

Abstract
The purpose of this work is to investigate the benefits of adaptive optics (AO) technology for optical coherence tomography angiography (OCTA). OCTA has shown great potential in non-invasively enhancing the contrast of vessels and small capillaries. Especially the capability of the technique to visualize capillaries with a lateral extension that is below the transverse resolution of the system opens unique opportunities in diagnosing retinal vascular diseases. However, there are some limitations of this technology such as shadowing and projection artifacts caused by overlying vasculature or the inability to determine the true extension of a vessel. Thus, the evaluation of the vascular structure and density based on OCTA alone can be misleading. In this paper we compare the performance of AO-OCT, AO-OCTA and OCTA for imaging retinal vasculature. The improved transverse resolution and the reduced depth of focus of AO-OCT and AO-OCTA greatly reduce shadowing artifacts allowing for a better differentiation and segmentation of different vasculature layers of the inner retina. The comparison is done on images recorded in healthy volunteers and in diabetic patients with distinct pathologies of the retinal microvasculature.
OCIS codes: (170.3890) Medical optics instrumentation, (170.4470) Ophthalmology, (110.1080) Active or adaptive optics, (110.4500) Optical coherence tomography
1. Introduction
Based on partial coherence interferometry [1, 2], optical coherence tomography (OCT) [3] represents a non-invasive optical imaging technique that provides cross sectional images with an axial resolution in the micrometer range. Due to its layered structure, the retina is well suited for OCT imaging which resulted in a large number of publications and various commercial products that incorporate OCT for retinal imaging [4, 5]. In order to improve the contrast between static (non-vascular) and non-static (perfused) tissue, the technique has been extended by comparing information (such as recorded B-scans) at the same tissue location that was recorded at different time points. After processing these signals, using a variety of methods, the result is a vasculature map of the retina which is comparable to state-of-the-art fluorescence angiography [6]. Thus the technique is often referred to as optical coherence angiography or optical coherence tomography angiography (OCTA) [7–10]. The method can be applied to various retinal diseases, among these frequently occurring retinal diseases such as diabetic retinopathy (DR) and the neovascular type of age-related macular degeneration (AMD). Due to its relatively simple implementation into OCT devices (only the scanning pattern and the data evaluation have to be modified) many manufactures of retinal OCT devices have updated their devices and OCTA has shown a high impact in the field of retinal imaging [11–15].
There are multiple advantages of using OCTA for assessing the vascular structure of the retina compared to other methods. OCTA relies on temporal signal changes within tissue introduced by flow which does not require any invasive administration of dyes. In contrast to OCTA, standard imaging modalities such as fluorescein angiography (FA) and indocyanine green angiography (ICGA) have to rely on those. Although the applied substances are approved for the use in humans, in some subjects these may cause allergic reactions or other side effects. Every examination with these instruments has therefore to be considered as a potential risk factor [16]. Thus, applicability of these techniques and the time intervals that can be used between examinations are limited. Due to its non-invasive nature and fast image acquisition time, 1-2 minutes as compared to 15-20 minutes in conventional angiography, OCTA allows a broader applicability to patients and imaging of the retina can be performed as frequently as needed [10]. In addition, OCTA provides both, vascular and structural information, which allows improved inspection of retinal pathologies.
Another advantage of OCTA is the ability to detect vasculature with an improved resolution and higher contrast (there is no fluorescence haze introduced by leakage) than in standard angiography methods [10]. Thus even small details like capillaries which have an extension below the transverse resolution of the system can be visualized although these appear larger than their true extension in the images [17]. Using multiphoton microscopy in comparison with OCTA these differences have been investigated in brain tissue [18].
Beside the high impact of OCTA there are also some limitations of this technique: Bulk motion between B-scans may produce line artifacts in the en-face projection images [17]. Especially when imaging patients with poor fixation capabilities these artifacts can be quite pronounced [10]. The projection effect largely depends on the time interval between B-scans. However, there is a trade-off between minimizing these artifacts (by increasing the B-scan rate) and sensitivity to slow flow speeds (which requires lower B-scan rates) that are present in capillaries.
Another issue in conventional OCTA is the limited lateral resolution of OCTA systems. Although micro-vasculature below the resolution limit can be detected, the true extension of the capillaries will be overestimated. The detected minimum size of a vessel will correspond to the transverse resolution of the system which is typically ~20 µm and much larger than the extension of small capillaries which measure ~3-6 µm in caliber. Most importantly, the occurrence of so called “projection artifacts” of anterior vessels into deeper layers often lead to misinterpretation of vascular layer localization [19]. The flow in anterior layers introduces phase and amplitude changes in the layers below which will wrongly be interpreted as true vessels in posterior layers by the angiography algorithm. These artifacts impede the differentiation between different vasculature layers and frequently only a depth integrated (over the anterior retinal layers) vessel map is produced by OCTA that shows the joint contribution of three different vascular plexus. Since a quantitative analysis of the vessel structure is very important [20], both influences need to be considered to provide measures that allow for a realistic detection of vascular structures at each layer. Furthermore, it is important to understand also the axial interconnections between the vessel beds that might be affected by pathologic changes. Intensity based extraction of angiographic details shows excellent performance for differentiating the capillaries and vessels both axially and transversally [21]. Although they profit from the strong natural contrast between blood and retinal bulk tissue, they are strongly dependent on segmentation performance [22], as well as on the achievable transverse resolution.
Adaptive optics (AO) essentially improves the transverse resolution of any optical retinal imaging method [23, 24]. The combination of AO with scanning laser ophthalmoscopy (SLO) achieved high resolution images of smallest structures of the retina such as foveal cones or rods [25–27]. However, the contrast of retinal vessels in standard confocal SLO images is rather poor. Thus additional techniques have been developed to increase the vascular contrast [28–30]. Most of these methods, such as the off-set pinhole technique, rely on the high scattering potential of vessels. Due to the high resolution of AO-SLO, the true lateral extension of small capillaries can be assessed. However, a clear differentiation between vasculature beds or measurement of the depth extension of a vessel is not possible because of the limited depth resolution in comparison with OCT. The combination of AO with OCT has convincingly shown to overcome these limitations. The high collection efficiency provided by AO-assisted systems already yield an increased contrast of vessels compared to standard OCT imaging which allows for a measurement of the three-dimensional extension of the vasculature structures [31–33].
A first proof of principle of AO-OCTA for imaging vasculature of the neurosensory retina as well as of the choroid has been presented earlier [34]. However, most of the data was recorded with a relatively small field of view (0.65° × 0.65°) and a direct comparison with commercial state of the art OCTA devices is still missing.
In this work we investigate the benefit of OCTA in combination with adaptive optics technology (AO-OCTA). The larger field of view (1.5° × 2°) and the faster imaging speed (200 kHz A-scan rate) of our previously introduced multimodal AO-OCT device [35] allow a more efficient volume stitching over a resulting field of view of 7° × 7°. AO-OCTA was applied to healthy volunteers and the improvement of image contrast was evaluated quantitatively. AO-OCTA data was compared to results from a commercial OCTA instrument and the instrument was furthermore tested in patients with diabetic retinopathy and its pathognomonic vascular pathologies.
2. Method
2.1 AO-OCT system
The AO-OCT system used in this study is a previously described prototype [35] that incorporates two imaging modalities in a compact design: AO-fundus photography and AO-OCT. In brief, AO correction is achieved with the use of a guide star, a 52 element deformable mirror (Mirao52-e RC, Imagine Eyes, Orsay, France), a Shack-Hartman (SH) wavefront sensor (Haso first, Imagine Optics, Orsay, France) and an AO loop software. The AO loop is run in closed loop mode at 15Hz. The AO-OCT system is based on a fiberized Michelson interferometer and uses a superluminescent diode with a center wavelength of 841nm and a bandwidth of ~50 nm which results in a theoretical axial resolution in the retina of ~5 µm. In order to slightly increase the power at the eye (and thus increase sensitivity) the previously used 95:5 coupler was replaced by a 90:10 coupler (Wavelength Flattened Coupler, Gould, Millersville, USA). The beam size at the sample arm entrance of the AO-OCT system is 3 mm and is increased through the imaging optics to ~5 mm at the eye. This yields a diffraction limited transverse resolution of ~4 µm in the retina and a depth of field of ~40 µm.
The optical power used for the measurements was 690 µW at 841 nm for the OCT imaging beam and 50 µW at 750 nm for the guide star. The combined light power of the OCT imaging beam and the guide star were below the limits for safe exposure according to the European standards for laser safety [36].
To achieve motion contrast we modified the scanning strategy for the fast axis scanner (x-scanner). Instead of using a triangular voltage waveform, a saw-tooth waveform was used. For the slow axis a triangular shaped stepwise waveform was used in such a way that four B-scans are acquired at the same sample location. The AO-OCT is operated with an A-scan rate of 200 kHz, which is translated into a B-scan (consisting of 310 A-scans) rate of 645 Hz. One volume acquisition takes 3.2 seconds (1.5° × 2° field of view consisting of 310 (x) times 1600 (y) pixels).
2.2 Imaging protocol and post processing
Imaging of healthy subjects and patients was performed under a protocol that was approved by the institutional ethics committee of the Medical University of Vienna and followed the tenets of the Declaration of Helsinki. Furthermore approval according to European medical device directive was granted from AGES (Austrian Agency for Health and Food Safety Ltd.). Informed consent was obtained from all subjects after explaining the form and nature of the measurements. Patients were recruited at the Department of Ophthalmology of the Medical University of Vienna. Inclusion criteria were the ability to fixate and negligible media opacities. For healthy subjects no drugs to dilate the pupil or to prevent accommodation were administered because the natural pupil size in the dark environment of the examination room was larger than 5mm. Patients were administered mydriatics to increase the pupil size. The age range of the healthy volunteers was between 23 and 44 years and between 26 and 72 years for the patients respectively.
In a measurement session four volumes per sample location were acquired. Each volume scan consisted of 400 sampling points (positions) along the slow scanning axis in which for each position 4 B-scans were recorded. Hence data sets of bad quality caused by micro-saccades or accommodation were excluded. The overall recording time per location including subject alignment was five minutes. Post processing of the data involved standard OCT data evaluation (subtraction of mean spectrum, transformation from λ- into k-space and fast fourier transformation) and OCTA evaluation. Thereby we used a method that is based on intensity differences described in detail previously [37]. Only tomograms that showed sufficiently high correlation were used to calculate the intensity differences. As such it rarely occurred that at some B-scan locations no angiographic data could be calculated. This occurred when all 4 B-scans corresponding to that location showed low correlation. In this case the B-scan was omitted. From the obtained volumes en-face projections for each vasculature layer were generated by depth integrating over en-face images that correspond to the depth extension of the corresponding vasculature layer. A maximum intensity projection was also tested for the generation of en-face images. But we did not observe any significant differences to images generated by depth integration. No layer segmentation algorithm was applied. The layers were manually segmented by drawing borders orthogonally to the A-scan direction. In case of a large inclination of the retinal layers (in respect to the horizontal plane), the B-scans were rotated in order to account for the inclination and to avoid overlapping of the vessel location extracted from the data set.
For a comparison of the results obtained with the AO-OCTA we recorded images with commercially available instruments (AngioPlex OCT Angiography, Carl Zeiss Meditec and AngioVue, Optovue). The width and position of the segmented layer that was used to generate the OCTA en-face images were manually adapted in order to best match the corresponding layers in AO-OCTA.
2.3 Evaluation of image contrast
To investigate the contrast in the AO-OCT and AO-OCTA images the Weber contrast (WC) was used as a contrast metric as proposed in [38]. The WC is defined as
| (1) |
where µs and µb are the mean intensity levels of the foreground (signal) and background (noise) region, respectively. The Weber contrast [39] is suitable as a contrast metric for images with a small target region on a large background, i.e. the mean intensity value of the image is in the range of µb, which is the case in the AO-OCT images of the vessel network. In this work, the foreground regions were found by defining the skeleton of the blood vessels using the AO-OCTA images. The vessel skeleton was determined by semi-automatically tracing of the vessels using Fiji Neurite Tracer [40] in a region-of-interest (ROI) of 165 × 165 pixels. The size of the ROI was chosen to evaluate regions with an increased presence of blood vessels. The ROI covers approximately 25% of the original image size. This procedure was performed for the different retinal plexuses. The background region was defined as the inverted skeleton and additionally excluding an area around the vessels with a distance of 7 pixels (corresponding to 10 µm) to each side of the skeleton. This area corresponds to the estimated area of the largest vessels present in the volumes. Figure 1 shows a schematic diagram on how fore- and background are determined.
Fig. 1.

Schematic diagram showing the different steps for calculating the Weber contrast value. These steps were performed for each volume and each plexus. The fore and background regions are indicated in white in the images on the right hand side.
3. Results
3.1 Healthy volunteers
Figure 2 shows representative B-scan intensity and angiography images of a healthy volunteer indicating the corresponding layers and the depth extension of each en-face projection image. Visualization 1 (7.3MB, AVI) shows a fly-through movie of the B-scans. On the left hand side the intensity image can be seen on a linear grey scale, while on the right hand side the corresponding angiography images are displayed. The shown intensity B-scans images are averaged over four images that were recorded at the same retinal location. The focus is set to the anterior layers. Due to the limited DOF the outer retinal layers appear blurred and individual photoreceptors cannot be resolved in these images.
Fig. 2.

Representative B-scan images of a healthy volunteer extracted from a volume acquired at a location vertical = 0° and nasal = 3° from the fovea. (A) Intensity image (linear grey scale), (B) AO-OCTA image (linear grey scale). Visualization 1 (7.3MB, AVI) shows a fly through of the B-scan images. The dashed lines show the corresponding borders for the en-face projection images. The different regions containing the vessel beds are indicated with the numbers 1-4. Blue: Posterior border of the topmost layer including the retinal nerve fiber layer (RNFL). Violet: Posterior border of the ganglion cell layer (anterior border is the blue line). Red: Posterior border of the inner plexiform layer. Green: Posterior border of the outer plexiform layer.
A direct comparison between en-face AO-OCTA images and intensity images is shown in Fig. 3. In this data set it is possible to distinguish and resolve the three major vascular beds (corresponding borders of the en-face projection are shown in Fig. 2.). In addition, vessels can be observed in the angiographic image of the topmost retinal layer (cf. Fig. 3(E)).
Fig. 3.

Side by side comparison between AO-OCT intensity images from different vasculature beds (top row: A, B, C, D) and the AO-OCTA images (bottom row: E, F, G, H). From left to right the corresponding depth integrated layers (cf. Fig. 2) are the nerve fiber layer, ganglion cell layer, inner plexiform layer and outer plexiform layer (the red arrow in E indicates a vessel that is not clearly visible in the corresponding intensity image. The red arrow in H indicates areas with low signal intensity, green arrow points to an artifact).
Using AO-OCT the depth of focus is limited and only part of the retina can be imaged sharply. In this data set the focus was set near the nerve fiber layer which results in a higher signal from the anterior two layers. In addition the angiography algorithm yields improved contrast enhancement in these layers. In the topmost layer, capillaries can be better visualized in the angiography image because in this layer capillaries and nerve fibers both show high signal intensity (cf. Figs. 3(A) and (E)). Thus the capillaries are not clearly seen on the intensity image (cf. Fig. 3(A)). Since the focus was set to the nerve fiber layer the signal intensity of deeper layers is reduced in these locations (cf. red arrow in Fig. 3(H)) which results in lower vessel contrast. In the intensity images of the upper layers two stripes of lower intensity can be seen (cf. green arrows in Fig. 3(A)). These are artifacts originating from accommodation (which was not paralyzed) of the subject. Within these stripes lower signal intensity in the anterior layers (cf. Figs. 3(A) and 3(B)) and higher signal intensity from the posterior layers (cf. Fig. 3(D)) can be observed.
Visually the contrast enhancement becomes evident when comparing AO-OCT intensity images and AO-OCTA images (cf. top row in Fig. 3 vs. bottom row). In order to quantify the gain of contrast, the Weber contrast metric described in section 2.3 was used. To determine the WC for the different retinal vessel layers (as shown in Fig. 2) four representative volumes recorded at different locations around the fovea region were evaluated. The mean value of WC of the four volumes is plotted as bar graphs in Fig. 4 for the AO-OCTA images (blue bar) and the AO-OCT intensity images (yellow bar) of each vessel layer (the numbering of the layers is given in Fig. 2). According to this evaluation, the WC for AO-OCTA images is more than three times higher for the ganglion cell layer when compared to the intensity images. However, the contrast enhancement through AO-OCTA is less pronounced for deeper layers.
Fig. 4.
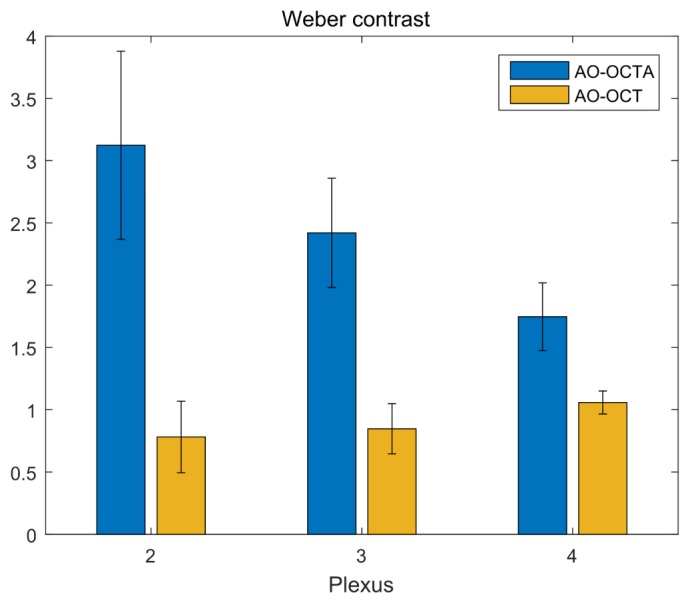
The mean Weber contrast determined for 4 volumes that were recorded at 4 different locations. Blue: WC for the angiography images. Yellow: WC for the AO-OCT intensity images. Error bars indicate the standard deviation. The x-axis indicates the number of plexus as shown in Fig. 2.
The high transverse resolution provided by AO-OCTA allows a better estimation of the true size of small capillaries. In addition the improved contrast compared with intensity based AO-OCT images and the lack of projection artifacts compared with normal OCTA images permit the visualization of interesting features as outlined in the following. Figure 5 shows six en-face projections integrated over different depths that were extracted from a single AO-OCTA volume. The AO-OCTA data set and the intensity images can be viewed in Visualization 2 (8.2MB, AVI) (left: intensity images of a linear grey scale, right: angiography images).
Fig. 5.

OCTA images retrieved from a healthy volunteer. (A) En-face projection depth integrated over the nerve fiber layer (Layer No. 1 in Fig. 2, the red arrow indicates a capillary within the nerve fiber layer, (B) En-face projection depth integrated over layer No.2 in Fig. 2, (C) En-face projection between the vessels of layer No. 2 and layer No.3 (The red circles indicate connecting vessels that are perpendicular to the vasculature beds and connect the vessel layers (B) and (D). The blue arrow points to a connecting vessel that is more inclined than the other connecting vessels, the red arrow indicates a vessel that can be seen in the B-scan image (G). (D) En-face projection over layer No. 3, (E) En-face projection between the vessels of layer No. 3 and layer No. 4 (The red circles indicate vessels that connect the central capillary plexus in (D) with the outer capillary plexus in (F), the blue arrow points to a connecting vessel with a large inclination, the yellow arrow points to a vessel that can be observed in the B-scan image displayed in (H). (F) En-face projection over layer No. 4. (G) Representative B-scan averaged over 3 frames extracted from Visualization 2 (8.2MB, AVI) at the location marked with a white line in (A) (The red arrow points to a connecting vessel that can be observed in (C). (H) Representative averaged B-scan extracted from Visualization 2 (8.2MB, AVI) at the location marked with a red line in (A) (The yellow arrow points to a vessel that can be seen in (E). The volume was recorded at a location 1.5° temporal and 3° inferior to the fovea.
The depth integration was mainly performed over areas indicated in Fig. 2. Additionally, to visualize connecting vessels, the depth integration was performed between the vessel beds excluding the information of the anterior and posterior vessels beds. The connecting vessels between vessel bed No. 2 (Fig. 5(A)) and vessel bed No. 3 (Fig. 5(D)) are shown in Fig. 5(C) and are marked with red circles. Most of the connecting vessels have an orientation that is nearly parallel to the imaging beam. Thus, these appear as small dots in the AO-OCTA images and are hardly visible. Vessels running obliquely are better visible and appear as a straight line in the en-face projection. The vessel is marked with a blue arrow in Fig. 5(C) and can be seen in the corresponding B-scan shown in Fig. 5(G) (cf. red arrow in Fig. 5(G)). Connecting vessels can also be observed between the vessel beds No. 3 and No. 4. In Fig. 5(E) these vessels are indicated with red circles. The blue arrow points to a connecting vessel that shows a large inclination to the imaging beam. The connecting vessel that is marked with a yellow arrow can also be observed in the corresponding B-scan (cf. Fig. 5(H)).
3.2 Comparison with a commercial device
In order to enable a good comparison with commercially available instruments we recorded several volumes in a healthy volunteer at different locations to enlarge the total field of view. En-face images that were generated from a selection of 25 volumes were stitched together to cover a total area of ~7° × 7° of the retina. In addition, the same subject was imaged with a commercially available instrument (AngioPlex OCT). In Figs. 6, 7 and 8 the AO-OCTA images retrieved from different depths (regions 2, 3 and 4 in Fig. 2) are shown side by side to the corresponding angiograms recorded with the commercial instrument. The depth integration was done over the same depth for the images from both instruments. The AO-OCTA image presented in Fig. 6 clearly shows the improved resolution provided by the instrument in comparison to the commercial instrument. Due to the limited transverse resolution of the commercial instrument (~20 µm), the small capillaries appear much larger (cf. Fig. 6(B)) than in the AO-OCTA image. In addition, the capillary network appears much denser in this image. This is mainly caused by influences from other vascular layers that contribute to the image. On the other hand the AO-OCTA image clearly shows a single vascular layer.
Fig. 6.

Vessel layer posterior to the nerve fiber layer (region 2 in Fig. 2). (A) AO-OCTA image consisting of 25 images that were stitched together. (B) Angiogram recorded with the commercial instrument. Field of view: ~7° × 7°. Depth integration of en-face images was identical for both images and is indicated in Fig. 2.
Fig. 7.

Vessel layer below the inner plexiform layer (region 3 in Fig. 2). (A) AO-OCTA image consisting of 25 images that were stitched together. (B) Angiogram recorded with the commercial instrument. Field of view: 7°x7°. Depth integration of en-face images was identical for both images.
Fig. 8.

Vessel layer below the outer plexiform layer (region 4 in Fig. 2). (A) AO-OCTA image consisting of 25 images that were stitched together. (B) Angiogram recorded with the commercial instrument. Field of view: 7° x 7°. Depth integration of en-face images was identical for both images.
Moving the en-face plane deeper into the retina the AO-OCTA image reveals a completely different vascular pattern (cf. Fig. 7(A)). Due to the higher numerical aperture of the system, shadowing artifacts are greatly reduced. Only shadows caused by lower signal levels below the larger vessels on the background of the AO-OCTA images can be observed. The superficial vessels do not contribute to the angiographic information of this layer. In contrast to that these artifacts are clearly present in the image retrieved with the commercial instrument (cf. Fig. 7(B)) where the large vessels from Fig. 6(B) are clearly visible.
Moving the en-face plane deeper into the retina a third vascular layer can be clearly seen in the AO-OCTA image (cf. Fig. 8(A)). This vessel pattern appears completely different compared to the previous patterns shown in Figs. 6(A) and 7(A). On the other hand, the image retrieved from the commercial instrument appears rather similar to the previous images shown in Figs. 6(B) and 7(B). Through a summation of the three vessel layers shown in Figs. 6(A), 7(A) and 8(A) a similar vessel pattern as with the commercial instrument can be obtained (cf. Fig. 9). However, because of the improved resolution provided by AO-OCTA more individual vessels can be observed. The color-coded display of the three vessel layers in Fig. 9(B) shows the complexity of the retinal vasculature and many overlapping vessels. Since the resolution of the AO-OCTA images in the 7° × 7° images is better than what can be displayed in the previous figures, we selected representative regions of interest to provide a more detailed comparison between AO-OCTA and the commercial instrument.
Fig. 9.

(A) Summation of the vessel layers shown in Figs. 6(A), 7(A), 8(A). (B) The different vessel layers shown in Figs. 6(A), 7(A) and 8(A) color coded to indicate the different depth locations acquired with AO-OCTA. Field of view: 7° × 7°.
As mentioned above, the commercial device can detect small capillaries but their apparent size is still determined by the transverse resolution of the system. Thus, vessels that are close together cannot be separated. Figures 10(A) and 10(B) show an example where a small capillary proceeds parallel to a large vessel. In the AO-OCTA image (Fig. 10(A)) both vessels can be clearly separated while in the image from the commercial angiogram (Fig. 10(B)) both vessels are merged together (cf. arrow in Fig. 10(B)). Figures 10(C) and 10(D) show a side by side comparison of a region containing an open vessel loop (cf. red arrow in both figures). In the image from the commercial instrument different closed loops can be observed that are not present in the AO-OCTA image. Figure 10(E) shows a region that contains a small vessel tree (cf. red arrow). Due to influences from other layers to the angiogram of the commercial instrument the vessel tree cannot be seen in Fig. 10(F).
Fig. 10.
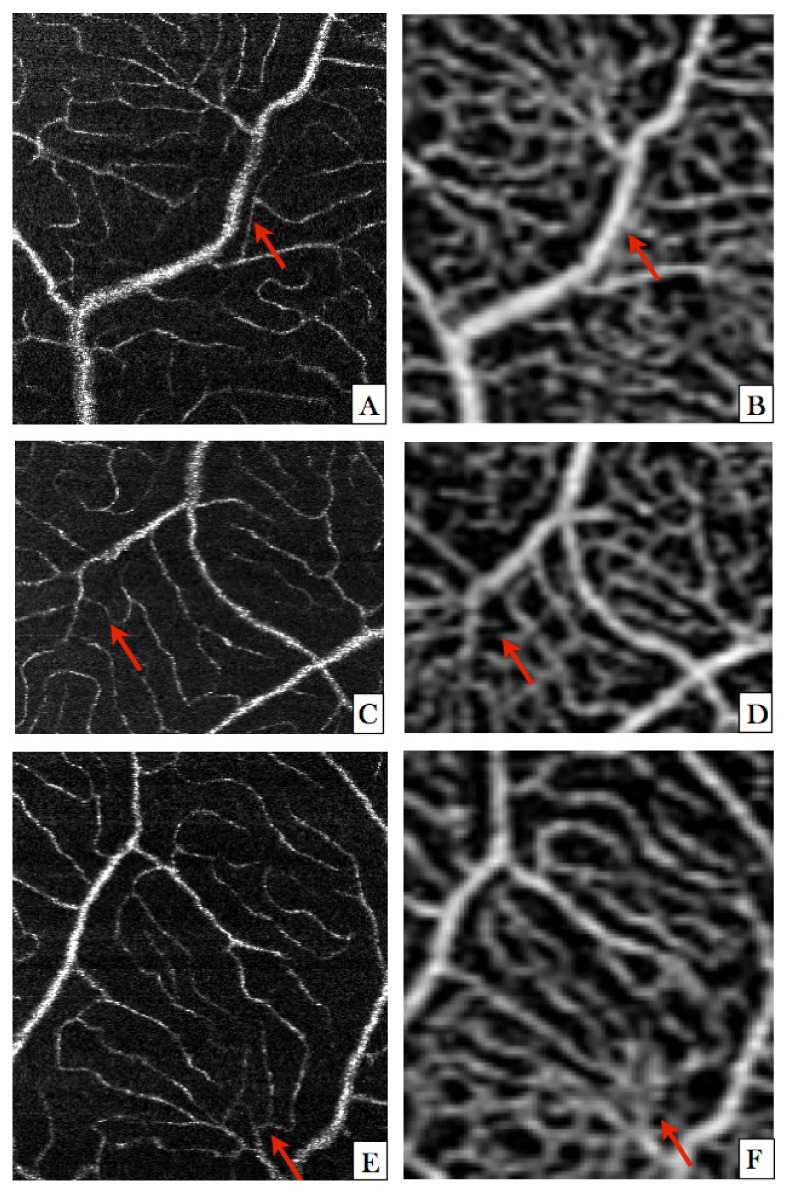
AO-OCTA images (left column) and OCTA images (right column) of selected regions of interest compared side by side. The retinal vessels are imaged in the macula region and are depth integrated over region 2 in Fig. 2. The field of view approximately corresponds to the area that can be imaged with the AO-OCTA using a single volume acquisition. (A) AO-OCTA image showing a small vessel (indicated with a red arrow) that proceeds parallel to a larger vessel. (B) The same region as in A) imaged with the commercial instrument. (C) AO-OCTA image showing a continuous vessel loop (indicated with the red arrow). (D) In this image the vessel loop (indicated with the red arrow) seems not to be connected with the main vessel on the left side. (E) AO-OCTA image showing three vessel junctions (indicated with a red arrow). (F) The same region as in E) imaged with the commercial instrument. The vessel junctions cannot be observed. Instead, closed vessel loops can be seen.
3.3 Patients with diabetic retinopathy
We additionally tested the performance of AO-OCTA in patients with diabetic retinopathy (DR). Several groups reported on early and late changes in the retinal micro-vasculature using OCTA [41–45]. Figure 11(A) shows an overview OCTA image recorded with a commercial instrument (AngioVue, Optovue; The AngioPlex OCT was not available for the patient measurements). A region of interest showing a microaneurysm is indicated with a red square. The microaneurysm is hardly detectable in the enlarged angiographic images presented in Figs. 11(B) and 11(C). For these enlarged figures different depth integrations were performed in order to better differentiate between superficial and deep vessel beds. In the OCT B-scan (Fig. 11(D)) that was recorded in the center of the region of interest, the microaneurysm is clearly visible. The AO-OCTA images provide additional information. In Fig. 11(E) an en-face projection of the angiographic data is displayed while Fig. 11(F) shows the corresponding intensity image. Both projections were performed by depth integrating over the area between the green lines in Figs. 11(G) and 11(H). Apart from the vascular plexus, microvascular changes like microaneurysm can be observed in detail (cf. red arrow in Fig. 11(F)). Perfused parts of the microaneurysm are displayed with higher contrast in the AO-OCTA image while in the AO-OCT image other (non-perfused) highly backscattering structures contribute to the image. The increased contrast provided by AO-OCTA enables the visualization of a small capillary (yellow arrow) that is not visible in the AO-OCT intensity image and the visualization of a capillary loop (blue arrow) that is otherwise obscured by surrounding backscattering tissue. The green arrow points to a hard exudate recognizable by their shape and high reflectivity which, although not perfused, is still visible in the AO-OCTA image. This is caused by the high signal intensity of this structure which shows small intensity fluctuations (introduced by residual motion between the B-scans) that are detected by the angiographic algorithm.
Fig. 11.

OCTA and AO-OCTA images of a patient with diabetic retinopathy. (A) Overview OCTA image recorded with a commercial instrument (the red square indicates the region of interest that has been imaged using AO-OCTA). (B) Enlarged region of interest (indicated by the red square in (A) depth integrated over the anterior layers (region 1 and 2 in Fig. 2). (C) The same region as in (B) but depth integrated over deeper retinal layers (region 3 and 4 in Fig. 2). (D) OCT B-scan recorded at the center of the region of interest shown in (A). (E) En-face AO-OCTA image depth integrated over the region between the green lines shown in (G). (F) En-face AO-OCT intensity image depth integrated over the same region as in (E). (G) AO-OCTA B-scan showing the microaneurysm (H) AO-OCT intensity image at same location as in (G). The red arrows in the images show the location of a microaneurysm. The green arrows point to a hard exudate. The blue arrows indicate a small capillary that appears to perform a twisted loop and is embedded in highly scattering media.
4. Discussion
The higher numerical aperture of AO-equipped instruments already yields improved contrast for retinal vessels [31–33]. This is mainly caused by increased backscattering of blood constituents compared to the surrounding tissue. Using AO-OCTA the contrast of vessels can be further increased ([34] and cf. Figs. 2 and 3) which is of specific importance for tissue regions where the surrounding tissue is also highly backscattering (as is the case for the retinal nerve fiber layer, cf. Figs. 3(A) and 3(E)) [46].
We want to summarize here several differences of our study in comparison with the previous proof of principle report of AO-OCTA [34]. First of all, the instruments used for both studies are significantly different. Our system uses light at 840nm with 200 kHz A-scan rate for imaging while the previous system imaged at 1020nm with 100 kHz A-scan rate. The current study was performed with an increased field of view (1.5° × 2°) which allows for a more efficient volume stitching (25 volumes for 7° × 7° instead of ~149 for ~5° × 5°). Due to the enhanced penetration provided by the longer imaging wavelength the previous report included the investigation of choroidal blood flow. Thus, the focus of the system was set to the photoreceptor layer. Although spherical aberration was introduced in order to increase the depth of focus, this resulted in a weak signal from the anterior layers which prevented the visualization of the full capillary network in layer 2. In contrast to that we set the focus to the anterior layers which resulted in a clear visualization of the capillary network (cf. Figs. 6–8). At the time of the initial study, commercial OCTA instruments were not yet available. Thus, to the best of our knowledge, our study is the first that allows for a direct comparison between AO-OCTA and OCTA. Finally, the initial study was limited to imaging of healthy volunteers while in this study we present first results of AO-OCTA in patients, thus demonstrating the high potential of this technology.
In comparison with standard OCTA, apart from the improved image resolution, projection artifacts are greatly suppressed using AO-OCTA (cf. Figs. 6, 7, 8). This is attributed to the tighter depth of focus that is associated with AO technology. Amplitude changes caused by overlying vessels are dispersed over a larger area and are therefore not detected by the angiography algorithm. This allows for a superior separation between the vascular beds, which signifies a clear advantage compared to standard OCTA or AO-SLO. Previous studies target a quantitative evaluation of the vessel structure or vessel tracing [20, 42]. However, using OCTA these studies are limited to the evaluation of the integrative vessel pattern consisting of several vessel beds which is not ideal. This problem can be reduced by using algorithms that remove projections artifacts [47]. A comparison with such algorithms and AO-OCTA on the retina is still missing and could be further investigated. In addition, the vessel diameter will be overestimated for all vessels that have a smaller diameter than the transverse resolution of the system. This effect will have a large influence on the vessel index parameter (ratio between vessel area and surrounding tissue). The implementation of AO-OCTA may overcome this limitation and corresponding parameter might be found with higher accuracy and for each vascular bed. The higher resolution and the angiographic data evaluation allow for the visualization of connecting vessels between the vascular beds. A similar finding has been presented previously with an OCTA prototype that showed a slightly better transverse resolution than commercially available instruments [46]. In this study we decided to use an amplitude based algorithm to generate the angiographic images. Different methods such as phase variance [7, 34], speckle variance [48], split spectrum decorrelation [49], or optical micro angiography [8] might be used as well.
One limitation of our study is that the layers for depth integration (in order to generate the en-face vasculature maps) were manually selected and that the individual retinal layers were not segmented automatically. Thus the separation between vascular layers relies on retinal layers that are nearly orthogonal to the imaging beam. This will be the case for imaging the macula area and for a centrally illuminated pupil. The curvature of the retina itself plays a minor role here because of the small field of view (1.5° × 2°). Nevertheless, segmentation of retinal layers will be essential for the generation of vessel images in pathologies where retinal layers are distorted (as the case in macula edema) or in imaging areas that are further away from the fovea. Close to the fovea the different vascular beds are in general difficult to differentiate because of their proximity. From the images presented in Figs. 6, 7, 8 it is noticeable that the foveal avascular zone has a different extension for each vascular layer in the AO-OCTA images. The topmost layer shows the smallest extension of the avascular zone. In the commercial system this could not be observed.
Another limitation of the presented AO-OCTA technique is the limited field of view that is provided by the instrument. In order to provide larger imaging regions, several volumes that are recorded at different locations have to be stitched together. Although one volume is recorded within a few seconds, the change in the retinal location is currently achieved with the use of the fixation target. This is time consuming and requires excellent compliance of the subject. A more efficient method is the employment of steering mirrors although this adds to the system complexity [50]. In addition the imaging speed of the instrument might be improved by using high speed swept laser sources [51].
An interesting aspect is the influence of the higher resolution to the scanning protocol of OCTA. There is a trade-off for all angiographic OCT methods between sensitivity to motion artifacts (which requires high B-scan rates) and sensitivity to slow motion (which requires low B-scan rates or sufficient time intervals between them). Since flow in capillaries is rather slow (ranges between 0.2 and 3.3 mm/s [52, 53]), the latter is very important to visualize these capillaries. Considering a transverse resolution of ~20 µm (as is the case in commercial systems) B-scan rates between 10 and 170 Hz are required to achieve a full speckle contrast between two alternate B-scans. The blood particle moves then 20 µm during the time period between B-scans. By increasing the resolution by a factor of 5 (as is the case in this study) the particle has to move only 4µm to generate the full speckle contrast. Thus, B-scan rates between 50 and 850 Hz (645 Hz have been used in the present study) are needed to detect flow within capillaries. Because subject motion will be more pronounced due to the higher resolution, the optimum B-scan rate (in terms of motion artifacts and sensitivity to slow speeds) needs to be much higher in high resolution OCT systems than in standard resolution systems.
5. Conclusion
In conclusion we have demonstrated AO-OCTA imaging at 840 nm in healthy volunteers and patients with DR. The improved contrast of this technique compared to intensity based AO-OCT has been shown qualitatively and quantitatively. A major advantage of this technology is the reduction of projection artifacts, which results in clear images of the different retinal vessel beds in contrast to standard OCTA. This allows a better estimation of the vessel index and an improved vessel tracing. First results in patients emphasize the potential of this technique for assessing microvascular changes in retinal disease.
Disclosures
LG, RL: Carl Zeiss Meditec (F), WD: Carl Zeiss Meditec (C), MP: Imagine Eyes (F).
Supplementary Material
Acknowledgments
The authors like to acknowledge Xavier Levecq and Franz Felberer from Imagine Eyes for their support and fruitful discussions and Carlos Reyes for his help with the measurements.
Funding
European project FAMOS (FP7 317744) and the Macular Vision Research Foundation (MVRF, USA).
References and links
- 1.Fercher A. F., Mengedoht K., Werner W., “Eye-Length Measurement by Interferometry with Partially Coherent Light,” Opt. Lett. 13(3), 186–188 (1988). 10.1364/OL.13.000186 [DOI] [PubMed] [Google Scholar]
- 2.Hitzenberger C. K., “Optical Measurement of the Axial Eye Length by Laser Doppler Interferometry,” Invest. Ophthalmol. Vis. Sci. 32(3), 616–624 (1991). [PubMed] [Google Scholar]
- 3.Huang D., Swanson E. A., Lin C. P., Schuman J. S., Stinson W. G., Chang W., Hee M. R., Flotte T., Gregory K., Puliafito C. A., Fujimoto J. G., “Optical coherence tomography,” Science 254(5035), 1178–1181 (1991). 10.1126/science.1957169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Drexler W., Fujimoto J. G., “State-of-the-art retinal optical coherence tomography,” Prog. Retin. Eye Res. 27(1), 45–88 (2008). 10.1016/j.preteyeres.2007.07.005 [DOI] [PubMed] [Google Scholar]
- 5.Wojtkowski M., Kaluzny B., Zawadzki R. J., “New directions in ophthalmic optical coherence tomography,” Optom. Vis. Sci. 89(5), 524–542 (2012). 10.1097/OPX.0b013e31824eecb2 [DOI] [PubMed] [Google Scholar]
- 6.Zhang A., Zhang Q., Chen C. L., Wang R. K. K., “Methods and algorithms for optical coherence tomography-based angiography: a review and comparison,” J. Biomed. Opt. 20(10), 100901 (2015). 10.1117/1.JBO.20.10.100901 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Makita S., Hong Y., Yamanari M., Yatagai T., Yasuno Y., “Optical coherence angiography,” Opt. Express 14(17), 7821–7840 (2006). 10.1364/OE.14.007821 [DOI] [PubMed] [Google Scholar]
- 8.An L., Wang R. K. K., “In vivo volumetric imaging of vascular perfusion within human retina and choroids with optical micro-angiography,” Opt. Express 16(15), 11438–11452 (2008). 10.1364/OE.16.011438 [DOI] [PubMed] [Google Scholar]
- 9.Wei E., Jia Y., Tan O., Potsaid B., Liu J. J., Choi W., Fujimoto J. G., Huang D., “Parafoveal retinal vascular response to pattern visual stimulation assessed with OCT angiography,” PLoS One 8(12), e81343 (2013). 10.1371/journal.pone.0081343 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Spaide R. F., Fujimoto J. G., Waheed N. K., “Image Artifacts in Optical Coherence Tomography Angiography,” Retina 35(11), 2163–2180 (2015). 10.1097/IAE.0000000000000765 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jia Y., Wei E., Wang X., Zhang X., Morrison J. C., Parikh M., Lombardi L. H., Gattey D. M., Armour R. L., Edmunds B., Kraus M. F., Fujimoto J. G., Huang D., “Optical Coherence Tomography Angiography of Optic Disc Perfusion in Glaucoma,” Ophthalmology 121(7), 1322–1332 (2014). 10.1016/j.ophtha.2014.01.021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.de Carlo T. E., Bonini Filho M. A., Chin A. T., Adhi M., Ferrara D., Baumal C. R., Witkin A. J., Reichel E., Duker J. S., Waheed N. K., “Spectral-Domain Optical Coherence Tomography Angiography of Choroidal Neovascularization,” Ophthalmology 122(6), 1228–1238 (2015). 10.1016/j.ophtha.2015.01.029 [DOI] [PubMed] [Google Scholar]
- 13.Thorell M. R., Zhang Q., Huang Y., An L., Durbin M. K., Laron M., Sharma U., Stetson P. F., Gregori G., Wang R. K., Rosenfeld P. J., “Swept-Source OCT Angiography of Macular Telangiectasia Type 2,” Ophthalmic Surg. Lasers Imaging Retina 45(5), 369–380 (2014). 10.3928/23258160-20140909-06 [DOI] [PubMed] [Google Scholar]
- 14.Keane P. A., Sim D. A., Agrawal R., Koutramanos N., Zarranz-Ventura J., Fruttiger M., Egan C. A., Tufail A., “The application of optical coherence tomography angiography in diabetic retinopathy,” Invest. Ophthalmol. Vis. Sci. 56, 5952 (2015). [Google Scholar]
- 15.Schmidt-Erfurth U., Waldstein S. M., “A paradigm shift in imaging biomarkers in neovascular age-related macular degeneration,” Prog. Retin. Eye Res. 50, 1–24 (2016). 10.1016/j.preteyeres.2015.07.007 [DOI] [PubMed] [Google Scholar]
- 16.de Carlo T. E., Romano A., Waheed N. K., Duker J. S., “A review of optical coherence tomography angiography (OCTA),” Int. J. Retina Vitreous 1(1), 5 (2015). 10.1186/s40942-015-0005-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Braaf B., Vermeer K. A., Vienola K. V., de Boer J. F., “Angiography of the retina and the choroid with phase-resolved OCT using interval-optimized backstitched B-scans,” Opt. Express 20(18), 20516–20534 (2012). 10.1364/OE.20.020516 [DOI] [PubMed] [Google Scholar]
- 18.Wang H., Baran U., Li Y., Qin W., Wang W., Zeng H., Wang R. K., “Does optical microangiography provide accurate imaging of capillary vessels?: validation using multiphoton microscopy,” J. Biomed. Opt. 19(10), 106011 (2014). 10.1117/1.JBO.19.10.106011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fabritius T., Makita S., Hong Y., Myllylä R., Yasuno Y., “Automated retinal shadow compensation of optical coherence tomography images,” J. Biomed. Opt. 14(1), 010503 (2009). 10.1117/1.3076204 [DOI] [PubMed] [Google Scholar]
- 20.Chu Z., Lin J., Gao C., Xin C., Zhang Q., Chen C. L., Roisman L., Gregori G., Rosenfeld P. J., Wang R. K., “Quantitative assessment of the retinal microvasculature using optical coherence tomography angiography,” J. Biomed. Opt. 21(6), 066008 (2016). 10.1117/1.JBO.21.6.066008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schmoll T., Singh A. S. G., Blatter C., Schriefl S., Ahlers C., Schmidt-Erfurth U., Leitgeb R. A., “Imaging of the parafoveal capillary network and its integrity analysis using fractal dimension,” Biomed. Opt. Express 2(5), 1159–1168 (2011). 10.1364/BOE.2.001159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dittrich E., Neji T., Schmoll T., Schriefl S., Ahlers C., Schmidt-Erfurth U., Leitgeb R. A., “Detection of Capillary Vessels in Optical Coherence Tomography Based on a Probabilistic Kernel,” in Proc. 13th Annual Meeting, Medical Image Understanding and Analysis, Dehmeshki J., A. H., D. G., eds. (Kingston University, 2009), pp. 37–41. [Google Scholar]
- 23.Carroll J., Kay D. B., Scoles D., Dubra A., Lombardo M., “Adaptive optics retinal imaging--clinical opportunities and challenges,” Curr. Eye Res. 38(7), 709–721 (2013). 10.3109/02713683.2013.784792 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Miller D. T., Kocaoglu O. P., Wang Q., Lee S., “Adaptive optics and the eye (super resolution OCT),” Eye (Lond.) 25(3), 321–330 (2011). 10.1038/eye.2011.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Dubra A., Sulai Y., “Reflective afocal broadband adaptive optics scanning ophthalmoscope,” Biomed. Opt. Express 2(6), 1757–1768 (2011). 10.1364/BOE.2.001757 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Dubra A., Sulai Y., Norris J. L., Cooper R. F., Dubis A. M., Williams D. R., Carroll J., “Noninvasive imaging of the human rod photoreceptor mosaic using a confocal adaptive optics scanning ophthalmoscope,” Biomed. Opt. Express 2(7), 1864–1876 (2011). 10.1364/BOE.2.001864 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Felberer F., Kroisamer J. S., Hitzenberger C. K., Pircher M., “Lens based adaptive optics scanning laser ophthalmoscope,” Opt. Express 20(16), 17297–17310 (2012). 10.1364/OE.20.017297 [DOI] [PubMed] [Google Scholar]
- 28.Tam J., Martin J. A., Roorda A., “Noninvasive Visualization And Analysis of Parafoveal Capillaries in Humans,” Invest. Ophthalmol. Vis. Sci. 51(3), 1691–1698 (2010). 10.1167/iovs.09-4483 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Chui T. Y. P., Vannasdale D. A., Burns S. A., “The use of forward scatter to improve retinal vascular imaging with an adaptive optics scanning laser ophthalmoscope,” Biomed. Opt. Express 3(10), 2537–2549 (2012). 10.1364/BOE.3.002537 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Pinhas A., Dubow M., Shah N., Chui T. Y., Scoles D., Sulai Y. N., Weitz R., Walsh J. B., Carroll J., Dubra A., Rosen R. B., “In vivo imaging of human retinal microvasculature using adaptive optics scanning light ophthalmoscope fluorescein angiography,” Biomed. Opt. Express 4(8), 1305–1317 (2013). 10.1364/BOE.4.001305 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Zawadzki R. J., Jones S. M., Olivier S. S., Zhao M., Bower B. A., Izatt J. A., Choi S., Laut S., Werner J. S., “Adaptive-optics optical coherence tomography for high-resolution and high-speed 3D retinal in vivo imaging,” Opt. Express 13(21), 8532–8546 (2005). 10.1364/OPEX.13.008532 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wang Q., Kocaoglu O. P., Cense B., Bruestle J., Jonnal R. S., Gao W., Miller D. T., “Imaging Retinal Capillaries Using Ultrahigh-Resolution Optical Coherence Tomography and Adaptive Optics,” Invest. Ophthalmol. Vis. Sci. 52(9), 6292–6299 (2011). 10.1167/iovs.10-6424 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Felberer F., Rechenmacher M., Haindl R., Baumann B., Hitzenberger C. K., Pircher M., “Imaging of retinal vasculature using adaptive optics SLO/OCT,” Biomed. Opt. Express 6(4), 1407–1418 (2015). 10.1364/BOE.6.001407 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kurokawa K., Sasaki K., Makita S., Hong Y. J., Yasuno Y., “Three-dimensional retinal and choroidal capillary imaging by power Doppler optical coherence angiography with adaptive optics,” Opt. Express 20(20), 22796–22812 (2012). 10.1364/OE.20.022796 [DOI] [PubMed] [Google Scholar]
- 35.Salas M., Drexler W., Levecq X., Lamory B., Ritter M., Prager S., Hafner J., Schmidt-Erfurth U., Pircher M., “Multi-modal adaptive optics system including fundus photography and optical coherence tomography for the clinical setting,” Biomed. Opt. Express 7(5), 1783–1796 (2016). 10.1364/BOE.7.001783 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.I. E. C. (IEC), “Safety of laser products,” in IEC 60825–1 (3rd edition 2014). [Google Scholar]
- 37.Blatter C., Klein T., Grajciar B., Schmoll T., Wieser W., Andre R., Huber R., Leitgeb R. A., “Ultrahigh-speed non-invasive widefield angiography,” J. Biomed. Opt. 17(7), 070505 (2012). 10.1117/1.JBO.17.7.070505 [DOI] [PubMed] [Google Scholar]
- 38.Lozzi A., Agrawal A., Boretsky A., Welle C. G., Hammer D. X., “Image quality metrics for optical coherence angiography,” Biomed. Opt. Express 6(7), 2435–2447 (2015). 10.1364/BOE.6.002435 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Peli E., “Contrast in complex images,” J. Opt. Soc. Am. A 7(10), 2032–2040 (1990). 10.1364/JOSAA.7.002032 [DOI] [PubMed] [Google Scholar]
- 40.Longair M. H., Baker D. A., Armstrong J. D., “Simple Neurite Tracer: open source software for reconstruction, visualization and analysis of neuronal processes,” Bioinformatics 27(17), 2453–2454 (2011). 10.1093/bioinformatics/btr390 [DOI] [PubMed] [Google Scholar]
- 41.Freiberg F. J., Pfau M., Wons J., Wirth M. A., Becker M. D., Michels S., “Optical coherence tomography angiography of the foveal avascular zone in diabetic retinopathy,” Graefes Arch. Clin. Exp. Ophthalmol. 254(6), 1051–1058 (2016). 10.1007/s00417-015-3148-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hwang T. S., Gao S. S., Liu L., Lauer A. K., Bailey S. T., Flaxel C. J., Wilson D. J., Huang D., Jia Y., “Automated quantification of capillary nonperfusion using optical coherence tomography angiography in diabetic retinopathy,” JAMA Ophthalmol. 134(4), 367–373 (2016). 10.1001/jamaophthalmol.2015.5658 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Couturier A., Mané V., Bonnin S., Erginay A., Massin P., Gaudric A., Tadayoni R., “Capillary plexus anomalies in diabetic retinopathy on optical coherence tomography angiography,” Retina 35(11), 2384–2391 (2015). 10.1097/IAE.0000000000000859 [DOI] [PubMed] [Google Scholar]
- 44.Agemy S. A., Scripsema N. K., Shah C. M., Chui T., Garcia P. M., Lee J. G., Gentile R. C., Hsiao Y. S., Zhou Q., Ko T., Rosen R. B., “Retinal vascular perfusion density mapping using optical coherence tomography angiography in normals and diabetic retinopathy patients,” Retina 35(11), 2353–2363 (2015). 10.1097/IAE.0000000000000862 [DOI] [PubMed] [Google Scholar]
- 45.Hwang T. S., Jia Y., Gao S. S., Bailey S. T., Lauer A. K., Flaxel C. J., Wilson D. J., Huang D., “Optical Coherence Tomography Angiography Features of Diabetic Retinopathy,” Retina 35(11), 2371–2376 (2015). 10.1097/IAE.0000000000000716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Gorczynska I., Migacz J. V., Zawadzki R. J., Capps A. G., Werner J. S., “Comparison of amplitude-decorrelation, speckle-variance and phase-variance OCT angiography methods for imaging the human retina and choroid,” Biomed. Opt. Express 7(3), 911–942 (2016). 10.1364/BOE.7.000911 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Zhang M., Hwang T. S., Campbell J. P., Bailey S. T., Wilson D. J., Huang D., Jia Y., “Projection-resolved optical coherence tomographic angiography,” Biomed. Opt. Express 7(3), 816–828 (2016). 10.1364/BOE.7.000816 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Mariampillai A., Standish B. A., Moriyama E. H., Khurana M., Munce N. R., Leung M. K. K., Jiang J., Cable A., Wilson B. C., Vitkin I. A., Yang V. X. D., “Speckle variance detection of microvasculature using swept-source optical coherence tomography,” Opt. Lett. 33(13), 1530–1532 (2008). 10.1364/OL.33.001530 [DOI] [PubMed] [Google Scholar]
- 49.Jia Y., Tan O., Tokayer J., Potsaid B., Wang Y., Liu J. J., Kraus M. F., Subhash H., Fujimoto J. G., Hornegger J., Huang D., “Split-spectrum amplitude-decorrelation angiography with optical coherence tomography,” Opt. Express 20(4), 4710–4725 (2012). 10.1364/OE.20.004710 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Burns S. A., Tumbar R., Elsner A. E., Ferguson D., Hammer D. X., “Large-field-of-view, modular, stabilized, adaptive-optics-based scanning laser ophthalmoscope,” J. Opt. Soc. Am. A 24(5), 1313–1326 (2007). 10.1364/JOSAA.24.001313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Klein T., Wieser W., Eigenwillig C. M., Biedermann B. R., Huber R., “Megahertz OCT for ultrawide-field retinal imaging with a 1050 nm Fourier domain mode-locked laser,” Opt. Express 19(4), 3044–3062 (2011). 10.1364/OE.19.003044 [DOI] [PubMed] [Google Scholar]
- 52.Riva C. E., Schmetterer L., “Microcirculation of the ocular fundus,” in Handbook of Physiology: Microcirculation, Tuma R.F., Duran W.N., Ley K., ed. (Elsevier, 2008). [Google Scholar]
- 53.Fallon T. J., Chowiencyzk P., Kohner E. M., “Measurement of retinal blood flow in diabetes by the blue-light entoptic phenomenon,” Br. J. Ophthalmol. 70(1), 43–46 (1986). 10.1136/bjo.70.1.43 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.