

Abstract
While workplace physical exercise can help manage musculoskeletal disorders, less is known about psychosocial effects of such interventions. This aim of this study was to investigate the effect of workplace physical exercise on psychosocial factors among workers with chronic musculoskeletal pain.
The trial design was a 2-armed parallel-group randomized controlled trial with allocation concealment. A total of 66 slaughterhouse workers (51 men and 15 women, mean age 45 years [standard deviation (SD) 10]) with upper limb chronic musculoskeletal pain were randomly allocated to group-based strength training (physical exercise group) or individual ergonomic training and education (reference group) for 10 weeks. Social climate was assessed with the General Nordic Questionnaire for Psychological and Social Factors at Work, and vitality and mental health were assessed with the 36-item Short Form Health Survey. All scales were converted to 0 to 100 (higher scores are better). Between-group differences from baseline to follow-up were determined using linear mixed models adjusted for workplace, age, gender, and baseline values of the outcome.
Mean baseline scores of social climate, mental health, and vitality were 52.2 (SD 14.9), 79.5 (SD 13.7), and 53.9 (SD 19.7), respectively. Complete baseline and follow-up data were obtained from 30 and 31 from the physical exercise and reference groups, respectively. The between-group differences from baseline to follow-up between physical exercise and reference were 7.6 (95% CI 0.3 to 14.9), −2.3 (95% CI -10.3 to 5.8), and 10.1 (95% CI 0.6 to 19.5) for social climate, mental health, and vitality, respectively. For social climate and vitality, this corresponded to moderate effect sizes (Cohen d = 0.51 for both) in favor of physical exercise. There were no reported adverse events.
In conclusion, workplace physical exercise performed together with colleagues improves social climate and vitality among workers with chronic musculoskeletal pain. Mental health remained unchanged.
Keywords: biopsychosocial, mental health, musculoskeletal disorders, occupational, social capital, social climate, vitality
1. Introduction
Musculoskeletal disorders and mental health problems are the major reasons for lost productivity, sickness absence, early retirement, and years lived with disability across Europe and the United States.[1–5] While good physical and psychosocial working conditions may partly protect against development and consequences of such health problems,[6] lifestyle factors such as regular physical exercise are important as well. Indeed, a recent review provided evidence of the importance of physical exercise as therapy in 26 different chronic diseases, ranging from psychiatric diseases to musculoskeletal disorders.[7] However, because the majority of such studies are based on specific patient populations, the results may not readily transfer to working populations. Furthermore, performing physical exercise on a regular basis is a challenge for most people,[8] and less than half of adults reach the recommended amount of daily physical activity.[9]
The workplace plays a fundamental role in most adult people's life, and from a public health perspective the workplace can be considered an important setting to promote a healthier lifestyle.[10–13] In the workplace setting, physical exercise in terms of strength training together with colleagues effectively reduces musculoskeletal pain symptoms and improves physical capacity.[14–18] Furthermore, a recent review of workplace interventions for common mental disorders indicated that physical exercise may reduce depressive and anxiety symptoms among workers with such problems, although clarity lacks concerning the type, amount, and intensity of physical exercise.[19] While the majority of previous studies focused on the direct effects on the symptomology of the individual worker—for example, musculoskeletal or mental symptoms—few have evaluated more distant effects such as the impact of physical exercise on the psychosocial working environment. In a study among healthcare workers at hospitals, group-based physical exercise at the workplace improved the psychosocial working environment in terms of social capital within working teams.[20] Thus, there may be some transference effects from interventions focusing on physical components of health to improved psychosocial working environment.
This article presents unpublished data on psychosocial factors from a previously published randomized controlled trial focusing on the effect of physical exercise on musculoskeletal pain among slaughterhouse workers with chronic upper limb pain.[18] Here, we present data on changes in social climate, mental health, and vitality. The between-group differences from baseline to follow-up between the physical exercise and reference group are the main analyses in accordance with Consolidated Standards of Reporting Trials (CONSORT),[21] but the within-group changes are also included for a more complete reporting of the data.
2. Methods
2.1. Study design and randomization
The study protocol[22] and primary outcome[18] of the present trial are published elsewhere. Briefly, we performed a parallel-group, examiner-blinded, randomized controlled trial with allocation concealment among 66 slaughterhouse workers from 2 large slaughterhouses in Denmark. The study was performed between August 2012 (summer in Denmark) and January 2013 (winter in Denmark), including baseline testing, 10-week intervention activities, and follow-up testing. Baseline testing of all participants was completed before randomization. Using a computer-generated random numbers table in the SAS statistical software (SAS version 9.3 SAS Institute, Cary, NC, US), each participant was randomly allocated (stratification variables: workplace and gender) to 10 weeks of group-based physical exercise at the workplace during working hours (strength training group, n = 33) or individual ergonomic training and education (reference group, n = 33). Immediately after randomization, participants and their supervisors at each workplace were informed by e-mail about group allocation. At baseline before randomization and at 10-week follow-up, participants replied to a questionnaire concerning work, health, social climate, mental health, and vitality. Table 1 shows baseline characteristics of the 66 participants.
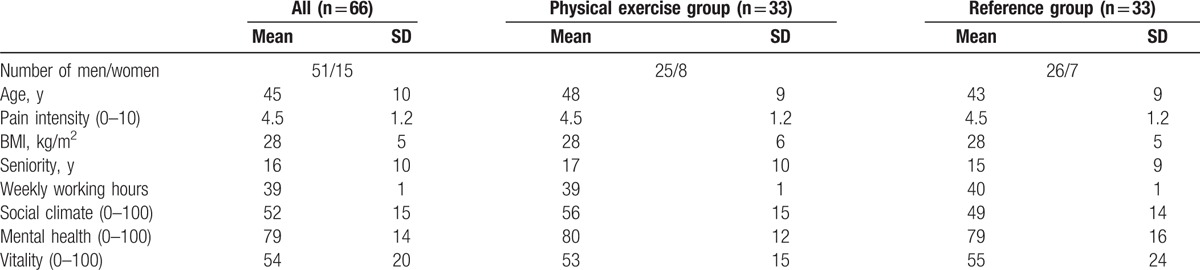
Table 1.
Demographics, work-related, and psychosocial characteristics of all randomized participants as well as for the 2 groups separately.
2.2. Participant eligibility and flow
Figure 1 shows the flow of participants through the trial. The recruitment was 2-phased. During the first phase, a screening questionnaire was administered to 645 slaughterhouse workers, of which 595 replied and 410 were interested to participate. To be eligible for the second phase of recruitment, participants had to be working at least 30 h/wk, have upper limb musculoskeletal pain of at least 3 on a scale of 0 to 10, at least some work disability, and not having participated in either strength training or ergonomics instruction during the last year. Based on these criteria, 145 participants were invited for a clinical examination, of which 135 showed up. Participants filled in the baseline questionnaire and went through an upper limb clinical examination. Of these, 69 workers were excluded due to various reasons (19—carpal tunnel syndrome, 4—hypertension, 1—serious cardiovascular disease, 19—no chronic pain, and 26—did not speak or understand Danish sufficiently to fill in the questionnaire). Thus, 66 met the final inclusion criteria of having upper chronic musculoskeletal pain of the shoulder, arm, and/or hand, which was defined as pain intensity in the shoulder, elbow/forearm, or hand/wrist of at least 3 on a 0 to 10 VAS scale during the last week; pain should have lasted more than 3 months; and frequency of pain of at least 3 d/wk during the last week. At 10-week follow-up, 3 and 2 participants of the physical exercise and reference groups, respectively, had dropped out of the study for reasons unrelated to the project.
Figure 1.
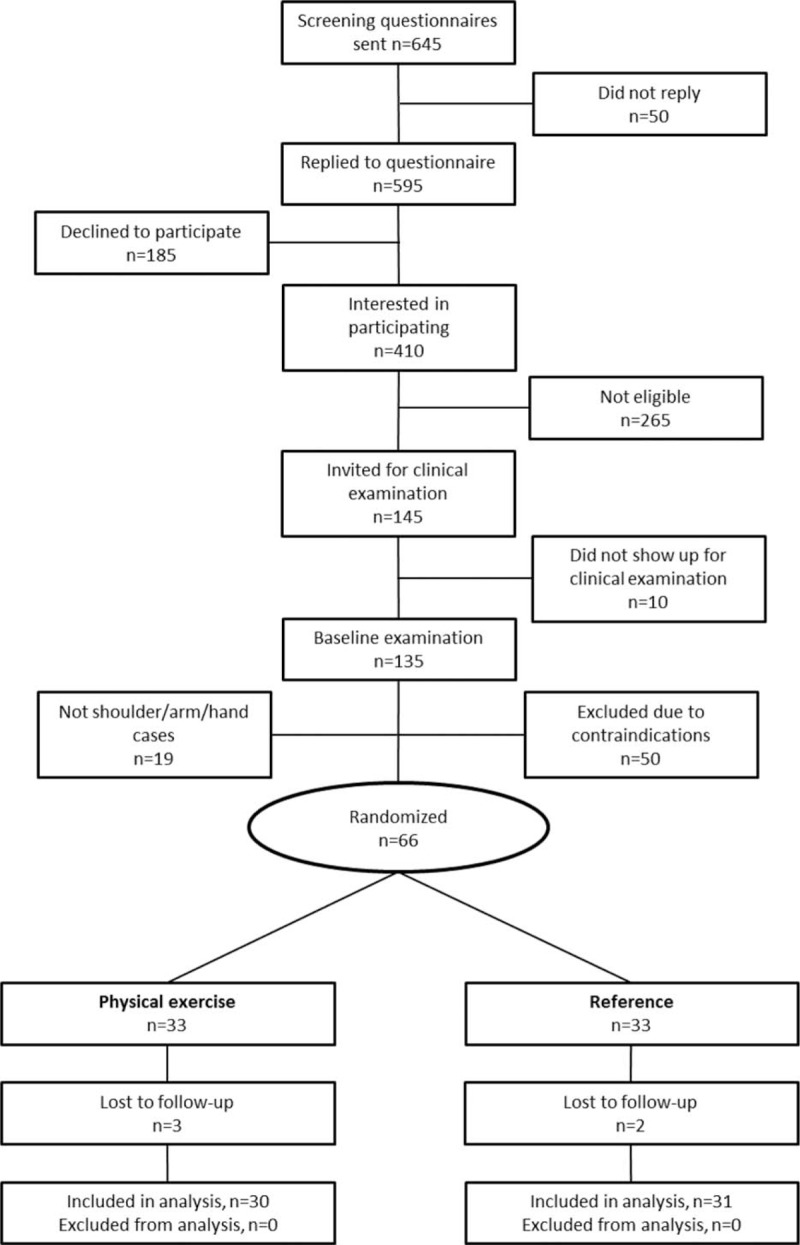
Flow of participants through the study.
2.3. Ethical approval and trial registration
The study was approved by The Danish National Ethics Committee on Biomedical Research (Ethical committee of Frederiksberg and Copenhagen; H-3-2010-062) and registered in ClinicalTrials.gov (NCT01671267) before enrollment of participants.
2.4. Data protection and accessibility
The study was notified to and registered by the Danish Data Protection Agency (journal number: 2010-54-1106) as part of the research program Implementation of Physical Exercise at the Workplace. All data will be made available through The Danish National Archives (Rigsarkivet) once all analyses of the study have been completed and published.
2.5. Interventions
The intervention activities are described in detail in an open-access article elsewhere.[22] Briefly, participants in the physical exercise group (n = 33) performed strength training at the workplace during working hours together with colleagues from the same slaughterhouse. At each slaughterhouse, the training was performed at a designated location equipped with the necessary training facilities and equipment (Sledgehammers (Hero-tools A/S, 8220 Brabrand, DK), TheraBand® elastic tubing (Performance Health, Akron, Ohio, US) elastic tubing and FlexBar® (Performance Health, Akron, Ohio, US), One Wicked Wrist Roller® (IronMind Enterprises, Inc. Nevada City, CA 95959 USA) wrist rollers, and Captains of Crush® grippers (IronMind Enterprises, Inc. Nevada City, CA 95959 USA). Eight different exercises (including shoulder rotation, ulnar and radial deviation, and flexion and extension of the hand) targeted the muscles of the shoulder, elbow/forearm, and wrist/hand. Each training session was supervised by an experienced instructor. Training load and resistance was increased throughout the intervention period according to the principle of periodization and progressive overload.[23] Starting with approximately 20 repetitions maximum during the first week, the exercise load was gradually increased, and repetitions decreased, so that 8 repetitions maximum became standard for most exercises during the last week. A total of 3 to 4 different exercises with 3 sets per exercise were performed during each training session in an alternating manner. The company allocated time during working hours for the participants to train 3 × 10 min/wk plus time for transportation to and from the training room.
Participants in the reference group (n = 33) received individualized ergonomic training and education based on a worksite analysis and a hazard prevention system, previously developed by the company. Health and safety managers and safety representatives with existing knowledge about ergonomic risk factors on the specific slaughterhouses delivered this intervention.
There were no cointerventions at the participating slaughterhouses, that is, no other intervention activities were initiated during the study period.
2.6. Outcomes
At baseline and 10-week follow-up, participants replied to a questionnaire concerning psychosocial factors. Social climate was determined using 5 questions from General Nordic Questionnaire for Psychological and Social Factors at Work,[24,25] in addition to a sixth question from another study.[26] The questions were phrased “How would you describe the social climate at your workplace….” competitive, encouraging and supportive, distrustful and suspicious, relaxed and comfortable, rigid and rule based, and conflict laden. Participants replied on a 5-point scale from “Not at all” to “To a very high degree”. Items 1, 3, 5, and 6 were reversed, and responses were converted to a score of 0 to 100. Accordingly, a higher score reflects a better social climate.
Mental health was determined using 4 questions based on the 36-item Short Form Health Survey (SF-36),[27] asking “How much of the time during the past 4 weeks....” have you been a very nervous person?, have you felt so down in the dumps that nothing could cheer you up?, have you felt calm and peaceful?, have you felt downhearted and blue?. Participants replied on a 6-point scale from “All the time” to “None of the time”, and subsequently responses were converted to a score of 0 to 100 (higher score is better).
Vitality was determined using 3 questions based on SF-36,[27] asking “How much of the time during the past 4 weeks....” did you feel full of pep?, did you have a lot of energy?, did you feel worn out?. Participants replied on a 6-point scale from “All the time” to “None of the time”, and subsequently responses were converted to a score of 0 to 100 (higher score is better).
2.7. Sample size calculation
The sample size calculation was performed before initiation of the study based on the primary outcome reported elsewhere (pain intensity of the shoulder, arm, and hand) and showed that at least 27 participants should be included in each group to achieve 95% statistical power to detect a between-group difference of 1.5 (scale 0–10) in pain intensity with a standard deviation of 1.5 and a P level of 0.05.[18] We did not perform an a priori sample size calculation for the psychosocial outcomes of this article. However, using the pooled standard deviations of the baseline to follow-up change scores of the present study, 30 participants in each group would provide a statistical power of 85%, 79%, and 57% to detect a 10 point between-group difference in social climate (ΔSD = 12.77), mental health (ΔSD = 13.85), and vitality (ΔSD = 17.69), respectively.
2.8. Statistical analyses
The changes from baseline to follow-up between the physical exercise and reference groups in social climate, mental health, and vitality, respectively, were evaluated using a linear mixed model. The change score was adjusted for the baseline value of the outcome, age, gender, and workplace. Analyses were performed using SAS statistical software (Proc Mixed, SAS version 9.3) according to the intention-to-treat principle. The estimation method was restricted maximum likelihood with degrees of freedom based on the Satterthwaite approximation. P levels of 0.05 or less were accepted as statistically significant. Outcomes are reported as within- and between-group least square mean differences with 95% confidence intervals of the change score from baseline to 10-week follow-up. The between-group differences from baseline to follow-up between the physical exercise and reference groups are the main analyses in accordance with CONSORT,[21] but the within-group changes are also included for a more complete reporting of the data.
In addition, effect sizes (Cohen d) were calculated as the between-group difference from baseline to 10-week follow-up divided by the pooled standard deviation at baseline.[28] According to Cohen, effect sizes of 0.20, 0.50, and 0.80 can be considered small, moderate, and large, respectively.
Finally, simple associations between single variables were tested by calculating Spearman rank correlation coefficient (rho).
3. Results
Table 1 shows demographics, work-related, and psychosocial characteristics of all participants and for the 2 groups separately. In spite of randomization, the physical exercise group had higher age than the reference group. Accordingly, we adjusted the statistical analyses for age.
At baseline, the mean scores of social climate, mental health, and vitality were 52.2 (SD 14.9), 79.5 (SD 13.7), 53.9 (SD 19.7), respectively, in the total study sample (n = 66). When comparing the 2 groups at baseline, the score for social climate was higher for the physical exercise than the reference group. This was adjusted for in the statistical analyses of changes from baseline to follow-up. At baseline, social climate was only weakly correlated with mental health (Spearman rho = 0.29, P < 0.05) and vitality (Spearman rho = 0.25, P < 0.05). Vitality and mental health were moderately correlated (Spearman rho = 0.59, P < 0.001).
Table 2 shows within- and between-group changes for the 2 groups from baseline to 10-week follow-up. The between-group differences for physical exercise versus reference were 7.6 (0.3 to 14.9), −2.3 (−10.3 to 5.8), and 10.1 (0.6 to 19.5) for social climate, mental health, and vitality, respectively. Thus, the change in mental health between physical exercise and reference was not significantly different. For social climate and vitality, the change between physical exercise and reference corresponded to moderate effect sizes in favor of physical exercise (Cohen d = 0.51 for both social climate and vitality).
Table 2.
Within- and between-group differences from baseline to follow-up in the strength training and reference groups. All scales are 0 to 100 (higher value is better). Values are differences of least square means and 95% confidence intervals.
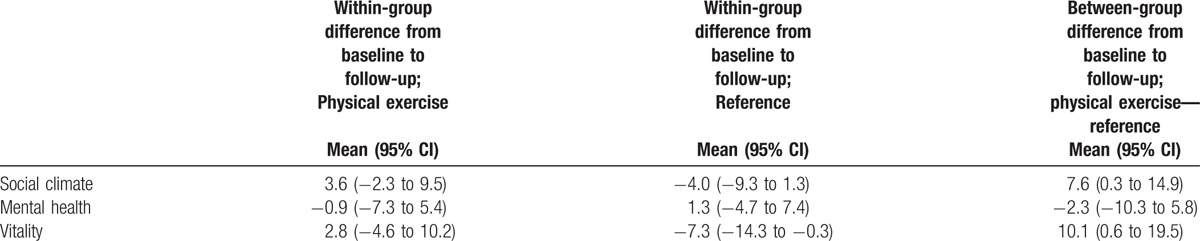
Table 3 shows that in the physical exercise group, the change from baseline to 10-week follow-up in social climate and vitality was not significantly associated (Spearman rho = 0.33, P = 0.09). However, the change in vitality was significantly associated with changes in pain intensity (Spearman r = −0.54, P < 0.01), which was not the case for social climate and pain (Spearman rho = −0.15, P = 0.43) or mental health and pain (Spearman rho = −0.03, P = 0.89).
Table 3.
Correlation matrix (Spearman rho and P values) for change scores in social climate, mental health, vitality, and pain intensity from baseline to follow-up for the physical exercise group.

There were no reported adverse events (harms) from any of the intervention activities based on feedback from the intervention providers and follow-up questionnaire to the participants.
4. Discussion
The main finding of the present study was that workplace physical exercise performed together with colleagues improves social climate and vitality with moderate effect sizes among workers with chronic musculoskeletal pain. Mental health scores did not improve with physical exercise. Thus, physical exercise performed at the workplace together with colleagues seems to have certain psychosocial benefits.
Social climate improved approximately 8 points on a scale of 0 to 100 in the physical exercise group compared with the reference group, corresponding to a moderate effect size. Interestingly, the changes in social climate occurred independently of the changes in pain intensity (rho = −0.15). Thus, contextual factors rather than the pain decrease per se may have led to improved perception of the social climate after the intervention. An obvious contextual factor is the fact that the physical exercise intervention—in contrast to the reference intervention—was performed in small groups at the workplace. This group-based approach may lead to a sense of belonging, improved solidarity, and collective self-efficacy, and thereby a more positive perception of the social climate. The present results concur with our previous finding that group-based strength training improves working relationships within teams among nurses at hospitals.[20] Thus, the process of performing meaningful intervention activities together—distinct from normal working tasks—may be the reason for the observed improvements of the psychosocial working environment.
Vitality improved approximately 10 points on a scale of 0 to 100 in the physical exercise group compared with the reference group, corresponding to a moderate effect size. Thus, physical exercise made the workers with chronic musculoskeletal pain feel more energetic and less worn out. The change was moderately related to pain reduction, which is in agreement with observational studies in patients showing that chronic pain conditions are associated with perceptions of fatigue and exertion.[29,30] In addition, the inverse relationship between the changes in pain and vitality in the present study further indicates that they share common underlying biopsychosocial mechanisms.
Mental health scores—which assessed the participant's degree of a dysphoric state of mind—did not change in this study. This may be due to a ceiling effect, that is, mental health scores at baseline were relatively high (approximately 80 on a scale of 0–100), leaving only small room for improvement. Accordingly, the present participants were not characterized of being in low spirits and dysphoric. This result contrasts with some previous studies showing a positive influence of physical exercise on mental health. However, these studies used either patients with a specific psychiatric diagnosis[7] or workers scoring relatively low on mental health at the beginning of the study.[19] Altogether, it seems plausible that physical exercise may benefit people with poor mental health, but that there is no additional benefit among otherwise mentally healthy adults who are active at the labor market.
Within-group analyses of the reference group showed a decrease of 7.3 points in vitality from baseline to follow-up. This finding should be seen in the light of the study period, that is, baseline during late summer in Denmark and follow-up during winter. Based on previous studies, vitality is known to be influenced by seasonal variations, being lower during winter than in the summer.[31] Murray et al[32] found lower mood in the winter in 10 out of 16 studies.[33] Thus, the within-group decrease of vitality in the reference group may simply be caused by seasonal variation. This can also explain the lack of significant within-group increase in vitality in the physical exercise group, that is, had they not received an intervention they would be likely to have experienced a decrease in vitality due to seasonal changes. This underscores the importance of keeping track on seasonality and using between-group differences as opposed to within-group differences as main results in randomized controlled trials.
Our study has both strengths and limitations. A strength of the present analyses is that the intervention activities did not specifically focus on psychosocial factors. Thus, placebo effects and expectation bias—which is common for perceptions of pain in interventions focusing on pain reduction[34]—is unlikely to have occurred for the present psychosocial outcomes. In addition, the parallel-group, examiner-blinded, randomized controlled trial design with allocation concealment protects against a number of biases.[21] For example, seasonal variations are known to influence perceived health and wellbeing, that is, work ability, pain symptoms, and psychosocial factors worsen during the winter.[35–39] Because the present study was carried out from summer (baseline) to winter (follow-up), a general worsening of the psychosocial factors would be expected. However, comparing the results of the physical exercise group with the reference group—that is, between-group differences from baseline to follow-up using the linear mixed model—effectively eliminates the influence of seasonal variation for the interpretation of the effectiveness of the physical exercise intervention. A limitation is that the present analyses should be considered exploratory in nature. Thus, we did not have a predefined hypothesis about physical exercise being able to improve the psychosocial factors of this study. However, this may also be considered a strength of the study because preconceived beliefs are unlikely to have influenced researchers and participants for these specific outcomes.
In conclusion, workplace physical exercise performed together with colleagues improves social climate and vitality with moderate effect sizes among workers with chronic musculoskeletal pain. Mental health scores remained unchanged.
Footnotes
Abbreviations: CONSORT = Consolidated Standards of Reporting Trials, QPS-Nordic = General Nordic Questionnaire for Psychological and Social Factors at Work, SF-36 = 36-item Short Form Health Survey.
Author contributions: LLA, RP, and ESU designed the study. ESU and MDJ collected the data. LLA analyzed the data, and all authors were involved in the data interpretation. LLA drafted the manuscript, and all coauthors revised it critically for important intellectual content. All authors have read and approved the final manuscript.
Funding/support: The study was supported by a grant from the Danish Parliament (Satspuljen 2012; Nye Veje) grant number 17.21.02.60. The funder had no influence on the study design or interpretation of results.
The authors have no conflicts of interest to disclose.
References
- [1].Andersen LL, Mortensen OS, Hansen JV, et al. A prospective cohort study on severe pain as a risk factor for long-term sickness absence in blue- and white-collar workers. Occup Environ Med 2011;68:590–2. [DOI] [PubMed] [Google Scholar]
- [2].The Work Foundation, Bevan S, Quadrello T, McGee R, et al. Fit For Work—Musculoskeletal Disorders in the European Workforce. 2009;1–143; Available from: http://www.fitforworkeurope.eu/Website-Documents/Fit%20for%20Work %20pan-European%20report.pdf [Internet]. [Google Scholar]
- [3].Durand M-J, Corbière M, Coutu M-F, et al. A review of best work-absence management and return-to-work practices for workers with musculoskeletal or common mental disorders. Work Read Mass 2014;48:579–89. [DOI] [PubMed] [Google Scholar]
- [4].Global Burden of Disease Study 2013 Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Lond Engl 2015;386:743–800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Wykes T, Haro JM, Belli SR, et al. Mental health research priorities for Europe. Lancet Psychiatry 2015;2:1036–42. [DOI] [PubMed] [Google Scholar]
- [6].van Vilsteren M, van Oostrom SH, de Vet HCW, et al. Workplace interventions to prevent work disability in workers on sick leave. Cochrane Database Syst Rev 2015;10:CD006955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Pedersen BK, Saltin B. Exercise as medicine—evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports 2015;25(suppl 3):1–72. [DOI] [PubMed] [Google Scholar]
- [8].Kohl HW, Craig CL, Lambert EV, et al. The pandemic of physical inactivity: global action for public health. Lancet Lond Engl 2012;380:294–305. [DOI] [PubMed] [Google Scholar]
- [9].WHO Global Recommendations on Physical Activity for Health. 2010;Geneva:World Health Organization, WHO Guidelines Approved by the Guidelines Review Committee; Available from: http://www.ncbi.nlm.nih.gov/books/NBK305057/. [Cited Jun 5, 2016; Internet]. [PubMed] [Google Scholar]
- [10].Guazzi M, Faggiano P, Mureddu GF, et al. Worksite health and wellness in the European union. Prog Cardiovasc Dis 2014;56:508–14. [DOI] [PubMed] [Google Scholar]
- [11].Malik SH, Blake H, Suggs LS. A systematic review of workplace health promotion interventions for increasing physical activity. Br J Health Psychol 2014;19:149–80. [DOI] [PubMed] [Google Scholar]
- [12].Rojatz D, Merchant A, Nitsch M. Factors influencing workplace health promotion intervention: a qualitative systematic review. Health Promot Int 2016;doi: 10.1093/heapro/daw015 [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- [13].Takala J, Hämäläinen P, Saarela KL, et al. Global estimates of the burden of injury and illness at work in 2012. J Occup Environ Hyg 2014;11:326–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Andersen LL, Saervoll CA, Mortensen OS, et al. Effectiveness of small daily amounts of progressive resistance training for frequent neck/shoulder pain: randomised controlled trial. Pain 2011;152:440–6. [DOI] [PubMed] [Google Scholar]
- [15].Coury HJ, Moreira RF, Dias NB. Evaluation of the effectiveness of workplace exercise in controlling neck, shoulder and low back pain: a systematic review. Rev Bras Fisioter 2009;13:461–79. [Google Scholar]
- [16].Jakobsen MD, Sundstrup E, Brandt M, et al. Effect of workplace- versus home-based physical exercise on musculoskeletal pain among healthcare workers: a cluster randomized controlled trial. Scand J Work Environ Health 2015;41:153–63. [DOI] [PubMed] [Google Scholar]
- [17].Lowe BD, Dick RB. Workplace exercise for control of occupational neck/shoulder disorders: a review of prospective studies. Environ Health Insights 2014;8(suppl 1):75–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Sundstrup E, Jakobsen MD, Andersen CH, et al. Effect of two contrasting interventions on upper limb chronic pain and disability: a randomized controlled trial. Pain Physician 2014;17:145–54. [PubMed] [Google Scholar]
- [19].Joyce S, Modini M, Christensen H, et al. Workplace interventions for common mental disorders: a systematic meta-review. Psychol Med 2016;46:683–97. [DOI] [PubMed] [Google Scholar]
- [20].Andersen LL, Poulsen OM, Sundstrup E, et al. Effect of physical exercise on workplace social capital: cluster randomized controlled trial. Scand J Public Health 2015;43:810–8. [DOI] [PubMed] [Google Scholar]
- [21].Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:c869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Sundstrup E, Jakobsen MD, Andersen CH, et al. Participatory ergonomic intervention versus strength training on chronic pain and work disability in slaughterhouse workers: study protocol for a single-blind, randomized controlled trial. BMC Musculoskelet Disord 2013;14:67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].American College of Sports, Medicine American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc 2009;41:687–708. [DOI] [PubMed] [Google Scholar]
- [24].Nordic Council of Ministers, Lindström K, Elo A, Skogstad A, et al. User's Manual for the QPS Nordic: Questionnaire on Psychological and Social Factors in the Working Life Evaluated in Denmark, Finland, Norway and Sweden—Google-søgning. 2000;Available from: https://www.google.nl/search?q=User%27s+manual+for+the+QPS+Nordic%3A+Questionnaire+on+psychological+and+social+factors+in+the+working+life+evaluated+in+Denmark%2C+Finland%2C+Norway+and+Sweden&ie=utf-8&oe=utf-8&client=firefox-b-ab&gfe_rd=cr&ei=NO9NV-eGB47u8wew27vIDw. [Cited May 31, 2016; Internet]. [Google Scholar]
- [25].Wännström I, Peterson U, Asberg M, et al. Psychometric properties of scales in the General Nordic Questionnaire for Psychological and Social Factors at Work (QPS): confirmatory factor analysis and prediction of certified long-term sickness absence. Scand J Psychol 2009;50:231–44. [DOI] [PubMed] [Google Scholar]
- [26].Persson R, Kristiansen J, Lund SP, et al. Classroom acoustics and hearing ability as determinants for perceived social climate and intentions to stay at work. Noise Health 2013;15:446–53. [DOI] [PubMed] [Google Scholar]
- [27].Bjorner JB, Thunedborg K, Kristensen TS, et al. The Danish SF-36 Health Survey: translation and preliminary validity studies. J Clin Epidemiol 1998;51:991–9. [DOI] [PubMed] [Google Scholar]
- [28].Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2ndHillsdale, N.J:Lawrence Erlbaum Associates; 1988. [Google Scholar]
- [29].Andersen LL, Nielsen PK, Søgaard K, et al. Torque-EMG-velocity relationship in female workers with chronic neck muscle pain. J Biomech 2008;41:2029–35. [DOI] [PubMed] [Google Scholar]
- [30].Pejovic S, Natelson BH, Basta M, et al. Chronic fatigue syndrome and fibromyalgia in diagnosed sleep disorders: a further test of the ‘unitary’ hypothesis. BMC Neurol 2015;15:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Partonen T, Lönnqvist J. Bright light improves vitality and alleviates distress in healthy people. J Affect Disord 2000;57:55–61. [DOI] [PubMed] [Google Scholar]
- [32].Murray G, Allen NB, Trinder J. A longitudinal investigation of seasonal variation in mood. Chronobiol Int 2001;18:875–91. [DOI] [PubMed] [Google Scholar]
- [33].Nova Science Publishers, Murray G. Seasonality, Personality and the Circadian Regulation of Mood. 2006;Available from: https://www.novapublishers.com/catalog/product_info.php?products_id=3780. [Cited Oct 23, 2016; Internet]. [Google Scholar]
- [34].Hrobjartsson A, Gotzsche PC. Placebo interventions for all clinical conditions. Cochrane Database Syst Rev 2004. CD003974.pp 1-454. [DOI] [PubMed] [Google Scholar]
- [35].Jakobsen MD, Sundstrup E, Brandt M, et al. Physical exercise at the workplace prevents deterioration of work ability among healthcare workers: cluster randomized controlled trial. BMC Public Health 2015;15:1174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Magnusson A, Boivin D. Seasonal affective disorder: an overview. Chronobiol Int 2003;20:189–207. [DOI] [PubMed] [Google Scholar]
- [37].Sundstrup E, Jakobsen MD, Brandt M, et al. Workplace strength training prevents deterioration of work ability among workers with chronic pain and work disability: a randomized controlled trial. Scand J Work Environ Health 2014;40:244–51. [DOI] [PubMed] [Google Scholar]
- [38].Takala EP, Viikari-Juntura E, Moneta GB, et al. Seasonal variation in neck and shoulder symptoms. Scand J Work Environ Health 1992;18:257–61. [DOI] [PubMed] [Google Scholar]
- [39].Persson R, Osterberg K, Garde AH, et al. Seasonal variation in self-reported arousal and subjective health complaints. Psychol Health Med 2010;15:434–44. [DOI] [PubMed] [Google Scholar]