

Abstract
Introduction
Both C-reactive protein (CRP) and procalcitonin (PCT) are accepted sepsis markers. However, there is still some debate concerning the correlation between their serum concentrations and sepsis severity. We hypothesised that PCT and CRP concentrations are different in patients with infection or with no infection at a similar severity of organ dysfunction or of systemic inflammatory response.
Patients and methods
One hundred and fifty adult intensive care unit patients were observed consecutively over a period of 10 days. PCT, CRP and infection parameters were compared among the following groups: no systemic inflammatory response syndrome (SIRS) (n = 15), SIRS (n = 15), sepsis/SS (n = 71) (including sepsis, severe sepsis and septic shock [n = 34, n = 22 and n = 15]), and trauma patients (n = 49, no infection).
Results
PCT and CRP concentrations were higher in patients in whom infection was diagnosed at comparable levels of organ dysfunction (infected patients, regression of median [ng/ml] PCT = -0.848 + 1.526 sequential organ failure assessment [SOFA] score, median [mg/l] CRP = 105.58 + 0.72 SOFA score; non-infected patients, PCT = 0.27 + 0.02 SOFA score, P < 0.0001; CRP = 84.53 - 0.19 SOFA score, P < 0.005), although correlation with the SOFA score was weak (R = 0.254, P < 0.001 for PCT, and R = 0.292, P < 0.001 for CRP). CRP levels were near their maximum already during lower SOFA scores, whereas maximum PCT concentrations were found at higher score levels (SOFA score > 12).
PCT and CRP concentrations were 1.58 ng/ml and 150 mg/l in patients with sepsis, 0.38 ng/ml and 51 mg/l in the SIRS patients (P < 0.05, Mann–Whitney U-test), and 0.14 ng/ml and 72 mg/l in the patients with no SIRS (P < 0.05). The kinetics of both parameters were also different, and PCT concentrations reacted more quickly than CRP.
Conclusions
PCT and CRP levels are related to the severity of organ dysfunction, but concentrations are still higher during infection. Different sensitivities and kinetics indicate a different clinical use for both parameters.
Keywords: calcitonin, C-reactive protein, infection, procalcitonin, sepsis, sequential organ failure assessment score, systemic inflammatory response syndrome
Introduction
The critically ill patient frequently presents similar clinical pictures in infection, organ dysfunction, and in the various severities of a systemic inflammatory response syndrome (SIRS). Also, differences in body temperature (BT), heart rate, white blood cell (WBC) count, and respiratory rate often are small. As a consequence, diagnosis of sepsis and infection can be difficult: positive bacteriological samples may be late or absent, the clinical interpretation of local colonisation may be ambiguous, and traditional markers of infection such as BT and WBC count may be unspecific.
Other parameters such as C-reactive protein (CRP) and procalcitonin (PCT) have been considered to evaluate the evolution of infections and sepsis in critically ill patients [1-5]. However, induction of these parameters is also multifactorial. Infection, severe systemic inflammation, organ dysfunction, tissue trauma, and many other aetiologies cause their induction (for reviews see [6,7]). To distinguish organ-dysfunction-related induction and infection-related CRP or PCT response can be difficult. Various recently published studies indicate that there is a significant relationship of PCT not only to infection and systemic inflammation, but also to organ dysfunction as well as various types of tissue trauma [7-12].
Given this information, a retrospective look at former studies indicates that classification according to the severity of organ dysfunction is not reported in every study, or that groups with infection or with no infection were not balanced well according to the severity of organ dysfunction. Since various conditions are known to induce a PCT response in vitro and in vivo, and the source of PCT production is not finally known, the role of infection in patients with multiple organ dysfunction syndrome should be further elucidated.
In the case of CRP, no definite correlation between infection and change of plasma concentrations have been documented [2], but some authors have reported that daily measurement of CRP is useful in the detection of sepsis and that it is more sensitive than currently used markers, such as BT and WBC count [13]. PCT also has been proposed as an indicator of the presence of infection [3-5], and definitively as a useful marker of the severity of sepsis [4,14,15]. However, in the clinical context it is often difficult to define CRP or PCT as an independent variable for diagnosis of infection due to the multiple causes of induction and the comorbidity of infection, systemic inflammation, organ dysfunction, endotoxinaemia, bacterial translocation, and tissue trauma in many critically ill patients. A variety of recent publications demonstrated conditions without infection that induce PCT (e.g. cardiogenic shock, major surgery including cardiac surgery, accidental trauma, pancreatitis, or burn trauma) [8,10-12,16-19].
Knowing these data, we sought to further define the features of CRP and PCT. We have analysed these features in critically ill patients with systemic inflammation who had infection (sepsis, severe sepsis, and septic shock) or had no infection at various severities of organ dysfunction (sequential organ failure assessment [SOFA] score), or a systemic inflammatory response (SIRS, and no SIRS). We have also compared the profile and kinetics of both parameters. Patients with trauma without infection were analysed as a separate group, since trauma may induce a significant response of PCT and CRP in some patients.
Materials and methods
From May 1999 to April 2000, all adult patients consecutively admitted to the mixed medicosurgical intensive care unit (ICU) at the Carlo Poma Hospital in Mantova, Italy were studied. Neurosurgical and elective surgical patients without complications were excluded. The study was approved by the local Ethics Committee and care of the patients was directed by the same existing protocols.
At the time of admission and every day thereafter, signs and symptoms, clinical and laboratory data including PCT, CRP, BT, WBC count, arterial blood-gas analysis, and lactate levels were collected and scheduled. Samples were collected for cultures depending on the clinical symptoms. We used the American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference definition of sepsis to identify patients with sepsis, severe sepsis, septic shock, and SIRS [20]. The SOFA score was used to describe a sequence of complications and the severity of organ dysfunction in critically ill patients [21]. The grading of sepsis was assessed with the sepsis score [22].
On the basis of clinical, laboratory and bacteriological findings, the patients were split into four groups and studied for 10 days: trauma group, patients admitted with trauma; SIRS group, patients who developed clinical signs of systemic inflammatory response [23] but had no defined source of infection; SEPSIS/SS group, patients with SIRS and a known source of infection and/or positive blood cultures (these patients were divided into sepsis, severe sepsis, and septic shock according to American College of Chest Physicians/Society of Critical Care Medicine criteria); and no SIRS group, medicosurgical patients without trauma or SIRS.
Infection was defined when clinical signs of systemic inflammatory response were present, determined by a definable source of infection (microbiology confirmed) and/or positive blood cultures.
Day 1 (T1) was defined as the first observational day at admission, and the next day was named T2 (day 2), then T3 (day 3), and so on. Collected data regarding the groups were double blinded to the results of the serum PCT level.
CRP was measured using a nephelometric method (BNA 100; Dade Behring, Marburg, Germany). Samples for PCT determination were stored at -20°C for < 2 weeks, and measurement was performed by immunoluminometric assay (B.R.A.H.M.S.; Diagnostica AG, Hennigsdorf/Berlin, Germany and LUMItest PCT ILMA-kit; Liamat Instruments, BYK Gulden, Italy). Lactate levels were measured using a blood-gas analyser (model 865; Ciba Corning Diagnostics Corp., Medfield, MA, USA).
Statistical analysis
The results are presented as the median and 25th/75th percentiles (data non-normally distributed). The Kolmogorov–Smirnov test was used to assess sample distributions. To compare two independent samples we used an unpaired t-test or the Mann–Whitney U-test (data non-normally distributed). To compare three independent groups we used analysis of variance or the Kruskal–Wallis test (data non-normally distributed) with Bonferroni corrections. Serial sample data from the same patient were compared by Wilcoxon's test for non-parametric paired samples. We used the chi-square test to compare proportions. Receiver operating characteristic (ROC) curves and the areas under the respective curve were calculated. The maximum PCT and CRP concentrations, the maximum SOFA score and sepsis score in the first 24 hours (T1) were used to calculate the ROC curves. Among the PCT, CRP, lactate and SOFA score, Pearson's correlation and the regression formula were calculated (y = a + bx).
For comparison, the slope of the regression lines was calculated using analysis of variance, and the crossing of the regression line at the y axis was calculated with analysis of covariance.
P < 0.05 was considered significant. Statistical calculations were performed with SPSS statistical software (version 10.0; SPSS Inc., Chicago, IL, USA).
Results
One hundred and fifty patients were studied: 15 no SIRS patients (respiratory, renal, and neurologic failure), 15 SIRS patients (two with respiratory failure, seven with cardiac failure, myocardial infarction, and pulmonary embolism, four with neurological diseases and stroke, and two with poisoning), 49 trauma patients (37 with multiple trauma and 12 with head injury only) and 71 sepsis/SS patients (26 with pneumonia, 24 with peritonitis, 13 with bloodstream infection, seven with soft tissue infection, and one with bacterial meningitis – 34 with sepsis, 22 with severe sepsis, and 15 with septic shock). A total of 1222 observation days (mean, 8 days; range, 1–10 days) were evaluated. The age range was from 15 to 89 years (median age, 59.2 years), and 96 patients were male (64%). Twenty-nine patients died with a mortality rate of 19% (eight patients with septic shock, six patients with severe sepsis and six patients with sepsis, four patients with SIRS, three patients with no SIRS, and two patients with trauma).
The CRP, PCT and Sepsis score values were higher both in sepsis and sepsis/SS groups versus SIRS and no SIRS groups (P < 0.05). The SOFA score and PCT level were higher in septic shock versus severe sepsis versus sepsis (P < 0.05). The lactate plasma level was higher in septic shock versus severe sepsis (P < 0.05), and the sepsis score was higher in severe sepsis versus sepsis (P < 0.05). The values at admission in the groups are presented in Table 1.
Table 1.
Procalcitonin (PCT), C-reactive protein (CRP), lactate and sepsis score values at different categories of the sequential organ failure assessment (SOFA) score and severity of systemic inflammation according to American College of Chest Physicians/Society of Critical Care Medicine (ACCP/SCCM) criteria
| SOFA | PCT (ng/ml) | CRP (mg/l) | Lactate (mmol/l) | Sepsis score | |
| Category of SOFA score (number of observations) | |||||
| 1–6 (n = 557) | 3 (2/5) | 0.37 (0.12/1.2) | 101 (53/161) | 1.24 (0.96/1.6) | 6 (3/10) |
| 7–12 (n = 156) | 9 (7/10) | 2.55 (0.85/9.95) | 140 (65/209) | 1.74 (1.2/2.43) | 13 (10/16) |
| 13–18 (n = 31) | 14 (13/15) | 8.5 (3.3/28.4) | 180 (115/219) | 3 (2.34/3.83) | 21.5 (16.25/25.75) |
| 19–24 (n = 13) | 19.5 (19/20) | 23.24 (2.28/50.92) | 154 (9.6/308) | 3.7 (3.5/5) | 25(24.25/25.75) |
| Category according to ACCP/SCCM criteria (number of patients) | |||||
| No SIRS (n = 15) | 3 (2–4.5) | 0.14 (0.07–0.29) | 72 (20–125) | 1.26 (0.64–1.38) | 3 (0–5.5) |
| SIRS (n = 15) | 4 (2.25–8.25) | 0.38 (0.16–0.93)* | 51 (19.5–80.5) | 2.13 (1.14–2.93)* | 3.5 (2–8.25) |
| Sepsis/SS (n = 71) | 6 (4–9) | 3 (1.48–15.26)** | 164 (75–222)** | 2.2 (1.27–3.74) | 11 (7–17)** |
| Sepsis (n = 34) | 4.5 (3–6) | 1.58 (0.41–3) ** | 150 (71–209)** | 1.37 (1–2.61) | 8.5 (3.75–12.25)** |
| Severe sepsis (n = 22) | 7 (6–8.25)† | 5.58 (1.84–32.93)† | 159 (75–209) | 2.19 (1.73–2.93) | 14.5 (9.25–19.75)† |
| Septic shock (n = 15) | 11 (9–15)d | 13.1 (6.1–42.2)‡ | 195 (75–272) | 3.7 (2.6–6.4)‡ | 15 (13.5–19.5) |
| Trauma patients (n = 49) | 5 (3–8) | 1.4 (0.3–5.1) | 40 (16–150) | 2.7 (1.7–5) | 3 (0–5.3) |
All patient groups without trauma were evaluated. Trauma patients were in a separate group. Data presented as median values (lower and upper quartiles). SIRS, systemic inflammatory response syndrome. * P < 0.05 versus no systemic inflammatory response syndrome (No-SIRS), ** P < 0.05 versus SIRS, † P < 0.05 versus sepsis, ‡ P < 0.05 versus severe sepsis.
The area under the ROC curve in the diagnosis of sepsis versus SIRS was 0.794 for CRP (cutoff, 90 mg/l) and was 0.731 for PCT (cut-off, 1.2 ng/ml) (P < 0.05) (Fig. 1). The area under the ROC curve in the diagnosis of sepsis/SS, excluding the trauma group (the diagnosis at admission is obvious), was 0.866 for PCT, 0.755 for CRP, 0.862 for sepsis score, and 0.731 for SOFA (P < 0.05 for all) (Fig. 2).
Figure 1.

Receiver operating characteristic (ROC) curves (95% confidence interval) for the prediction of sepsis versus systemic inflammatory response syndrome. C-reactive protein (CRP) (thin dashed line), 0.794 (0.644–0.944) (standard error, 0.05; P < 0.05); best cut-off, 90 mg/l; sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV), 74, 85, 92, and 53. Procalcitonin (PCT) (thick solid line), 0.731 (0.587–0.875) (standard error, 0.05; P < 0.05); best cut-off, 1.2 ng/ml; sensitivity, specificity, NPV, and PPV, 63, 87, 92, and 51. Sepsis score (thin solid line), 0.701 (0.534–0.869) (standard error, 0.08; P = 0.055). Sequential organ failure assessment score (thick dashed line), 0.505 (0.299–0.711) (standard error, 0.105; P = 0.96).
Figure 2.
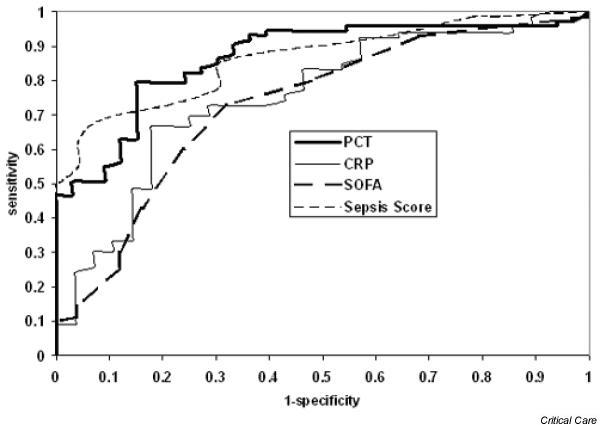
Receiver operating characteristic (ROC) curves (95% confidence interval) for the prediction of sepsis/SS; the trauma group was excluded (diagnosis at admission was obvious). Procalcitonin (PCT) (thick solid line), 0.866 (0.79–0.93) (standard error, 0.04; P < 0.001); best cut-off, 1.11 ng/ml; sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV), 79, 85, 92, and 65. Sepsis score (thin dashed line), 0.862 (0.78–0.93) (standard error, 0.04; P < 0.001); best cut-off, 5.5; sensitivity, specificity, NPV, and PPV, 66, 71, 66, and 71. C-reactive protein (CRP) (thin solid line), 0.755 (0.64–0.86) (standard error, 0.05; P < 0.001); best cut-off, 128 mg/l; sensitivity, specificity, NPV, and PPV, 67, 82, 90, and 51. Sequential organ failure assessment (SOFA) score (thick dashed line), 0.731 (0.61–0.84) (standard error, 0.06; P < 0.001); best cut-off, 4.5; sensitivity, specificity, NPV, and PPV, 73, 68, 86, and 47.
The admission PCT values of trauma patients who developed sepsis (not included in sepsis/SS) were higher than in patients without septic complications: 3.4 (2.63–12.71) ng/ml versus 1.2 (0.5–5.2) ng/ml (P < 0.05). Trauma patients at the moment of septic complications did not present a significant increase of plasma CRP values, but did present an early and quick significant increase of PCT, as compared with concentrations measured 1 day prior to the diagnosis: 153 ± 89 mg/l versus 174 ± 84 mg/l for CRP (P = not significant) and 0.85 (0.45–1.14) ng/ml versus 2.1 (1.01–6.14) ng/ml for PCT (P < 0.05).
The time courses of the median CRP level, PCT level, SOFA score and sepsis score in the sepsis group were analysed (Fig. 3). CRP and PCT levels were significantly higher in the sepsis group versus the SIRS and no SIRS groups from T1 to T5 (P < 0.05). The maximum serum PCT levels were seen 1 day earlier (T1) than CRP in sepsis/SS (3 ng/ml; range, 1.48–15.26 ng/ml), at T1 in the SIRS (0.38 ng/ml; range, 0.16–0.93 ng/ml) and the no SIRS groups (0.14 ng/ml; range, 0.07–0.29 ng/ml), and at T2 in the trauma group (1.41 ng/ml; range, 0.4–4.2 ng/ml).
Figure 3.
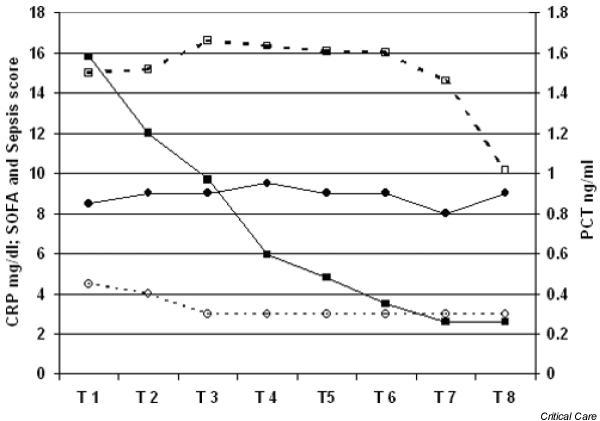
Median serum procalcitonin (PCT, ng/ml), C-reactive protein (CRP, mg/dl), sequential organ failure assessment (SOFA) score and sepsis score (score values) time course in sepsis (34 patients). Six nonsurvivors: one in T2, one in T5, one in T6, and three in T8-T9. ■, PCT; □, CRP; ●, sepsis score; ○ SOFA score.
The maximum serum CRP levels were at T2–T3 in the sepsis/SS group (165 mg/l; range, 107–216 mg/l), at T3 in the no SIRS group (89 mg/l; range, 37–122 mg/l), at T5 in the SIRS group (103 mg/l; range, 38–154 mg/l) and at T8 in the trauma group (116 mg/l; range, 67–158 mg/l), which was later compared with PCT.
In the sepsis/SS group only the SOFA score at admission was predictive of outcome (Fig. 4): non-survivors achieved higher scores than survivors (10.5; range, 5.7–14.2 versus 5; range, 4–7; P < 0.001).
Figure 4.
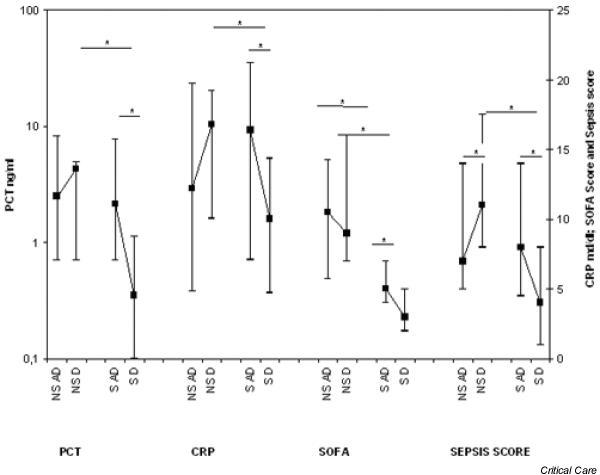
Sepsis/SS group: median and 25th/75th percentiles of procalcitonin (PCT), C-reactive protein (CRP), sequential organ failure assessment (SOFA) score and sepsis score in nonsurvivors (NS) and survivors (S) at admission (AD) and discharge (D). * P < 0.05.
Correlations with SOFA score
When PCT, CRP and lactate concentrations were analysed according to the various severities of organ dysfunction measured by the SOFA score, weak correlations of PCT and CRP, and increasing values of both parameters during more severe stages of organ dysfunction were observed.
In nontrauma patients, correlation of the PCT level and SOFA score was 0.254, that of the CRP level and SOFA score was 0.292, and the correlation was 0.378 for lactate (P < 0.001 for all; Pearson's correlation). To indicate the different induction characteristics of the parameters, concentrations of each parameter during four different groups of SOFA score are presented in Table 1. PCT and lactate concentrations were low in patients with low score values of the SOFA score, and maximum concentrations were observed only at higher score values, indicating multiple organ dysfunction, especially at SOFA > 12. On the contrary, CRP values were near their maximum levels already during minor score values (< 12), and did not increase much further in patients with higher score values. Lactate plasma levels had only a limited range of concentrations (10th/90th percentiles from 0.7 at lower SOFA scores to 6.5 at higher scores).
Correlation and regression were calculated for the infection parameters and SOFA score in noninfected and infected patients. In both groups, lactate values correlated weakly with the SOFA score: 0.35 and 0.382, respectively, in noninfected and infected patients (P < 0.001); in the infection group, correlation was 0.247 for PCT and 0.286 for CRP (P < 0.001). When measurements at time points with and without infection were compared, CRP and PCT concentrations were more increased in patients with infection, indicated by the higher slope (b) of the regression line, at similar SOFA score levels (P < 0.02 for PCT, and P < 0.001 for CRP).
The regression (y = a + bx) for the PCT level and SOFA score was PCT = 0.27 + 0.02 SOFA score in noninfected patients and was PCT = -0.848 + 1.526 SOFA score in infected patients (Fig. 5). The respective values for the CRP level were CRP = 84.53 - 0.19 SOFA score and CRP = 105.58 + 0.72 SOFA score (Fig. 6).
Figure 5.
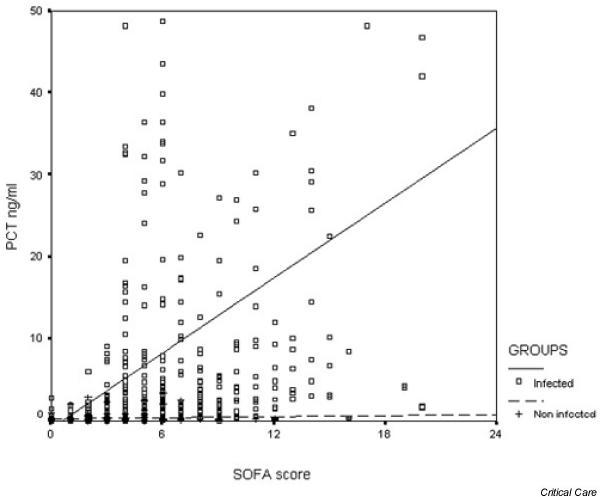
Procalcitonin (PCT)–sequential organ failure assessment (SOFA) correlation in infected patients (PCT = -0.84 + 1.526 × SOFA score, ng/ml) and noninfected patients (PCT = 0.27 + 0.02 × SOFA score, ng/ml). * P < 0.02. □ and solid line, infected and regression line; + and dashed line, noninfected and regression line.
Figure 6.
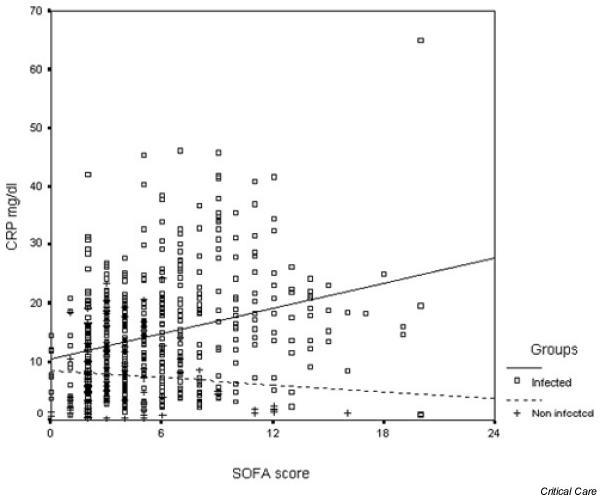
C-reactive protein (CRP)–sequential organ failure assessment (SOFA) correlation in infected patients (CRP = 105.58 + 0.72 × SOFA score, mg/l) and noninfected patients (CRP = 84.53 - 0.19 × SOFA, mg/l). Data presented in mg/dl. * P < 0.001. □ and solid line, infected and regression line; + and dashed line, noninfected and regression line.
Crossing of the regression line at the y axis for PCT is low, but it is high (84/105 mg/l) for CRP, indicating the higher reactivity of this parameter in the less severe stages of disease as compared with PCT. Accordingly, when CRP and PCT were categorised according to four groups of the SOFA score in noninfected and infected patients (not including trauma patients), lower PCT concentrations despite higher score levels of organ dysfunction (SOFA score) were seen in patients without infections. However, the low number of measurements in patients with high SOFA score values who had no infection limits further statistical evaluation of the data (Table 2).
Table 2.
Procalcitonin (PCT), C-reactive protein (CRP), and lactate plasma levels at various severities of organ dysfunction, categorised according to four groups of the sequential organ failure assessment (SOFA) score, comparing patients with and without infection and trauma
| Category of SOFA score (number of observations, noninfected/infected) | Noninfected | Infected | P, noninfected /infected | Trauma (number of trauma observations) |
| PCT (ng/ml) | ||||
| 1–6 (n = 180/377) | 0.14 (0.08/0.33) | 0.62 (0.24/2.12) | < 0.001 | 0.25 (0.08–0.9) (n = 368) |
| 7–12 (n = 24/132) | 0.25 (0.2/0.3) | 2.43 (1.2/8.68) | < 0.001 | 5.54 (0.86–12.87) (n = 88) |
| 13–18 (n = 1/30) | 0.41 | 8.5 (3.39/29.59) | n.s. | 54 (15.58–122.4) (n = 9) |
| 19–24 (n = 0/13) | - | 23.24 (2.28/50.9) | - | - |
| Pearson's correlation | 0.108 (P = n.s.) | 0.247 (P < 0.001) | 0.465 (P <0.001) | |
| Regression, y = a + bx | 0.27 + 0.02 × SOFA score | -0.84 + 1.526 × SOFA score | < 0.02 | -5 + 2.16 × SOFA score |
| CRP (mg/l) | ||||
| 1–6 (n = 180/377) | 68 (28/121) | 121 (68/176) | < 0.001 | 91 (49.8–148) (n = 368) |
| 7–12 (n = 24/132) | 47(15/81) | 181 (78/271) | < 0.001 | 110 (64–151) (n = 88) |
| 13–18 (n = 1/30) | 12.3 | 183 (128/219) | n.s. | 94 (n = 9) |
| 19–24 (n = 0/13) | - | 154 (9.6/308) | - | - |
| Pearson's correlation | 0.069 (P = n.s.) | 0.286 (P < 0.001) | 0.095 (P = n.s.) | |
| Regression, y = a + bx | 84.53 - 0.19 × SOFA score | 105.58 + 0.72 × SOFA score | < 0.001 | 95 + 0.24 × SOFA score |
| Lactate (mmol/l) | ||||
| 1–6 (n = 180/377) | 1.21 (0.96/1.44) | 1.3 (1.04/1.69) | n.s. | 1.1 (0.86–1.51) (n = 368) |
| 7–12 (n = 24/132) | 1.55 (1.22/3.54) | 1.69 (1.2/2.2) | n.s. | 2.09(1.19–2.61) (n = 88) |
| 13–18 (n = 1/30) | 2.8 | 3.07 (2.25/3.59) | n.s. | 5.58 (n = 9) |
| 19–24 (n = 0/13) | - | 3.69 (3.52/5) | - | - |
| Pearson's correlation | 0.350 (P < 0.002) | 0.382 (P < 0.001) | 0.431 (P <0.001) | |
| Regression, y = a + bx | 0.918 + 0.14 × SOFA score | 0.968 + 0.12 × SOFA score | n.s. | 0.516 + 0.235 × SOFA score |
Data presented as median values (lower and upper quartiles). P value from Mann–Whitney U-test.
Discussion
Various studies report higher PCT and CRP values in patients with bacterial infection as compared with those with viral infection, autoimmune disorders, or other nonbacterial infection-related inflammatory disease [24-28], and in patients with sepsis, severe sepsis or septic shock with documented infections [15]. The role of PCT and CRP in the diagnosis of infection was evaluated [14]; PCT and CRP were significantly higher in patients with infection as compared with those without infection. However, beside infection-related induction of PCT, there are plenty of data indicating an inflammation-related induction of PCT [10-12,16-18]. Various further stimuli, meanwhile, are known to induce PCT, CRP, and cytokines beside bacterial endotoxins or bacterial products [29-31]. A detailed analysis of the influence of the various severities of organ dysfunction has not been conducted in these studies. A relation of PCT and various severities of organ dysfunction has been published previously, supporting the observation of organ dysfunction and systemic inflammation-related induction of PCT and CRP. However, in this previous study by Meisner and colleagues, patients were not separated according to the presence of infection or its absence [9].
In the present study, not only plasma levels of PCT and CRP were compared at the various severities of systemic inflammation and sepsis, but also plasma levels in patients with and without infection at different levels of organ dysfunction, assessed by the SOFA score [21,32]. Furthermore, we have described the kinetics of both parameters in critically ill patients with trauma, with SIRS and with sepsis (SIRS and infection).
PCT and CRP concentrations, despite organ dysfunction, were higher in patients with infection, indicated by the higher slope of regression and higher plasma levels at comparable categories of the SOFA score in patients with infection, and the higher values in corresponding categories of the SOFA score. These data indicate that PCT and CRP indeed are parameters that, in particular, are more strongly induced in patients in whom the systemic inflammatory response is complicated by infection, or vice versa. When the data were categorised according to four groups of the SOFA score, data were valid only for lower score groups (SOFA < 12), since the number of patients analysed without infection was too small for statistical analysis during more severe stages of organ dysfunction.
We also report different further features of CRP and PCT. CRP concentrations were high already during the less severe stages of organ dysfunction and systemic inflammation, but values were not much further increased during the more severe stages of disease. On the contrary, PCT levels especially increased in patients with organ dysfunction, severe sepsis or septic shock.
Also the kinetics were different for both parameters. PCT concentrations had their maximum levels prior to those of CRP, and the concentrations more rapidly declined as compared with CRP. Various aspects are thus required to describe the clinical usefulness of such parameters for the diagnosis of sepsis and infection in critically ill patients.
In the present study, higher levels of PCT and CRP in patients with sepsis as compared with those with SIRS only were also reported. Higher levels of PCT and CRP during sepsis as compared with SIRS or no SIRS have been described previously in numerous publications [4,8]. Some studies, on the contrary, do not indicate a significant difference. As a consequence, the usefulness of PCT and CRP in discriminating between SIRS and sepsis is debated.
Whereas a significant increase of PCT during severe sepsis and septic shock remains undisputed and is the major strength of PCT, the role of PCT in the discrimination of SIRS, no SIRS and sepsis is equivocal, although the majority of studies indicate higher values in patients with sepsis. The ambiguous conclusions of different studies regarding the diagnostic accuracy of PCT and CRP are mainly due to the lack of a gold standard for infection, the propagation and misuse of an insensitive assay in the wrong clinical setting (e.g. early infection or immunocompromised patients), and the negligence of the fact that, as for all hormones, different cut-off levels have to be used according to the clinical questions asked. But the definition of infection is a methodological limitation in all similar studies.
In the present study, infection was defined when clinical signs of systemic inflammatory response were present, determined by a definable source of infection (microbiology confirmed) and/or positive blood cultures. Therefore, potentially infected patients with negative cultures would be misclassified into the SIRS group.
Povoa and colleagues [13] and Mimoz and colleagues [33] found that the 'normal' plasma CRP level in critically ill patients rarely lies within the normal range for a healthy population. CRP also was not useful in distinguishing evolution of sepsis in severe sepsis and septic shock [34], and septic complications in patients with trauma [35]; in the late post-traumatic period, the CRP values remained high [11,18,36]. Elevated concentrations of serum CRP at admission are correlated with an increased risk of organ failure and death [37]. In our study, patients with SIRS or no SIRS also had elevated CRP levels, but the CRP over time was significantly higher in sepsis/SS patients. However, during the course of the disease we did not observe significant changes in the CRP sepsis-related level. Also, in septic patients, CRP values increased to a maximum level only at T2–T3 and remained elevated for many days.
The PCT level, on the contrary, remains in the lower range during infection or systemic inflammation of less gravity, and high levels are found during severe sepsis and septic shock. Some authors found that PCT (and CRP) had poor sensitivity and specificity for the diagnosis of infection [14]. The discriminative power is higher for diagnosis of sepsis, severe sepsis or septic shock [15,34]. In our study, elevated PCT levels closely marked the sepsis versus the SIRS and versus the no SIRS groups, and also in demarking the severe sepsis and septic shock groups; during the ICU stay, PCT and CRP values increased in septic complications. This fact is helpful in patients with SIRS and when signs of sepsis are misleading and/or absent. Nevertheless, we observed that in septic events plasma PCT increased or lowered more quickly than CRP; perhaps this is related to a more rapid PCT kinetics (Fig. 3). The maximum PCT level in the sepsis/SS group was at T1, and this kinetic characteristic allows anticipation of a diagnosis of sepsis 24–48 hours before the CRP level would.
Day-to-day evaluation of the common parameters are useful to predict evolution of sepsis and clinical outcome; only patients who survived presented a significant reduction of CRP level, PCT level, SOFA score and sepsis score values. In the trauma group, when infectious complications occurred, the PCT values rose promptly and marked the septic event. Moreover, we observed that trauma patients who developed sepsis presented at ICU admission with higher PCT levels than patients with a favourable evolution to recovery. These trauma patients with a higher PCT level at admission are at risk of infections and must be strictly monitored with bacteriological samples to recognise septic complications.
For low PCT and CRP plasma values (approximately 0.3–0.6 ng/ml and 60–80 mg/l, respectively), the diagnosis of sepsis from SIRS is not simple in ICU patients; neither of these two markers alone possesses good discriminant value, especially in a heterogeneous mix of diseases. The SIRS concept is simple but aspecific, and in a patient with sepsis the degree of sepsis and his/her organ dysfunction cannot be identified by a single marker. Like other workers, we agree that PCT and CRP levels may be useful together with full clinical assessment including signs of sepsis, bacteriological data, and organ function evaluation [9,37,38]. We found that the increase and decrease of PCT values correlated with the worsening or the healing of the sepsis and systemic inflammatory response, respectively.
Conclusions
The data of the present study indicate that PCT and CRP both are infection-related parameters. However, both proteins are also induced during noninfectious causes of systemic inflammation and in patients with organ dysfunction. Both parameters have different kinetics and profiles of induction: the kinetics of CRP is slower than that of PCT, and CRP concentrations are induced near to their maximum also during less severe symptoms of systemic inflammation and organ dysfunction. Thus, in critically ill patients, both parameters (CRP and PCT) provide different information. In patients with severe systemic inflammation, severe sepsis, and organ dysfunction, PCT has demonstrated itself to be a parameter with a wide range of concentrations and clinically useful kinetics, thus being the better parameter of the two to estimate the severity, prognosis, and time course of disease.
Key messages
• Both CRP and PCT were higher in patients in whom infection was diagnosed at comparable levels of organ dysfunction; CRP was already increased during minor severity of organ dysfunction and sepsis, but did not further increase during more severe stages of the disease.
• PCT on the contrary was low during SIRS and sepsis, but high in patients with severe sepsis/septic shock and higher categories of the SOFA score.
• PCT reacted more quickly than CRP and this kinetic characteristic allows anticipation of a diagnosis of sepsis 24-48 hours before the CRP level would.
• In the trauma patient, when infectious complication occurred, PCT values rose promptly and marked the septic event.
Competing interests
None declared.
Abbreviations
BT = body temperature; CRP = C-reactive protein; ICU = intensive care unit; PCT = procalcitonin; ROC = receiver operating characteristic; SIRS = systemic inflammatory response syndrome; SOFA = sequential organ failure assessment; SS = whole group of sepsis including, sepsis, severe sepsis and septic shock; WBC = white blood cell.
Contributor Information
Gian Paolo Castelli, Email: gianpaolo.castelli@inwind.it.
Claudio Pognani, Email: claudio.pognani@tin.it.
References
- Yentis SM, Soni N, Sheldon J. C-reactive protein as an indicator of resolution of sepsis in the intensive care unit. Intensive Care Med. 1995;21:602–605. doi: 10.1007/BF01700168. [DOI] [PubMed] [Google Scholar]
- Matson A, Soni N, Sheldon J. C-reactive protein as a diagnostic test of sepsis in the critically ill. Anaesth Intensive Care. 1991;19:182–186. doi: 10.1177/0310057X9101900204. [DOI] [PubMed] [Google Scholar]
- Assicot M, Gendrel D, Carsin H, Raymond J, Guilbaud J, Bohoun C. High serum procalcitonin concentrations in patients with sepsis and infection. Lancet. 1993;341:515–518. doi: 10.1016/0140-6736(93)90277-N. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Al-Nawas B, Krammer I, Shah PM. Procalcitonin in diagnosis of severe infections. Eur J Med Res. 1996;1:331–333. [PubMed] [Google Scholar]
- Gramm HJ, Beier W, Zimmermann J, Oedra N, Hannemann L, Boese-Landgraf J. Procalcitonin (ProCT) – a biological marker of the inflammatory response with prognostic properties. Clin Intensive Care. 1995;[Abstract] 6(Suppl 2):71. [Google Scholar]
- Meisner M, Reinhart K. Is procalcitonin really a marker of sepsis? Int J Intensive Care. 2001;8:15–25. [Google Scholar]
- Meisner M. Pathobiochemistry and clinical use of procalcitonin. Clin Chim Acta. 2002;323:17–29. doi: 10.1016/S0009-8981(02)00101-8. [DOI] [PubMed] [Google Scholar]
- de Werra I, Jaccard C, Corradin SB, Chiolero R, Yersin B, Gallati H, Assicot M, Bohuon C, Baumgartner JD, Glauser MP, Heumann D. Cytokines, nitrite/nitrate, soluble tumor necrosis factor receptors, and procalcitonin concentrations: Comparisons in patients with septic shock, cardiogenic shock, and bacterial pneumonia. Crit Care Med. 1997;25:607–613. doi: 10.1097/00003246-199704000-00009. [DOI] [PubMed] [Google Scholar]
- Meisner M, Tschaikowsky K, Palmaers T, Schmidt J. Comparison of procalcitonin (PCT) and C-reactive protein (CRP) plasma concentrations at different SOFA scores during the course of sepsis and MODS. Crit Care. 1999;3:45–55. doi: 10.1186/cc306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wanner GA, Keel M, Steckholzer U, Beier W, Stocker R, Ertel W. Relationship between procalcitonin plasma levels and severity of injury, sepsis, organ failure, and mortality in injured patients. Crit Care Med. 2000;28:950–957. doi: 10.1097/00003246-200004000-00007. [DOI] [PubMed] [Google Scholar]
- Meisner M, Tschaikowsky K, Hutzler A, Schick C, Schüttler J. Postoperative plasma concentrations of procalcitonin after different types of surgery. Intensive Care Med. 1998;24:680–684. doi: 10.1007/s001340050644. [DOI] [PubMed] [Google Scholar]
- Carsin H, Assicot M, Feger F, Roy O, Pennacino I, Le Bever H, Ainaud P, Bohuon C. Evolution and significance of circulating procalcitonin levels compared with IL-6, TNF-alpha and endotoxin levels early after thermal injury. Burns. 1997;23:218–224. doi: 10.1016/S0305-4179(96)00124-6. [DOI] [PubMed] [Google Scholar]
- Povoa P, Almeida E, Moreira P, Fernandes A, Mealha R, Aragao A, Sabino H. C-reactive protein as an indicator of sepsis. Intensive Care Med. 1998;24:1052–1056. doi: 10.1007/s001340050715. [DOI] [PubMed] [Google Scholar]
- Ugarte H, Silva E, Mercan D, De Mendonca A, Vincent J-L. Procalcitonin used as a marker of infection in the intensive care unit. Crit Care Med. 1999;27:498–504. doi: 10.1097/00003246-199903000-00024. [DOI] [PubMed] [Google Scholar]
- Müller B, Becker KL, Schächinger H, Rickenbacher PR, Huber PR, Zimmerli W, Ritz R. Calcitonin precursors are reliable markers of sepsis in a medical intensive care unit. Crit Care Med. 2000;28:977–983. doi: 10.1097/00003246-200004000-00011. [DOI] [PubMed] [Google Scholar]
- Brunkhorst FM, Clark AL, Forycki ZF, Anker SD. Pyrexia, procalcitonin, immune activation and survival in cardiogenic shock: the potential importance of bacterial translocation. Int J Cardiol. 1999;72:3–10. doi: 10.1016/S0167-5273(99)00118-7. [DOI] [PubMed] [Google Scholar]
- Meisner M, Hutzler A, Tschaikowsky K, Harig F, von der Emde J. Postoperative plasma concentration of procalcitonin and C-reactive protein in patients undergoing cardiac and thoracic surgery with and without cardiopulmonary bypass. Cardiovasc Eng. 1998;3:174–178. [Google Scholar]
- Meisner M, Rauschmayer C, Schmidt J, Feyrer R, Cesnevar R, Bredle D, Tschaikowsky K. Early increase of procalcitonin after cardiovascular surgery in patients with non-infectious and infectious postoperative complications. Intensive Care Med. 2002;28:1094–1102. doi: 10.1007/s00134-002-1392-5. [DOI] [PubMed] [Google Scholar]
- Rau B, Steinbach G, Gansauge F, Mayer M, Grünert A, Beger HG. The role of procalcitonin and interleukin-8 in the prediction of infected necrosis in acute pancreatitis. Gut. 1997;41:832–840. doi: 10.1136/gut.41.6.832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20:864–874. [PubMed] [Google Scholar]
- Vincent JL, Moreno R, Takala J, Willats S, De Medonca A, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996;22:707–710. doi: 10.1007/s001340050156. [DOI] [PubMed] [Google Scholar]
- Elebute EA, Stoner HB. The grading of sepsis. Br J Surg. 1983;70:29–31. doi: 10.1002/bjs.1800700111. [DOI] [PubMed] [Google Scholar]
- Rangel-Frausto MS, Pittet D, Costigan M, Hwang T, Davis C, Wenzel RP. The natural history of the systemic inflammatory response syndrome (SIRS) JAMA. 1995;273:117–123. doi: 10.1001/jama.273.2.117. [DOI] [PubMed] [Google Scholar]
- Gendrel D, Raymond J, Assicot M, Moulin F, Iniguez JL, Lebon P, Bohuon C. Measurement of procalcitonin levels in children with bacterial and viral meningitis. Clin Infect Dis. 1997;24:1240–1242. doi: 10.1086/513633. [DOI] [PubMed] [Google Scholar]
- Brunkhorst FM, Eberhard OK, Brunkhorst R. Discrimination of infectious and noninfectious causes of early acute respiratory distress syndrome by procalcitonin. Crit Care Med. 1999;27:2172–2176. doi: 10.1097/00003246-199910000-00016. [DOI] [PubMed] [Google Scholar]
- Eberhard OK, Haubitz M, Brunkhorst FM, Kliem V, Koch KM, Brunkhorst R. Usefulness of procalcitonin for differentiation between activity of systemic autoimmune disease (systemic lupus erythematosus/systemic antineutrophil cytoplasmatic antibody-associated vasculitis) and invasive bacterial infection. Arthritis Rheum. 1997;40:1250–1256. doi: 10.1002/1529-0131(199707)40:7<1250::AID-ART9>3.0.CO;2-A. [DOI] [PubMed] [Google Scholar]
- Hammer S, Meisner F, Dirschedl P, Höbel G, Fraunberger P, Meiser B, Reichardt B, Hammer C. Procalcitonin: a new marker for diagnosis of acute rejection and bacterial infection in patients after heart and lung transplantation. Transpl Immunol. 1998;6:235–241. doi: 10.1016/S0966-3274(98)80013-0. [DOI] [PubMed] [Google Scholar]
- Kuse ER, Langefeld I, Jaeger K, Kulpmann WR. Procalcitonin in fever of unknown origin after liver transplantation: a variable to differentiate acute rejection from infection. Crit Care Med. 2000;28:555–559. doi: 10.1097/00003246-200002000-00044. [DOI] [PubMed] [Google Scholar]
- Oberhoffer M, Stonans I, Russwurm S, Stonane E, Vogelsang H, Junker U, Jaeger L, Reinhart K. Procalcitonin expression in human peripheral blood mononuclear cells and its modulation by lipopolysaccharides and sepsis related cytokines in vitro. J Lab Clin Med. 1999;134:49–55. doi: 10.1016/s0022-2143(99)90053-7. [DOI] [PubMed] [Google Scholar]
- Müller B, White JC, Nylen ES, Snider RH, Becker KL, Habener JF. Ubiquitous expression of the calcitonin-I gene in multiple tissues in response to sepsis. J Clin Endocrinol Metab. 2001;86:396–404. doi: 10.1210/jc.86.1.396. [DOI] [PubMed] [Google Scholar]
- Linscheid P, Seboek D, Nylen ES, Langer I, Sclatter M, Becker KL, Keller U, Muller B. In vitro and in vivo calcitonin I gene expression in parenchymal cells: a novel product of human adipose tissue. Endocrinology. 2003;144:5578–5584. doi: 10.1210/en.2003-0854. [DOI] [PubMed] [Google Scholar]
- Moreno R, Vincent JL, Matos R, Mendonca A, Centraine F, Thijs L, Takala J, Sprung C, Antonelli M, Bruining H, Willatts S. The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. Intensive Care Med. 1999;25:686–696. doi: 10.1007/s001340050931. [DOI] [PubMed] [Google Scholar]
- Mimoz O, Benoist JF, Edouard AR, Assicot M, Bohoun C, Samii K. Procalcitonin and C-reactive protein during the early posttraumatic systemic inflammatory response syndrome. Intensive Care Med. 1998;24:185–188. doi: 10.1007/s001340050543. [DOI] [PubMed] [Google Scholar]
- Brunkhorst FM, Wegscheider K, Forycki ZF, Brunkhorst R. Procalcitonin for early diagnosis and differentiation of SIRS, sepsis, severe sepsis, and septic shock. Intensive Care Med. 2000;26(Suppl):S148–S152. doi: 10.1007/s001340051134. [DOI] [PubMed] [Google Scholar]
- Benoist JF, Mimoz O, Assicot M. Procalcitonin in severe trauma. Ann Biol Clin Paris. 1998;56:571–574. [PubMed] [Google Scholar]
- Fassbender K, Pargger H, Müller W. Interleukin-6 and acute-phase protein concentrations in surgical intensive care unit patients: diagnostic signs in nosocomial infection. Crit Care Med. 1993;21:1175–1180. doi: 10.1097/00003246-199308000-00017. [DOI] [PubMed] [Google Scholar]
- Lobo SM, Lobo FR, Bota DP, Lopes-Ferreira F, Soliman HM, Melot C, Vincent JL. C-reactive protein levels correlate with mortality and organ failure in critically ill patients. Chest. 2003;123:2043–2049. doi: 10.1378/chest.123.6.2043. [DOI] [PubMed] [Google Scholar]
- Vincent JL, Mercan D. Dear Sirs, what is your PCT? Intensive Care Med. 2000;26:1170–1171. doi: 10.1007/s001340000605. [DOI] [PubMed] [Google Scholar]