

Abstract
Background:
We have reported that handheld confocal laser endomicroscopy (CLE) can be used with various nonspecific fluorescent dyes to improve the microscopic identification of brain tumor and its boundaries. Here, we show that CLE can be used experimentally with tumor-specific fluorescent labeling to define glioma margins in vivo.
Methods:
Thirteen rats underwent craniectomy and in vivo imaging 21 days after implantation with green fluorescent protein (GFP)-labeled U251 (n = 7) cells or epidermal growth factor receptor (EGFR) overexpressing F98 cells (n = 6). Fluorescein isothiocyanate (FITC) conjugated EGFR fluorescent antibody (FITC-EGFR) was applied for contrast in F98 tumors. Confocal images of normal brain, obvious tumor, and peritumoral zones were collected using the CLE system. Bench-top confocal microscopy and hematoxylin and eosin-stained sections were correlated with CLE images.
Results:
GFP and FITC-EGFR fluorescence of glioma cells were detected by in vivo visible-wavelength fluorescence CLE. CLE of GFP-labeled tumors revealed bright individual satellite tumor cells within peritumoral tissue, a definitive tumor border, and subcellular structures. Imaging with FITC-EGFR labeling provided weaker contrast in F98-EGFR tumors but was able to delineate tumor cells. Imaging with both methods in various tumor regions correlated with standard confocal imaging and clinical histology.
Conclusions:
These data suggest that in vivo CLE of selectively tagged neoplasms could allow specific interactive identification of tumoral areas. Imaging of GFP and FITC-EGFR provides real-time histologic information precisely related to the site of microscopic imaging of tumor.
Keywords: Confocal laser endomicroscopy, confocal microscopy, green fluorescent protein, fluorescent antibody, malignant gliomas, molecular imaging
INTRODUCTION
Gliomas are diffusively growing malignant primary tumors of the central nervous system. The penetrating nature of gliomas means that total resection is an illusory goal. Tumor cells invade surrounding tissue, and thus, by definition, are not resected. Remaining cells act as protagonists for what is interpreted eventually on imaging as tumor recurrence. Historically and practically, the ability to detect the tumor margin for surgery has been limited by the inability to identify the margin on a cellular basis in vivo. Nevertheless, data from various investigations have highlighted the importance of the extent of resection and its influence on patient survival.[1,5,11,20,23,33]
Consequently, techniques that would allow surgeons to intraoperatively delineate a microscopic in vivo margin and to identify tumor beyond the resection cavity would be a significant advance. 5-aminolevulinic acid (5-ALA) is a photosensitizer precursor that is converted into protoporphyrin IX (PPIX), an actual photosensitizer that is part of the endogenous heme cycle.[22] 5-ALA-based fluorescence appears useful for the macroscopic detection of the general region of a glioma, although there is limited information on microscopic imaging of such regions during human surgery.[25,30] 5-ALA-based fluorescence has a higher sensitivity to tumor regions compared to magnetic resonance imaging (MRI).[27] In addition, 5-ALA-based fluorescence is highly selective, even though it may also be taken up by normal or reactive cells at the tumor-brain boundary.[2]
Fluorescence imaging techniques have improved in vivo real-time identification of the infiltrating edge of tumors as well as assessment of their histologic features. Confocal laser endomicroscopy (CLE) yields fluorescence-based images of brain tissue in vivo with cellular resolution (“optical biopsies”). The feasibility of handheld CLE in a murine malignant glioma model to distinguish between normal brain, microvasculature, and tumor margins has been evaluated.[12,14,26,34] Furthermore, clinical trials to assess the feasibility of CLE for human brain tumor applications have been completed.[3,4,7,13,16,18,24]
CLE allows investigators to evaluate cytoarchitectural information from several topical or systemically delivered fluorophores in experimental and human brain tumors: Fluorescein sodium, acridine orange, acriflavine, cresyl violet, 5-ALA, and indocyanine green.[12,14,25] These fluorophores, however, stain not only tumor cells but also adjacent structures. It is challenging to distinguish cell subtypes, i.e., reactive astrocytes vs. glioma. Thus, the development of tumor-specific fluorophores could yield a powerful technique that improves the differentiation of brain tumor cells. Here, we report the utility of CLE to define tumor margins in vivo after malignant glioma cells were selectively labeled with green fluorescent protein (GFP) or a fluorescein isothiocyanate (FITC) conjugated epidermal growth factor receptor (EGFR) fluorescent antibody (FITC-EGFR). We compared this labeling technique to standard benchtop system confocal and hematoxylin and eosin (H and E) histologic preparations and the use of in vivo CLE with nonspecific fluorescent stain labeling.
MATERIALS AND METHODS
Animals
Thirteen male Crl:NIH-Foxn1rnu rats (5 weeks old) were obtained from Charles River Laboratories International, Inc. (Wilmington, Massachusetts, USA). Experiments were performed in accordance with the guidelines and regulations set forth by the National Institutes of Health's Guide for the Care and Use of Laboratory Animals and were approved by the Institutional Animal Care and Use Committee of Barrow Neurological Institute and St. Joseph's Hospital and Medical Center, Phoenix, Arizona.
Brain tumor models
Green fluorescent protein tumor model
To generate constitutively fluorescent glioma cells, GFP was cloned into mammalian retroviral expression vector pLXSN (Clonetech, Mountain View, California, USA). Virus was generated using GFP cDNA cloned in pLXSN and packaged using Phoenix A cells. U251 human glioma cells (American Type Culture Collection, Manassas, Virginia, USA) were infected with the virus and selected for GFP expression by fluorescence-activated cell sorting.
Epidermal growth factor receptor tumor model
In human gliomas, EGFR is commonly overexpressed.[9] We generated rodent tumors that overexpressed the human form of this protein to test the feasibility of fluorescently labeling EGFR in vivo. Rodent allografts were produced by implanting F98 glioma cells infected to constitutively overexpress human EGFR (American Type Culture Collection, Manassas, Virginia, USA).
Intracranial implantation
Each rat was anesthetized by intraperitoneal injection of a mixture of xylazine (80 mg/kg) and ketamine (10 mg/kg) and affixed in a stereotactic headframe (Model 900, David Kopf Instruments, Tujunga, California, USA). A 20-mm incision was made in the skin overlying the skull, exposing the coronal suture and bregma. A bur hole was made 3.5 mm to the right of bregma. The tumor cells were infused at a depth of 4.5 mm below the surface of the brain after the syringe (World Precision Instruments, Sarasota, Florida, USA) was advanced 5 mm to create a 0.5-mm pocket. The cell suspension was infused over 3 minutes using a UMP3-1 UltraMicroPump microinjector (World Precision Instruments, Sarasota, Florida, USA) set to a volume of 10 μL with an infusion rate of 3.33 μL/minute. The needle was withdrawn 2 minutes after the injection to minimize the backflow of the cell suspension. Bone wax was used to cover the bur hole. The skin incision was closed with interrupted sutures.
Animal surgery
Twenty-one days after xenograft implantation, the rats underwent a craniectomy and durotomy to expose the surfaces of both cerebral hemispheres and for intraoperative imaging. Animals underwent appropriate general anesthesia, as described earlier, and oxygen supply and body temperature were maintained throughout the procedure. Intraparenchymal brain tumors were macroscopically identified in the right hemisphere of all rats designated for main experiments. Saline irrigation provided successful hemostasis throughout the procedure. After imaging was performed, anesthetized animals were euthanized following institutional guidelines.
In vivo confocal laser endomicroscopy
In vivo CLE was performed using the Optiscan 5.1 system. This system contains a handheld miniaturized scanner designed as a rigid probe with a 6.3-mm outer diameter, providing a working length of 150 mm (Optiscan Pty. Ltd., Victoria, Australia and Zeiss Meditec AG, Jena, Germany). A 488-nm diode laser provided incident excitation light, and fluorescent emission was detected at 505-585 nm using a band-pass filter, both via a single optical fiber acting as the excitation and detection pinholes for confocal isolation of the focal plane. The detector signal was digitized synchronously with the scanning to construct images parallel to the tissue surface (en face optical sections). Laser power was typically set to 550–900 μW for brain tissue; maximum power was limited to 1000 μW. A field of view of 475 × 475 μm (approximately 1000 × magnification on a 21-inch screen) was scanned either at 1024 × 512 pixels (0.8/s frame rate) or at 1024 × 1024 pixels (at 1.2/s frame rate) with a lateral resolution of 0.7 μm and an axial resolution (i.e., effective optical slice thickness) of approximately 4.5 μm. The resulting images were stored digitally and could be recorded as time-lapse series. During the procedure, a foot pedal provided remote control of the variable confocal imaging plane depth from the surface to a depth of 0 to 500 μm.
The confocal probe affixed to a retractor system was moved gently along the surface of the brain tissue to obtain images from several regions of interest (ROIs). ROIs included normal brain, regions of obvious tumor, and the transitional zone between what appeared to be the normal brain and tumor. The probe was moved smoothly between different ROIs without losing contact with the tissue. Images were acquired by optical sectioning of the tissue from each ROI at the brain surface and from deeper structures. Unique aspects of individual cells and surrounding neoplastic tissue were seen as the endomicroscopic probe acquired images throughout its focal depth range. The total imaging time was approximately 20 minutes per rat.
In vivo fluorescent antibody labeling
Tumor cells were labeled in vivo with a fluorescently conjugated antibody. FITC was conjugated to EGFR antibody to provide an excitation-emission spectrum similar to GFP (Abcam, Cambridge, Massachusetts, USA). The fluorescently conjugated antibody was infused into the tumor region 24 hours prior to imaging. Intraoperative imaging with CLE was performed on the fluorescently labeled EGFR-overexpressing tumors. Frank tumor regions, tumor margins, and contralateral brain were examined for the appearance of fluorescently labeled cells.
Tissue sampling, histology, and data processing
Multiple cold-cut biopsies were harvested from each rat. Brain tissue slices (0.5 cm2) containing several ROIs were cut parallel to the surface. After the in vivo imaging, tissue was imaged ex vivo with a Zeiss 710 inverted laser scanning confocal microscope. For comparison to the CLE, we equipped the Zeiss 710 with a Plan Apochromat 20 × 0.8 NA objective, and set the confocal aperture for 1 Airy unit. Areas imaged using the confocal microscope and CLE were marked with tissue ink so that locations could be precisely correlated and validated with conventional histology. The tissue was placed in a cassette for standard formalin fixation and paraffin embedding. Histologic assessment was performed using standard light microscopic evaluation of 5- μm thick H and E–stained sections with an Olympus BX60 upright microscope. Careful labeling and grouping of acquired confocal images and specific biopsy samples ensured correct correlation.
4’,6-diamidino-2-phenylindole staining for green fluorescent protein-labeled tumors
One biopsy from each animal with GFP-labeled tumors was fluorescently labeled with 4’,6-diamidino-2-phenylindole (DAPI; Invitrogen, Carlsbad, California, USA) to specifically label all cell nuclei. We identified GFP-labeled tumor cells by excitation with a 488-nm diode laser and collecting 505–525-nm emissions. We identified DAPI-labeled nuclei by 405-nm diode laser excitation and 415–465-nm emission. DAPI-labeled nuclei of tumor and nontumor areas were counted. Two-tailed Student's t-tests were used to compare nuclei counts from tumor and nontumor areas. The significance level was set at P < 0.05.
RESULTS
Confocal laser endomicroscopy imaging of green fluorescent protein-labeled cells
Intraoperative CLE of GFP-labeled cells allowed selective identification of the tumor margin while providing striking optically identifiable cellular and subcellular structures within the tumor cells, which correlated with confocal and conventional histology and with known tumor tissue architecture. Within obvious neoplastic tissue, imaging of cellular GFP produced images morphologically consistent with cytoplasmic labeling of tumor cells. These features included hypercellularity, pleomorphism, atypia, and possible mitoses [Figures 1 and 2]. Other regions presented a complex mixture of these patterns. Mostly nonfluorescent normal-appearing brain was punctuated by large pleomorphic cells consistent with an infiltrative margin. Satellite tumor cell clusters were surrounded by brain tissue [Figures 1–3]. Critically, individual tumor cells within brain tissue could be identified within the 475 × 475- μm field of view, and a definitive tumor border and/or invading cells could be identified. Confocal endomicroscopy of normal-appearing brain distant from the tumor revealed tissue that did not fluoresce with indistinguishable histologic features [Figures 1 and 3]. Blood artifacts were not detected.
Figure 1.
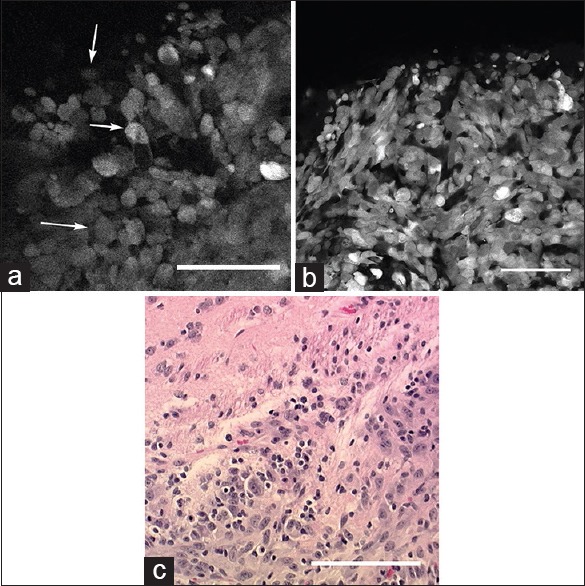
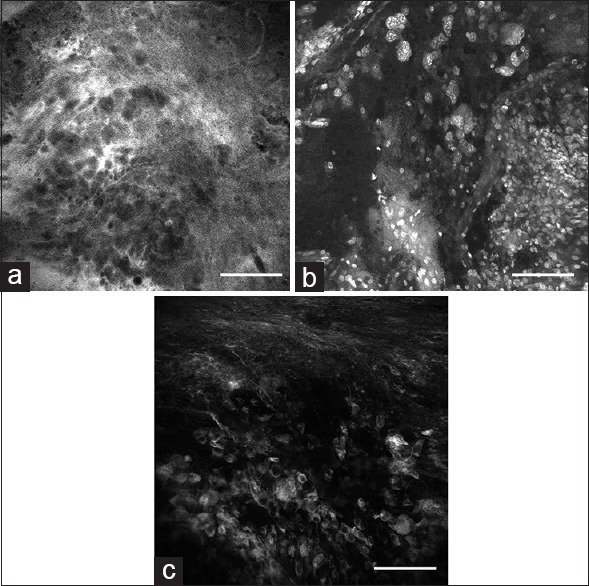
(a) In vivo image of the tumor border obtained with the confocal endomicroscope demonstrates intracellular distribution of green fluorescent protein. Atypical cells (arrows) consistent with tumor cells are identified within regions of cellular tumor and infiltrating edge. (b) Ex vivo bench-top confocal and (c) Hematoxylin and eosin (×20) images from the same region of interest demonstrate atypical cells within the tumor and tumor edge, similar to the in vivo image. Scale bar 100 μm. Used with permission from Barrow Neurological Institute, Phoenix, Arizona
Figure 2.
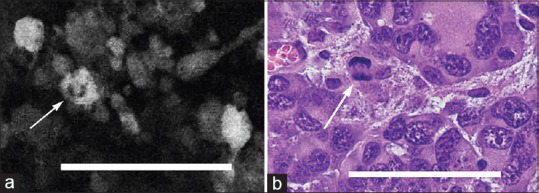
(a) In vivo image obtained with the confocal endomicroscope using green fluorescent protein reveals a possible mitotic figure in a tumor cell (arrow). (b) Hematoxylin and eosin-stained section (×40) from the same region of interest shows a similar mitotic figure (arrow). Scale bar 100 μm. Used with permission from Barrow Neurological Institute, Phoenix, Arizona
Figure 3.
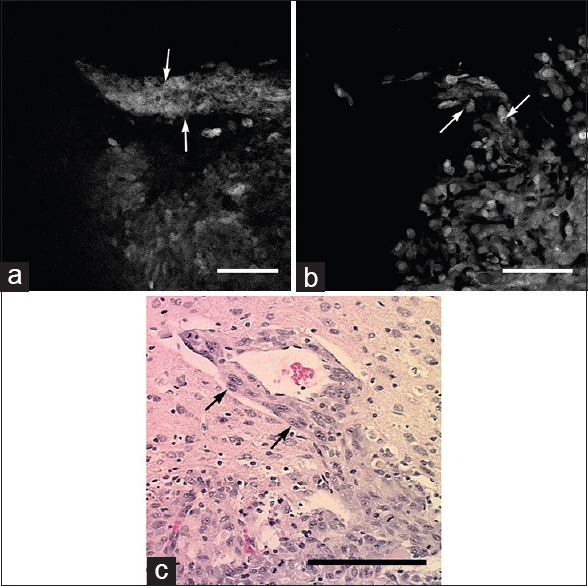
Images obtained from tumor border. (a) In vivo confocal endomicroscope image demonstrates tumor cells aligned along a blood vessel progressing out from the main tumor mass (arrows). (b) Ex vivo bench-top confocal and (c) Hematoxylin and eosin section (×20) from the same region of interest show similar histologic features (arrows). Scale bar 100 μm. Used with permission from Barrow Neurological Institute, Phoenix, Arizona
Evaluation of DAPI-stained specimens with conventional confocal microscope showed hypercellular tissue corresponding to tumor areas on H and E staining. These regions also showed intensive green fluorescence. Areas containing significantly fewer DAPI-stained nuclei appeared to be normal brain tissue with H and E staining and lacked green fluorescence when imaged in the same optical plane [Figures 4 and 5].
Figure 4.
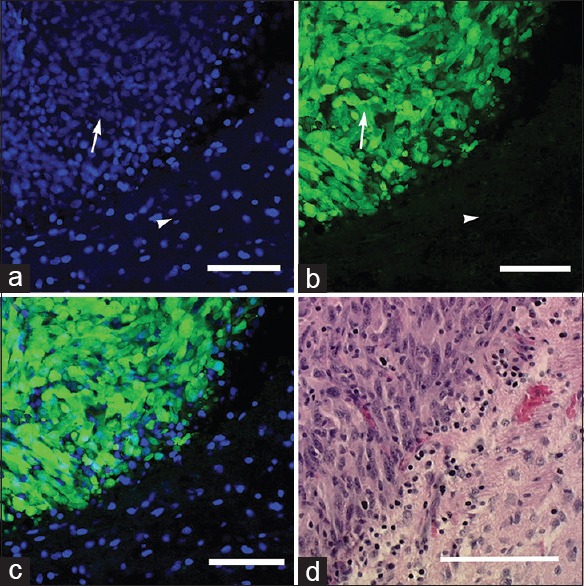
Ex vivo images obtained with the bench-top confocal microscope: (a) 4’,6-diamidino-2-phenylindole (DAPI) staining shows areas of hypercellular tumor (arrow) and normal adjacent brain tissue (arrowhead); (b) green fluorescent protein-labeled tumor cells (arrow) and nonfluorescent normal brain tissue (arrowhead); and (c) merged DAPI-GFP image. (d) Hematoxylin and eosin section (×20) from the same region of interest shows similar histologic characteristics. Scale bar 100 μm. Used with permission from Barrow Neurological Institute, Phoenix, Arizona
Figure 5.
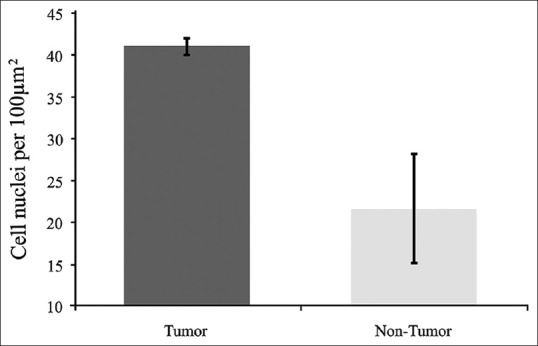
Comparison of cell nuclei (4’,6-diamidino-2-phenylindole staining) counts of tumor and nontumor areas. Tumor cell nuclei count 53 in 10 slides. Non-tumor cell nuclei count 21 in 3 slides. Error bars are ± 1 SD. (Comparison by t-test, P < 0.05, indicating statistically significant difference). Used with permission from Barrow Neurological Institute, Phoenix, Arizona
Confocal laser endomicroscopy imaging of fluorescein isothiocyanate fluorescent antibody-labeled cells
CLE images were clear enough to reveal cellular and subcellular detail of FITC conjugated antibody selectively labeled tumor cells in vivo [Figure 6]. CLE revealed strong fluorescent delineation of tumors cells within the same tumor regions [Figure 6] and images provided similar information compared with ex vivo imaging using the benchtop confocal microscope. The normal brain contained numerous unlabeled cells. Minimal fluorescence from the surface of tumor-free brain suggests that washing removed unbound elements of the fluorescent antibody [Figure 7]. We detected fluorescence from perivascular cells in deep tumor regions and within vasculature from normal brain. This finding suggests the infused fluorescent antibody entered the blood stream and general circulation. Typical H and E staining patterns of hypercellularity and pleomorphism were evident in the examined tissue from the same microregion as labeled and imaged fluorescently. This finding suggests in vivo fluorescent antibody staining did not interfere with traditional histologic processing of brain tissue.
Figure 6.

Fluorescein isothiocyanate conjugated epidermal growth factor receptor antibody labels tumor cells in the tumor core and margin. (a and d) In vivo images acquired with Optiscan 5.1. (b and e) Corresponding ex vivo images collected with Zeiss benchtop confocal microscope. Note similar fluorescent regions and image quality. (c and f) Corresponding Hematoxylin and eosin images. Scale bar equals 20 μm. Used with permission from Barrow Neurological Institute, Phoenix, Arizona
Figure 7.

Seven-fold greater laser power required to visualize autofluorescence from tumor-free brain regions. Note corresponding fluorescent artifact between images (arrowhead) and non-labeled cell bodies (arrows). Image (a) taken with confocal endomicroscope, image (b) taken with bench-top Zeis 710 confocal microscope (higher laser power), and image (c) is the corresponding Hematoxylin and eosin image. Scale bar equals 20 μm. Used with permission from Barrow Neurological Institute, Phoenix, Arizona
DISCUSSION
This study represents a definitive in vivo application of visible-wavelength fluorescence CLE for imaging specific molecular fluorescent labeling of an infiltrative human glioma cell line and a rodent glioma cell line using EGFR as a detected marker of importance to human malignant glioma. The fluorescence corresponded to tumor cells, which made their identification precise and not confounded by fluorescent signal from the background and adjacent structures.
A previous pilot study in a murine glioma cell line allowed CLE detection of second tyrosinase-related protein (TRP-2), a bound protein overexpressed in GL261 mouse glioma cells.[6] In that study, the tumor was not stained homogeneously, which precluded the clear visualization of the tumor-brain interface. In the present study, CLE of GFP and FITC-EGFR labeling was very clear, nearly homogenous, and enabled us to easily identify the same microtumor regions comparable to bench-top confocal and H and E histologic methods. The results suggest that in vivo CLE combined with a tumor-specific fluorescent molecular labeling is a viable method to detect tumor cells intraoperatively. However, this detection technique requires that the labeling fluorophores strictly match the detection system's operating parameters.
Although the CLE 475 × 475- μm field of view is constrained, extremely rapid scans of a large operative field are possible by simply moving the instrument to various location for acquisition of an “optical biopsy.” The main advantage of the instrument is its ability to study large regions of tumor or resection beds over time periods that multiple frozen section biopsies covering the same area cannot approach. Further development of clinically effective imaging agents could provide instant and real-time intraoperative histopathology while potentially eliminating delays associated with operating room work-flow, processing, and interpretation of frozen sections. Our ability to quickly assess multiple tumor regions is encouraging, although the current probe design creates challenges for imaging deep or remote regions.[24]
In vivo detection and appropriate interpretation of tissue cytoarchitecture by CLE is critically dependent on imaging agents. Earlier studies suggest that CLE fluorescent images developed from fluorescein, acridine orange, acriflavine, cresyl violet percholate, 5-ALA, and indocyanine green can discriminate features of tumor and normal brain [Figure 8].[24,25,26] However, most of these fluorophores cannot be used in vivo in the human brain because of evidence that they may be mutagens. In addition, some of these agents interact with erythrocytes to generate artifacts that decrease CLE image quality and thereby affect analysis. They do allow relatively straightforward discrimination of normal brain and frank tumor. Tumor border areas and areas of blood–brain barrier disruption can be difficult to interpret when stained with fluorophores that produce nonspecific tissue interaction. Specific labeling of brain tumors with fluorescent antibodies, which has been used for tumors in other organ systems, would be a more feasible approach. The results with CLE and FITC-EGFR suggest that an optimized method for in vivo application of this agent may provide a means for selectively labeling and imaging tumor cells in situ to acquire decisive molecular information during neurosurgery. Safe labels developed for rapid application to the tumor intraoperatively and combined with CLE may obviate the need for tumor cells to metabolize a compound, such as with 5-ALA, to produce a detectable fluorescent signal. The 5-ALA is given orally to patients approximately 4 hours prior to imaging. An oral administration route creates a significant delay in fluorescence because of the conversion time of 5-ALA into PPIX.
Figure 8.
In vivo images obtained with the confocal endomicroscope using (a) fluorescein sodium, (b) acriflavine, (c) indocyanine green from the tumor border region reveal nonspecific staining characteristics of tumor cells, as well as other brain tissue components compared to green fluorescent protein. Scale bar 100 μm. Used with permission from Barrow Neurological Institute, Phoenix, Arizona
Previous studies have suggested that a learning curve is associated with the interpretation of confocal images, especially those of tissue labeled with relatively nonspecific fluorescent agents.[14,24,25,26] Combining portable in vivo imaging technology, such as CLE, with selective labeling techniques that specifically target tumor cells should allow straightforward and rapid tumor cell identification and eliminate problems related to nonspecific staining artifacts, providing valuable intraoperative information regarding tumor boundaries and infiltration. For example, because CLE images may be confounded by erythrocytes when using fluorescein, the absence of blood artifacts facilitates acquiring a minimal number of highly informative images from each ROI. Our experiments with GFP-labeled U251 cells and FITC-EGFR labeled cells make clear that CLE can be used to identify tumors at the cellular level [Figure 2].
GFP is a 238-amino acid polypeptide with numerous experimental applications. We used it in this setting for its convenient and specific labeling and to assess the ability of CLE to image within a human glioma cell line. It has been used in vivo as a marker for gene expression for protein localization and folding and as a probe for protein-to-protein interactions.[10] Excitation at 395 nm and 475 nm (very close to the 488-nm excitation of the endomicroscope) leads to green fluorescence emission at 503 nm and 508 nm. When used as an intracellular cytoplasmic contrast agent, GFP provides subcellular visualization of features such as nuclei and cytoplasmic inclusions. When present in glioma cells, cytoplasmic GFP allows accurate assessment of atypical pleomorphic cells and possible mitotic figures. A previous investigation showed potential toxicity of GFP.[15,17] GFP-containing constructs that localize GFP in the nucleus can show damage, possibly related to free-radical generation and damage to DNA. GFP expression also can have adverse effects on morphology and behavior in some animal models. This is a potential limitation of applying GFP in humans.[15,17] However, in this proof-of-principle study, our results show that if such a technique were to be developed, CLE would allow clear detection of appropriately labeled cells in vivo, provided that the imaging system and fluorescent label are within the same laser wavelength range.
FITC is a small fluorophore similar to the clinical contrast agent fluorescein. Although we did not observe a loss of fluorescence signal intensity while imaging FITC-EGFR, images generated by the endomicroscope during in vivo and ex vivo imaging of FITC were less bright and distinct compared to those imaged with GFP labeling. This difference in signal strength may be partially related to the concentrated cytoplasmic expression of GFP within transduced tumor cells compared to greater cell membrane expression of EGFR in transduced cells. Some variants of EGFR represent only a small range of the unique glioma surface molecules that may be exploited as labeling targets that may be imaged with CLE.[28,31,32] Improving the fluorescence detection of the endomicroscope may also enhance future attempts to selectively label and image tumors with FITC.
In this study, tumor cells constitutively expressing GFP or overexpressing EGFR were implanted into rat brains. Our results show that the concept of human in vivo imaging of selective molecular fluorescent labeling of human and rodent glioma cells with a portable intraoperative CLE system is promising.[21] The less invasive characteristics of the particular glioma cell lines used here represent a more challenging scenario wherein the endomicroscope was still adept at identifying the specifically labeled invading tumor cells away from the tumor mass [Figure 3]. In vivo fluorescent imaging of specifically labeled ovarian cancer cells has been reported but not on the microscopic scale reported here.[29] Resection of neoplasms identified by molecular fluorescence imaging with cell-penetrating peptides that can be activated has been reported to decrease residual cancer and to improve survival following resection.[19]
Although the range of this 488-nm CLE system would seem to be restrictive and specific molecular labels may not be visible because they are out of the detectable operating parameters of the system, such labels could conceivably be conjugated directly to a different fluorophore within the system's detection range (a relatively simple chemistry problem) and thus become viewable and informative. As CLE technology grows, multiple bandwidth imaging, e.g. including near-infrared spectrum laser, or widely tunable laser, may become available allowing imaging of multiple co-localized tumor cell fluorescent labels for greater specificity and selectivity.[8] The ability to selectively image tumor cells in vivo on a microscopic level with CLE has significant potential for improving intraoperative diagnoses and guidance for invasive brain tumor surgery that may have profound influence over the extent of resection.
CONCLUSIONS
CLE with specific fluorescence labeling using GFP and an FITC-EGFR conjugated antibody provided real-time in vivo histologic information precisely related to the site of microscopic imaging of an animal glioma model. Correlative histopathologic tumor features were identified, and a definitive tumor border was delimited, especially with the rapid and dynamic positioning of the imaging probe. The data suggest that in vivo CLE of selectively fluorescently tagged neoplasms allows interactive identification of tumor areas in the investigated animal glioma model. Establishing protocols for safe delivery of specifically targeted fluorescent molecules, either inserted into glioma cells before surgery or applied to the tumor intraoperatively, to be used with CLE in humans should be possible. In principle, this imaging technology could substantially improve intraoperative decisions during the resection of brain tumors and radically change the neurosurgery-neuropathology workflow in the operating room.
Financial support and sponsorship
Funding for this study was provided by Barrow Neurological Foundation and the Newsome Endowed Chair in Neurosurgery Research at Barrow Neurological Institute. The Optiscan 5.1 confocal endomicroscope system and Zeiss LSM 710 were provided by Carl Zeiss Meditec AG (Jena, Germany), which has no financial interest in this study at Barrow Neurological Institute.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Contributor Information
Nikolay L. Martirosyan, Email: neuropub@dignityhealth.org;.
Joseph Georges, Email: Neuropub@dignityhealth.org.
M. Yashar S. Kalani, Email: Neuropub@dignityhealth.org.
Peter Nakaji, Email: neuropub@dignityhealth.org.
Robert F. Spetzler, Email: neuropub@dignityhealth.org.
Burt G. Feuerstein, Email: Neuropub@dignityhealth.org.
Mark C. Preul, Email: neuropub@dignityhealth.org.
REFERENCES
- 1.Ammirati M, Vick N, Liao YL, Ciric I, Mikhael M. Effect of the extent of surgical resection on survival and quality of life in patients with supratentorial glioblastomas and anaplastic astrocytomas. Neurosurgery. 1987;2:201–6. doi: 10.1227/00006123-198708000-00012. [DOI] [PubMed] [Google Scholar]
- 2.Ando T, Kobayashi E, Liao H, Maruyama T, Muragaki Y, Iseki H, et al. Precise comparison of protoporphyrin IX fluorescence spectra with pathological results for brain tumor tissue identification. Brain Tumor Pathol. 2011;28:43–51. doi: 10.1007/s10014-010-0002-4. [DOI] [PubMed] [Google Scholar]
- 3.Breuskin D, Divincenzo J, Kim YJ, Urbschat S, Oertel J. Confocal laser endomicroscopy in neurosurgery: A new technique with much potential. Minim Invasive Surg 2013. 2013:851819. doi: 10.1155/2013/851819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Charalampaki P, Javed M, Daali S, Heiroth HJ, Igressa A, Weber F. Confocal Laser Endomicroscopy for Real-time Histomorphological Diagnosis: Our Clinical Experience With 150 Brain and Spinal Tumor Cases. Neurosurgery. 2015;62(Suppl 1):171–6. doi: 10.1227/NEU.0000000000000805. [DOI] [PubMed] [Google Scholar]
- 5.Devaux BC, O’Fallon JR, Kelly PJ. Resection, biopsy, and survival in malignant glial neoplasms. A retrospective study of clinical parameters, therapy, and outcome. J Neurosurg. 1993;78:767–75. doi: 10.3171/jns.1993.78.5.0767. [DOI] [PubMed] [Google Scholar]
- 6.Fenton KE, Martirosyan NL, Abdelwahab MG, Coons SW, Preul MC, Scheck AC. In vivo visualization of GL261-luc2 mouse glioma cells by use of Alexa Fluor-labeled TRP-2 antibodies. Neurosurg Focus. 2014;36:E12. doi: 10.3171/2013.12.FOCUS13488. [DOI] [PubMed] [Google Scholar]
- 7.Foersch S, Kiesslich R, Waldner MJ, Delaney P, Galle PR, Neurath MF, et al. Molecular imaging of VEGF in gastrointestinal cancer in vivo using confocal laser endomicroscopy. Gut. 2010;59:1046–55. doi: 10.1136/gut.2009.202986. [DOI] [PubMed] [Google Scholar]
- 8.Georges JF, Martirosyan NL, Eschbacher J, Nichols J, Tissot M, Preul MC, et al. Sulforhodamine 101 selectively labels human astrocytoma cells in an animal model of glioblastoma. J Clin Neurosci. 2014;21:846–51. doi: 10.1016/j.jocn.2014.02.007. [DOI] [PubMed] [Google Scholar]
- 9.Hatanpaa KJ, Burma S, Zhao D, Habib AA. Epidermal growth factor receptor in glioma: Signal transduction, neuropathology, imaging, and radioresistance. Neoplasia. 2010;12:675–84. doi: 10.1593/neo.10688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hsu ST, Blaser G, Jackson SE. The folding, stability and conformational dynamics of beta-barrel fluorescent proteins. Chem Soc Rev. 2009;38:2951–65. doi: 10.1039/b908170b. [DOI] [PubMed] [Google Scholar]
- 11.Lacroix M, Abi-Said D, Fourney DR, Gokaslan ZL, Shi W, DeMonte F, et al. A multivariate analysis of 416 patients with glioblastoma multiforme: Prognosis, extent of resection, and survival. J Neurosurg. 2001;95:190–8. doi: 10.3171/jns.2001.95.2.0190. [DOI] [PubMed] [Google Scholar]
- 12.Martirosyan NL, Cavalcanti DD, Eschbacher JM, Delaney PM, Scheck AC, Abdelwahab MG, et al. Use of in vivo near-infrared laser confocal endomicroscopy with indocyanine green to detect the boundary of infiltrative tumor. J Neurosurg. 2011;115:1131–8. doi: 10.3171/2011.8.JNS11559. [DOI] [PubMed] [Google Scholar]
- 13.Martirosyan NL, Eschbacher JM, Kalani MY, Turner JD, Belykh E, Spetzler RF, et al. Prospective evaluation of the utility of intraoperative confocal laser endomicroscopy in patients with brain neoplasms using fluorescein sodium: Experience with 74 cases. Neurosurg Focus. 2016;40:E11. doi: 10.3171/2016.1.FOCUS15559. [DOI] [PubMed] [Google Scholar]
- 14.Martirosyan NL, Georges J, Eschbacher JM, Cavalcanti DD, Elhadi AM, Abdelwahab MG, et al. Potential application of a handheld confocal endomicroscope imaging system using a variety of fluorophores in experimental gliomas and normal brain. Neurosurg Focus. 2014;36:E16. doi: 10.3171/2013.11.FOCUS13486. [DOI] [PubMed] [Google Scholar]
- 15.Mawhinney RM, Staveley BE. Expression of GFP can influence aging and climbing ability in Drosophila. Genet Mol Res. 2011;10:494–505. doi: 10.4238/vol10-1gmr1023. [DOI] [PubMed] [Google Scholar]
- 16.Meza D, Wang D, Wang Y, Borwege S, Sanai N, Liu JT. Comparing high-resolution microscopy techniques for potential intraoperative use in guiding low-grade glioma resections. Lasers Surg Med. 2015;47:289–95. doi: 10.1002/lsm.22347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Misteli T, Spector DL. Applications of the green fluorescent protein in cell biology and biotechnology. Nature Biotechnol. 1997;15:961–4. doi: 10.1038/nbt1097-961. [DOI] [PubMed] [Google Scholar]
- 18.Mooney MA, Zehri AH, Georges JF, Nakaji P. Laser scanning confocal endomicroscopy in the neurosurgical operating room: A review and discussion of future applications. Neurosurg Focus. 2014;36:E9. doi: 10.3171/2013.11.FOCUS13484. [DOI] [PubMed] [Google Scholar]
- 19.Nguyen QT, Olson ES, Aguilera TA, Jiang T, Scadeng M, Ellies LG, et al. Surgery with molecular fluorescence imaging using activatable cell-penetrating peptides decreases residual cancer and improves survival. Proc Natl Acad Sci U S A. 2010;107:4317–22. doi: 10.1073/pnas.0910261107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nitta T, Sato K. Prognostic implications of the extent of surgical resection in patients with intracranial malignant gliomas. Cancer. 1995;75:2727–31. doi: 10.1002/1097-0142(19950601)75:11<2727::aid-cncr2820751115>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 21.Olson ES, Jiang T, Aguilera TA, Nguyen QT, Ellies LG, Scadeng M, et al. Activatable cell penetrating peptides linked to nanoparticles as dual probes for in vivo fluorescence and MR imaging of proteases. Proc Natl Acad Sci U S A. 2010;107:4311–6. doi: 10.1073/pnas.0910283107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Peng Q, Berg K, Moan J, Kongshaug M, Nesland JM. 5-Aminolevulinic acid-based photodynamic therapy: Principles and experimental research. Photochem Photobiol. 1997;65:235–51. doi: 10.1111/j.1751-1097.1997.tb08549.x. [DOI] [PubMed] [Google Scholar]
- 23.Rostomily RC, Spence AM, Duong D, McCormick K, Bland M, Berger MS. Multimodality management of recurrent adult malignant gliomas: Results of a phase II multiagent chemotherapy study and analysis of cytoreductive surgery. Neurosurgery. 1994;35:378–88. doi: 10.1227/00006123-199409000-00004. [DOI] [PubMed] [Google Scholar]
- 24.Sanai N, Eschbacher J, Hattendorf G, Coons SW, Preul MC, Smith KA, et al. Intraoperative confocal microscopy for brain tumors: A feasibility analysis in humans. Neurosurgery. 2011;68(2 Suppl Operative):282–90. doi: 10.1227/NEU.0b013e318212464e. [DOI] [PubMed] [Google Scholar]
- 25.Sanai N, Snyder LA, Honea NJ, Coons SW, Eschbacher JM, Smith KA, et al. Intraoperative confocal microscopy in the visualization of 5-aminolevulinic acid fluorescence in low-grade gliomas. J Neurosurg. 2011;115:740–8. doi: 10.3171/2011.6.JNS11252. [DOI] [PubMed] [Google Scholar]
- 26.Sankar T, Delaney PM, Ryan RW, Eschbacher J, Abdelwahab M, Nakaji P, et al. Miniaturized handheld confocal microscopy for neurosurgery: Results in an experimental glioblastoma model. Neurosurgery. 2010;66:410–7. doi: 10.1227/01.NEU.0000365772.66324.6F. [DOI] [PubMed] [Google Scholar]
- 27.Schucht P, Knittel S, Slotboom J, Seidel K, Murek M, Jilch A, et al. 5-ALA complete resections go beyond MR contrast enhancement: Shift corrected volumetric analysis of the extent of resection in surgery for glioblastoma. Acta Neurochir. 2014;156:305–12. doi: 10.1007/s00701-013-1906-7. [DOI] [PubMed] [Google Scholar]
- 28.Tabori U, Rienstein S, Dromi Y, Leider-Trejo L, Constantini S, Burstein Y, et al. Epidermal growth factor receptor gene amplification and expression in disseminated pediatric low-grade gliomas. J Neurosurg. 2005;103(4 Suppl):357–61. doi: 10.3171/ped.2005.103.4.0357. [DOI] [PubMed] [Google Scholar]
- 29.van Dam GM, Themelis G, Crane LM, Harlaar NJ, Pleijhuis RG, Kelder W, et al. Intraoperative tumor-specific fluorescence imaging in ovarian cancer by folate receptor-alpha targeting: First in-human results. Nature Med. 2011;17:1315–9. doi: 10.1038/nm.2472. [DOI] [PubMed] [Google Scholar]
- 30.Widhalm G, Wolfsberger S, Minchev G, Woehrer A, Krssak M, Czech T, et al. 5-Aminolevulinic acid is a promising marker for detection of anaplastic foci in diffusely infiltrating gliomas with nonsignificant contrast enhancement. Cancer. 2010;116:1545–52. doi: 10.1002/cncr.24903. [DOI] [PubMed] [Google Scholar]
- 31.Wikstrand CJ, McLendon RE, Friedman AH, Bigner DD. Cell surface localization and density of the tumor-associated variant of the epidermal growth factor receptor, EGFRvIII. Cancer Res. 1997;57:4130–40. [PubMed] [Google Scholar]
- 32.Wikstrand CJ, Reist CJ, Archer GE, Zalutsky MR, Bigner DD. The class III variant of the epidermal growth factor receptor (EGFRvIII): Characterization and utilization as an immunotherapeutic target. J Neurovirol. 1998;4:148–58. doi: 10.3109/13550289809114515. [DOI] [PubMed] [Google Scholar]
- 33.Wood JR, Green SB, Shapiro WR. The prognostic importance of tumor size in malignant gliomas: A computed tomographic scan study by the Brain Tumor Cooperative Group. J Clin Oncol. 1988;6:338–43. doi: 10.1200/JCO.1988.6.2.338. [DOI] [PubMed] [Google Scholar]
- 34.Zehri AH, Ramey W, Georges JF, Mooney MA, Martirosyan NL, Preul MC, et al. Neurosurgical confocal endomicroscopy: A review of contrast agents, confocal systems, and future imaging modalities. Surg Neurol Int. 2014;5:60. doi: 10.4103/2152-7806.131638. [DOI] [PMC free article] [PubMed] [Google Scholar]