have high noise exposure both in day and at night. High correlation is also between variables dealing with combination traffic and neighbourhood noise and the general rates of noise annoyance/sleep disturbance, but these variables are not identical. Traffic and neighbourhood noise are dominant sources of noise, but other sounds could also contribute to the general rate of annoyance/sleep disturbance (e.g. natural sounds and sounds from unknown origin).
Comparison of the relevance of the variety of indicators revealed that the source-specific indicators are usually weak − only the association between traffic noise and hypertension was shown to be significant in the elderly population. In contrast, indicators that combine levels of annoyance/disturbance from multiple sources or that are based on the total rate of annoyance/disturbance are better indicators in many situations, as they are associated with the studied diseases more frequently than the source-specific factors. Factors based on the combination of traffic and neighbourhood noise are significantly associated with hypertension and stroke while the general rate of noise annoyance (and sleep disturbance) is significantly associated with ischaemic heart disease.
The strong point of the current study lies in its two-phase design which enables elaboration of hypotheses in the first phase and their independent validation in the second phase. In this manner, we have overcome a statistical problem of multiple testing which is present in almost all to date published papers on this topic. One possible solution of this problem is to use Bonferonni or some other correction, leading to use of lower significance level. It would give too conservative results. We solved the problem in other way − we tested the associations significant in the first dataset on new independent dataset, and only the associations significant in both datasets were considered as confirmed. The reduction of false-significant results might be quite dramatic as seen from the comparison of Tables 6 and 7.
Comparison of our results with those of other studies has to be done cautiously; studies involve populations of varying ages with various predictors, adjustments for variables and health endpoints. Furthermore, the degree of noise annoyance/sleep disturbance was not addressed directly in our questionnaire but was calculated during data summarization. In view of this, comparison of results is indicative. Comparison is given for significant associations.
Independently validated overall results reveal a relationship between traffic noise annoyance and hypertension in the elderly (OR 1.38), whereas in the LARES study,[15] this relationship was demonstrated in the adult population (OR 1.42) and in a Berlin, Germany study[4,20] for all respondents aged 31–70 (OR 1.29, road traffic noise only). Other associations detected in our study are based on the general rates or combined subjective responses to noise, in contrast to the majority of other studies which deal with source-specific (traffic or neighbourhood) subjective responses and are therefore not comparable.
A greater number of comparable results can be found among the partial results from the first phase in 2007. The interdependence between traffic noise and hypertension (OR 1.47 for adults aged 30–60 and 1.60 for all respondents aged 30–80) demonstrated in our study corresponds to results from LARES[15] (OR 1.42 for adults) and is slightly greater than that quoted in the study in Berlin, Germany[4,20] (OR 1.29 for all respondents aged 31–70). We have demonstrated the significant association between neighbourhood noise annoyance and hypertension for seniors (OR 1.51), whereas in the LARES,[15] this association was detected in the adult population (OR 1.42). We found a significant association between traffic noise sleep disturbance and hypertension in all respondents (OR 1.44), whereas the German study (general population sample)[4,21] revealed greater interdependency (OR 2.32 for all respondents aged 31–70). The relationship between sleep disturbance from non-specific sources and hypertension (OR 1.26 for all respondents) is comparable to that found by LARES,[14] although in this case, it was confirmed in the adult group only (OR 1.5).
Comparison with other studies dealing with ischaemic heart disease is problematic because the majority of the studies show the relationship between angina pectoris and myocardial infarction, or heart attack, separately. The association between neighbourhood noise annoyance and stroke was demonstrated by this study for seniors (OR 2.63) as in the LARES study[14] (OR 2.4 for seniors). The present study as well as LARES[14] gives insignificant results for the relationship between sleep disturbance for noise from non-specific sources and stroke.
The majority of the studies restrict their focus to partial aspects of mutual relationships among noise levels, feelings of discomfort and the effects on human health. However, in practice these factors are interconnected [Figure 2]. It is worth noting that there might be a two-way causal effect between feelings of discomfort and disease. Subjectively perceived permanent feelings of discomfort might cause cardiovascular problems in accordance with the stress theory of noise effects.[3,13] On the other hand, ill persons, along with the elderly and children, are regarded as groups vulnerable to noise.[22] Health condition is also considered a potential effect modifier of the relationship between noise annoyance and disease.[23] Not even our study can determine the prevailing direction of effects in the relationship between discomfort associated with subjective perception of noise and disease because the analysed data are acquired from a cross-sectional study which is generally unsuitable for demonstrating causality. We are likewise aware of other possible major limitations of the study, such as the summarization of effects of partial noise sources to transportation and neighbourhood noise. Determining the effects of a series of partial sound sources was primarily included in the questionnaire because this information was desired for other purposes. Although categorization of respondents according to their feelings of discomfort was performed so as to yield proportional representation of individual groups similar to LARES,[14] different formulations of questions and the necessity of summarizing noise from a number of sources may lead to disparate results, complicating comparison to other studies. Further, there is adjustment of models only for age and socio-economic characteristics but not for other possible causes of the diseases, as could be revealed by anamnesis or lifestyle factors. The reason for this is that the study was targeted at comparison of the effects of individual subjective responses to noise and not specific diseases and their causes.
Figure 2.
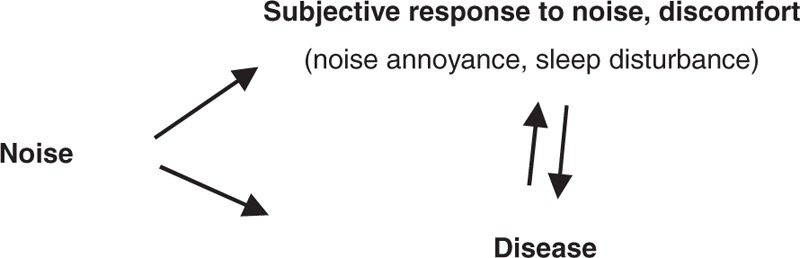
Supposed relationships among noise, subjective response to noise and noise impact on human health
Conclusion
We have investigated different types of subjective responses to noise and their relationships. High correlation can be found between the general rate of annoyance/sleep disturbance and variables dealing with traffic noise. Traffic noise evidently plays a major role in the general discomfort caused by noise. We have also studied the association of subjective responses to noise with selected chronic diseases (hypertension, ischaemic heart disease and stroke). Only one association was significant for source-specific factors − the association between traffic noise and hypertension. Factors that include multiple sources of noise or that are based on total rates of annoyance/disturbance are associated with the studied diseases more frequently. The combination of traffic and neighbourhood noise is significantly associated with hypertension and stroke whereas the general rate of noise annoyance (and sleep disturbance) is significantly associated with ischaemic heart disease. The importance of independent validation of the hypotheses created by multiple models fitting was demonstrated.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The authors would like to acknowledge the support of Ms. Růžena Kubínová, MD, the chief of the national Environmental Health Monitoring System in the Czech Republic, the part of which was the present study.
References
- 1.Babisch W, Dutilleux G, Paviotti M, Backman A, Gergely B, McManus B, et al. Good Practice Guide on Noise Exposure and Potential Health Effects. Copenhagen: European Environmental Agency; 2010. [Google Scholar]
- 2.Burden of Disease from Environmental Noise − Quantification of Healthy Life Years Lost in Europe. Copenhagen: WHO Regional Office for Europe; 2011. [Google Scholar]
- 3.Babisch W. The noise/stress concept, risk assessment and research needs. Noise Health. 2002;4:1–11. [PubMed] [Google Scholar]
- 4.Babisch W. Transportation noise and cardiovascular risk: Updated review and synthesis of epidemiological studies indicate that the evidence has increased. Noise Health. 2006;8:1–29. doi: 10.4103/1463-1741.32464. [DOI] [PubMed] [Google Scholar]
- 5.Babisch W. Road traffic noise and cardiovascular risk. Noise Health. 2008;10:27–33. doi: 10.4103/1463-1741.39005. [DOI] [PubMed] [Google Scholar]
- 6.Babisch W, Kamp Iv. Exposure-response relationship of the association between aircraft noise and the risk of hypertension. Noise Health. 2009;11:161–8. doi: 10.4103/1463-1741.53363. [DOI] [PubMed] [Google Scholar]
- 7.van Kempen EE, Kruize H, Boshuizen HC, Ameling CB, Staatsen BA, de Hollander AE. The association between noise exposure and blood pressure and ischemic heart disease: A meta-analysis. Environ Health Perspect. 2002;110:307–17. doi: 10.1289/ehp.02110307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Miedema HE, Vos H. Exposure-response relationships for transportation noise. J Acoust Soc Am. 1998;104:3432–45. doi: 10.1121/1.423927. [DOI] [PubMed] [Google Scholar]
- 9.Miedema HE, Oudshoorn CG. Annoyance from transportation noise: Relationships with exposure metrics DNL and DENL and their confidence intervals. Environ Health Perspect. 2001;109:409–16. doi: 10.1289/ehp.01109409. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Babisch W, Houthuijs D, Pershagen G, Cadum E, Katsouyanni K, Velonakis M, et al. Annoyance due to aircraft noise has increased over the years − Results of the HYENA study. Environ Int. 2009;35:1169–76. doi: 10.1016/j.envint.2009.07.012. [DOI] [PubMed] [Google Scholar]
- 11.Miedema HE, Vos H. Noise annoyance from stationary sources: Relationships with exposure metric day-evening-night level (DENL) and their confidence intervals. J Acoust Soc Am. 2004;116:334–43. doi: 10.1121/1.1755241. [DOI] [PubMed] [Google Scholar]
- 12.Hurtley CH, Bengs D, editors. Night Noise Guidelines for Europe. Copenhagen: WHO Regional Office Europe; 2009. [Google Scholar]
- 13.Babisch W, Pershagen G, Selander J, Houthuijs D, Breugelmans O, Cadum E, et al. Noise annoyance − A modifier of the association between noise level and cardiovascular health? Sci Total Environ. 2013;452-453:50–7. doi: 10.1016/j.scitotenv.2013.02.034. [DOI] [PubMed] [Google Scholar]
- 14.Niemann H, Maschke Ch. WHO LARES Final Report Noise Effects and Morbidity. Geneva: WHO; 2004. [Google Scholar]
- 15.Niemann H, Bonnefoy X, Braubach M, Hecht K, Maschke C, Rodrigues C, et al. Noise-induced annoyance and morbidity results from the pan-European LARES study. Noise Health. 2006;8:63–79. doi: 10.4103/1463-1741.33537. [DOI] [PubMed] [Google Scholar]
- 16.Maschke C, Niemann H. Health effects of annoyance inducted by neighbour noise. Noise Control Eng J. 2007;55:348–56. [Google Scholar]
- 17.Ohrström E, Barregård L, Andersson E, Skånberg A, Svensson H, Angerheim P. Annoyance due to single and combined sound exposure from railway and road traffic. J Acoust Soc Am. 2007;122:2642–52. doi: 10.1121/1.2785809. [DOI] [PubMed] [Google Scholar]
- 18.Puklová V, editor. Environmental Health Monitoring System, Summary Report, 2014. Prague: National Institute of Public Health; 2015. Available from: http://www.szu.cz/uploads/documents/chzp/souhrnna_zprava/Szu_15_CD.pdf . [Google Scholar]
- 19.Vandasová Z, Vencálek O, Dobisík O. Two decades of noise monitoring: Changes of noise values in urban localities in the Czech Republic. Hygiena. 2013;58:100–5. In Czech. [Google Scholar]
- 20.Babisch W, Issing H, Kruppa B, Wiens D. Verkehrslarm und Herzinfarkt, Ergebnisse zweier Fall-Kontroll-Studien in Berlin. WaBoLu-Hefte 2/92. Berlin: Institut fur Wasser-, Boden-, und Lufthygiene, Umweltbundesamt; 1992. [Google Scholar]
- 21.Muller D, Kahl H, Dortrschy R, Bellach B. Umwelteinwirkungen und Beschwerdenhaufigkeit, Ergebnisse einer Kohortenstudie. SozEp-Hefte 2/1994. Berlin: Institut fur Sozialmedizin und Epidemiologie, Bundesgesundheitsamt; 1994. [Google Scholar]
- 22.Berglund B, Lindvall T, Schwela DH, editors. Guidelines for Community Noise. Geneva: WHO; 1999. [Google Scholar]
- 23.Babisch W, Ising H, Gallacher JE. Health status as a potential effect modifier of the relation between noise annoyance and incidence of ischaemic heart disease. Occup Environ Med. 2003;60:739–45. doi: 10.1136/oem.60.10.739. [DOI] [PMC free article] [PubMed] [Google Scholar]