

Abstract
Introduction
Dental caries pose distinct challenges when it comes to determining their microbial etymology. Streptococcus mutans play an important role in dental caries. The aim of the present study was to compare oral microbiota in infants delivered by these different routes. A study was conducted on 40 infants. Swab sample collection was done for the detection of S. mutans. Our study indicated no differences in oral microbiota in infants due to mode of delivery.
Aim
To assess whether infants born through cesarean section delivery or infants born through normal delivery influence the initial acquisition of S. mutans in infants.
Settings and design
The study was carried out on the premises of Bharati Hospital, Pune, wherein 40 infants (3-36 months) were enrolled for the study. Two groups were designed.
Group I: Infants born with cesarean section delivery
Group II: Infants born with normal section delivery
Materials and methods
Bacterial swab sampling was done in the participants for the detection of S. mutans. Colony-forming units on each plate were determined for the estimation of S. mutans level in oral cavity.
Statistical analysis used
Bar diagram analysis and chi-square test were performed to derive p-value.
Results
The p value derived at the end of the study was 0.52. Hence, analysis of data demonstrates no significant influence of cesarean section delivery and normal delivery on oral microbiota development in infants.
Conclusion
Initial acquisition of oral S. mutans in infants is not dependent on the mode of delivery.
Key Messages
Initial acquisition of S. mutans, Mode of delivery.
How to cite this article
Ubeja RG, Bhat C. Mode of Delivery and Its Influence on the Acquisition of Streptococcus mutans in Infants. Int J Clin Pediatr Dent 2016;9(4):326-329.
Keywords: Cesarean section, Normal delivery, Oral micro-biota, Streptococcus mutans.
INTRODUCTION
During and shortly after birth, various bacterial species colonize the epithelial surfaces in the oral cavity of bac-terially naive infants.1 In vaginally delivered infants, the first exposure to microorganisms occurs during passage through the birth canal, whereas in infants born through cesarean section (henceforth referred to as C-section in the paper), the first exposure to bacteria is from the skin of parents and health providers, and medical equipment.2 Mutants Streptococci were detected more frequently and at a younger age in the oral cavity of children delivered by C-section than those delivered vaginally.1 Streptococcus mutans transmission in the oral cavity of the children is more frequent from the saliva of mother who infects the child during her care, especially if she herself does not maintain oral hygiene, lacks treatment for caries in her oral cavity, and basic hygiene rules are neglected.3
A prominent source from where bacteria might be acquired by newborn infant is the parturient canal. Vaginally delivered infants offer oral bacteria in less hospitable environment. They develop more resistance to these bacteria in their first year of life, in part because of exposure to a greater variety and intensity of bacteria from their mothers and the surrounding environment at birth. C-section babies have less bacterial exposure at birth and therefore show less resistance.4
The aim of our study is to assess whether infants born through cesarean section delivery or infants born through normal vaginal delivery influence the initial acquisition of S. mutans in infants.
MATERIALS AND METHODS
Case history sheets was taken from the participating mothers, who then signed informed consent at recruitment. The mothers completed a questionnaire on other possible confounders, such as health issues (allergy, infections, or stomach problems). Saliva was chosen as the study specimen in the predentate rather than plaque, as saliva frequently reflects the overall oral flora and serves as a reservoir for any tooth-associated species. Thus the variety of ecological sites to be indirectly assessed consequently increases with the effect of presence of teeth. The procedures followed were in accordance with the ethical guidelines laid down by the Helsinki Declaration and the Ethical Committee at Bharati Vidyapeeth Dental College and Hospital, Pune.
Forty infants (3-36 months) were enrolled for the study. Two groups were designed (Flow Chart 1)
Flow Chart 1:
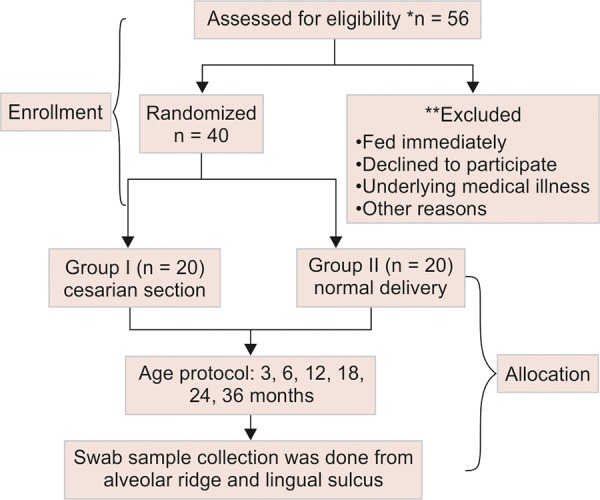
Schematic representation of the study, from infant enrollment to swab sampling
Group I: Infants born with cesarean section delivery
Group II: Infants born with normal section delivery.
Bacterial Sample Collection
Swab sampling was done in the participants for detection of S. mutans with SalivaBio Infant’s Swab (SIS),5 Biogenuix Medsystems Pvt Ltd, New Delhi, India. Sufficient saliva is usually absorbed in few minutes. All the samples were placed in the sterile plastic test tube and processed within 1 hour of the collection of sample. The swab was placed in 1 mL of 0.5 M phosphate buffer (pH: 7) solution prepared by mixing the buffer powder in distilled water and was vortexed for 1 minute. The sample was diluted in the ratio 1:10 with the phosphate buffer solution and was then vortexed. A 50-μL volume of each dilution was pipetted onto each mitis salivarius-bacitracin sucrose agar plate6-9 (Fig. 1) and evenly distributed using sterile spreaders for the cultivation of S. mutans. The plates were incubated at 37°C for 72 hours, and the number of colonies was counted based on the colony character. The colonies had crusted glass appearance and colony-forming units on each plate were numerated for the estimation of S. mutans level in the oral cavity (Fig. 2).
Fig. 1:
Mitis salivarius-bacitracin sucrose agar plate used for study
Fig. 2:
The solution pipetted onto mitis salivarius-bacitracin sucrose agar plate for further incubation and study of S. mutans colonies
RESULTS
The saliva sample was collected from infants who are 3, 6, 12, 18, 24, and 36 months and the numbers participating at different age groups was tabulated (Table 1).
Table 1: Samples of 40 infants aged 3 to 36 months, classified into two groups. Group I denotes sampling of 20 infants delivered through cesarean section. Group II denotes sampling of 20 infants delivered through normal delivery mode
| Age |
Group I (n = 20) Cesarean section delivery |
Group II (n = 20) Normal delivery |
|||
| 3 months | 3 | 1 | |||
| 6 months | 4 | 3 | |||
| 12 months | 7 | 2 | |||
| 18 months | 2 | 8 | |||
| 24 months | 0 | 4 | |||
| 36 months | 4 | 2 |
In Tables 2 and 3, the number of infants in whom S. mutans was present and absent in different mode of deliveries was tabulated. Relative occurrence of S. mutans in C-section and normal mode of delivery was derived (Graph 1). Statistical analysis in infants was done separately for C-section and normal delivery with the help of bar diagrams (Graphs 2 and 3).
Table 2: Classification of occurrence of S. mutans in infants delivered through C-section
|
C-section* delivery
-S. mutans occurrence |
|||||||
| Age | Present | Absent | Total | ||||
| 3 months | 0 | 1 | 1 | ||||
| 6 months | 1 | 2 | 3 | ||||
| 12 months | 1 | 1 | 2 | ||||
| 18 months | 3 | 5 | 8 | ||||
| 24 months | 1 | 3 | 4 | ||||
| 36 months | 2 | 0 | 2 | ||||
*C-section = Cesarean section
Table 3: Classification of occurrence of S. mutans in infants delivered through normal delivery
|
Normal delivery -S. mutans occurrence |
|||||||
| Age | Present* | Absent | Total | ||||
| 3 months | 1 | 2 | 3 | ||||
| 6 months | 2 | 2 | 4 | ||||
| 12 months | 4 | 3 | 7 | ||||
| 18 months | 2 | 0 | 2 | ||||
| 24 months | 0 | 0 | 0 | ||||
| 36 months | 1 | 3 | 4 | ||||
Graph 1:
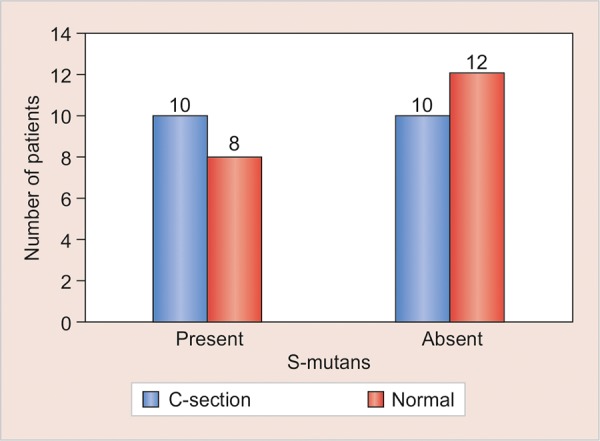
Relative occurrence of S. mutans in C-section and normal mode of delivery (C-section = Cesarean section)
Graph 2:
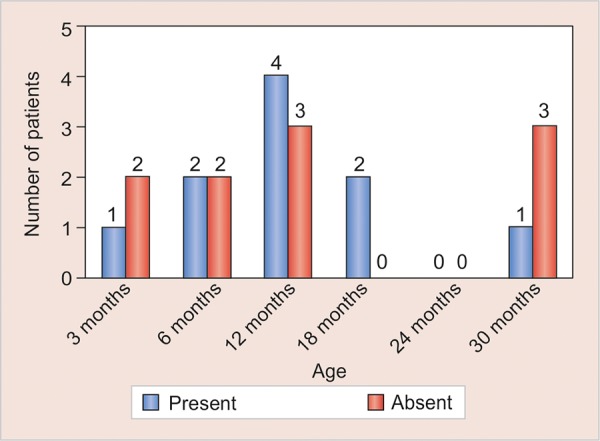
Occurrence of S. mutans in C-section delivery relative to infant age (C-section = Cesarean section)
Graph 3:
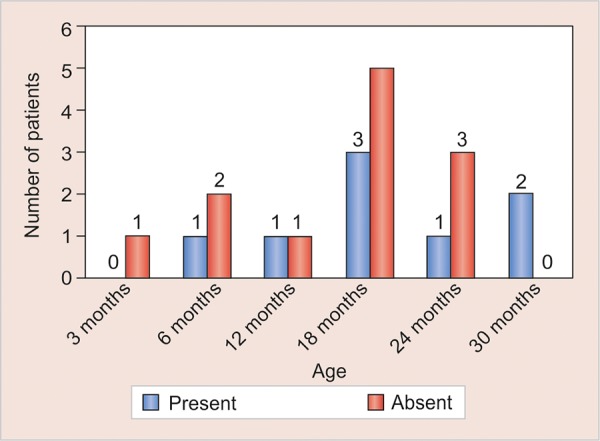
Occurrence of S. mutans in normal delivery relative to infant age
Chi-square test is used and the p value obtained is 0.52; hence the results were not statistically significant (Table 4).
Table 4: Infants with S. mutans presence and absence in normal and C-section delivery categories. The resulting p-value of the study derived is 0.52, which is statistically insignificant
| Mode of delivery | |||||||
| S. mutans | C-section* | Normal | p-value | ||||
| Present | 10 | 8 | 0.52 | ||||
| Absent | 10 | 12 | |||||
| Total | 20 | 20 | |||||
*C-section = Cesarean section
The results derived demonstrate no significant influence of cesarean section delivery and normal delivery on occurrence of S. mutans in infants.
DISCUSSION
This study emphasizes on the mode of delivery affecting establishment of S. mutans in the oral cavity of infants, which is the causative organism for the dental caries so that early intervention can be taken. The immune defense system of a newborn is reinforced by extensive exposure to maternal microorganisms through birth canal; thus, it was speculated that birth by cesarean section would have an impact on infant’s oral colonization of S. mutans.2
Saliva rather than plaque was chosen as the study specimen in the predentate as the saliva is frequently taken as reflection of overall oral flora and serve as reservoir for any tooth-associated species, thus promoting the effect of teeth, consequently increasing the variety of ecological sites to be indirectly assessed.9-12
Higher numbers of taxa were detected among infants delivered vaginally, compared with those delivered by C-section, with probes to the 16S rRNA gene of cultivated and uncultivated oral bacteria in a microarray format.7 The socioeconomic status of the family appeared to be an important factor in the early colonization of micro-organism.8 Isenberg et al reported that cesarean-born children had significantly decreased numbers of bacterial species and colony-forming units than vaginally delivered children, suggesting that by avoiding passage through birth canal, C-section infants may be less likely to be exposed to various bacterial species and strains from the mothers.13
This can be attributed to the awareness of the mothers with high socioeconomic status and education concerning feeding and oral hygiene practices of their infants.
CONCLUSION
This study supports the premise that mode of delivery does not correlate the early colonization of S. mutans in the oral cavity of infants from 3 to 36 months.
Footnotes
Source of support: Nil
Conflict of interest: None
REFERENCES
- 1.Li Y, Caufield PW, Dasanyake AP, Weiner HW, Vermund SH. Mode of delivery and other maternal factors influence the acquisition of Streptococcus mutans in infants. J Dent Res. 2005 Sep;84(9):806–811. doi: 10.1177/154405910508400905. [DOI] [PubMed] [Google Scholar]
- 2.Lif Holgerson P, Harnevik L, Hernell O, Tanner ACR, Johansson I. Mode of birth delivery affects oral microbiota in infants. J Dent Res Oct. 2011;90(10):1183–1188. doi: 10.1177/0022034511418973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Merglova V, Koberova-Ivancakova R, Broukal Z, Dort J. The presence of cariogenic and periodontal pathogens in the oral cavity of one-year-old infants delivered pre-term with very low birthweights: a case control study. BMC Oral Health. 2014 Sep 1;14:109. doi: 10.1186/1472-6831-14-109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Torrey JC, Reese K. Initial aerobic flora of newborn infants. Am J Dis Child. 1945 Apr;69(4):208–214. [Google Scholar]
- 5.Slowey PD. Commercial saliva collecting tools. J Calif Dent Assoc. 2013 Feb;41(2):97–99, 102-105. [PubMed] [Google Scholar]
- 6.Loesche WJ. Role of Streptococcus mutans in human dental decay. Microbiol Rev. 1986 Dec;50(4):353–380. doi: 10.1128/mr.50.4.353-380.1986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Berkowitz RJ, Jordan HV, White G. The early establishment of Streptococcus mutans in the mouth of infants. Arch Oral Biol. 1975 Mar;20(3):171–174. doi: 10.1016/0003-9969(75)90005-9. [DOI] [PubMed] [Google Scholar]
- 8.Paster BJ, Dewhirst FE. Molecular microbial diagnosis. Periodontology 2000. 2009;51:38–44. doi: 10.1111/j.1600-0757.2009.00316.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tanzer JM, Livingston J, Thompson AM. The microbiology of primary dental caries in humans. J Dent Educ. 2001 Oct;65(10):1028–1037. [PubMed] [Google Scholar]
- 10.Mattos-Graner RO, Corrêa MSNP, do Rosa’rioe O, Latorre M, Peres RCR, Mayer MPA. Mutans streptococci oral colonization in 12-30 month-old Brazilian children over a one year follow-up period. J Public Health Dent. 2001 Summer;61(3):161–167. doi: 10.1111/j.1752-7325.2001.tb03384.x. [DOI] [PubMed] [Google Scholar]
- 11.Vachirarojpisan T, Shinada K, Kawaguchi Y, Laungwechakan P, Somkote P, Detsomboonrat P. Early childhood caries in children aged 6-19 months. Community Dent Oral Epidemiol. 2004 Apr;32(2):133–142. doi: 10.1111/j.0301-5661.2004.00145.x. [DOI] [PubMed] [Google Scholar]
- 12.Karn TA, O’Sullivan DM, Tinanoff N. Colonization of mutans streptococci in 8 to 15 month old children. J Public Health Dent. 1998 Summer;58(3):248–249. doi: 10.1111/j.1752-7325.1998.tb03001.x. [DOI] [PubMed] [Google Scholar]
- 13.Isenberg SJ, Apt L, Yoshimori R, McCarty JW, Alvarez SR. Source of the conjunctivital bacterial flora at birth and implications for opthalmia neonaturum prophylaxis. Am J Ophthalmol. 1988 Oct 15;106(4):458–462. doi: 10.1016/0002-9394(88)90883-5. [DOI] [PubMed] [Google Scholar]