

Abstract
Background:
Cerebral hyperperfusion after carotid endarterectomy (CEA) is defined as an increase in ipsilateral cerebral blood flow (CBF). Practically, however, prompt and precise assessment of cerebral hyperperfusion is difficult because of limitations in the methodology of CBF measurement during the perioperative period. Arterial spin labeling (ASL) is a completely noninvasive and repeatable magnetic resonance perfusion imaging technique that uses magnetically-labelled blood water as an endogenous tracer. To clarify the usefulness of ASL in the management of cerebral hyperperfusion, we investigated signal changes by ASL with a single 1.5-s post-labeling delay on visual inspection.
Methods:
Thirty-two consecutive patients who underwent CEA were enrolled in this retrospective study.
Results:
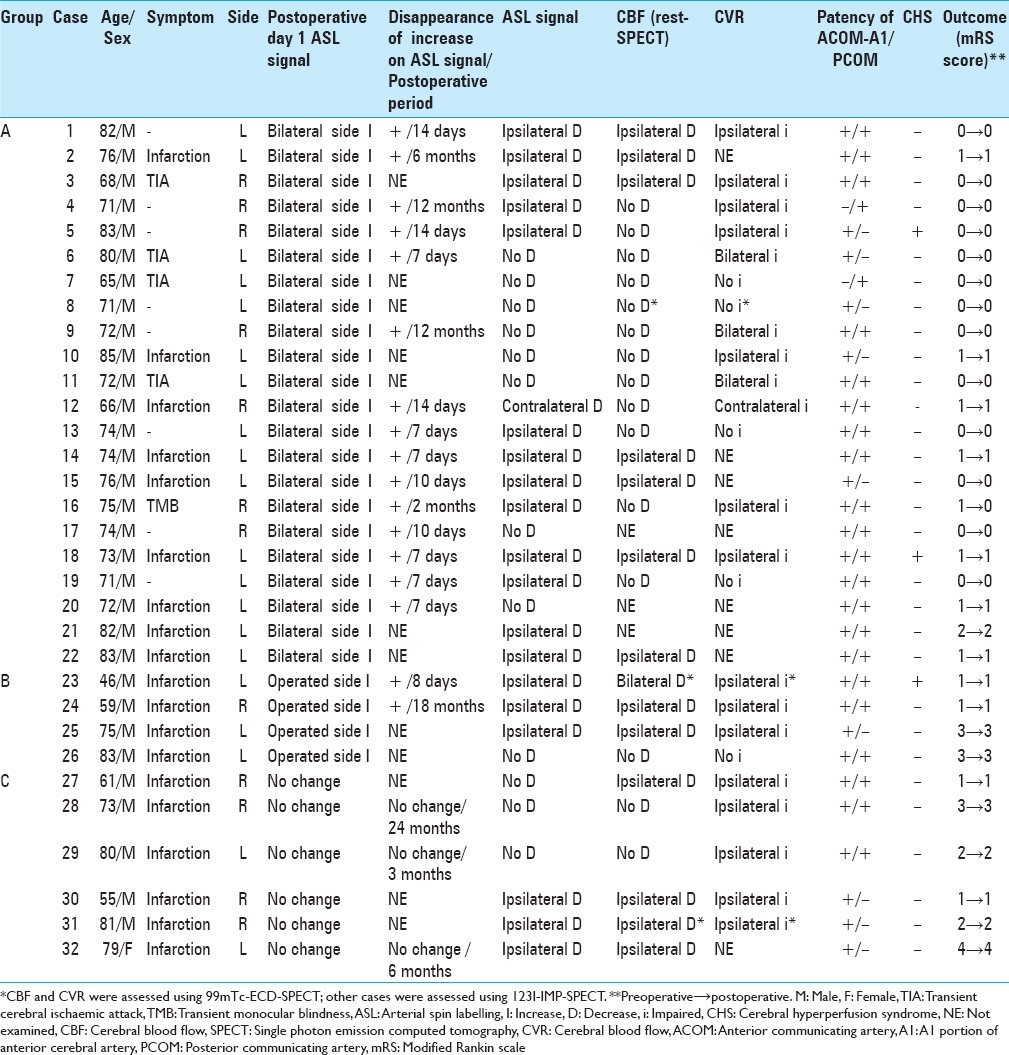
On postoperative day 1, 22 (68.8%) and 4 (12.5%) patients exhibited increased ASL signals bilaterally (Group A) and on the operated side (Group B), respectively. Follow-up ASL showed improvement in these findings. Six (18.8%) patients showed no change (Group C). There was no apparent correlation between ASL signals on postoperative day 1 and the preoperative hemodynamic state, including the cerebrovascular reserve (P = 0.2062). Three (9.4%) patients developed cerebral hyperperfusion syndrome (two in Group A and one in Group B). Coincidence in the localization of increased ASL signals and electroencephalographic abnormalities was noted in these patients.
Conclusion:
Visual analysis of ASL with a single post-labeling delay overestimates CBF and cannot identify patients at risk of cerebral hyperperfusion syndrome probably because of the strong effect of the shortened arterial transit time immediately after CEA. However, ASL may be used as for screening.
Keywords: Arterial spin labeling, carotid endarterectomy, cerebral hyperperfusion, cerebral hyperperfusion syndrome
INTRODUCTION
Cerebral hyperperfusion after carotid endarterectomy (CEA) is defined as a major increase in ipsilateral cerebral blood flow (CBF) after surgical repair of carotid stenosis that is well beyond the metabolic demands of the brain tissue.[4,25,29,31,33,37] However, prompt and precise assessment of cerebral hyperperfusion is often difficult because of limitations in the methodology of CBF measurement during the perioperative period.[4,25,29,31,33,37] Previous reports have demonstrated cerebral hyperperfusion after CEA with transcranial Doppler, Xe-enhanced computed tomography (CT), or single-photon emission CT (SPECT) using 99mTc-ethylcysteinate dimer (ECD) or N-isopropyl-[123I] b-iodoamphetamine (IMP).[9,10,13,20,24,25,26,32,37] The criteria for cerebral hyperperfusion vary among these studies.[25,29,37] Diagnosis of cerebral hyperperfusion syndrome (CHS) is based not only on evidence of hyperperfusion on these CBF studies but also on the presence of clinical symptoms such as seizures, deterioration of consciousness (including restlessness), and the development of focal neurological signs such as motor weakness.[25,28,29,37]
Among the various CBF studies performed to date, SPECT has been widely used in Japan to assess the cerebral hemodynamic state and quantify the regional CBF and hemodynamic reserve by measuring the patient's cerebrovascular reactivity (CVR) to acetazolamide loading.[17,22,28,34] Ogasawara et al.[28] reported that IMP-SPECT can be used to preoperatively measure the CVR and identify patients at risk for cerebral hyperperfusion; in addition, post-CEA monitoring of CBF, including immediately after CEA, allows for timely and reliable identification of patients at risk for CHS. However, repeating SPECT studies is practically difficult because administration of the exogenous radioisotope is required.
A new magnetic resonance (MR) perfusion imaging technique with arterial spin labeling (ASL) was recently developed to assess the regional CBF without the need for contrast administration.[2,5,6,7,8,21,32] Because ASL uses magnetically-labelled blood water as an endogenous tracer,[30] it is a completely noninvasive and repeatable perfusion imaging technique. Previous authors demonstrated a close correlation between ASL and SPECT imaging in terms of assessment of the CBF status.[19,27,32,35,36] However, ASL has some drawbacks. It has a time delay called the “post-labeling delay” (PLD) between inversion of blood spins passing through the labeling plane in the neck and collection of images in the head after the labelled blood flows into the cerebral tissue.[2] An ASL sequence with no delay compensation is considerably susceptible to the arrival time of labelled blood in tissue; namely, the arterial transit time (ATT).[6,7,8] Recent ASL studies have generally used a single PLD that typically ranges from 1.5 to 2.0 s as a trade-off between maintaining adequate diagnostic quality and allowing sufficient delay for visualizing tissue perfusion in clinical MR imaging machines.[11,21,39] In steno-occlusive cerebrovascular disease, however, the ATT is generally prolonged due to stenosis or occlusion of the major arteries.[39] Labelled blood that travels via collateral pathways of the circle of Willis or secondary collateral pathways, including those associated with leptomeningeal anastomosis, may also exhibit an increased ATT.[11,20,26] In this situation, conventional ASL measurements using a single PLD may lead to an underestimation of tissue perfusion.[11] Conversely, following CEA, improvement of the delayed anterograde flow in the internal carotid artery (ICA) may shorten the ATT, and ASL may lead to an overestimation of the CBF.[36]
In this report, we demonstrate the chronological changes in ASL signals with a single PLD of 1.5 s immediately after CEA, and compare these findings with preoperative clinical conditions and hemodynamic states. A previous study reported signal changes on ASL with a single PLD of 1.5 s at 3 months postoperatively.[3] The purpose of this study was to determine whether ASL can assess post-CEA hemodynamic changes and identify patients at risk for CHS.
PATIENTS AND METHODS
Patients
Thirty-two consecutive patients with ipsilateral ICA stenosis underwent CEA at Kyushu Rosai Hospital from November 2011 to April 2016. The inclusion criteria for CEA used in our institute are carotid stenosis of ≥70% or 50–69% with repeated ischemic cerebrovascular events, activities of daily living corresponding to a modified Rankin Scale (mRS) score of ≤2 in asymptomatic patients and 3 or 4 in symptomatic patients with repeated ischemic cerebrovascular events, small or no infarction on MR imaging, and absence of major occlusive disease (≥70% in diameter) distal to the carotid stenosis. Thirty-one of the 32 patients were men, and 1 was a woman. The mean age of the patients was 73.0 years (range, 46–85 years). We reviewed all medical records. Informed consent was obtained from all the patients.
Cerebral blood flow measurements
Arterial spin labeling measurements
Routine MR imaging and ASL perfusion imaging were performed using a 3T-MR unit (Signa HDxt 3.0T version 23; GE Healthcare, Milwaukee, WI, USA). ASL was prepared using a three-dimensional (3D) spiral fast-spin echo sequence with background suppression for perfusion imaging covering the entire brain. A pulsed continuous scheme was employed. Other acquisition parameters were as follows: Four arms with 1004 points in each spiral arm, phase encoding in the z direction = 32, section thickness = 4 mm, Time to repeat (TR) = 4728 (AUTO) s, post-label wait = 1.525 s (1.5 s), and number of excitation (NEX) = 3. The acquisition time was 2 min 22 s.
All patients underwent preoperative ASL examination with routine MR examination. In all patients, a second ASL examination was performed on postoperative day 1 (POD1); i.e., immediately after extubation of the orotracheal tube. At that time, routine MR imaging was also performed to rule out the appearance of perioperative de novo ischemic events. Follow-up ASL was performed when needed. The timing of follow-up ASL varied in this study. Evaluation of decreased or increased ASL signals was based on visual inspection by two experienced radiologists who were blind to the clinical and imaging data. No differences in the radiologists’ interpretations were noted on independent assessments.
Single photon emission computed tomography measurements
Using SPECT (Headtome SET-031; Shimadzu Co., Kyoto, Japan), CBF was semiquantitatively measured before and 15 min after intravenous injection of 10 mg/kg of acetazolamide (ACZ) on separate days at an interval of 2 to 3 days. Regions of interest were placed automatically in the target area (e.g. in the middle cerebral artery [MCA] territory) using commercially available software (E. CAM Signature; Toshiba Medical, Tokyo, Japan/GMS7700R). The CVR to ACZ was calculated as follows: CVR (%) =100 × (CBFACZ − CBFREST)/CBFREST, where CBFREST and CBFACZ represent CBF before and after intravenous injection of ACZ, respectively. A CVR of <20% was considered to be a reduced CVR according to a previous report.[28]
Twenty-nine patients underwent preoperative SPECT imaging at rest. In 24 patients, CVR was assessed with an ACZ challenge. Of these 24 patients, 21 were assessed with IMP-SPECT and 3 with ECD-SPECT.
Electroencephalography
Twenty-nine of the 32 patients underwent routine EEG recording preoperatively and on POD1. Follow-up EEG was performed in 3 patients who developed CHS. Routine EEG recordings were obtained from an 18-channel digital EEG machine (Neurofax; Nihon-Kohden, Tokyo, Japan) with electrode placement according to the International EEG 10-20 system. The EEG recordings were performed for at least 30 min for each patient at rest.
Perioperative management of patients
Twenty-eight patients underwent CEA more than 1 month after the last ischemic event, and 4 patient underwent CEA urgently. All CEA procedures were performed under an operative microscope with the use of internal shunts.
After CEA, general anesthesia with propofol was continued under controlled ventilation until the next morning. Blood pressure was maintained at <130 mm Hg (systolic) and <90 mm Hg (diastolic) in all patients using intravenous nicardipine. Immediately after extubation, all patients underwent routine MR imaging examination including ASL, as described above. In patients with increased ASL signals, arterial blood pressure was more closely monitored and strict control of blood pressure using intravenous nicardipine and diltiazem and an oral angiotensin II receptor blocker was continued until POD7. Diagnosis of CHS was based on the appearance of clinical symptoms and EEG abnormalities that could explain the clinical findings in addition to evidence of increased ASL signals. In Case 5, postoperative ECD-SPECT was also performed to confirm the cerebral hyperperfusion. Functional outcomes were assessed at discharge using the mRS.[38]
RESULTS
Relationship between preoperative arterial spin labeling signals and preoperative single photon emission computed tomography
[Table 1]. Preoperative ASL signals mostly coincided with the CBF map on resting SPECT with visual inspection. However, ASL had a tendency to underestimate the CBF. On preoperative ASL, 19 of 32 patients exhibited decreased ASL signals on the ipsilateral side. On preoperative SPECT of these patients, an ipsilateral decrease in the CBF was noted in 12 patients, no decrease was noted 5, and a bilateral decrease was noted in 1. Nine of the 12 patients with no decreased signal on ASL also exhibited no decreased CBF on SPECT. One other patient showed a decreased CBF of the ipsilateral side on SPECT. In a patient with decreased ASL signals on the contralateral side, no decreased CBF was noted on SPECT.
Table 1.
Clinical profile of 32 patients with carotid stenosis who underwent carotid endarterectomy
Arterial spin labeling signals on postoperative day 1 and their chronological course
On POD1, 22 (68.8%) of 32 patients exhibited increased ASL signals on both sides (Group A) [Figure 1a]. All patients except two (Case 5; detailed clinical course described below and Case 18) did not develop a de novo neurological deficit attributed to increased ASL signals on both sides. The increased ASL signals were improved in all 15 patients who underwent re-examination of their CBF by follow-up ASL. The increased ASL signals had disappeared by POD7 in six patients, by POD14 in 5, by postoperative month 2 in 1, by postoperative month 6 in 1, and by postoperative month 14 in 2.
Figure 1.
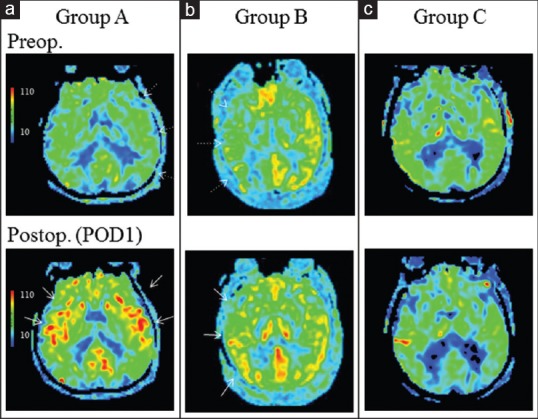
(a) Group A (Case 6): Preoperative (Preop.) perfusion images with arterial spin labeling (ASL) showed decreased signals in the affected hemisphere (white dotted arrows) (upper panel). Postoperative (Postop.) ASL on postoperative day 1 (POD1) showed increased signals in both hemispheres (white arrows) (lower panel). (b) Group B (Case 24): Preoperative ASL showed decreased signals in the affected hemisphere (white dotted arrows) (upper panel). ASL on POD1 showed increased signals only in the operated hemisphere (white arrows) (lower panel). (c) Group C (Case 29): Preoperative ASL showed decreased signals in both hemispheres (upper panel). ASL on POD1 showed no increased signals (lower panel)
Four (12.5%) patients demonstrated increased ASL signals only on the operated side (Group B) [Figure 1b]. All patients except one (Case 23; detailed clinical course described below) did not develop a de novo neurological deficit attributed to the ipsilateral increased ASL signals. Two patients underwent re-examination of their CBF by follow-up ASL; the increased ASL signals had disappeared by POD8 in one patient and by postoperative month 18 in the other.
Six (18.8%) patients showed no change in their postoperative ASL signals compared with the preoperative ASL images (Group C) [Figure 1c]. None of these patients developed de novo neurological deficits. Three patients underwent re-examination of their CBF by follow-up ASL, and the ASL signals exhibited no change in all 3 patients.
Relationship between arterial spin labeling signals on postoperative day 1 and pre and postoperative clinical conditions
Preoperatively, 13 of 22 patients in Group A were asymptomatic or had a history of transient ischemic attack or transient monocular blindness. Nine patients had experienced small but symptomatic infarctions. The preoperative mRS score was 0 in 13 patients, 1 in 8 patients, 2 in 1 patient. Their mRS scores did not change postoperatively except one (Case 16; improved).
In contrast, all patients in Groups B and C had old infarctions. In Group B, the preoperative mRS score was 1 in 2 patients and 3 in 2 patients. In Group C, the preoperative mRS score was 1 in 2 patients, 2 in 2 patients, 3 in 1 patient, and 4 in 1 patient. The mRS scores in Groups B and C did not change postoperatively.
Relationship between arterial spin labeling signals on postoperative day 1 and preoperative hemodynamic state
There was no apparent correlation between the ASL signals on POD1 and the preoperative hemodynamic state, as indicated by preoperative ASL, CBF detected by SPECT at rest, and CVR. Among 22 patients in Group A, the preoperative ASL signals exhibited an ipsilateral decrease in 13 patients, no decrease in 8, and a contralateral decrease in 1 with contralateral internal carotid artery occlusion. Preoperative SPECT imaging showed an ipsilateral decrease in the CBF in seven patients and no decrease in twelve. CVR impairment was observed on the ipsilateral side in 7 of 15 patients, bilaterally in 3, and on the contralateral side in 1 with contralateral ICA occlusion. Four patients demonstrated no CVR impairment.
In 4 patients in Group B, the preoperative ASL signals exhibited an ipsilateral decrease in 3 patients and no decrease in 1. Preoperative SPECT images showed an ipsilateral decrease in the CBF in 2 patients, a bilateral decrease in one, and no decrease in one. CVR impairment was observed on the ipsilateral side in 3 patients, and 1 patient demonstrated no CVR impairment.
In 6 patients in Group C, the preoperative ASL signals exhibited an ipsilateral decrease in 3 patients and no decrease in 3. Preoperative SPECT images showed an ipsilateral decrease in the CBF in 4 patients and no decrease in 2. CVR impairment was observed on the ipsilateral side in 5 of the 6 patients.
Conversely, in 15 patients with impaired ipsilateral CVR, increased ASL signals on POD1 were seen on both sides in 7 patients and unilaterally in 3. However, in the remaining 5 patients, increased ASL signals were not seen. In 5 patients without ipsilateral CVR impairment, increased ASL signals on POD1 were seen on both sides in 4 patients and unilaterally in 1. The lack of a correlation between the ASL signals on POD1 and CVR was statistically significant (P = 0.2062, Chi-square test using JMP Pro 10.0.2 [SAS Institute Inc., Cary, NC, USA]).
There was also no apparent correlation between ASL signals on POD1 and patency of the anterior communicating artery-A1 portion of the anterior cerebral artery (ACOM-A1) and the ipsilateral posterior communicating artery (PCOM) on MR angiography. The ACOM-A1 was not patent in only 2 patients in Group A. The ipsilateral PCOM was patent in 17 of 22 patients in Group A, 3 of 4 patients in Group B, and 3 of 6 patients in Group C.
Development of cerebral hyperfusion syndrome
Three out of 32 (9.4%) patients exhibited CHS. These 3 patients were Case 5 and Case 18 in Group A, and Case 23 in Group B. The detailed clinical courses and hemodynamic as well as EEG findings of Case 5 and Case 23 are described below as representative cases because the clinical profiles and EEG findings of Case 18 were quite similar to those of Case 5.
Representative cases
Case 5 (Group A)
An 83-year-old man presented with asymptomatic severe stenosis of the right ICA. He had a history of smoking, hypertension, hyperlipidaemia, aortic regurgitation, and chronic heart failure. His neurological examination revealed no remarkable findings. 3D-CTA revealed severe stenosis of the right ICA at the bifurcation of the common carotid artery [Figure 2a]. Preoperative ASL showed decreased signals in the right MCA territory [Figure 2b]. IMP-SPECT imaging at rest demonstrated mild CBF reduction in the right MCA territory [Figure 2c]. CVR impairment in the right anterior cerebral artery and MCA territory was noted with ACZ loading [Figure 2d].
Figure 2.

Case 5 (Group A). (a) Preoperative three-dimensional computed tomographic angiography (3D-CTA) revealed severe stenosis of the right internal carotid artery (ICA) at the bifurcation of the common carotid artery. (b) Preoperative magnetic resonance perfusion image with arterial spin labeling (ASL) showed decreased signals in the right middle cerebral artery (MCA) territory (white dotted arrows). (c) Single-photon emission computed tomography with N-isopropyl-[123I] b-iodoamphetamine at rest demonstrated mild reduction of cerebral blood flow in the right MCA territory (white dotted arrows). (d) With acetazolamide loading, impairment of cerebrovascular reserve in the right anterior cerebral artery (ACA) and MCA territories was noted (white dotted arrows). (e) On POD1, diffusion-weighted imaging failed to reveal any de novo ischemic lesions. (f) ASL on POD1 clearly showed increased signals in the bilateral ACA and MCA territories, especially on the right side (white arrows). (g) Electroencephalography on POD1 showed slow-wave activities in the bilateral frontal regions (Fp1, Fp2, F3, and F4 of International EEG 10-20 system, black lines) with poorly organized background activities. Asterisks indicate motion artefact due to restless confusion. (h) ASL on POD14 showed disappearance of the increased signals. The preoperative decreased ASL signals in the right MCA territory were also improved. (i) Postoperative 3D-CTA confirmed that the ICA stenosis was improved
On POD1 after CEA, the patient exhibited mildly restless confusion and a talkative state. Although no de novo ischemic events were observed on diffusion-weighted imaging [Figure 2e], ASL clearly showed increased ASL signals on both sides, especially the right [Figure 2f]. EEG on POD1 showed slow-wave activities in the bilateral frontal regions (Fp1, Fp2, F3, and F4 of International EEG 10-20 system) with poorly organized background activities [Figure 2g], indicating diffuse dysfunction, especially concentrated in the bilateral frontal regions. Under a diagnosis of CHS, further intensive control of systolic blood pressure within 100 to 120 mm Hg was performed with intravenous nicardipine, and a free radical scavenger was administered. On POD3, his restlessness was fully resolved. ASL on POD14 showed disappearance of the ASL signal increase [Figure 2h]. The preoperatively decreased ASL signals in the right MCA territory were also improved. Furthermore, 3D-CTA confirmed that the ICA stenosis had improved [Figure 2i]. EEG on POD14 showed disappearance of slow waves in the bifrontal regions. The patient was discharged without neurologic deficits on POD16. His mRS score was 0 (unchanged from the preoperative state).
Case 23 (Group B)
A 46-year-old man presented with transient weakness of his right limbs. He had a history of smoking, hypertension, hyperlipidemia, diabetes mellitus, atrial fibrillation, and chronic heart failure. He had no abnormal neurological findings, although he had an old infarction in the white matter of the left frontal lobe. 3D-CTA revealed severe stenosis of the left ICA [Figure 3a]. Preoperative ASL showed decreased signals in the left MCA territory [Figure 3b]. A preoperative ECD-SPECT image obtained at rest demonstrated mild reduction of CBF in the left MCA territory [Figure 3c]. ACZ challenge depicted CVR impairment in the left MCA territory [Figure 3d].
Figure 3.

Case 23 (Group B). (a) Three-dimensional computed tomographic angiography revealed severe stenosis of the left internal carotid artery. (b) Preoperative arterial spin labeling (ASL) showed decreased signals in the left middle cerebral artery (MCA) territory. (c) Preoperative single-photon emission computed tomography (SPECT) image with 99mTc-ethylcysteinate dimer (ECD) demonstrated reduction of cerebral blood flow in the left MCA territory. (d) Acetazolamide challenge depicted impairment of cerebrovascular reactivity in the left MCA territory. (e) On POD1, diffusion-weighted imaging failed to reveal de novo ischemic events, although an old infarction in the white matter of the left frontal lobe was observed. (f) ASL clearly demonstrated increased signals in the operated left hemisphere. A perfusion defect of the old infarction lesion in the white matter of the left frontal lobe was prominent because the ASL signal in the left hemisphere was increased. (g) Electroencephalography on POD1 showed atypical triphasic waves in the left frontotemporal region (Fp1, F3, and F7, black lines) on diffuse slow-wave activities. (h) ECD-SPECT on POD2 still demonstrated hyperperfusion in the left MCA territory. (i) ASL on POD8 showed no laterality in the ASL signals
On POD1, the patient was found to have motor aphasia. Diffusion-weighted imaging failed to reveal de novo ischemic events, although T2 shine-through of the old infarction in the white matter of the left frontal lobe was observed [Figure 3e]. ASL demonstrated increased ASL signals in the operated left hemisphere [Figure 3f]. A perfusion defect of the old infarction lesion in the white matter of the left frontal lobe became prominent with increased ASL signals in its surroundings. EEG on POD1 showed atypical negative-positive-negative triphasic waves in the left frontotemporal region (Fp1, F3, and F7) on diffuse slow-wave activities [Figure 3g]. The triphasic wave in the left frontotemporal region exhibited “sharp-wave and slow-wave” complex morphologies. The patient was diagnosed with nonconvulsive status epilepticus associated with CHS based on our previous reports.[8,12,23,24,36,37] Fosphenytoin (750 mg) was administered. Intensive systolic blood pressure control at 100–120 mm Hg with intravenous nicardipine and the use of a free radical scavenger relieved the patient's symptoms. On POD2, his aphasia had fully resolved. ECD-SPECT on POD2 still demonstrated hyperperfusion in the left MCA territory [Figure 3h]. On POD8, the increased ASL signals in the left hemisphere were improved [Figure 3i], and EEG showed disappearance of the atypical triphasic waves with physiologically normal background activities without subsequent oral administration of any anticonvulsants. The patient was discharged with no neurologic deficits on POD20. His mRS score was 1 (unchanged from the preoperative state).
DISCUSSION
Preoperative ASL signals with a single PLD of 1.5 s mostly coincided with the CBF map on resting SPECT, supporting the findings of previous reports.[27,30,32,35,36] However, ASL had a tendency to underestimate the CBF probably because of the prolonged ATT in patients with carotid stenosis.[11]
The incidence of post-CEA hyperperfusion detected with SPECT reportedly ranges from 0.5 to 40.0%.[13,16,19,28,29,36,37] These contradictory results are probably attributed to different timing of post-CEA CBF measurements and the various quantitative criterion of hyperperfusion.[25,37] Ogasawara et al.[28] strictly defined post-CEA hyperperfusion as a ≥100% increase in CBF on IMP-SPECT compared with preoperative values and observed ipsilateral hyperperfusion immediately after CEA in 8 (15.6%) out of 51 patients.
In the present study, we measured ASL signals immediately after extubation on POD1 because general anesthesia using propofol was continued until the morning of POD1. Twenty-two (68.8%) and 4 (12.5%) of the 32 patients exhibited increased ASL signals bilaterally and on the operated side, respectively. Follow-up ASL showed improvement in these findings. The higher incidence of transiently increased ASL signals in our study is apparently attributed to the shortening of the ATT not only to the increased CBF. Immediately after CEA, improvement in anterograde ICA perfusion on the operated side and no need for slow streaming collaterals resulted in shortening of the ATT not only in the ipsilateral hemisphere but also in the contralateral hemisphere.
Previous authors have clearly demonstrated that patients with poor preoperative CVR have a potentially increased risk of post-CEA hyperperfusion.[17,28] This is because the cerebral vessels are expanded and the cerebral blood volume is elevated in conditions of poor cerebrovascular reactivity, in which the cerebral vessels cannot constrict if the perfusion pressure is normalized by revascularization. Cerebral perfusion will rise as a result.[17,28] In the present study, the absence of a correlation between preoperative CVR impairment and cerebral hyperperfusion (Groups A and B) may support the idea that ASL with a single PLD does not accurately reflect the CBF.
To overcome these shortcomings of ASL with a single PLD and to achieve quantitative measurements of CBF and ATT, a multiple-PLD ASL approach has been used.[39] Wang et al.[39] presented a multi-PLD ASL protocol using four PLDs of 1.5, 2.0, 2.5, and 3.0 s to achieve simultaneous measurements of CBF and ATT in a total scan time of 11.2 min in patients with moyamoya disease. In addition to the longer scan time, calculation of CBF and ATT requires special software and a workstation; it is not practical for clinical use. Uchihashi et al.[36] demonstrated the usefulness of another ASL quantification approach named quantitative star labeling of arterial region (QUASAR) in the assessment of cerebral hyperperfusion.[18,36] However, it also requires offline data processing with special software and a workstation. In contrast, the acquisition time of our single-PLD method was as short as 2 min 22 s, and a special calculation was not required. Although visual inspection was subjective, no assessment difference was noted with independent interpretations by two radiologists in the present study. Thus, post-CEA hemodynamic changes, including an increased CBF and shortening of the ATT, could be promptly estimated immediately after routine MR examination.
In the present study, 3 patients (Case 5 and Case 18 in Group A, Case 23 in Group B) developed CHS. In Case 5 and 18, on POD1, increased ASL signals were noted on both the sides, and EEG showed slow-wave activities in the bilateral frontal regions with poorly organized background activities, indicating diffuse dysfunction, especially in the bilateral frontal regions. Disinhibition of the bilateral frontal lobes caused by cerebral hyperperfusion explained the patient's restlessness. In our previous report,[24] EEG findings demonstrated that the pathophysiological mechanism of CHS following superficial temporal artery–MCA anastomosis is also cortical dysfunction.
In Case 23, atypical triphasic waves were observed in the frontal region of the ipsilateral side. Atypical triphasic waves are now generally accepted as one of the EEG features in patients with nonconvulsive status epilepticus, although there is still argument against true ictal discharges.[24] A number of reports of patients with CHS have not examined epileptic ictal hyperperfusion[12,21] despite epilepsy being one of the most common clinical manifestations of CHS.[12,23,24] As described in our previous reports,[12,24] ictal hyperperfusion could be included as a pathophysiological condition of CHS.
In these three cases, coincidence in the localization of the increased ASL signals and EEG abnormalities was noted. We speculate that the pathophysiological mechanism of CHS is not straightforward and that the marked increase in the CBF on the ipsilateral side was not the sole factor involved in the development of CHS. Increased flow velocity (i.e. shortening of the ATT) could be an additional factor, as measured with transcranial Doppler by previous authors.[9]
Because a limitation of our study is the small number of patients (n = 32), further studies in a large cohort should be conducted with a more sophisticated ASL method. We recently developed dual PLD method, instead of single PLD method that we used in this study.[1,11] To assess the slowly streaming collateral pathway in chronic steno-occlusive disease, we selected another PLD of 2.5 s, in addition to the routinely used PLD of 1.5 s. In our previous reports,[1,11] we validated the setting of the dual PLDs of 1.5 and 2.5 s by measuring the ATT and identifying the angiographic circulation, including the collateral network, in the target area using digital subtraction angiography. On the contrary, shortening of the ATT is demonstrated immediately after CEA and adequate another PLD setting should be explored. Another promising ASL technique is superselective ASL that enables the measurement of flow territories. This ASL method is able to selectively label various sized vessels from the major arteries down to smaller intracranial vessels supplying brain territories of various sizes.[14,15] This regional perfusion image can track alterations in perfusion territories upon CEA.[15]
CONCLUSION
In conclusion, owing to the effect of the ATT, ASL with a single PLD does not accurately reflect the CBF value and cannot identify patients at risk of CHS. However, ASL is completely noninvasive and can be performed as a part of routine MR imaging examination. Furthermore, ASL can promptly evaluate post-CEA hemodynamic changes, including both an increased CBF and shortening of the ATT. Although a more sophisticated ASL method should be explored, ASL with a single PLD may be used as screening test for cerebral hyperperfusion at present.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors thank Dr. Hiroyuki Nomiyama and Dr. Seitaro Shin for interpreting the SPECT and ASL images.
Footnotes
Contributor Information
Takafumi Shimogawa, Email: shimogawa28@gmail.com.
Takato Morioka, Email: takato@ns.med.kyushu-u.ac.jp.
Tetsuro Sayama, Email: tsayama@ns.med.kyushu-u.ac.jp.
Sei Haga, Email: sei.haga@gmail.com.
Tomoaki Akiyama, Email: akiyama.tomoaki@gmail.com.
Kei Murao, Email: mrok19840314@gmail.com.
Yuka Kanazawa, Email: yu8850@gmail.com.
Yoshihiko Furuta, Email: frt@kyudai.jp.
Ayumi Sakata, Email: asakata@med.kyushu-u.ac.jp.
Shuji Arakawa, Email: shuji6031@gmail.com.
REFERENCES
- 1.Akiyama T, Morioka T, Shimogawa T, Haga S, Sayama T, Kanazawa Y, et al. Arterial spin-labeling magnetic resonance perfusion imaging with dual postlabeling delay in internal carotid artery steno-occlusion: Validation with digital subtraction angiography. J Stroke Cerebrovasc Dis. 2016;pii:S1052. doi: 10.1016/j.jstrokecerebrovasdis.2016.06.005. [DOI] [PubMed] [Google Scholar]
- 2.Alsop DC, Detre JA. Multisection cerebral blood flow MR imaging with continuous arterial spin labeling. Radiology. 1998;208:410–6. doi: 10.1148/radiology.208.2.9680569. [DOI] [PubMed] [Google Scholar]
- 3.Ances BM, McGarvey ML, Abrahams JM, Maldjian JA, Alsop DC, Zager EL, et al. Continuous arterial spin labeled perfusion magnetic resonance imaging in patients before and after carotid endarterectomy. J Neuroimaging. 2004;14:133–8. [PubMed] [Google Scholar]
- 4.Coutts SB, Hill MD, Hu WY, Sutherland GR. Hyperperfusion syndrome: Toward a stricter definition. Neurosurgery. 2003;53:1053–69. doi: 10.1227/01.neu.0000088738.80838.74. [DOI] [PubMed] [Google Scholar]
- 5.Deibler AR, Pollock JM, Kraft RA, Tan H, Burdette JH, Maldjian JA. Arterial spin-labeling in routine clinical practice, part 1: Technique and artifacts. AJNR Am J Neuroradiol. 2008;29:1228–34. doi: 10.3174/ajnr.A1030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Deibler AR, Pollock JM, Kraft RA, Tan H, Burdette JH, Maldjian JA. Arterial spin-labeling in routine clinical practice, part 2: Technique and artifacts. AJNR Am J Neuroradiol. 2008;29:1235–41. doi: 10.3174/ajnr.A1030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Deibler AR, Pollock JM, Kraft RA, Tan H, Burdette JH, Maldjian JA. Arterial spin-labeling in routine clinical practice, part 3: Technique and artifacts. AJNR Am J Neuroradiol. 2008;29:1428–35. doi: 10.3174/ajnr.A1030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Detre JA, Alsop DC, Vives LR, Maccotta L, Teener JW, Raps EC. Noninvasive MRI evaluation of cerebral blood flow in cerebrovascular disease. Neurology. 1998;50:633–41. doi: 10.1212/wnl.50.3.633. [DOI] [PubMed] [Google Scholar]
- 9.Fujimoto S, Toyoda K, Inoue T, Hirai Y, Uwatoko T, Kishikawa K, et al. Diagnostic impact of transcranial color-coded real-time sonography with echo contrast agents for hyperperfusion syndrome after carotid endarterectomy. Stroke. 2004;35:1852–6. doi: 10.1161/01.STR.0000133131.93900.ff. [DOI] [PubMed] [Google Scholar]
- 10.Fujimura M, Kaneta T, Mugikura S, Shimizu H, Tominaga T. Temporary neurologic deterioration due to cerebral hyperperfusion after superficial temporal artery-middle cerebral artery anastomosis in patients with adult-onset moyamoya disease. Surg Neurol. 2007;67:273–82. doi: 10.1016/j.surneu.2006.07.017. [DOI] [PubMed] [Google Scholar]
- 11.Haga S, Morioka T, Shimogawa T, Akiyama T, Murao K, Kanazawa Y, et al. Arterial spin labeling perfusion magnetic resonance image with dual postlabeling delay: A correlative study with acetazolamide 123I-Iodoanphetamine single-photon emission computed tomography. J Stroke Cerebrovasc Dis. 2016;25:1–6. doi: 10.1016/j.jstrokecerebrovasdis.2015.08.025. [DOI] [PubMed] [Google Scholar]
- 12.Hamamura T, Morioka T, Sayama T, Mukae N, Arakawa S, Maeda H, et al. Cerebral hyperperfusion syndrome associated with non-convulsive status epilepticus following superficial temporal artery-middle cerebral artery anastomosis – A case report. Neurol Med Chir. 2010;50:1099–104. doi: 10.2176/nmc.50.1099. [DOI] [PubMed] [Google Scholar]
- 13.Hayashi K, Horie N, Suyama K, Nagata I. Incidence and clinical features of symptomatic cerebral hyperperfusion syndrome after vascular reconstruction. World Neurosurg. 2012;78:447–54. doi: 10.1016/j.wneu.2011.10.041. [DOI] [PubMed] [Google Scholar]
- 14.Helle M, Norris DG, Rüfer S, Alfke K, Jansen O, van Osch MJ. Superselective pseudocontinuous arterial spin labeling. Magn Reson Med. 2010;64:777–86. doi: 10.1002/mrm.22451. [DOI] [PubMed] [Google Scholar]
- 15.Helle M, Rüfer S, van Osch MJ, Nabavi A, Alfke K, Norris DG, et al. Superselective arterial spin labeling applied for flow territory mapping in various cerebrovascular diseases. J Magn Reson Imaging. 2013;38:496–503. doi: 10.1002/jmri.24041. [DOI] [PubMed] [Google Scholar]
- 16.Hirooka R, Ogasawara K, Sasaki M, Yamadate K, Kobayashi M, Suga Y, et al. Magnetic resonance imaging in patients with cerebral hyperperfusion and cognitive impairment after carotid endarterectomy. J Neurosurg. 2008;108:1178–83. doi: 10.3171/JNS/2008/108/6/1178. [DOI] [PubMed] [Google Scholar]
- 17.Hosoda K, Kawaguchi T, Shibata Y, Kamei M, Kidoguchi K, Koyama J, et al. Cerebral vasoreactivity and internal carotid artery flow help to identify patients at risk for hyperperfusion after carotid endarterectomy. Stroke. 2001;32:1567–73. doi: 10.1161/01.str.32.7.1567. [DOI] [PubMed] [Google Scholar]
- 18.Hosoda K. The Significance of Cerebral Hemodynamics Imaging in Carotid Endarterectomy: A Brief Review. Neurol Med Chir. 2015;55:782–8. doi: 10.2176/nmc.ra.2015-0090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Iwanaga T, Harada M, Kubo H, Funakoshi Y, Kunikane Y, Matsuda T. Operator-bias-free Comparison of Quantitative Perfusion Maps Acquired with Pulsed-continuous Arterial Spin Labeling and Single-photon-emission Computed Tomography. Magn Reson Med Sci. 2014;13:239–49. doi: 10.2463/mrms.2013-0117. [DOI] [PubMed] [Google Scholar]
- 20.Jorgensen LG, Schroeder TV. Defective cerebrovascular autoregulation after carotid endarterectomy. Eur J Vasc Surg. 1993;7:370–9. doi: 10.1016/s0950-821x(05)80252-x. [DOI] [PubMed] [Google Scholar]
- 21.Kanazawa Y, Morioka T, Arakawa S, Furuta Y, Nakanishi A, Kitazono T. Non-convulsive partial status epilepticus mimicking recurrent infarction revealed by diffusion weighted and ASL perfusion MR images. J Stroke Cerebrovasc Dis. 2015;24:731–8. doi: 10.1016/j.jstrokecerebrovasdis.2014.09.026. [DOI] [PubMed] [Google Scholar]
- 22.Kuroda S, Houkin K, Kamiyama H, Mitsumori K, Iwasaki Y, Abe H. Long-term prognosis of medically treated patients with internal carotid or middle cerebral artery occlusion: Can acetazolamide test predict it? Stroke. 2001;32:2110–6. doi: 10.1161/hs0901.095692. [DOI] [PubMed] [Google Scholar]
- 23.Morioka T, Sayama T, Mukae N, Hamamura T, Yamamoto K, Kido T, et al. Nonconvulsive status epilepticus during perioperative period of cerebrovascular surgery. Neurol Med Chir. 2011;51:171–9. doi: 10.2176/nmc.51.171. [DOI] [PubMed] [Google Scholar]
- 24.Morioka T, Sayama T, Shimogawa T, Mukae N, Hamamura T, Arakawa S, et al. Electroencephalographic evaluation of cerebral hyperperfusion syndrome following superficial temporal artery-middle cerebral artery anastomosis. Neurol Med Chir. 2013;53:388–95. doi: 10.2176/nmc.53.388. [DOI] [PubMed] [Google Scholar]
- 25.Moulakakis KG, Mylonas SN, Sfyroeras GS, Andrikopoulos V. Hyperperfusion syndrome after carotid revascularization. J Vasc Surg. 2009;49:1060–8. doi: 10.1016/j.jvs.2008.11.026. [DOI] [PubMed] [Google Scholar]
- 26.Naylor AR, Whyman M, Wildsmith JA, McClure JH, Jenkins AM, Merrick MV, et al. Immediate effects of carotid clamp release on middle cerebral artery blood flow velocity during carotid endarterectomy. Eur J Vasc Surg. 1993;7:308–16. doi: 10.1016/s0950-821x(05)80014-3. [DOI] [PubMed] [Google Scholar]
- 27.Noguchi T, Kawashima M, Irie H, Ootsuka T, Nishihara M, Matsushima T, et al. Arterial spin-labeling MR imaging in moyamoya disease compared with SPECT imaging. Eur J Radiol. 2011;80:e557–62. doi: 10.1016/j.ejrad.2011.01.016. [DOI] [PubMed] [Google Scholar]
- 28.Ogasawara K, Yukawa H, Kobayashi M, Mikami C, Konno H, Terasaki K, et al. Prediction and monitoring of cerebral hyperperfusion after carotid endarterectomy by using single-photon emission computerized tomography scanning. J Neurosurg. 2003;99:504–10. doi: 10.3171/jns.2003.99.3.0504. [DOI] [PubMed] [Google Scholar]
- 29.Ogasawara K, Sakai N, Kuroiwa T, Hosoda K, Iihara K, Toyoda K, et al. Intracranial hemorrhage associated with cerebral hyperperfusion syndrome following carotidendarterectomy and carotid artery stenting: Retrospective review of 4494 patients. J Neurosurg. 2007;107:1130–6. doi: 10.3171/JNS-07/12/1130. [DOI] [PubMed] [Google Scholar]
- 30.Pizzini FB, Farace P, Manganotti P, Zoccatelli G, Bongiovanni LG, Golay X, et al. Cerebral perfusion alterations in epileptic patients during peri-ictal and post-ictal phase: PASL vs DSC-MRI. Magn Reson Imaging. 2013;31:1001–5. doi: 10.1016/j.mri.2013.03.023. [DOI] [PubMed] [Google Scholar]
- 31.Reigel MM, Hollier LH, Sundt TM, Jr, Piepgras DG, Sharbrough FW, Cherry KJ. Cerebral hyperperfusion syndrome: A cause of neurologic dysfunction after carotid endarterctomy. J Vasc Surg. 1987;5:628–34. [PubMed] [Google Scholar]
- 32.Sugino T, Mikami T, Miyata K, Suzuki K, Houkin K, Mikuni N. Arterial spin-labeling magnetic resonance imaging after revascularization of moyamoya disease. J Stroke Cerebrovasc Dis. 2013;22:811–6. doi: 10.1016/j.jstrokecerebrovasdis.2012.05.010. [DOI] [PubMed] [Google Scholar]
- 33.Sundt TM, Jr, Sharbrough FW, Piepgras DG, Kearns TP, Messick JM, Jr, O’Fallon WM. Correlation of cerebral blood flow and electroencephalographic changes during carotid endarterectomy, with results of surgery and hemodynamics of cerebral ischemia. Mayo Clin Proc. 1981;56:533–43. [PubMed] [Google Scholar]
- 34.Takeuchi R, Matsuda H, Yonekura Y, Sakahara H, Konishi J. Noninvasive quantitative measurements of regional cerebral blood flow using technetium-99m-L, L-ECD SPECT activated with acetazolamide: Quantification analysis by equal-volume-split 99mTc-ECD consecutive SPECT method. J Cereb Blood Flow Metab. 1997;17:1020–32. doi: 10.1097/00004647-199710000-00003. [DOI] [PubMed] [Google Scholar]
- 35.Tanaka Y, Nagaoka T, Nair G, Ohno K, Duong TQ. Arterial spin labeling and dynamic susceptibility contrast CBF MRI in postischemic hyperperfusion, hypercapnia, and after mannitol injection. J Cereb Blood Flow Metab. 2011;31:1403–11. doi: 10.1038/jcbfm.2010.228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Uchihashi Y, Hosoda K, Zimine I, Fujita A, Fujii M, Sugimura K, et al. Clinical application of arterial spin-labeling MR imaging in patients with carotid stenosis: Quantitative comparative study with single-photon emission CT. AJNR Am J Neuroradiol. 2011;32:1545–51. doi: 10.3174/ajnr.A2525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.van Mook WN, Rennenberg RJ, Schurink GW, van Oostenbrugge RJ, Mess WH, Hofman PA, et al. Cerebral hyperperfusion syndrome. Lancet Neurol. 2005;4:877–88. doi: 10.1016/S1474-4422(05)70251-9. [DOI] [PubMed] [Google Scholar]
- 38.Van Swieten JC, Koudstaal PJ, Visser MC, Schouten HJ, van Gijn J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke. 1988;19:604–7. doi: 10.1161/01.str.19.5.604. [DOI] [PubMed] [Google Scholar]
- 39.Wang DJ, Alger JR, Qiao JX, Gunther M, Pope WB, Saver JL, et al. Multi-delay multi-parametric arterial spin-labeled perfusion MRI in acute ischemic stroke-Comparison with dynamic susceptibility contrast enhanced perfusion imaging. Neuroimage Clin. 2013;6:1–7. doi: 10.1016/j.nicl.2013.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]